Embed Size (px)
Citation preview
) 353–358www.elsevier.com/locate/knee
The Knee 13 (2006
The evolution of osteoarthritis in 103 patients with ACL reconstructionat 17 years follow-up
T. Aït Si Selmi a,⁎, D. Fithian b, P. Neyret a
a Centre Livet of Orthopaedics Surgery and Traumatology, Hôpital de la Croix Rousse, Centre Livet 69300Caluire, Franceb Kaiser Permanente Medical Group, 250 Travelodge Drive, El Cajon, CA 92020, USA
Received 26 January 2006; accepted 28 February 2006
Abstract
Aim: To evaluate the functional and radiological outcome of a bone–tendon–bone anterior cruciate ligament reconstruction, at long-termfollow-up.Methods: A retrospective study of 148 patients, of which 103 were available for long-term follow-up. Complete functional and radiologicalevaluation (International Knee Documentation Committee scale) were performed in 89 out of the 103 patients [Anderson AF. Rating scales.In: Fu FH, Harner CD, Vince KG, (Eds.). Knee Surgery, Baltimore, Williams and Wilkins vol. 1, 1994; 12, pp. 275-296].Results: The mean follow-up time was 17.4 years. Subjectively, 88% of the patients were very satisfied or satisfied. According to the IKDCscore 55% had type A symptoms, 29% type B, 12% type C, and 4% type D. The IKDC ligament evaluation showed 14.9% type A, 44.8%type B, 35.8% type C, and 4.5% type D. At the review 22.7% had a narrowing <50% (C) and 4.7% a narrowing >50% (D). Onset ofosteoarthritis showed an association with the status of the medial meniscus. Knees with a preserved (healthy or sutured) medial meniscus hada significantly (p<0.05) better radiological outcome. Among these, 9% had a joint space narrowing <50% (C) and 2% had a narrowing>50% (D). Medial meniscectomy, residual laxity, and femoral chondral defects were associated with osteoarthritis.Conclusion: The outcome of anterior cruciate ligament reconstruction plus extra-articular tenodesis is good in the very long term, particularlyin knees with a preserved medial meniscus.© 2006 Elsevier B.V. All rights reserved.
Keywords: ACL reconstruction; Long-term follow-up; Osteoarthritis; Laxity; Meniscal lesions
1. Introduction
The outcome following ACL reconstruction has been thesubject of a number of studies. However, most of thesepublications present short mid term follow-up of a few years[1,13,26]. Reports of 10 years or longer follow-up are rare[11,18,24]. From our view, long-term follow-up is vital inorder to assess the functional and radiological outcome, andthe possible relation to the development of knee joint osteo-arthritis (OA). To the best of our knowledge, there are nopublished studies of ACL reconstructions with more than15 years follow-up time.
⁎ Corresponding author. Tel.: +33 4 72 07 19 73; fax: +33 4 72 07 17 96.E-mail address: [email protected] (T. Aït Si Selmi).
0968-0160/$ - see front matter © 2006 Elsevier B.V. All rights reserved.doi:10.1016/j.knee.2006.02.014
The aim of the present study was to determine the fate ofknees reconstructed with an ACL graft combined with aLemaire extra-articular tenodesis (Dejour procedure), at 11and 17 years after surgery. At such a long time after the indexprocedure, the outcome with regard to sport activities isdifficult to assess, as a natural decline in athletic activity willbe found due to factors other than knee function, as forexample age and social circumstances. However, the linksbetween osteoarthritis (OA) and laxity can be analysed along time after the index procedure.
This retrospective study was performed at a mean follow-up time of 17 years, in 103 patients out of a population of148 that were previously reviewed 11 years after surgery,following an ACL reconstruction with a Dejour procedure[10].The study was intended to identify prognostic factors

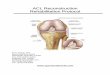
Fig. 2. Extra-articular tenodesis (Lemaire procedure).
354 T. Aït Si Selmi et al. / The Knee 13 (2006) 353–358
influencing the long-term outcome after this type of kneesurgery.
2. Materials and methods
In 1992, 148 patients treated surgically between January 1978and June 1983 for chronic ACL tears by Prof. H. Dejour werereviewed at a mean follow-up of 11.5 years [11]. Those patientswere operated with an open procedure combining an intra-articular reconstruction with a bone–tendon–bone graft, basedupon the technique originally described by Jones [15], associatedwith an extra-articular tenodesis as described by Lemaire [17].This combined technique was first described by Dejour et al. [11]and is referred to as the Dejour procedure. The intra-articulargraft was made up of the central one-third of the patellar tendon,with a bone block at either end. The proximal bone block wasinserted into a femoral socket, and the other bone block insertedinto a tibial tunnel. Both bone blocks were fixed with a wire anda screw with a washer (Fig. 1). The extra-articular tenodesis wasperformed with a 10-mm-wide and 18-cm-long strip of fascia latabased at Gerdy's tubercle and passed under the lateral collateralligament (LCL) through a femoral bone tunnel, and back underthe LCL finally ending in a bone tunnel under Gerdy's tubercle.The tendon fixation was performed with the limb in neutralrotation and the knee at 30° of flexion (Fig. 2).
Through the arthrotomy the condition of the joint was observed,and chondral lesions were registered in particular.
The postoperative regime varied during the period of observa-tion. Patients operated between 1978 and 1980 were immobilized ina plaster cast in slight flexion for 45 days after surgery. From 1981onwards the patients were mobilized immediately after surgery in aremovable splint, following a standardised exercise program.
At the time of this review, 103 of the 148 patients could belocated. Five patients had died before the follow-up. Of the 103patients found, 89 underwent an evaluated complete clinical and aradiological examination. Fourteen patients could be contacted bytelephone and of these, 9 sent in radiographs of their knees. Ninepatients had had bilateral ACL tears, of which 5 had bilateral ACLreconstructions. (In the present study, the number of patient equalsthe number of knees as no one knee was included in the analysis,in cases of bilateral tears.) Of the patient population, 79 weremales and there were 60 right knees. The mean age at injury was
Fig. 1. ACL graft.
22 years (range: 12 to 38 years). The mean age at reconstructionwas 25 years (range 16–43 years), while the mean age at reviewwas 42 years (range 29–61 years).
On average there was a long interval between the injury andreconstruction (mean 36.6 months, range 1 month–19 years). Duringthat time, various surgical procedures had been performed, such as 21medial meniscectomies, three lateral meniscectomies, four ACLrepairs of unknown types, five intra-articular ACL reconstructionsusing the Lindeman technique [19], nine posteromedial reconstruc-tions, two isolated Lemaire reconstructions, three medial transfers ofthe tibial tubercle and two arthroscopies. At the time of thereconstruction, another 38 medial meniscectomies were performed.
Overall, 59 patients had undergone partial or complete medialmeniscectomy either before or at reconstruction, 21 were done pre-operatively and 38 during the index ACL reconstruction. The other44 patients had a medial meniscus that was healthy (32 knees) orwas sutured (12 knees). Twelve meniscus repairs had beenperformed, between 1981 and 1983, through an arthrotomyposterior to the collateral ligament, using vertical absorbablesutures.
After the index reconstruction, nine (16%) medial meniscec-tomies had been performed. In four cases (7%), a meniscus thatwas healthy at the time of Dejour reconstruction subsequentlyrequired removal. The remaining five (9%) were in the group of 12patients who had had meniscal suturing. Two patients wererevised.
After the index reconstruction, seven high tibial valgusosteotomies were performed, in order to relieve pain and to controlthe progression of degenerative joint disease. Additional proceduresincluded two screw removals, two arthrolysis for stiffness, and fourarthroscopies for loose bodies.
The overall assessment was made using the IKDC evaluationform [3], which rates symptoms and function, as well as clinical andradiological findings.
For the radiographic analysis, bilateral radiographs were takenfor comparison. The set of radiographs consisted of AP andlateral views in single-leg stance, a 45° flexion view in two-leg
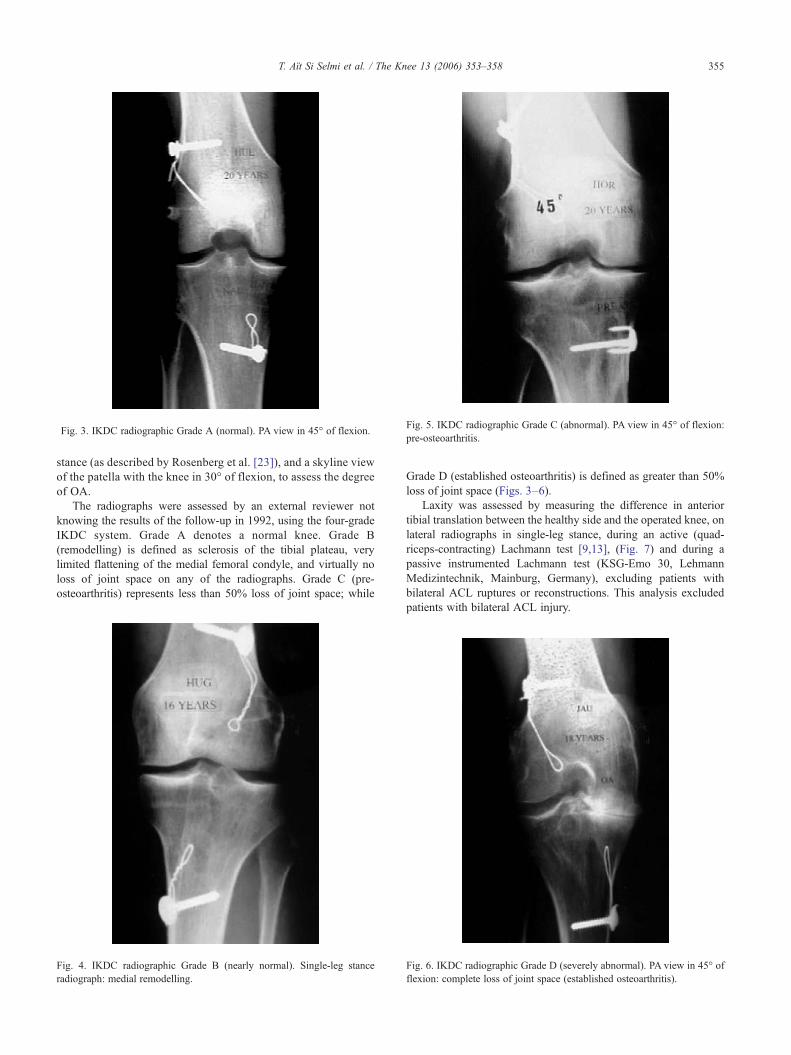
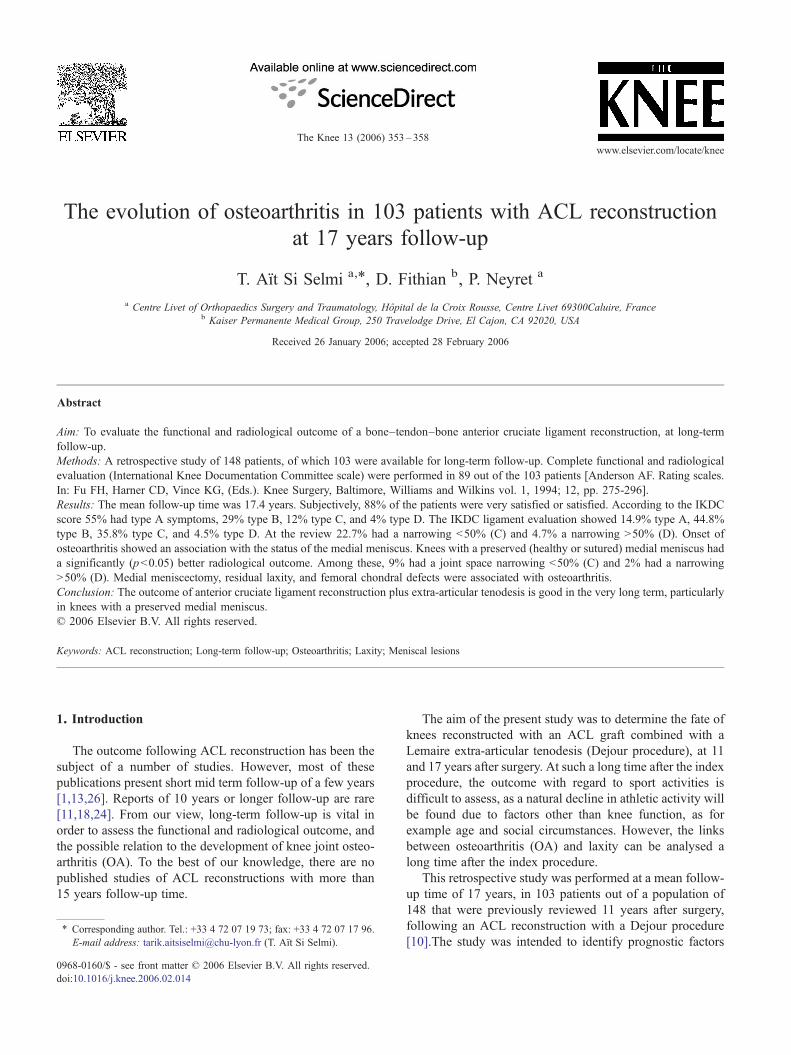
Fig. 5. IKDC radiographic Grade C (abnormal). PA view in 45° of flexion:pre-osteoarthritis.
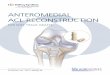
Fig. 3. IKDC radiographic Grade A (normal). PA view in 45° of flexion.
355T. Aït Si Selmi et al. / The Knee 13 (2006) 353–358
stance (as described by Rosenberg et al. [23]), and a skyline viewof the patella with the knee in 30° of flexion, to assess the degreeof OA.
The radiographs were assessed by an external reviewer notknowing the results of the follow-up in 1992, using the four-gradeIKDC system. Grade A denotes a normal knee. Grade B(remodelling) is defined as sclerosis of the tibial plateau, verylimited flattening of the medial femoral condyle, and virtually noloss of joint space on any of the radiographs. Grade C (pre-osteoarthritis) represents less than 50% loss of joint space; while
Fig. 4. IKDC radiographic Grade B (nearly normal). Single-leg stanceradiograph: medial remodelling.
Grade D (established osteoarthritis) is defined as greater than 50%loss of joint space (Figs. 3–6).
Laxity was assessed by measuring the difference in anteriortibial translation between the healthy side and the operated knee, onlateral radiographs in single-leg stance, during an active (quad-riceps-contracting) Lachmann test [9,13], (Fig. 7) and during apassive instrumented Lachmann test (KSG-Emo 30, LehmannMedizintechnik, Mainburg, Germany), excluding patients withbilateral ACL ruptures or reconstructions. This analysis excludedpatients with bilateral ACL injury.
Fig. 6. IKDC radiographic Grade D (severely abnormal). PA view in 45° offlexion: complete loss of joint space (established osteoarthritis).
Fig. 7. Dynamic comparative X-rays (left: normal knee, right: index knee). In this example there is no side to side difference.
Table 2
356 T. Aït Si Selmi et al. / The Knee 13 (2006) 353–358
2.1. Statistical analysis
The data was analysed by Student's t-test, and Chi-square test.Significance was defined as p<0.05.
3. Results
3.1. General evaluation
Data related to symptoms or standard findings are summarizedin Tables 1 and 2. The mean flexion was 134° in the operated sideversus 137° in the non-affected knee.
3.2. Ligament evaluation
According to the IKDC scoring system laxity was: −1 to +2 mm(A) in 27.4% of the cases, +3 to +5 mm (B) in 35.5%, +6 to+10 mm (C) in 30.6 % and more than 10 mm (D) in 6.5%. In 71%of the patients the Lachmannn test showed a firm end-point. In 89%there was no pivot shift, 9% had a glide while 2% had a major pivotshift. The mean residual laxity found using the active Lachmann testwas 4.1 mm (S.D.: 3) in the whole series. In patients with a healthyor sutured medial meniscus it was 3.9 mm (S.D.: 3.4), while patientswho had undergone medial meniscectomy had a mean value of4.2 mm (S.D.: 3.2).
The ligament evaluation showed 14.9% of knees to be Grade A,44.8% were Grade B, 35.8 % were Grade C, and 4.5% were GradeD (Table 1).
Table 1Final evaluation with IKDC standard evaluation form
A B C D
Subjective assessment 34% 54% 10% 2%Symptoms 55% 29% 12% 4%Ligament evaluation 14.9% 44.8% 35.8% 4.5%Radiographic findings 51.1% 21.6% 22.7% 4.7%Final evaluation 11% 44% 39% 6%
3.3. Radiological findings
Radiography showed 51.1% of the operated knees to be normal(A), 21.6% to have a remodelling (B), 22.7% pre-osteoarthritis (C)and 4.7% an established OA (D).
Of the patients who had undergone medial meniscectomy,37.2% had pre-osteoarthritis or established OA. Osteoarthriticlesions were seen to affect only the medial tibiofemoral compart-ment in 66%, and in 30% both compartments were involved, thoughwith the medial compartment more affected than the lateral. In twocases, however, the osteoarthritic lesions were mainly in the lateraltibiofemoral compartment, although the patients concerned had notundergone removal of the lateral meniscus. Of the patients with ahealthy or sutured meniscus, 13.5% had pre-osteoarthritis, orestablished OA.
The lateral tibiofemoral compartment of patients who hadundergone lateral meniscectomy showed pre-osteoarthritis in 5% ofthe cases, and established OA in 9%. It should be noted that, in twothirds of the OA cases, all three knee compartments were involved,with the medial compartment worst affected, especially in patientswho had undergone medial meniscectomy.
The condition of the opposite knee was also assessed. Pre-osteoarthritis was seen in 2% of the contralateral knees, whileestablished OA was found in 7%.
Statistical analysis showed the measured laxity (anterior tibialtranslation) to correlate strongly with the degree of OA (p=0.001),
Symptoms (IKDC ratings)
Symptoms Highest activity level without significant symptoms
Strenuousactivity
Moderateactivity
Lightactivity
Sedentaryactivity
Pain 65% 24% 6% 5%Swelling 73% 20% 6% 1%Partial giving
way91% 6% 3% 0%
Full givingway
97% 3% 0% 0%

Table 3Side to side anterior tibial translation: radiographic evaluation
Meniscus
Healthy orsutured
Meniscectomy
Comparative anteriortibial translation(X-ray)
−1 to 2 mm 37.5% 21%3 to 5 mm 37.5% 34%6 to 10 mm 25% 34%>10 mm 0% 11%
357T. Aït Si Selmi et al. / The Knee 13 (2006) 353–358
with or without meniscectomy. In the meniscectomized knees,anterior tibial translation was increased (p=0.05) (Table 3). Thedegree of OA correlated strongly with a history of medialmeniscectomy (p=0.002), especially where the meniscectomyhad been performed prior to the ligament reconstruction. Wherethe time from injury to reconstruction had been long, there was agreater frequency of meniscectomies in the meantime, and at thereview these patients had a greater residual laxity (p=0.05). Kneesin which chondral lesions had been found at reconstruction showedto be at much greater risk for subsequent OA. These lesions showedevidence of cartilage wear at an early stage, before the degenerativejoint disease becomes radiologically evident.
4. Discussion
It is common knowledge that since 1980 the methods ofgraft fixation and the operative technique have changedconsiderably with the use of arthroscopy, and more activerehabilitation programs. Despite the evolution of surgicaltechniques, the principles remain the same. It is important todemonstrate the long-term effects of surgical intervention.This is the longest reported follow-up of ACL reconstruction.At the time these procedures were done (1978 to 1983), thetime from ligament injury to ligament surgery tended to belong (1–230 months). We believe this explains the largenumber of meniscectomies performed prior to or at ligamentreconstruction (57%). In 60% of these cases, the meniscec-tomies were total. In the review of our patient material, wetherefore felt it necessary to distinguish between two patientcategories: (1) patients with an isolated ACL tear, and (2)patients with an ACL injury associated with a meniscectomyprior to or at ligament reconstruction [7,12,14,16,22]. Atthese long follow-up times it should also be kept in mind thatthe patient's functional demands and physical activitiesnormally have decreased.
4.1. Residual laxity and OA
The mean side to side difference of an average 3.9 mmshows evidence of a non-optimal surgical control of laxity.Such laxity was also found in other corresponding studies[1,2]. This persistent residual laxity shows that the attempt toprevent OA by stabilisation was not completely successful inthe long term.
Another important result was that the functional outcomedid not appear directly linked to the anatomical result. Few ofthe patients complained of giving way, 97% felt that their
knees were perfectly stable. On clinical examination, 89% ofthe patients had no pivot shift. This could suggest that theextra-articular Lemaire tenodesis may make up for theresidual laxity after the intra-articular ACL reconstruction,by preventing or diminishing a pivot shift. Nevertheless, acontrolled trial is necessary to confirm this thought.
Finally, the Lemaire procedure has been thought ofputting the lateral joint at risk by weakening the lateralrestraints, but no medial/lateral imbalance was observed inour series. It should be borne in mind that none of ourpatients had had associated posterolateral lesions prior to theindex procedure.
4.2. Meniscectomy and OA
Previous studies have shown the role, not only of the ACLrupture [25], but also of meniscectomy [20] in the evolutionof arthritis. We believe that residual laxity and meniscectomyare additive risk factors in the development of arthritis,among other non-mechanical factors [5,6,21].
4.3. Frequency of OA
The rate of significant OA in the present study may havebeen to some extent a function of patient age, since 19patients were over 50 years old at review. However, of thenon-operated contralateral knees without ACL tears, only 7%had established OA and 2% had pre-osteoarthritis. The rate ofdegenerative joint disease was especially high among themeniscectomized patients, who had a 45% rate in all of mixedpre-osteoarthritis and established OA. However, it should beborne in mind, as shown by Neyret et al. [20], that an isolatedmedial meniscectomy without any ACL injury leads to a pre-osteoarthritis rate of 10%, and an OA rate of 90%, at 20 yearsfollow-up. Interestingly, knees that were free from OA at11 years follow-up [9] were still normal at 17 years.
In the knees with a preserved medial meniscus only 2%had established OA, and 9% had pre-osteoarthritis. This is inaccordance with earlier published results in non-surgicallytreated ACL tears [4]. In our study the residual laxity wasinterpreted as a contributing factor in the development of OA.Other factors are also known to contribute to degenerativejoint disease, such as chondral lesions seen at surgery, inparticular lesions in the medial compartment [19]. Thisassociation was also found in the present study.
Two patients with advanced OA had pre-osteoarthriticlesions prior to the ligament reconstruction. In these patients,the degenerative joint disease progressed in less than 4 years.It appeared in these two cases, as if the ligament reconstruc-tion could trigger the OA development, as previouslydescribed by Dejour [8,12,13].
In the light of our findings, we feel that radiographsshould be carefully analysed prior to any intended ligamentreconstruction procedure, to look for evidence of degen-erative joint lesions. This is particularly important in olderpatients who have previously undergone meniscectomy.

358 T. Aït Si Selmi et al. / The Knee 13 (2006) 353–358
4.4. Fate of healthy and sutured menisci
Secondary meniscal lesions after ACL reconstructionprovide indirect evidence of the difficulties to obtain fullcontrol of anterior tibial translation. After the ligamentreconstruction, nine secondary medial meniscectomies hadbeen performed. Four of these procedures were for theremoval of a previously healthy or a partially resectedmeniscus, and five were for the removal of a suturedmeniscus. Despite that reconstruction did not seem to protecta meniscal suture or the meniscus itself in these cases, the rateof secondary meniscectomies was much lower compared tothe figures reported in studies of the natural history of ACLtears treated non-operatively [4,10,12,14].
5. Conclusion
The present study demonstrates that ACL reconstructiondoes not always prevent the onset of OA when the medialmeniscus is removed. The functional subjective outcome 17years after surgery was generally satisfactory. It wasexcellent in those patients whose medial meniscus hadbeen preserved. The relatively high rate of degenerative jointlesions should be seen in the light of the natural history ofnon-operated ACL tears [12]. However, this comparison isdifficult to make since the patients in the two groups are notnecessarily comparable.
References
[1] Aglietti P, Buzzi R, Giron F, Biddau F, Sasso F. Arthroscopic assistedanterior cruciate ligament reconstruction with the central third patellartendon. A 5–8 year follow-up. Knee Surg Sports Traumatol Arthrosc1997;5:138–44.
[2] Aglietti P, Buzzi R, D'andria S, Zaccherotti F. Long-term study ofanterior cruciate ligament reconstruction for chronic instability usingthe central one-third patellar tendon and a lateral extraarticulartenodesis. Am J Sports Med 1992;20:38–45.
[3] Anderson AF. Rating scales. In: Fu FH, Harner CD, Vince KG,(Eds.). Knee Surgery, Baltimore, Williams and Wilkins vol. 1, 1994;12, pp. 275–296.
[4] Anderson C, Odensten M, Gillquist G. Knee function after surgical ornonsurgical treatment of acute rupture of the anterior cruciate ligament:a randomized study with a long-term follow-up period. Clin OrthopRelat Res 1991;261:255–63.
[5] Cameron M, Buchgraber A, Passler H, Vogt M, Thonar E, Fu F, et al.The natural history of the ACL deficient knee. Changes in synovialfluid cytokin and keratan sulfate concentration. Am J Sports Med1997;6:751–4.
[6] Chol C, Ait Si Selmi T, Chambat P, Neyret P. Devenir à 17 ans de reculdes ligamentoplasties du ligament croisé antérieur avec ménisqueinterne sain ou saturé. Rev Chir Orthop 2002;88(2):157–62.
[7] Daniel DM, Stone ML, Dobson BE, Fithian DC, Rossman DJ,Kaufman KR. Fate of the ACL-injured patient. A prospective outcomestudy. Am J Sports Med 1994;22(5):632–44.
[8] Dejour H, Neyret P, Boileau P, Donell ST. Anterior cruciate ligamentreconstruction combined with valgus tibial osteotomy. Clin Orthop1994;299:220–8.
[9] Dejour H, Walch G, Chambat P, et al. Active subluxation in extension.A new concept of study of the ACL deficient knee. Am J Knee Surg1988;4:204–11.
[10] Dejour H, Walch G, Neyret P, Adeleine P. Résultats des laxitéschroniques antérieures opérées. A propos de 251 cas revus avec unrecul minimum de 3 ans. Rev Chir Orthop 1988;74:622–36.
[11] Dejour H, Dejour D, Ait Si Selmi T. Laxités antérieures chroniques dugenou traitées par greffe libre de tendon rotulien avec plastie latéraleextra-articulaire. Rev Chir Orthop 1999;85:777–89.
[12] Fithian DC, Paxton LW, Goltz DH. Fate of the anterior cruciateligament-injured knee. Orthop Clin North Am 2002;33(4):621–36.
[13] Franklin JL, Rosenberg TD, Paulos LE, France EP. Radiographicassessment of instability of the knee due to rupture of the anteriorcruciate ligament. A quadriceps contraction technique. J Bone JointSurg A 1991;73-A:365–72.
[14] Hawkins RJ, Misamore GW, Merritt TR. Follow-up of the acute non-operated isolated ACL tear. Am J Sports Med 1986;14:205–10.
[15] Jones K. Reconstruction of the anterior cruciate ligament. A techniqueusing the central one-third patellar ligament. J Bone Joint Surg A1963;45-A:925–32.
[16] Kannus P, Jarvinen M. Conservatively treated tears of the anteriorcruciate ligament. Long-term results. J Bone Joint Surg A 1987;69-A:1007–12.
[17] Lemaire M. Résultats de la plastie extra-articulaire palliative de larupture du ligament croisé antérieur. Rev Chir Orthop 1983;69:278–82.
[18] Lerat JL, Chotel F, Besse JL, Moyen B, Binet G, Craviari T, et al. Lesrésultats après 10 à 16 ans du traitement de la laxité antérieure du genoupar reconstruction du ligament croisé antérieur avec un greffe dutendon rotulien associée à une plastie extra-articulaire externe. RevChir Orthop 1998;1:712–27.
[19] Lindeman. La plastie des ligaments croisés par greffe tendineusepédiculée. Z Orthop 1979:316–34.
[20] Neyret P, Walch G, Dejour H. La méniscectomie interne intramuraleselon la technique de A. Trillat. Résultat à long terme de 258interventions. Rev Chir Orthop 1988;74:637–46.
[21] O'Connor BL, Palmoski MJ, Brandt KD. Neurogenic accelerationof degenerative joint lesions. J Bone Joint Surg A 1985;67-A:562–572.
[22] Rongieras F, Ait Si Selmi T, Neyret P. Histoire naturelle des ruptures duLCA. Index Traumatol Sport 1998;5(Suppl 1):67–73.
[23] Rosenberg TD, Paulos LE, Parker RD, Coward DB, Scott SM. Theforty-five-degree posteroanterior flexion weight-bearing radiograph ofthe knee. J Bone Joint Surg A 1988;70-A(10):1479–82.
[24] Selva O, Chambat P, Telos WG, Casalonga D, Bonnin M.Reconstruction du LCA avec un recul moyen supérieur à 10 ans.Rev Chir Orthop 1997;83(Suppl 2):14.
[25] Setton LA, Mow VC, Müller FJ, Pita JC, Howell DS. Mechanicalproperties of articular cartilage are significantly altered followingtransection of the anterior cruciate ligament. J Orthop Res1994;12:451–63.
[26] Shelbourne KD, Klootwyk TE,Wilckens JH, DE Carlos MS. Ligamentstability two to six years after anterior cruciate ligament reconstructionwith autogenous patellar tendon graft and participation in acceleraterehabilitation program. Am J Sports Med 1995;23:575–9.








![ACL Repair Surgical Considerations · 2020-05-28 · Currently, ACL reconstruction is the gold-standard surgi-cal technique for ACL injury [2]. Reconstruction can be performed by](https://img.dokumen.tips/doc/110x75/5fa24ffede223e23942088ce/acl-repair-surgical-considerations-2020-05-28-currently-acl-reconstruction-is.jpg)