Embed Size (px)
Citation preview

The Enema Continence Catheter in Spina Bifida: Successful Bowel Management
By B. Shandling and R.F. Gilmour
Toronto, Canada
�9 Patients with spina bifida who have fecal incontinence are managed by means of a large-volume saline enema. To facilitate administration of the enema, a special catheter has been devised that prevents leakage of the enema fluid. Continence has been achieved in 112 children and youths with spina bifida who were managed in this fashion. �9 1987 by Grune & Stratton. Inc.
INDEX WORDS: Spina bifida; fecal incontinence; neuro- genic bowel.
I NDIVIDUALS with spina bifida, and, in the case of children, their parents, face a multiplicity of prob-
lems. One of the most unpleasant is that of fecal incontinence. The very existence of this handicap is rarely spoken about, and its management is frequently left to untrained individuals. 1"2
At the Hugh MacMillan Medical Centre in Toron- to, we developed a system of management for coping with fecal incontinence, and to facilitate this, we devised a special enema continence catheter (ECC; Cardiomed Supplies, Gormley, Ontario).
MATERIALS AND METHODS
If parents are managing the problems of the child's fecal inconti- nence successfully enough to render them reluctant to change, we do not suggest a radical change in the management. However, if parents are unaccepting of the fecal incontinence and wish to attempt to make the child more socially acceptable, we recommend an enema regimen. Lukewarm tap water, to which 1 teaspoon of kitchen salt per 500 mL is added, is run into the colon in the amount of 20 mL/kg. In order to prevent instant leakage of the enema solution from the incontinent anus because of absent sphincter control, we first insert the inflatable end of the ECC. The balloon is inflated and (often with the patient sitting upright on the toilet) the fluid is rapidly run in. When the total volume has been administered, the balloon is deflated, the ECC removed, and the liquid contents of the colon are immediately expressed by kneading the abdomen in an isoperistaltic direction, following the course of the colon.
It is best to administer the enema before bedtime; the entire procedure usually takes 15 to 20 minutes. Although at first adminis- tered daily, many patients require the enema only once every 48 hours. However, it is not advisable to administer the enema less frequently than that.
It usually takes at least 2 weeks before full continence is obtained. If the patient is constipated, as many spina bifida patients are, the enema may fail to dissolve or dislodge the balls of feces. Therefore, we usually prescribe a dose of magnesium citrate to clear out the colonic contents. The patient is then advised to ingest at least a tablespoon of natural wheat bran or an appropriate dose of some laxative on a daily basis. Metamucil (Searle Laboratories, Chicago) is well tolerated and serves this purpose.
RESULTS
We categorized the level of success of m a n a g e m e n t as incont inent or continent . Incont inent patients defe- cate unpredic tably and into their clothing or pads daily. Cont inen t patients have the abil i ty not to defe- cate into clothing or pads and are able to expel the bowel contents at a chosen t ime in a designated place. Such cont inent children will have no more than three inadver tent minor escapes of fecal mater ia l dur ing a month.
We treated 281 children with spina bifida. Of this group 112 were provided with the ECC; their ages are indicated in Fig 1. Before adopting our regimen all were totally incontinent . With the use of the ECC, we succeeded in achieving a cont inence rate of 100%.
Four parents permanent ly abandoned the use of the ECC, explaining that they preferred their child to be incont inent , ra ther than to cont inue to adminis ter the enemas. Five patients re turned to using the ECC after init ial ly discarding it.
Three patients developed allergic phenomena when a prototype was assembled in our laboratory. The components of this prototype had been approved for medical use in the Uni ted States, but inconsistency in the s tandards of the manufac tu re r ' s supply developed. The EC C is now manufac tu red from different compo- nents approved by the Canad ian Bureau of Medical Devices, and there have been no problems.
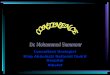
The EC C has an inflatable balloon, which is placed within the rectum (Fig 2). There is an exterior baffle that locks the balloon in place within the rectum, preventing its displacement in a cephalad direction, thus prevent ing the escape of enema fluid (Fig 3).
DISCUSSION
It is regret table that the problem of fecal inconti- nence in spina bifida, so devastat ing in its social
From the Department of Urodynamics, Hospital for Sick Chil- dren, the University of Toronto, and the Hugh MacMillan Medical Centre, Toronto.
Presented at the 33rd Annual Congress of the British Association of Paediatric Surgeons, Birmingham, England, July 16-18, 1986.
Address reprint requests to B. Shandling, FRCS, 555 University Ave, Toronto, Ontario, Canada MFG 1XS.
�9 1987 by Grune & Stratton, Inc. 0022-3468/87/2203-0022503.00/0
Journal of Pediatric Surgery, Vol 22, No 3 (March), 1987: pp 271-273 271

272 SHANDLING AND GILMOUR
10-
r
n=112
0
age (yrs.) 2 4 6 8 10 12 14 16 18 20
Fig 1. Age range,
consequences, has not received adequate attention. The problem is widespread, as evidenced by the amount of referrals we receive and our lengthy waiting list. Our urological colleagues will not insert an artifi- cial sphincter in any patient until we have first insti- tuted our regimen of bowel management.
There are several ways of handling fecal inconti- nence. ~-7 We found that the use of laxatives alone is of
Fig 2. ECC with balloon inflated in rectal ampulla. Rectum (A), End nozzle (B), Bal loon (C), Baff le (D), Ca the te r (E), Air Intake (F).
Fig 3. Barium enema with ECC in place showing continence of barium,
no value; administering too small a dose accomplishes nothing, while administering too large a dose to an incontinent patient will only result in profound embar- rassment. Digital disimpaction is unpleasant to per- form and only succeeds in emptying the distal rectal ampulla. More feces from the proximal bowel rapidly descend to pack the emptied segment of rectum.
Bearing in mind that none of our patients can resist the push of peristalsis, the most effective regimen consists of regular and complete elective emptying of the colon, which takes 24 to 48 hours to become filled again. No investigator has previously commented on the fact that with neurologic fecal incontinence, there is nothing to prevent enema fluid from flowing out of the incompetent anus during its instillation. Thus, standard enemas are difficult, if not impossible, to administer. Therefore it is hardly surprising that pub- lished results of enema management document the achievement of social continence in only 50% of patients. 5 This problem is successfully overcome by the use of the ECC, which, for the first time, permits the efficient administration of an enema to a patient with fecal incontinence without the enema solution leaking out. Clearly, for those patients using the ECC, the method is successful, otherwise it would have been abandoned.
The ECC can also be used to facilitate reduction of an intussusception with a barium enema. The usual taping in of the enema catheter becomes unnecessary.
The aims of any bowel program in spina bifida must be to make the patient as independent as possible and

SUCCESSFUL BOWEL MANAGEMENT IN SPINA BIFIDA 273
predictably continent. This is achieved by a large- volume saline enema used in conjunction with the ECC.
REFERENCES
1. Leigh R J, Turnberg LA; Faecal Incontinence: The unvoiced symptom. Lancet 1:1349-1351, 1982
2. Vigliarolo D: Managing bowel incontinence in children with meningomyelocele. Am J Nurs 80:105-107, 1980
3. White J J, Shaker I: The management of neurological fecal
incontinence, in Freeman JM (ed): Practical Management of Meningomyelocele. Baltimore, University Press, 1974, pp 198-217
4. White J J, Suzuk H, E1 Shafie M, et al: A physiologic rationale for the management of neurologic rectal incontinence in children. Pedatric 49:888-893, 1972
5. Forsythe I, Kinley JG: Bowel control of children with spina bifida. Dev Med Child Neurol 12:27-31, 1970
6. Dietrich S, Okamoko G: Bowel training for children with neurogenic dysfunction: A follow-up. Arch Phys Med Rehabil 63:166-170, 1982
7. Taylor N, Berni R, Horning MR: Neurogenic bowel manage- ment. Am Fam Physician 7:126-218, 1973