Embed Size (px)
Citation preview

Electronic copy available at: http://ssrn.com/abstract=2157310Electronic copy available at: http://ssrn.com/abstract=2157310
1
The effect of self help groups on access to maternal health services:
evidence from rural India
Somen Saha1*, Peter Annear
1, Swati Pathak
2
Abstract
Background: The main challenge for achieving universal health coverage in India is ensuring
effective coverage for poor and vulnerable communities, with high levels of income and
gender inequity in access to health care. Self help groups (SHGs), a small economically
homogeneous affinity group of the rural poor voluntarily coming together to save small
amount and provide collateral free loans, is considered the cornerstone of much of the
microfinance activity. SHGs are perceived to influence health outcome, particularly maternal
and child health knowledge and service utilization. Evidence about the impact of SHGs on
health has, however, have been derived from pilot level interventions and is thus limited in
scope. Widening this scope by using data from the national District Level Household Survey
(DLHS-3), this paper analyzes the influence of the presence of SHGs on maternal health
service uptake in rural India.
Methods: DLHS-3 collected information on 643,944 ever married women from 22,825
villages in India. The primary predictor variable was presence of SHG in village. The
outcome variables were: institutional delivery; feeding newborns colostrums; knowledge
about female sterilization, IUD, oral pills, emergency contraception, and female condom; and
ever used oral pills, IUD, and female sterilization. Stepwise logistic regression was applied
to estimate the influence controlling for respondent education, occupation, heard or seen
health messages, availability of educational facilities, and the existence of a village health
and sanitation committee.
Results: Respondents from villages with SHG were more likely to have delivered in an
institution, feed newborn colostrums, know and utilize family planning products and services.
These results are positive and significant after controlling for individual and village level
1 Nossal Institute for Global Health University of Melbourne, Level 4, Alan Gilbert Building, 161 Barry St, Carlton,
Victoria, 3010, Australia. 2 Indian Institute of Management, Ahmedabad, Gujarat 380015, India
* Corresponding author: Nossal Institute for Global Health University of Melbourne, Level 4, Alan Gilbert Building, 161
Barry St, Carlton, Victoria, 3010, Australia. Tel: +61 0415 914 459. Email: [email protected].
Electronic copy available at: http://ssrn.com/abstract=2157310Electronic copy available at: http://ssrn.com/abstract=2157310
2
heterogeneities, and are consistent with existing literature that the social capital generated
through women’s participation in SHG, influence health outcome.
Conclusion: The study concludes that the presence of SHGs in a village is associated with
higher knowledge of family planning and maternal health service uptake in rural India. Also
our results indicates the need for complementary health programmes to build up on the
solidarity and social capital generated as a result of the association, to have maximum impact
on community health. To achieve the goal of improving public health, there is a need to
better understand the benefit of systematic collaboration between public health community
and these grassroots organizations.

3
Introduction
As India quest to achieve universal health coverage, the main challenge would be to expand
coverage to its citizens with protection from the costs of at least some basic health services.
The poor generally have worse health outcomes and access to care compared to the non-poor.
Evidences from low and middle income countries shows access barriers to health services are
likely to be more difficult to overcome for the poor and other vulnerable groups, as the costs
of access, lack of information and cultural barriers impede them from benefiting from public
spending (Ensor & Cooper, 2004; McNamee, Ternent, & Hussein, 2009). Poor health
contributes to the persistence of India’s high poverty rates, with health expenditures driving
39 million families into poverty each year (Selvaraj & Karan, 2009). Even when treatment is
sought, significantly smaller sums of money are spent on treatment of women than on men
(Iyer, Sen, & George, 2007). DLHS -3 (2007-08) data reveal that in rural India only 37.9%
women delivered their last child in an institution, and unmet need for limiting and spacing
were 22.8% and 14.1% respectively. While the problems of poor health are multi-
dimensional, approaches to find their solutions are largely unisectoral. Ensor and Cooper
(Ensor & Cooper, 2004) note that interventions to address barriers to health services should
follow pragmatic policy routes that go beyond the traditional boundaries of the public health
sector. Outside the health sector SHGs have emerged as a development strategy having a
primary focus on poverty alleviation and empowerment of women. In India there has been a
particular focus to improve financial accessibility to ensure sustainability of social services,
thus, in effect, transforming and expanding self-help groups into economically oriented co-
operatives (Nayar KR, 2004). SHGs can, in many ways, be considered the cornerstone of
much of the microfinance activity in India. These small groups (10-20 members each) of
predominantly rural women coming together to form savings and credit organizations, are
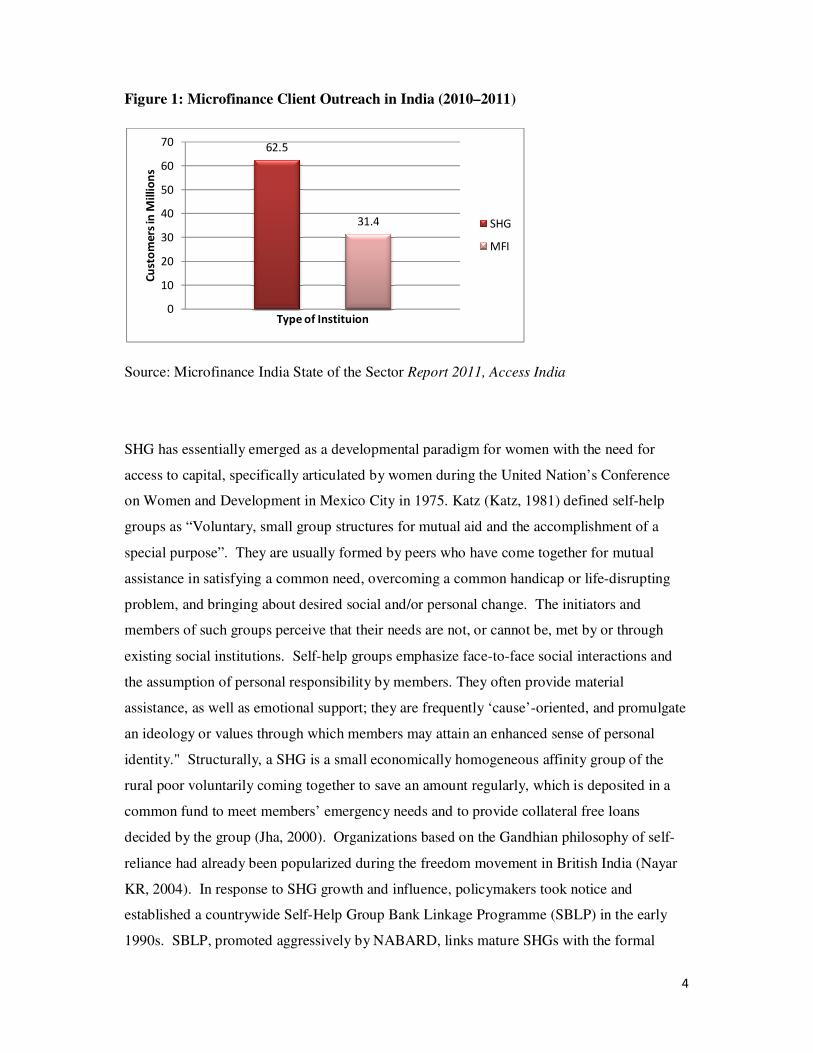
well established in the country. Ninety-three million clients (impacting over 300 million
people including households) are engaged by Microfinance Institutions (MFIs) and SHG -
Bank Linkage programmes (Srinivasan, 2012) (Figure 1).
4
Figure 1: Microfinance Client Outreach in India (2010–2011)
Source: Microfinance India State of the Sector Report 2011, Access India
SHG has essentially emerged as a developmental paradigm for women with the need for
access to capital, specifically articulated by women during the United Nation’s Conference
on Women and Development in Mexico City in 1975. Katz (Katz, 1981) defined self-help
groups as “Voluntary, small group structures for mutual aid and the accomplishment of a
special purpose”. They are usually formed by peers who have come together for mutual
assistance in satisfying a common need, overcoming a common handicap or life-disrupting
problem, and bringing about desired social and/or personal change. The initiators and
members of such groups perceive that their needs are not, or cannot be, met by or through
existing social institutions. Self-help groups emphasize face-to-face social interactions and
the assumption of personal responsibility by members. They often provide material
assistance, as well as emotional support; they are frequently ‘cause’-oriented, and promulgate
an ideology or values through which members may attain an enhanced sense of personal
identity." Structurally, a SHG is a small economically homogeneous affinity group of the
rural poor voluntarily coming together to save an amount regularly, which is deposited in a
common fund to meet members’ emergency needs and to provide collateral free loans
decided by the group (Jha, 2000). Organizations based on the Gandhian philosophy of self-
reliance had already been popularized during the freedom movement in British India (Nayar
KR, 2004). In response to SHG growth and influence, policymakers took notice and
established a countrywide Self-Help Group Bank Linkage Programme (SBLP) in the early
1990s. SBLP, promoted aggressively by NABARD, links mature SHGs with the formal
62.5
31.4
0
10
20
30
40
50
60
70C
ust
om
ers
in M
illi
on
s
Type of Instituion
SHG
MFI
5
banking system (commercial banks, Regional Rural Banks and cooperative banks). SHGs are
linked to Regional Rural Banks (RRB), commercial banks and cooperative banks to access
microcredit as a source of additional capital for the group members to supplement their
savings. The Government of India through Swarnajayanti Gram Swarojgar Yojana (SGSY)
intended to provide self-employment to millions of villagers. Poor families living below the
poverty line were organized into SHGs established with a mixture of government subsidy and
credit from investment banks. The main aim of these SHGs was to bring the poor families
above the poverty line and concentrate on income generation. The SHGs are aided,
supported and trained by non-governmental organizations (NGOs), community based
organizations (CBOs), individuals, banks and self-help promoting institutions.
Self help groups are perceived to influence health outcomes, particularly maternal and child
health knowledge and service utilization, a priority area for Millennium Development Goals
(MDGs) 4 and 5. SHGs are regarded as the most exciting and least recognized resource for
improving public health (Humphreys & Ribisl, 1999). The social capital generated through
women’s participation in community organization influence health outcomes, as argued, by
Nobles and Fankenberg (Nobles & Frankenberg, 2009) and DeLoach and Lamanna (DeLoach
& Lamanna, 2011). Social capital is defined by Putnam (Putnam, 1993) as features of social
organization, such as trust, norms and networks, that can improve the efficiency of society by
facilitating coordinated actions. Woolcock (Woolcock, 1998) further split social capital into
three connecting strands: bonding social capital i.e. ties between immediate family members,
neighbours and close friends; bridging social capital i.e. ties between people from different
ethnic, geographical, and occupational backgrounds; and linking social capital i.e. ties
between poor people and those in positions of influence in formal organizations such as
banks, schools etc. It is believed that self help groups are mobilized by existing bonding
social capital, and then build linking social capital as the group members get involved in
activities (Kanak & Iiguni, 2007). NGOs like SEWA, BRAC, and Grameen Bank have
extensively engaged in promoting health related activities through SHG participation.
Studies have shown the positive effect of SHGs on exclusion (Mohindra, Haddad, &
Narayana, 2008), improved childcare and contraceptive use (Hadi, 2001, 2002), and neo-natal
mortality (Tripathy et al., 2010). However, Nayar (Nayar KR, 2004) noted that the few
success stories noted are in the context of large organizations that incorporate self help
activities as just one component. Therefore, it is hard to tease out the contribution of self
help independent of other concurrent activities or the organizational infrastructure. Much of
6
the existing evidence that contributes to the cause and effect relationships has also been
criticized as consisting of choice based sampling and self-selection bias (Pitt, Khandker,
McKernan, & Latif, 1999).
As a result, despite decades of existence, and national programmes to promote SHG
strategies, evidence of the link between SHGs and improved health outcomes is limited to
that derived from small pilot level interventions in India. There has been an absence of
sufficiently substantial data to carry out an analysis to find this evidence. According to Nayar
(Nayar KR, 2004) there is as yet no convincing evidence that in societies with unmet demand
for regulated health care, SHGs can become a "third option" to replace ailing government
health services. While there exist large panel datasets to examine the association between the
poverty alleviation effort and health outcome in Bangladesh (Islam & Maitra, 2011), there
was no conscious effort in India to collect such information. DLHS-3 had a question on the
presence of a SHG in its village level questionnaire. This gave us an opportunity to analyze
and report in this paper on the influence of SHGs on the reproductive and child health (RCH)
knowledge and practices of the women in those villages. Even our analysis can provide only
a partial picture, as it does not have information on the women’s participation in SHG
activities. However, with information on 643,944 ever married women from 22,825 villages
in India, this presents our best available option to analyze the influence of the presence of
SHGs on women’s RCH knowledge and practices.
Data and descriptive statistics
We used data from the third round of the District Level Household Survey (DLHS-3)
conducted in 2007-08 in 601 districts from 34 states and union territories of India.
Information was collected from 22,825 villages in India (through the village questionnaire)
and from 643,944 ever married women (15 – 49 years) through the ever married women’s
questionnaire. DLHS-3 adopted a multi-stage stratified systematic sampling design which
resulted in national and state-representative samples after applying sampling weights to
control for complex survey design (IIPS, 2010). The DLHS-3 is designed to provide
information on family planning, maternal and child health, reproductive health of ever
married women and adolescent girls, and utilization of maternal and child healthcare services
at the district level in India. In addition, DLHS-3 also provides information on new-born
care, post-natal care within 48 hours, role of the Associated Social Health Activist (ASHA) in
7
enhancing reproductive and child health care, and the coverage of Janani Suraksha Yojana
(JSY), a conditional cash transfer programme to increase births in health facilities. At village
level DLHS-3 asked questions about presence of SHGs in the village. Unit level data from
the village file and ever married women file were merged to conduct the analysis.
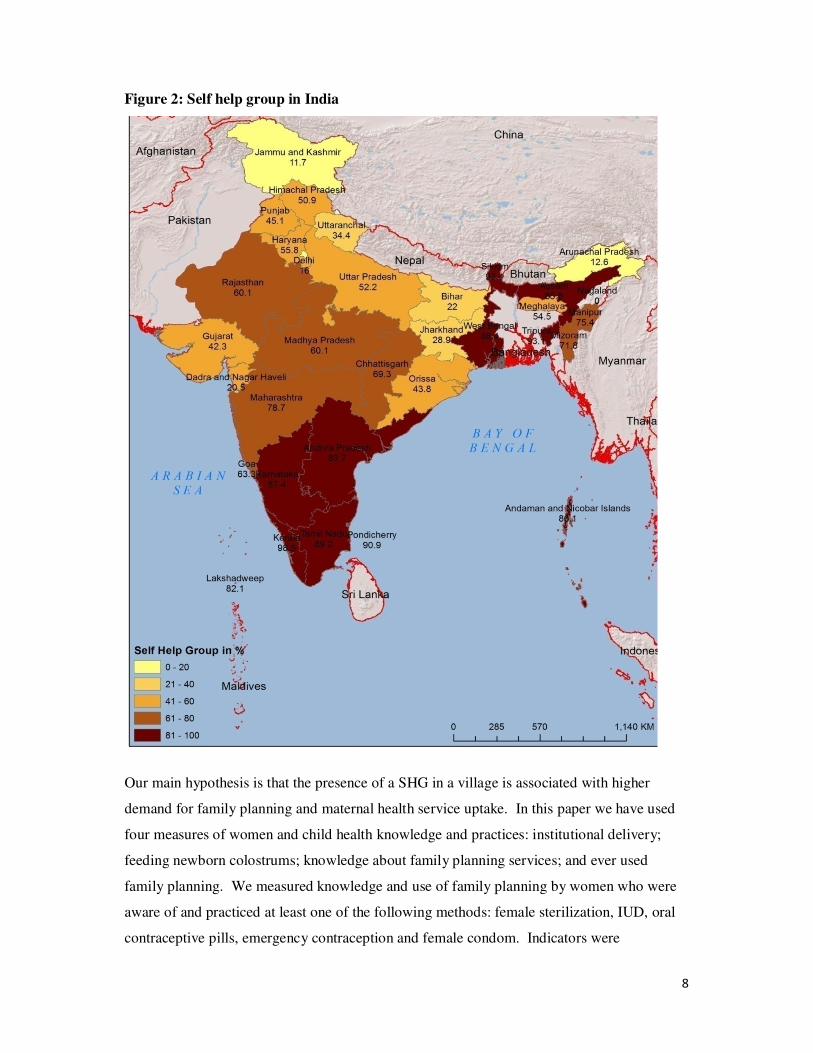
As per DLHS-3 data, 57.9 percent of Indian villages have a self help group (Figure 2). The
majority of these groups are present in southern and north-eastern India, followed by
Maharashtra, Chhattisgarh, Rajasthan and Madhya Pradesh.
8
Figure 2: Self help group in India
Our main hypothesis is that the presence of a SHG in a village is associated with higher
demand for family planning and maternal health service uptake. In this paper we have used
four measures of women and child health knowledge and practices: institutional delivery;
feeding newborn colostrums; knowledge about family planning services; and ever used
family planning. We measured knowledge and use of family planning by women who were
aware of and practiced at least one of the following methods: female sterilization, IUD, oral
contraceptive pills, emergency contraception and female condom. Indicators were

9
transformed into binary measures by re-coding all Yes as 1 and No as 0. For place of
delivery: deliveries at hospital, dispensary, urban health centre (UHC)/urban primary health
centre (UPHC), community health centre (CHC)/Rural hospital, primary health centre (PHC),
Sub center, Ayush hospital/clinic, NGO/Trust clinic, Private hospital/clinic, and on way to
hospitals were re-coded as 1, and delivery at home and work place were re-coded as 0. Data
analysis was done using SPSS Version 19.
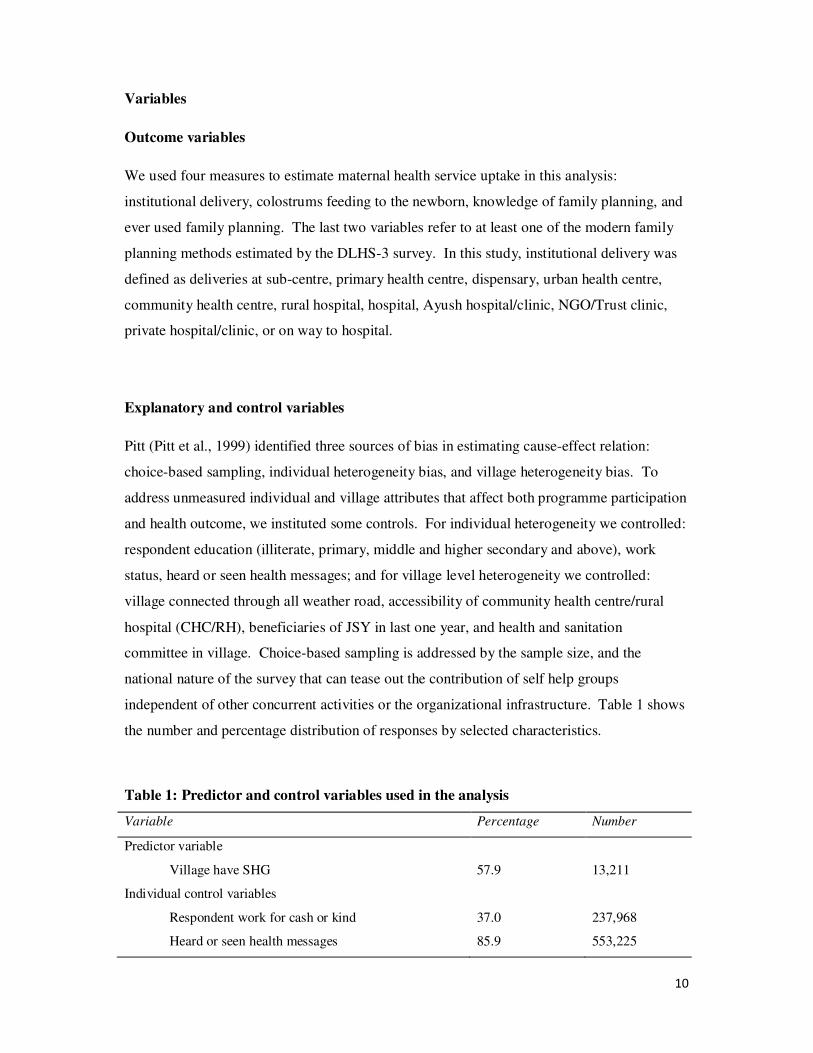
The descriptive statistics (Figure 3) show some interesting findings on the four measures of
women and child health knowledge and practices. The overall use of family planning was
found to be very low. The presence of a SHG has a positive and strong correlation with all
four measures of knowledge and practices. Households in villages with a SHG are more
likely to go for institutional delivery, more likely to feed newborns colostrums, more likely to
have knowledge of and use family planning products and services, compared to households in
villages without a SHG. Members engaged in self help activity feel the sense of connectivity
and discuss issues ranging from place of delivery to feeding the baby, and family planning
products and services.
Figure 3: Study variables in villages with and without SHG
61%
84%
99%
65%
34%
73%
90%
55%
Institutional
Delivery
Feeding Colostrums Knowledge of Family
Planning
Ever used Family
Planning
Characteristics of study variables in
villages with and without SHG
Yes No
10
Variables
Outcome variables
We used four measures to estimate maternal health service uptake in this analysis:
institutional delivery, colostrums feeding to the newborn, knowledge of family planning, and
ever used family planning. The last two variables refer to at least one of the modern family
planning methods estimated by the DLHS-3 survey. In this study, institutional delivery was
defined as deliveries at sub-centre, primary health centre, dispensary, urban health centre,
community health centre, rural hospital, hospital, Ayush hospital/clinic, NGO/Trust clinic,
private hospital/clinic, or on way to hospital.
Explanatory and control variables
Pitt (Pitt et al., 1999) identified three sources of bias in estimating cause-effect relation:
choice-based sampling, individual heterogeneity bias, and village heterogeneity bias. To
address unmeasured individual and village attributes that affect both programme participation
and health outcome, we instituted some controls. For individual heterogeneity we controlled:
respondent education (illiterate, primary, middle and higher secondary and above), work
status, heard or seen health messages; and for village level heterogeneity we controlled:
village connected through all weather road, accessibility of community health centre/rural
hospital (CHC/RH), beneficiaries of JSY in last one year, and health and sanitation
committee in village. Choice-based sampling is addressed by the sample size, and the
national nature of the survey that can tease out the contribution of self help groups
independent of other concurrent activities or the organizational infrastructure. Table 1 shows
the number and percentage distribution of responses by selected characteristics.
Table 1: Predictor and control variables used in the analysis
Variable Percentage Number
Predictor variable
Village have SHG 57.9 13,211
Individual control variables
Respondent work for cash or kind 37.0 237,968
Heard or seen health messages 85.9 553,225
11
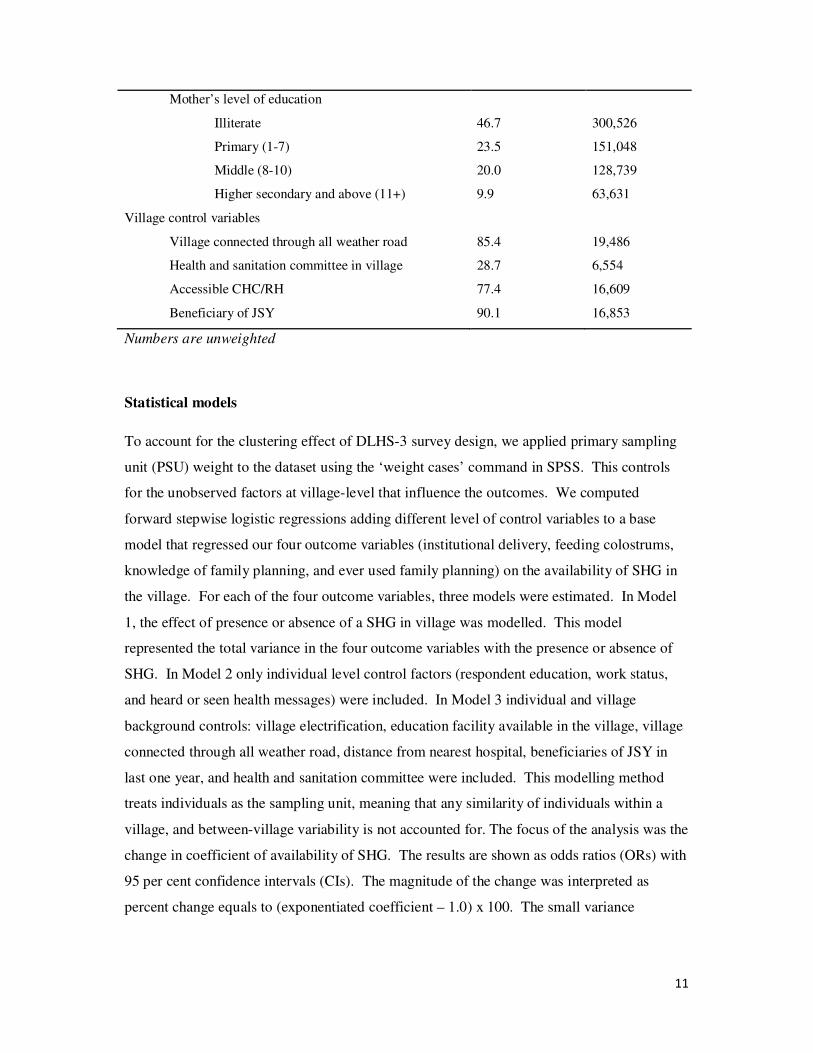
Mother’s level of education
Illiterate
Primary (1-7)
Middle (8-10)
Higher secondary and above (11+)
46.7
23.5
20.0
9.9
300,526
151,048
128,739
63,631
Village control variables
Village connected through all weather road
Health and sanitation committee in village
Accessible CHC/RH
Beneficiary of JSY
85.4
28.7
77.4
90.1
19,486
6,554
16,609
16,853
Numbers are unweighted
Statistical models
To account for the clustering effect of DLHS-3 survey design, we applied primary sampling
unit (PSU) weight to the dataset using the ‘weight cases’ command in SPSS. This controls
for the unobserved factors at village-level that influence the outcomes. We computed
forward stepwise logistic regressions adding different level of control variables to a base
model that regressed our four outcome variables (institutional delivery, feeding colostrums,
knowledge of family planning, and ever used family planning) on the availability of SHG in
the village. For each of the four outcome variables, three models were estimated. In Model
1, the effect of presence or absence of a SHG in village was modelled. This model
represented the total variance in the four outcome variables with the presence or absence of
SHG. In Model 2 only individual level control factors (respondent education, work status,
and heard or seen health messages) were included. In Model 3 individual and village
background controls: village electrification, education facility available in the village, village
connected through all weather road, distance from nearest hospital, beneficiaries of JSY in
last one year, and health and sanitation committee were included. This modelling method
treats individuals as the sampling unit, meaning that any similarity of individuals within a
village, and between-village variability is not accounted for. The focus of the analysis was the
change in coefficient of availability of SHG. The results are shown as odds ratios (ORs) with
95 per cent confidence intervals (CIs). The magnitude of the change was interpreted as
percent change equals to (exponentiated coefficient – 1.0) x 100. The small variance
12
inflation factor of 1.09 (not reported) indicated the absence of any significant collinearity
between explanatory variables in the regression model.
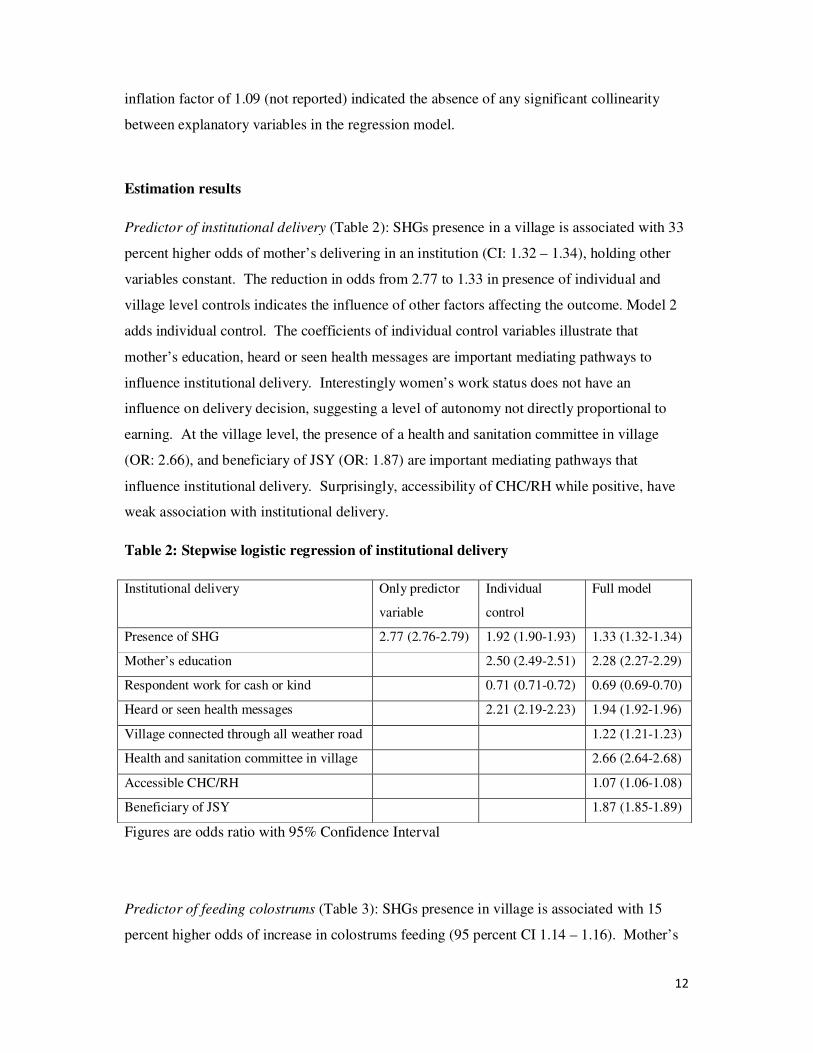
Estimation results
Predictor of institutional delivery (Table 2): SHGs presence in a village is associated with 33
percent higher odds of mother’s delivering in an institution (CI: 1.32 – 1.34), holding other
variables constant. The reduction in odds from 2.77 to 1.33 in presence of individual and
village level controls indicates the influence of other factors affecting the outcome. Model 2
adds individual control. The coefficients of individual control variables illustrate that
mother’s education, heard or seen health messages are important mediating pathways to
influence institutional delivery. Interestingly women’s work status does not have an
influence on delivery decision, suggesting a level of autonomy not directly proportional to
earning. At the village level, the presence of a health and sanitation committee in village
(OR: 2.66), and beneficiary of JSY (OR: 1.87) are important mediating pathways that
influence institutional delivery. Surprisingly, accessibility of CHC/RH while positive, have
weak association with institutional delivery.
Table 2: Stepwise logistic regression of institutional delivery
Institutional delivery Only predictor
variable
Individual
control
Full model
Presence of SHG 2.77 (2.76-2.79) 1.92 (1.90-1.93) 1.33 (1.32-1.34)
Mother’s education 2.50 (2.49-2.51) 2.28 (2.27-2.29)
Respondent work for cash or kind 0.71 (0.71-0.72) 0.69 (0.69-0.70)
Heard or seen health messages 2.21 (2.19-2.23) 1.94 (1.92-1.96)
Village connected through all weather road 1.22 (1.21-1.23)
Health and sanitation committee in village 2.66 (2.64-2.68)
Accessible CHC/RH 1.07 (1.06-1.08)
Beneficiary of JSY 1.87 (1.85-1.89)
Figures are odds ratio with 95% Confidence Interval
Predictor of feeding colostrums (Table 3): SHGs presence in village is associated with 15
percent higher odds of increase in colostrums feeding (95 percent CI 1.14 – 1.16). Mother’s
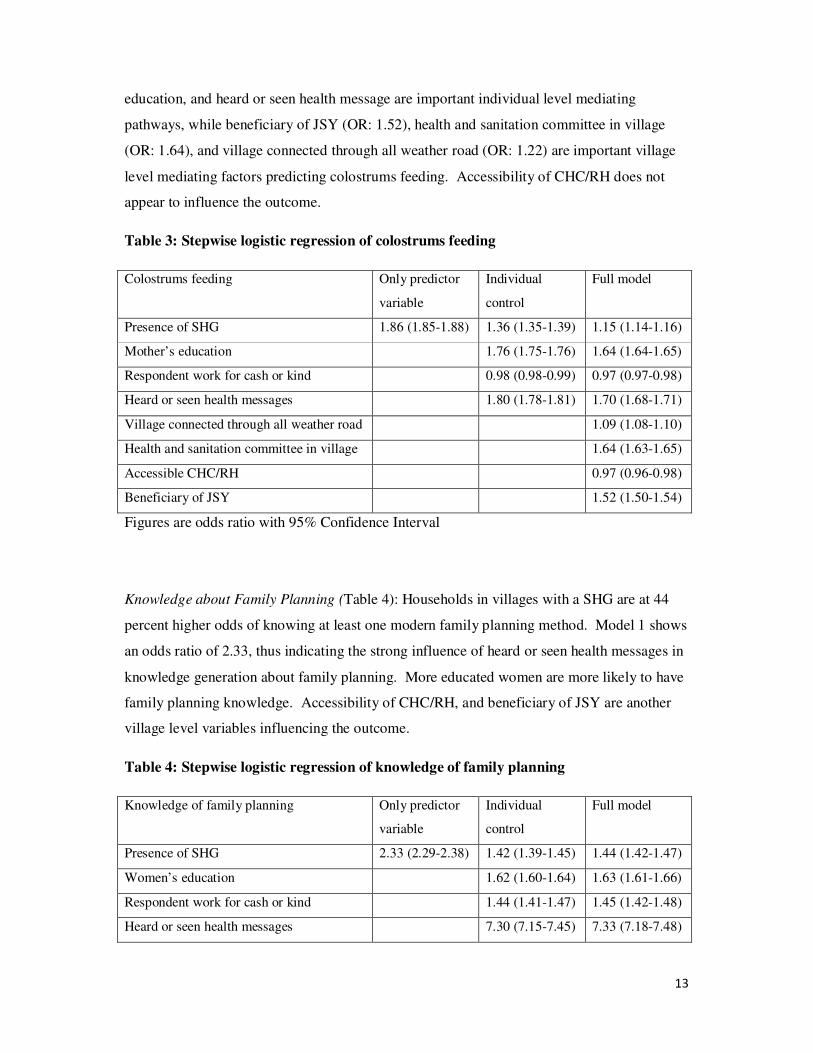
13
education, and heard or seen health message are important individual level mediating
pathways, while beneficiary of JSY (OR: 1.52), health and sanitation committee in village
(OR: 1.64), and village connected through all weather road (OR: 1.22) are important village
level mediating factors predicting colostrums feeding. Accessibility of CHC/RH does not
appear to influence the outcome.
Table 3: Stepwise logistic regression of colostrums feeding
Colostrums feeding Only predictor
variable
Individual
control
Full model
Presence of SHG 1.86 (1.85-1.88) 1.36 (1.35-1.39) 1.15 (1.14-1.16)
Mother’s education 1.76 (1.75-1.76) 1.64 (1.64-1.65)
Respondent work for cash or kind 0.98 (0.98-0.99) 0.97 (0.97-0.98)
Heard or seen health messages 1.80 (1.78-1.81) 1.70 (1.68-1.71)
Village connected through all weather road 1.09 (1.08-1.10)
Health and sanitation committee in village 1.64 (1.63-1.65)
Accessible CHC/RH 0.97 (0.96-0.98)
Beneficiary of JSY 1.52 (1.50-1.54)
Figures are odds ratio with 95% Confidence Interval
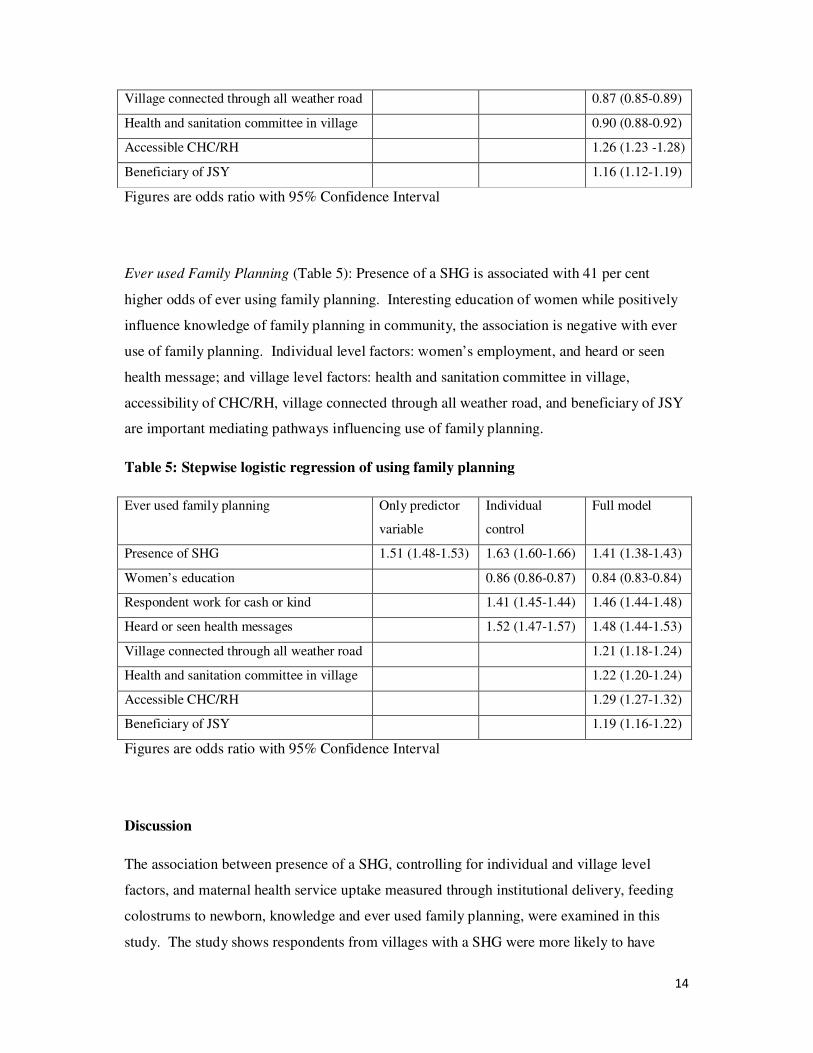
Knowledge about Family Planning (Table 4): Households in villages with a SHG are at 44
percent higher odds of knowing at least one modern family planning method. Model 1 shows
an odds ratio of 2.33, thus indicating the strong influence of heard or seen health messages in
knowledge generation about family planning. More educated women are more likely to have
family planning knowledge. Accessibility of CHC/RH, and beneficiary of JSY are another
village level variables influencing the outcome.
Table 4: Stepwise logistic regression of knowledge of family planning
Knowledge of family planning Only predictor
variable
Individual
control
Full model
Presence of SHG 2.33 (2.29-2.38) 1.42 (1.39-1.45) 1.44 (1.42-1.47)
Women’s education 1.62 (1.60-1.64) 1.63 (1.61-1.66)
Respondent work for cash or kind 1.44 (1.41-1.47) 1.45 (1.42-1.48)
Heard or seen health messages 7.30 (7.15-7.45) 7.33 (7.18-7.48)
14
Village connected through all weather road 0.87 (0.85-0.89)
Health and sanitation committee in village 0.90 (0.88-0.92)
Accessible CHC/RH 1.26 (1.23 -1.28)
Beneficiary of JSY 1.16 (1.12-1.19)
Figures are odds ratio with 95% Confidence Interval
Ever used Family Planning (Table 5): Presence of a SHG is associated with 41 per cent
higher odds of ever using family planning. Interesting education of women while positively
influence knowledge of family planning in community, the association is negative with ever
use of family planning. Individual level factors: women’s employment, and heard or seen
health message; and village level factors: health and sanitation committee in village,
accessibility of CHC/RH, village connected through all weather road, and beneficiary of JSY
are important mediating pathways influencing use of family planning.
Table 5: Stepwise logistic regression of using family planning
Ever used family planning Only predictor
variable
Individual
control
Full model
Presence of SHG 1.51 (1.48-1.53) 1.63 (1.60-1.66) 1.41 (1.38-1.43)
Women’s education 0.86 (0.86-0.87) 0.84 (0.83-0.84)
Respondent work for cash or kind 1.41 (1.45-1.44) 1.46 (1.44-1.48)
Heard or seen health messages 1.52 (1.47-1.57) 1.48 (1.44-1.53)
Village connected through all weather road 1.21 (1.18-1.24)
Health and sanitation committee in village 1.22 (1.20-1.24)
Accessible CHC/RH 1.29 (1.27-1.32)
Beneficiary of JSY 1.19 (1.16-1.22)
Figures are odds ratio with 95% Confidence Interval
Discussion
The association between presence of a SHG, controlling for individual and village level
factors, and maternal health service uptake measured through institutional delivery, feeding
colostrums to newborn, knowledge and ever used family planning, were examined in this
study. The study shows respondents from villages with a SHG were more likely to have
15
delivered in an institution, fed newborns colostrums, known about and utilized family
planning products and services. Community agents like networks of microfinance and self
help groups are new ways to involve communities in the oversight, planning or operations of
health services. They also give the communities avenues to voice their concerns. These
groups provide a unique space, in which solidarity is created through promoting shared
visions and goals and combining collective strengths. The trust and social capital empower
communities and positively influence individual and community health. However, on their
own, SHGs can have limited impact. This is explained by the relatively low odds ratio in
presence of individual and village level controls. Clearly, in order to have maximum impact
on community health, there is a need for additional complementary health programmes to
build on the solidarity and social capital generated as a result of the group. Our study shows
women’s work status, and the presence of a health and sanitation committee in a village have
minimal effect on maternal health service uptake. While the former points to lack of
autonomy in decision making, the later indicates the need to strengthen village health and
sanitation committee to take a more active role in the community.
The study had some limitations, which need to be considered when interpreting the results.
First, we did the analysis at the aggregate country level. This masks the variation in spread
and intensity of SHG activity in India as depicted in Figure 2. Second, presence of a SHG in
the village could only partially explain the level of activity. Women’s participation in SHG
(Schurmann & Johnston, 2009), availability of credit (Islam & Maitra, 2011), and duration of
association (Hamad & Fernald, 2010; Mohindra et al., 2008) are other key predictors that the
DLHS-3 survey, due its scope and intent, did not collect. Nonetheless this large national
level dataset deals with two important biases discussed in previous studies: choice based
sampling (Pitt et al., 1999), and teasing out the contribution of self help groups in the
organizational infrastructure (Nayar KR, 2004). Third, our modelling method treats
individuals as the sampling unit, and any similarities of individuals within a village, and
between-village variability is not accounted for. Hence, while we expect little difference in
odds ratio, standard errors for village level variables may be slightly higher than reported.
The fourth limitation relates to the nature of the DLHS-3 survey, such as self reported
information of respondents and the cross sectional nature of the survey, as described by Jat et
al (Jat, Ng, & San Sebastian, 2011). Therefore, we could only examine the association
between explanatory variables and four indicators of maternal health services uptake and
could not draw conclusions about causality.

16
Conclusion
The study concludes that the presence of SHGs in a village is associated with higher demand
for family planning and maternal health service uptake in rural India. Also our results
indicate the need for additional complementary health programmes to build on the solidarity
and social capital generated as a result of the group, in order to have maximum impact on
community health. Our analysis of the national level data shows there is a strong case for
policy makers to work closely with these groups and better leverage their power for health
improvement and poverty reduction. This has implications for low and middle income
countries where barriers to access to health services, and information and cultural barriers,
prevent the poor and vulnerable groups from benefiting from public spending. Self help
groups are an innovative way to combine poverty alleviation and community health
interventions into an integrated strategy that leverages existing resources to achieve greater
impact and scale. By linking financial services for the poor with proven community health
interventions, two fundamental needs can be met simultaneously. Some highly effective, low
cost interventions to promote health and sanitation awareness that can be carried out with the
help of these groups include: provision of health savings accounts and loans in case of major
illness, encouraging the adoption of better sanitation practices and clean water, provision of
low-cost generic drug points, and discounted preferred provider network at the village-level.
To achieve the goal of improving public health, there is a need to better understand the
benefits of systematic collaboration between the public health community and these
grassroots organizations.
Acknowledgement: The research is supported by a Research Higher Degree grant from Nossal
Institute for Global Health, University of Melbourne, Australia, and Welcome Trust Capacity
Strengthening Strategic Award to the Public Health Foundation of India and a consortium of UK
Universities. We acknowledge the statistical advice received from the Statistical Consulting Centre at
University of Melbourne. An earlier version of this paper was presented at the Global Maternal Health
Conference, Arusha, Tanzania.
17
References
DeLoach, S. B., & Lamanna, E. (2011). Measuring the impact of microfinance on child health
outcomes in Indonesia. World Development, 39(10), 1808-1819.
Ensor, T., & Cooper, S. (2004). Overcoming barriers to health service access: influencing the demand
side. Health Policy and Planning, 19(2), 69-79.
Hadi, A. (2001). Promoting health knowledge through micro-credit programmes: experience of BRAC
in Bangladesh. Health Promotion International, 16(3), 219-227.
Hadi, A. (2002). Integrating prevention of acute respiratory infections with micro-credit programme:
experience of BRAC, Bangladesh. Public health, 116(4), 238-244.
Hamad, R., & Fernald, L. C. H. (2010). Microcredit participation and nutrition outcomes among
women in Peru. Journal of Epidemiology and Community Health, 66(6).
Humphreys, K., & Ribisl, K. M. (1999). The case for a partnership with self-help groups. Public Health
Reports, 114(4), 322.
IIPS. (2010). District Level Household Survey (DLHS-3), 2007–08. India. Mumbai: International
Institute for Population Sciences
Islam, A., & Maitra, P. (2011). Health shocks and consumption smoothing in rural households: Does
microcredit have a role to play? Journal of Development Economics, 97(2), 232-243.
Iyer, A., Sen, G., & George, A. (2007). The dynamics of gender and class in access to health care:
Evidence from rural Karnataka, India. International Journal of Health Services, 37(3), 537-
554.
Jat, T. R., Ng, N., & San Sebastian, M. (2011). Factors affecting the use of maternal health services in
Madhya Pradesh state of India: a multilevel analysis. International Journal for Equity in
Health, 10(1), 59.
Jha, A. K. (2000). Lending to the Poor: Designs for Credit. Economic and Political Weekly, 606-609.
Kanak, S., & Iiguni, Y. (2007). Microfinance programs and social capital formation: The present
scenario in a rural village of Bangladesh. The International journal of applied economics and
finance, 1(2), 97-104.
Katz, A. H. (1981). Self-help and mutual aid: An emerging social movement? Annual review of
sociology, 7, 129-155.
McNamee, P., Ternent, L., & Hussein, J. (2009). Barriers in accessing maternal healthcare: evidence
from low-and middle-income countries. Expert Review of Pharmacoeconomics and
Outcomes Research, 9(1), 41-48.
Mohindra, K., Haddad, S., & Narayana, D. (2008). Can microcredit help improve the health of poor
women? Some findings from a cross-sectional study in Kerala, India. International Journal for
Equity in Health, 7, 2.
Nayar KR, K. C. a. R. O. (2004). Self-help: What future role in health care for low and middle-income
countries? International Journal for Equity in Health, 3(1).
Nobles, J., & Frankenberg, E. (2009). Mothers' community participation and child health. Journal of
health and social behavior, 50(1), 16-30.
Pitt, M., Khandker, S., McKernan, S., & Latif, M. (1999). Credit programs for the poor and
reproductive behavior in low-income countries: are the reported causal relationships the
result of heterogeneity bias? Demography, 36(1), 1-21.
Putnam, R. (1993). Making Democracy Work. Civic traditions in modern Italy. Princeton University
Schurmann, A. T., & Johnston, H. B. (2009). The group-lending model and social closure: microcredit,
exclusion, and health in Bangladesh. Journal of health, population, and nutrition, 27(4), 518.
Selvaraj, S., & Karan, A. K. (2009). Deepening health insecurity in India: evidence from national
sample surveys since 1980s. Econ Polit Wkly, 44, 55-60.
Srinivasan, N. (2012). Microfinance India: state of the sector report 2011: Sage Publications Pvt. Ltd.
Tripathy, P., Nair, N., Barnett, S., Mahapatra, R., Borghi, J., Rath, S., . . . Sinha, R. (2010). Effect of a
participatory intervention with women's groups on birth outcomes and maternal depression

18
in Jharkhand and Orissa, India: a cluster-randomised controlled trial. The Lancet, 375(9721),
1182-1192.
Woolcock, M. (1998). Social capital and economic development: Toward a theoretical synthesis and
policy framework. Theory and society, 27(2), 151-208.





























