Embed Size (px)
Citation preview

JANUARY 2015 | CATARACT & REFRACTIVE SURGERY TODAY EUROPE 51
COV
ER FOCU
S
We are fortunate to have a broad range of IOL options in Europe, including many types of presbyopia-correcting IOLs. In this somewhat crowded field, properly eval-uating new lenses and decid-ing which one is best suited
for an individual patient can be challenging.With few exceptions, today’s manufacturers produce IOLs
from high-quality materials that allow the creation of edge designs that protect against epithelial cell migration. Some design features have become so broadly available that they no longer play a crucial role in our decision-making, like the 360° square-edge design of most posterior chamber IOLs. Haptic design, however, remains an important criterion for toric IOLs because of the haptics’ role in rotational stability.
ADOPTING PRESBYOPIA-CORRECTING IOLs
We have a preference for premium lenses (eg, multifocal, trifocal, toric) based on IOL platforms that are known to us already. If the basic lens model performs well, then the pre-mium model will also usually perform well. Beyond this, we look primarily at two factors in deciding whether to adopt a new presbyopia-correcting IOL: optical quality param-
eters and performance of the IOL at various distances and lighting conditions.
Optical quality parameters. At our center in Heidelberg, Germany, we have access to optical bench testing equipment. Using validated eye models, optical bench testing can predict the optical performance or sharpness of images viewed through an IOL at any distance, from a few centimeters to optical infinity, at different pupil sizes. The better the initial optical performance of an IOL, the more degradation of image quality a patient can tolerate before needing spectacles. An IOL with high-quality vision will also perform better across a wider range of defocus and may be more forgiving of mild residual refractive error or decentration. For example, the higher the modulation transfer function (MTF) value, the more contrast is transferred to the image, resulting in greater contrast sensitivity.
Optical bench testing also helps to characterize the optical aber-rations inherent to any lens material, which affect the quality and range of vision that is possible with an IOL made from that mate-rial. For example, we are realizing the importance of chromatic aberration (CA), which occurs when individual wavelengths of light are out of focus, causing blur and reduced contrast sensitiv-ity. The average eye has approximately 2.00 D of longitudinal CA between 400 and 700 nm and 0.80 D between 500 and 640 nm.1 Achromatic IOL technology (ie, materials with a high Abbe num-ber) can correct longitudinal CA and, especially when combined
In a crowded market, evaluating a lens’ optical and clinical performance and matching them to patient needs are keys to success.
BY GERD U. AUFFARTH, MD, PhD; AND FLORIAN T.A. KRETZ, MD
THE EVALUATION OF NEW PRESBYOPIA-CORRECTING IOLs
Figure 1. Achromatic IOL technology (right) can correct
longitudinal chromatic aberration.
• Optical quality as measured on an optical bench can predict the performance or sharpness of images produced by a given IOL model.
• This information can be complemented by data on the IOL’s clinical performance at various distances and lighting levels and its ability to meet patients’ visual demands.
• All of these data must be factored together in the selection of an IOL that will best suit the individual patient.
AT A GLANCE

52 CATARACT & REFRACTIVE SURGERY TODAY EUROPE | JANUARY 2015
COV
ER F
OCU
S
with correction of spherical aberration, enhance retinal image quality without negatively affecting depth of focus (Figure 1).2,3
Clinical performance. Data on an IOL’s performance on the optical bench can be complemented by data on that IOL’s clini-cal performance at various distances and lighting levels and its ability to meet a given patient’s visual demands.
We take great care in evaluating patients’ typical reading dis-tances. We seat patients at a computer and ask them to place the monitor where it would be in their home or office, and we have them hold a book or handheld electronic device to mea-sure their reading distance. Through questionnaires and patient history forms, we also determine how much time they spend at different visual distances for work, hobbies, and daily activities.
It is not uncommon today for so-called near vision tasks to be at what we would in the past have considered an intermedi-ate distance. For example, patients may be working on a laptop or using a tablet or smart phone at 60 cm instead of holding a book at 30 to 40 cm. We see this reflected in the growing
popularity of low-add multifocal IOLs, with add powers of 1.50 to 2.75 D instead of the traditional 3.00 to 4.00 D.
We also want to know about halos and glare. In patients who drive at night or have high retinal function, and will therefore be more likely bothered by photic phenomena, choosing a lens with less risk of these side effects may take precedence over all other considerations.
Pupil independence is another important factor to consider in matching the IOL to the patient. Someone who expects spec-tacle independence but works in low lighting conditions, for example, is likely to be dissatisfied with a pupil-dependent IOL.
Pupil independence is a function of optics and lens material, not necessarily lens design. Diffractive multifocal, trifocal, and extended range of vision IOLs can be either pupil-dependent, as with the AcrySof Restor (Alcon) and Hoya’s extended depth of focus IOL (Gemetric), or pupil-independent, as with the Tecnis Multifocal (Abbott Medical Optics) and the AT LISA tri (Carl
The WIOL-CF lens can extend depth of focus.
By Laura Straub, Editor-in-Chief
Developed to resemble the properties of the natural crystal-line lens in size, material, shape, and function, the Wichterle IOL–Continuous Focus (WIOL-CF; Medicem) is among the recent group of extended depth of focus IOLs to hit the market. The company calls its lens a bioanalogic polyfocal IOL, intended for the treatment of cataract and presbyopia in patients who demand supreme visual acuity in the intermediate and distance ranges and who wish to maintain or restore their vision in the near range. The WIOL-CF has a 9-mm optic, is made of a soft hydrogel to enable shape change and accommodation, and has a natural pupillary influence on focus.
The IOL’s shape is created by spin-casting technology, whereby the lens is rotated in the mold; because no mechanical cutting or polishing is used during the manufacturing process, the lens is very smooth. Like the crystalline lens, the surface of the WIOL-CF has a negative charge mediated by carboxylate groups.
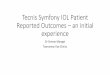
The negative charge and the lens’ smooth surface ensure that the WIOL-CF is resistant to posterior capsular opacification, as the convex hyperbolic surface closely adheres to the posterior capsule (Figure 1).
CLINICAL RESULTSAccording to company literature, long-term results (2–9 years;
average, 5.6 years) from 40 patients implanted with the lens are available. Mean binocular UCVA for near, intermediate, and dis-tance vision was 0.36, 0.12, and 0.01, respectively, and more than 97% of patients scored their social functioning at 99 of 100 and spectacle independence at 98 of 100.1
1. Mazal Z. Long-term results of WIOL-CF intraocular lens implantation. Paper presented at: the Congress of Czech Society of Refractive and Cataract Surgery; May 2014; Ostrava, Czech Republic.
THE FIRST BIOANALOGIC IOL
MEDICEM International GmbH Baarerstrasse 8, 6300 Zug Switzerland
www.wiols.com www.medicem.com
Negative charge and smooth surface makes WIOL–CF® resistant to opacifi cation caused byadsorption of proteins and creation of biofi lm that is often followed by adhesion and proliferation of fi broblasts. The cells cannot attach and grow on the negatively charged and smooth surface. The smooth and convex hyperbolic surface of WIOL–CF® closely adheres to the posterior capsule and does not allow penetration of cells behind the lens.
Comparison of the biological activity on the various types of surface
STABILITY AND LONG-TERMRELIABILITYTransparency, elasticity, water per-meability, shape memory and othercharacteristics of the WIOL–CF®
material are durable and its functionis very stable. It o ers users long-termand consistent function.
Transparency of implanted WIOL–CF�® measuredby Scheimpfl ug camera (up to 7 years afterimplantation)
WIOL–CF�® fi lls the posterior partof the capsule and closely adheres to it
Tissue culture dish
WIOL–CF® achieves its results through a unique design and material developed to resembleproperties of the natural crystalline lens. Implantation of WIOL–CF® restores many of the chara-cteristics of the young natural crystalline lens in terms of its optics, function and position in the eye. It provides the retina and brain with comprehensive and understandable visual information.WIOL–CF® represents a leading technology for the treatment of cataract and presbyopiafor patients, who demand more than visual acuities on predefi ned distances.
01234567
0 1 2 3 4 5 6 7 8
Time from surgery (years)
Op
acit
y (%
)
Reference:Stoy VA, et al. ASCRS–ASOA, San Francisco, 2006
® resistant to opacifi cation caused byadsorption of proteins and creation of biofi lm that is often followed by adhesion and proliferation of fi broblasts. The cells cannot attach and grow on the negatively charged and smooth surface.
Commercial hydrophilic acrylate with 25�% hydration, posterior surface of IOL
Surface of WIOL–CF®.Seeded fi broblasts do not profi lerate or adhere, remain isolated and it is easy to wash them from the surface of the lens.
Figure 1. The WIOL-CF is resistant to posterior capsular
opacification and adheres closely to the posterior capsule.
Cour
tesy
of M
edice
m
SPIN-CASTING TECHNOLOGYInstead of lathe-cutting and polishing or cast molding, the WIOL-CF IOL is manufactured using spin-casting technology.
(Continued on page 55)

JANUARY 2015 | CATARACT & REFRACTIVE SURGERY TODAY EUROPE 53
COV
ER FOCU
S
The IC-8 IOL can improve near and intermediate vision without sacrificing distance vision.
By Robert Edward Ang, MD
As a researcher, I am fascinated by new technol-ogy and have focused my interest on presbyopia treatments through participation in studies of corneal inlays; accommodating, multifocal, and extended depth of focus IOLs; and cornea-based procedures. Based upon the success of the small-aperture concept demonstrated by the Kamra corneal inlay (AcuFocus), I was interested in the
potential to expand the concept and technology to my cataract patients.
MINIMIZED COMPROMISEI have tried many presbyopia treatments and have learned that
there is always something to gain by presbyopia correction—but not without some sacrifice. The most common complaint of patients, especially those with multifocal IOLs, is photic phenom-ena, including glare and halos. On the other hand, the most often reported downside of accommodating and extended depth of focus technologies is inadequate near vision. The IC-8 small-aperture IOL (AcuFocus; Figure 1), a one-piece hydrophobic acrylic lens, seems to minimize these shortcomings and provide adequate near vision.
To date, I have implanted the IC-8 in the nondominant eye in nine patients with cataracts following standard phacoemulsifica-tion.1 At 1-year postoperative, mean near UCVA in these patients is J2, and mean intermediate and distance UCVAs are each 20/20.1 I asked patients to compare their pre- and postoperative vision and rate symptoms such as fluctuating vision, distortion, glare, halos, night vision, and overlapping images; all of their responses indicated minimal side effects. I also asked patients to compare these factors with their untreated eye, and all reported similar or better results in the IC-8 eye than in the fellow eye.
A retina specialist and four technicians of varying experi-ence levels assessed the ease of performing visual field, fundus photography, and retinal OCT examinations with the IC-8 in place. All reported that they were able to complete the diag-nostic testing successfully with only minor adaptations.
AN EYE TOWARD THE FUTUREThe small-aperture principle seems to work regardless of the pres-ence of corneal irregularity. The IC-8 lens provides an alternative in situations in which I am hesitant to use a multifocal IOL. Having technology with the ability to improve near and intermediate vision without sacrificing distance vision is exciting, and, in time, I expect the indications to grow.
1. Ang R. Visual and optical performance with a small-aperture intraocular lens: first report. Paper presented at: the
XXXII Congress of the ESCRS; London; September 13-17, 2014.
SMALL-APERTURE TECHNOLOGY FOR THE CATARACT PATIENT
STUDY RESULTS • In nine patients implanted with the IC-8
IOL, mean near UCVA was J2 and mean intermediate and distance UCVAs were 20/20 at 1-year postoperative.
• With the IOL implanted, diagnostic testing was completed successfully with only minor adaptations.
Figure 1. Eye implanted with an IC-8 small aperture IOL.
Robert Edward Ang, MDn Senior Refractive Surgeon, Asian Eye Institute, Philippinesn [email protected] Financial disclosure: Clinical investigator (AcuFocus)

54 CATARACT & REFRACTIVE SURGERY TODAY EUROPE | JANUARY 2015
COV
ER F
OCU
S
The RevIOL Tri-ED lens provides continuous depth of vision.
By Pavel Stodulka, MD, PhD
I am keen on searching for new and progressive ophthalmic technologies and am known to be an early adopter of many innovations, including trifocal IOLs and laser-assisted cataract surgery.
Because adding the FineVision trifocal IOL (PhysIOL) to our armamentarium revolu-tionized our refractive practice, I have been sure to keep a close eye on other new trifo-cal IOL designs.
ACTIVE-DIFFRACTIVE OPTICI have had positive experiences with
VSY’s other products, and, therefore, when the company announced its entrance into the trifocal IOL market with the RevIOL Tri-ED (Figure 1), I was happy to give it a try. It is a plate-haptic hydrophilic acrylic IOL with a hydrophobic surface and a trifocal
diffractive structure on its anterior surface. The combination of an active-diffractive optic structure with proprietary curvature and slightly negative asphericity results in extended depth of focus for presbyopic patients (Figure 2). According to the com-pany, the diffractive zone design creates higher modular transfer function values between the near to intermediate and inter-mediate to distance focusing areas com-pared with monofocal, bifocal, and other tri-focal IOLs and clearer vision at all distances.1 The active-diffractive optic also protects the retina by blocking pale blue light.
Because we do not yet have a true accommodating IOL, I like VSY’s idea of developing the trifocal concept further. The selected disparity between near and intermediate focus (3.00 D of add for near and 1.50 D for intermediate) seems to work effectively to create sharp vision at all distances.
We are currently assessing the defocus curve and clinical results with the RevIOL Tri-ED. Initial results with this lens seem promising, and my patients have been enjoying spectacle independence in their usual daily activities. I expect more new tri-focal IOLs will enter the market soon.
1. Data on file with VSY.
EXTENDED DEPTH OF FOCUS IN A TRIFOCAL IOL
IOL DESIGN • The RevIOL Tri-ED is a plate-haptic hydrophilic acrylic IOL
with a trifocal diffractive structure on its anterior surface.
• The IOL provides a near add of 3.00 D and an intermediate add of 1.50 D.
Figure 1. Features of the RevIOL Tri-ED.
Figure 2. The RevIOL Tri-ED’s active-diffractive optic results in extended depth of focus.
Imag
es co
urte
sy of
VSY
Pavel Stodulka, MD, PhDn Chief Eye Surgeon, CEO of Gemini Eye
Clinics, Czech Republicn [email protected] Financial disclosure: None

JANUARY 2015 | CATARACT & REFRACTIVE SURGERY TODAY EUROPE 55
COV
ER FOCU
S
Zeiss Meditec) IOLs. Some pupil-dependent lenses reduce glare and halos, which is a positive charac-teristic for sharp distance vision at night; however, the tradeoff is that these lenses sacrifice near acu-ity in dim light.
All of these issues must be factored into the selection of an IOL that will best suit the patient. A pupil-dependent IOL that provides crisp dis-tance vision and minimal night vision disturbances may be a good choice for a nighttime taxi driver but not for a mechanical engineer who wants to be spectacle-free while working in a poorly illumi-nated facility.
PUTTING IT ALL TOGETHERWe recently had the opportunity to evaluate
the Tecnis Symfony IOL (Abbott Medical Optics; Figure 2), the first lens to rely on an echelette design for an elongated depth of focus, resulting in an extended range of vision. In essence, instead of splitting light into two or three focal points, the IOL spreads the focal point wider, so that there
is a clear image over a range of vision. Defocus curves for this IOL depict an extended range rather than distance and near peaks; however, the tradeoff is some loss of acuity in the very near range. (Editor’s Note: Several other IOL technologies dedicated to extending depth of focus are described in detail in the accompanying sidebars.)
Current studies have shown a clinically signifi-cant increase in range of vision with the Tecnis Symfony compared with the Tecnis monofocal (ZCB00). A sustained mean BCVA of 20/20 or bet-ter was reported through 1.50 D of defocus with the Symfony, with a 1.00 D increase in the range of vision throughout the defocus curve.4
The optic material of this lens corrects for both spherical and chromatic aberration, correcting for at least 0.75 D of lateral CA compared with the phakic eye and providing a high-quality retinal image. Like the other IOLs on the Tecnis platform, the Symfony is pupil-independent, with little deg-radation of near and intermediate acuity in dim
The Symfony IOL provides sharp vision from distance to near.
By Aylin Kiliç, MD
Today’s patients expect almost perfect vision after cataract surgery. They want to see near without glasses, and they desire comfortable vision with-out any complications such as halos and glare.
Because the Symfony IOL (Abbott Medical Optics) is pupil independent, quality of vision does not change as the pupil expands in dark conditions. For those who drive at night or
enjoy hobbies typically done in poor light, pupil independence is important.
Although multifocal IOLs continue to undergo modifications to enhance distance and near vision, unwanted side effects are still problematic. The Symfony IOL does not cause any distur-bance in distance vision and can compensate for chromatic aber-rations between the shorter blue and longer red wavelengths. This is because the lens does not have multiple focal points, as other multifocal IOLs do. When light approaches an echellette grating surface, as on the Symfony’s optic, it is diffracted into spe-cific directions that vary according to step height and area. The design of the Symfony, therefore, provides an extended range of vision to the patient without producing glare and halos.
In my limited experience with the IOL, which includes four eyes to date, distance BCVA always remains unchanged or improved after surgery. At the final follow-up visits, distance visual acuity is 20/20 or better in the majority of eyes. Additionally, there have been no significant complaints of visual disturbances.
Unlike multifocal IOLs that create a fixed number of focal points, the Symphony has provided my patients with continuous sharp vision from distance to near. The lens has provided improved con-trast sensitivity and sharper distance vision compared with other pupil-dependent multifocal IOLs that I have used. I plan to analyze a larger series of patients with longer follow-up.
HIGH PATIENT SATISFACTION
NO DISTURBANCES • The Symfony IOL can compensate for
chromatic aberrations between the shorter blue and longer red wavelengths.
Aylin Kiliç, MDn Dunya Eye Hospital, Turkeyn [email protected] Financial disclosure: None
Figure 2. The echelette
design of the Tecnis Symfony
provides an elongated depth
of focus, resulting in an
extended range of vision.
(Continued from page 52)
(Continued on page 59)

JANUARY 2015 | CATARACT & REFRACTIVE SURGERY TODAY EUROPE 59
COV
ER FOCU
S
light. The echelette design reduces the incidence of glare and halos to monofocal IOL levels.5
CONCLUSIONIn our practice, the Tecnis Symfony lens will likely be a good
choice for patients who want excellent UCVA for distance and intermediate-near tasks and those with high retinal function or night driving demands who would be bothered by glare and halos. Patients who do not need good vision in dim light, have heavy true near visual demands, and do not want to wear read-ing glasses even for fine print might be better served by a multi-focal IOL. With the availability of more presbyopic IOL designs, surgeons should be aware of the performance characteristics of different lens features in order to truly customize lens selection for each patient. n
1. Nagata T, Kubota S, Watanabe I, Aoshima S. Chromatic aberration in pseudophakic eyes. Nihon Ganka Gakkai Zasshi. 1999;103(3):237-242.2. Weeber HA, Piers PA. Theoretical performance of intraocular lenses correcting both spherical and chromatic aberration. J Refract Surg. 2012;28(1):48-52.3. Artal P, Manzanera S, Piers P, Weeber H. Visual effect of the combined correction of spherical and longitudinal chromatic aberra-tions. Opt Express. 2010;18(2):1637-1648.4. 166, Data on File. Extended Range of Vision IOL 3-Month Study Results (NZ).5. Auffarth GU. Clinical experience with an extended range of vision 1-Piece IOL. Paper presented at: the XXXII Congress of the ESCRS; September 13-17, 2014; London.
Gerd U. Auffarth, MD, PhDn Chairman of the Department of Ophthalmology, University of
Heidelberg, Germanyn Director of the International Vision Correction Research
Center & David J. Apple Laboratory for Ocular Pathology, Heidelberg, Germany
n [email protected] Financial disclosure: Consultant, Travel grants and lecture fees
(Abbott Medical Optics)
Florian T.A. Kretz, MDn Senior Research Specialist, International Vision Correction
Research Center & David J. Apple Laboratory for Ocular Pathology, Heidelberg, Germany
n [email protected] Financial disclosure: Consultant, Travel grants and lecture fees
(Abbott Medical Optics)
Professor Auffarth discusses his experience with the Symfony IOL.
WATCH IT NOW
(Continued from page 55)