Embed Size (px)
Citation preview

The Epidemiology andEtiology of PerthesDisease
Daniel C. Perry, MB ChB(Hons), MRCS (Eng)a,*,Andrew J. Hall, MB BS, MSc, PhD, FRCP, FFPH, FMedScibKEYWORDS
� Epidemiology � Etiology � Perthes � Geography � Incidence
Perthes disease occurs in around 5 boys for everyaffected girl. The disease affects children between2 and 14 years old with the peak age of onset,among white children, being 5 years old. The ageof onset has been demonstrated to be later amongIndian children.1 Approximately 15% of cases arebilateral.
GEOGRAPHY
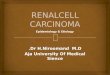
There is a marked geographic variation in thefrequency of Perthes disease. Studies of incidenceare difficult to directly compare, as inappropriatepopulation denominators have sometimes beenused. Table 1 shows those studies where theannual incidence rates have been calculated usinga denominator of 0- to 14-year-old child years.
There is a significant geographic variation indisease incidence between countries, within coun-tries, and even between small local areas. Equato-rial regions have a low incidence of disease whileNorthern Europe has the highest documented inci-dence. This divergence may at least partly be ex-plained by race, because evidence from theEastern Cape of South Africa shows that blackAfrican children living alongside African whiteshave a substantially lower disease incidence, andpeople of mixed race an intermediate level (black:0.45; mixed race: 1.7; white: 10.8 per 100,000 chil-dren 0–14 years old).5 Investigators from predom-inantly white countries, with significant blackpopulations, have similarly identified few cases of
The authors have nothing to disclose.a Department of Child Health, University of Liverpool, Lb Department of Infectious Disease Epidemiology, LondoStreet, London, WC1E 7HT, UK* Corresponding author.E-mail address: [email protected]
Orthop Clin N Am 42 (2011) 279–283doi:10.1016/j.ocl.2011.03.0020030-5898/11/$ – see front matter � 2011 Elsevier Inc. All
Perthes disease among black children, NewYork, USA: 14 black children among 358 Perthesdisease cases15; Connecticut, USA: 2 black chil-dren among 203 cases19; Massachusetts, USA: 1black child amongst 86 cases.2 Population studiesfrom Asian countries have found an incidencebetween that of black and white individuals, withincidence rates of 0.93 per 100,000 children 0 to14 years old from a population study of Japan,13
and 3.85 per 100,000 children 0 to 14 years oldin Korea (see Table 1).11
There is data to show regional disease distribu-tions within three countries, namely England, India,and Norway. All show a variation in incidence of atleast twofold. In England the southern region ofWessex had half the incidence of Merseyside inthe North West, with Trent in the Midlands havingan intermediate value (11.1 vs 7.6 vs 5.5 casesper 100,000 children 0–14 years old per annum).4
In India, incidence in Vellore (south-east) was0.4 per 100,000 per annum for 0- to 14-year-oldswhereas in Manipal (south-west) it was 4.4.1 InNorway, an incidence of 3.6 in Northern Finmarkcounty contrasted with 16.7 per 100,000 perannum in Western Sogn og Fjordane.14
Incidence even varies notably within small areas.This divergence was first demonstrated withinMerseyside (United Kingdom), with a very highincidence in inner-city Liverpool prompting in-vestigators to examine the relationship betweendeprivation and disease.6,10 A steep social classgradient of disease from 4 per 100,000 per annum
iverpool, L12 2AP, UKn School of Hygiene and Tropical Medicine, Keppel
rights reserved. orthopedic.th
eclinics.com
Table 1Annual incidence of Perthes disease in children aged 0 to 14 years by country and region
Year Study Location
Annual Incidence Figuresper 100,000 Population(0–14 y old)
Males Females Overall
1966 Molloy and MacMahon2 Massachusetts, USA — — 5.7
1972 Gray et al3 British Columbia, Canada 8.4 1.6 5.1
1978 Barker et al4 Wessex, UK 8.7 2.0 5.5
1978 Barker et al4 Merseyside, UK 16.9 5.0 11.1
1978 Barker et al4 Trent, UK 12.0 3.0 7.6
1982 Purry5 Eastern Cape, South Africa (Blacks) — — 0.5
1982 Purry5 Eastern Cape, South Africa (Mixed race) — — 1.7
1982 Purry5 Eastern Cape, South Africa (Whites) — — 10.8
1983 Hall et al6 Liverpool, UK 25.8 4.9 15.6
1988 Joseph et al1 Vellore, Eastern India — — 0.4
1988 Joseph et al1 Udupi, Western India — — 4.4
1989 Hall and Barker7 Yorkshire, UK — — 6.1
1992 Moberg and Rehnberg8 Uppsala, Sweden 8.5 2.1 6.3
2000 Kealey et al9 Northern Ireland — — 11.6
2001 Margetts et al10 Liverpool, UK — — 8.7
2005 Rowe et al11 Korea 6.1 1.5 3.8
2005 Pillai et al12 Southwest Scotland — — 15.4
2006 Kim et al13 Japan 1.5 0.2 0.9
2006 Wiig et al14 Norway — — 9.2
Perry & Hall280
in Social Class 1 (highest social standing) to31.7 per 100,000 per annum in Social Class5 (lowest social standing)was found.6 Similar socialclass and deprivation trends have now beenreported by several other studies,12,16 althoughthis association is not universally demonstrated.17
TIME TRENDS
Few studies have sought to measure the influenceof time on disease incidence. Between 1924 and1960, Peic18 reviewed outpatient data from anorthopedic clinic in Dortmund, Germany. He notedthat the incidence of cases tended to increase 5years after a period of economic recession.However, his method of case ascertainment anddefinition of source population raises doubts asto the robustness of this association. A Scottishstudy similarly noted an association between“gross value added” (a measure of regional wealth)and the incidence of Perthes disease, though theperiod of observation was just 10 years and casenumbers were small.12 The only area to recordtrends in disease incidence over a prolongedperiod is Merseyside.6,10 The disease incidencehas been measured from 1976, with the last
published data considering the period up to1995. The incidence within Liverpool was foundto have halved between the 1976 and 1995, withrates falling from 16.9 to 8.7 cases per 100,000per annum. This time period was associated witha progressive increase in the standard of livingwithin the city, which may account for the declinein incidence.The pattern of variation in incidence by social
class, over small geographic areas, and with timeall indicate a major environmental influence in thecause of the disease. This influence appears toact early in childhood or in prenatal life. Familystudies show that in large case series diseaseoccurs in approximately 0.5% to 0.8% of theparents and 2% to 4% of siblings of affectedchildren.3,19,20 Twin pairs within such case serieshave identified 10 dizygous pairs and 5 monozy-gous pairs, each with a single concordantpair.19,21–23 Given this low concordance in twins,it seems likely that familial aggregation is attribut-able to a shared environment rather than a geneticsusceptibility.Analysis of the age distribution of onset of cases
shows that it conforms toa log-normaldistribution.24
This pattern is typical of incubation periods and is

Epidemiology and Etiology of Perthes Disease 281
consistent with a single exposure acting at a criticalperiod in the hip development, either prenatally or inthe first 2 years of life.
ASSOCIATIONSStature
The most detailed observation of growth inPerthes disease was published in 1978.25 Thislarge, cross-sectional, anthropometric study in-volved 232 children with Perthes disease from 3centers in the United Kingdom. A control groupwas drawn from primary schools in 2 of the3 regions. The results demonstrated a subtleglobal growth disturbance in affected individualswith the demonstration of a normal head size, yetincreasing growth restriction as one progresseddistally along limb units, such that the hands andfeet were most disproportionate compared withhead size: a pattern of dysmorphism describedas “rostral sparing” (Fig. 1). Given the strongsocioeconomic gradient of Perthes disease, itwas however unclear whether this growth abnor-mality was a function of urban deprivation ora true disease-related phenomenon. A furtherstudy therefore sought to compare anthropometryin siblings of affected children matching for urbandeprivation as well as other familial factors.26 Thisstudy of 38 cases and 49 sibling controls demon-strated a clear growth restriction most notable inthe feet of affected children (see Fig. 1).
This association with abnormal growth and thepossibility of an intrauterine cause raises the ques-tion of whether there is an association with shapeand size at birth of the affected children.
Birth Proportions
Birth weight has been studied in several settings,but no association with Perthes disease hasbeen consistently found.14,23,27 The study of birthweight is problematic given the potential
Fig. 1. Pattern of abnormal growth in Perthes disease.(Modified from Burwell R, Dangerfield P, Hall D, et al.Perthes’ disease. An anthropometric study revealingimpaired and disproportionate growth. J Bone JointSurg Br 1978;60(4):464; with permission.)
confounding variables including socioeconomicstatus, parity, and parental smoking. Thus a recentSwedish study by Bahmanyar and colleagues28
considered smoking, gestational age, and birthweight simultaneously, concluding that an associ-ation exists between birth weight of less than1500 g and Perthes disease (odds ratio [OR]3.46, 95% confidence interval [CI] 1.11–10.84).The wide confidence intervals indicate the smallnumber of cases falling within this group (9 of731 cases). It is possible that this associationresulted from avascular necrosis precipitated bysteroid use for neonatal chronic lung diseaserather than true Perthes disease.
A Norwegian birth registry study is the first toshow an association with birth length.14 The riskof Perthes disease was increased by 50% in thoseunder 50 cm at birth compared with those over50 cm. Although little account of confoundingwas made, in particular of socioeconomic status,this is the first study to examine, and find, thatthe growth abnormality was present at birth.
Congenital Malformations
One influence of an intrauterine exposure might beon congenital malformations. Catterall and col-leagues29 originally demonstrated an associationbetween Perthes disease and inguinal hernias andgenitourinary malformations, with the frequency ofan inguinal hernia being 8 times the expectednumber.Other series have failed to replicate genito-urinary associations,19,21 but recently the associa-tion with undescended testicles was found usingtheMedical Birth Registry of Norway.14 Other asso-ciations suchas inguinal herniascouldnotbeexam-ined, as such details are not recorded in this birthregister, but a strong association with Downsyndrome was found. A case-control study in Not-tingham (United Kingdom) of minor congenital ab-normalities using standardized criteria and a singleobserver found a marked increase in Perthes-affected children, with nearly half exhibiting one ofthe abnormalities versus 23% of controls.30
HYPOTHESES
The clear association with growth and the potentialfor an intrauterine effect have led to two specifichypotheses: nutritional deficiency and parentalsmoking.
Manganese deficiency has so far been investi-gated because of the known consequences ofgrowth abnormalities in chickens, and epiphysealdysplasia in rats. An initial case-control studyamongst children with Perthes disease found anassociation,31 but this was not confirmed in a

Perry & Hall282
second smaller study nor by supplementation afterdisease onset.32
Maternal smoking is a known cause of impairedgrowth in the fetus. Several studies have attemptedto examine apotential relationship, but the only oneto do this adequately was based on the Swedishinpatient register. A large case-control study of852 cases and 4432 controls using linkage to themother’s maternal records concluded that therewas a significantly increased risk of Perthes dis-ease with maternal or paternal smoking, witha dose-related effect on risk (adjusted OR 1.4 for<10 cigarettes/day, and OR 2.0 for >10 ciga-rettes/day).28 The investigators considered socio-economic status as a confounder, although it isunclear how this was measured.Neither of these hypotheses have been satisfac-
torily resolved one way or the other. The difficultyis that good data and biologic samples are neededfrom the mother when she is pregnant (for cotinineor trace metal measurements), but the disease isinsufficiently common to allow this to be donewithin existing birth cohorts.Two other hypotheses relate to postulated later-
stage events in the disease pathogenesis. One ishyperactive behavior as a cause of increasedtrauma to the growing hip, and the second isa coagulation abnormality leading to the vascularocclusion.Several investigators have commented on
behavior abnormalities in their patientswith Perthesdisease. One study has documented this usingstandardized validated questionnaires.33 In a seriesof 24 children with the disease, 8 had a behaviouralprofile within the spectrum of the attention deficithyperactivity disorder (ADHD). However, therewere no controls, and this rate was merelycompared to the expected population ADHD prev-alence of 3% to 5%.Thrombophilic tendencies have been the
subject of a series of studies over the last 15years, and these have been systematically re-viewed. A total of 475 Perthes cases wereincluded in the review by Kenet and colleagues,34
who concluded that there were no significantdifferences in antithrombin activity, protein S orC activity, or antiphospholipid antibodies. Thereview was equivocal over a possible relationshipbetween Perthes disease and the Factor V Leidenmutation, requiring more cases to define the truerelationship. The one study since this reviewincluded 169 cases of Perthes disease and 512controls.35 This study demonstrated several asso-ciations including a propensity toward Factor VLeiden mutations (OR 3.3; 95% CI 1.6–6.7) anda raised Factor VIII level (OR 7.5; 95% CI 2.2–25.2). However, this study was so flawed in design
and analysis that it adds nothing to the earlierreview.In terms of these hypotheses, therefore,
behavior has not yet been adequately tested andthe studies of coagulopathy appear to excludeany major association.
SUMMARY
Perthes disease, despite a century of research,remains of unknown etiology. However, anyhypothesis must fit into the clear epidemiologicframework that we have. The disease is associ-ated with deprived populations, and is muchmore common in white children than in Asians orAfricans. It is associated with a global growthdisorder characterized by delayed and dispropor-tionate growth. The causal insult appears to occurvery early in a child’s life, with early changes inskeletal development probably evident at birth.The association with congenital malformations isconsistent with this timing. Regarding the inci-dence of Perthes disease, the strong gradient insocial class and the variation in the factors geog-raphy and time confirm that the major cause isenvironmental and not genetic.Future research is therefore needed to expand
our knowledge of descriptive epidemiology;further work on changes in incidence over timewould be particularly valuable. Studies are neededto examine the specific hypotheses related toparental smoking, nutritional deficiency in preg-nancy, and behavior. However, most urgent aresome new hypotheses and adequately designedstudies to address them.
REFERENCES
1. Joseph B, Chacko V, Rao BS, et al. The epidemi-
ology of Perthes’ disease in south India. Int J Epide-
miol 1988;17(3):603–7.
2. Molloy MK, MacMahon B. Incidence of Legg-
Perthes disease (osteochondritis deformans).
N Engl J Med 1966;275(18):988–90.
3. Gray IM, Lowry RB, Renwick DH. Incidence and
genetics of Legg-Perthes disease (osteochondritis
deformans) in British Columbia: evidence of polygenic
determination. J Med Genet 1972;9(2):197–202.
4. Barker DJ, Dixon E, Taylor JF. Perthes’ disease of the
hip in three regions of England. J Bone Joint Surg Br
1978;60(4):478–80.
5. Purry NA. The incidence of Perthes’ disease in three
population groups in the Eastern Cape region of
South Africa. J Bone Joint Surg Br 1982;64(3):286–8.
6. Hall AJ, Barker DJ, Dangerfield PH, et al. Perthes’
disease of the hip in Liverpool. Br Med J (Clin Res
Ed) 1983;287(6407):1757–9.

Epidemiology and Etiology of Perthes Disease 283
7. Hall AJ, Barker DJ. Perthes’ disease in Yorkshire.
J Bone Joint Surg Br 1989;71(2):229–33.
8. Moberg A, Rehnberg L. Incidence of Perthes’
disease in Uppsala, Sweden. Acta Orthop Scand
1992;63(2):157–8.
9. Kealey WD, Moore AJ, Cook S, et al. Deprivation,
urbanisation and Perthes’ disease in Northern
Ireland. J Bone Joint Surg Br 2000;82(2):167–71.
10. Margetts BM, Perry CA, Taylor JF, et al. The inci-
dence and distribution of Legg-Calve-Perthes’
disease in Liverpool, 1982–95. Arch Dis Child
2001;84(4):351–4.
11. Rowe SM, Jung ST, Lee KB, et al. The incidence of
Perthes’ disease in Korea: a focus on differences
among races. J Bone Joint Surg Br 2005;87(12):
1666–8.
12. Pillai A, Atiya S, Costigan PS. The incidence of
Perthes’ disease in Southwest Scotland. J Bone
Joint Surg Br 2005;87(11):1531–5.
13. Kim W, Hiroshima K, Imaeda T. Multicenter study for
Legg-Calve-Perthes disease in Japan. J Orthop Sci
2006;11(4):333–41.
14. Wiig O, Terjesen T, Svenningsen S, et al. The epide-
miology and aetiology of Perthes’ disease in Norway.
A nationwide study of 425 patients. J Bone Joint
Surg Br 2006;88(9):1217–23.
15. Katz JF. Legg-Calve-Perthes disease: a statistical
evaluation of 358 cases. Mt Sinai J Med 1973;
40(1):20–47.
16. Hall AJ, Barker DJ, Lawton D. The social origins of
Perthes’ disease of the hip. Paediatr Perinat Epide-
miol 1990;4(1):64–70.
17. Sharma S, Sibinski M, Sherlock DA. A profile of
Perthes’ disease in Greater Glasgow: is there an
association with deprivation? J Bone Joint Surg Br
2005;87(11):1536–40.
18. Peic S. Contribution to Perthes’ disease. Z Orthop
Ihre Grenzgeb 1962;96:276–82.
19. Fisher RL. An epidemiological study of Legg-Perthes
disease. J Bone Joint Surg Am 1972;54(4):769–78.
20. Wansbrough R, Carrie A, Walker N, et al. Coxa pla-
na, its genetic aspects and results of treatment with
the Long Taylor Walking Caliper: a long-term follow-
up study. J Bone Joint Surg Am 1959;41(1):135.
21. Harper PS, Brotherton BJ, Cochlin D. Genetic risks
in Perthes’ disease. Clin Genet 1976;10(3):178–82.
22. Lappin K, Kealey D, Cosgrove A, et al. Does low
birthweight predispose to Perthes’ disease?
Perthes’ disease in twins. J Pediatr Orthop B 2003;
12(5):307–10.
23. Wynne-Davies R, Gormley J. The aetiology of
Perthes’ disease. Genetic, epidemiological and
growth factors in 310 Edinburgh and Glasgow
patients. J Bone Joint Surg Br 1978;60(1):6–14.
24. Hall AJ, Barker DJ. The age distribution of Legg-
Perthes disease. An analysis using Sartwell’s incu-
bation period model. Am J Epidemiol 1984;120(4):
531–6.
25. Burwell R, Dangerfield P, Hall D, et al. Perthes’
disease. An anthropometric study revealing
impaired and disproportionate growth. J Bone Joint
Surg Br 1978;60:461–77.
26. Hall AJ, Barker DJ, Dangerfield PH, et al. Small feet
and Perthes’ disease. A survey in Liverpool. J Bone
Joint Surg Br 1988;70(4):611–3.
27. Molloy MK, Macmahon B. Birth weight and Legg-
Perthes disease. J Bone Joint Surg Am 1967;49(3):
498–506.
28. Bahmanyar S, Montgomery SM, Weiss RJ, et al.
Maternal smoking during pregnancy, other
prenatal and perinatal factors, and the risk of
Legg-Calve-Perthes disease. Pediatrics 2008;
122(2):e459–64.
29. Catterall A, Lloyd-Roberts G, Wynne-Davies R.
Association of Perthes’ disease with congenital
anomalies of genitourinary tract and inguinal region.
Lancet 1971;297(7707):996–7.
30. Hall DJ, Harrison MH, Burwell RG. Congenital abnor-
malities and Perthes’ disease. Clinical evidence that
children with Perthes’ disease may have a major
congenital defect. J Bone Joint Surg Br 1979;
61(1):18–25.
31. Hall AJ, Margetts BM, Barker DJP, et al. Low
blood manganese levels in Liverpool children
with Perthes’ disease. Paediatr Perinat Epidemiol
1989;3(2):131–5.
32. Perry CA, Taylor JF, Nunn A, et al. Perthes disease
and blood manganese levels. Arch Dis Child 2000;
82(5):428.
33. Loder RT, Schwartz EM, Hensinger RN. Behav-
ioral characteristics of children with Legg-Calve-
Perthes disease. J Pediatr Orthop 1993;13(5):
598–601.
34. Kenet G, Ezra E, Wientroub S, et al. Perthes’ disease
and the search for genetic associations: collagen
mutations, Gaucher’s disease and thrombophilia.
J Bone Joint Surg B 2008;90:1507–11.
35. Vosmaer A, Pereira RR, Koenderman JS, et al.
Coagulation abnormalities in Legg-Calve-Perthes
disease. J Bone Joint Surg Am 2010;92(1):121–8.