Embed Size (px)
Citation preview

Lhfish Jorrmcd of Phsrir Surge:,’ ( 1996). 49, 383-389 % 1996 The B&h Association of Plastic Surgeons
The distally based superficial sural flap for reconstruction of the lower leg and foot
N. Rajacic, M. Darweesh, K. Jayakrishnan, R. K. Gang and S. Kojic
Al-B~btain Center for Plastic, Reconstructive Surgery and Burns, Kuwuit University, Kuwait
SUMMAR Y. We describe our experience with the use of distally based superficial sural flaps for coverage of defects in the lower leg and foot in 21 patients. In 18 patients the flap was successfully transferred, in 2 cases partial necrosis of the flap occurred and 1 flap failed completely. In 18 cases the flap was used as a fasciocutaneous flap and in 3 cases as a fascial flap only. The advantages of this flap are: easy and quick dissection, hence saving operating time, minimal morbidity of donor site and preservation of major arteries of the leg. Although the flap was described as reliable for covering defects around the ankle joint, we have been able to cover defects of the dorsum of the foot distally and up to the mid-third of the tibia proximally.
Coverage of soft tissue defects of the lower one third of the leg and of the foot is always a difficult problem to tackle. Various methods of reconstruction to cover such defects include the use of cross-leg flaps,’ local cutaneous, fascial or fasciocutaneous flaps based either proximally2~’ or distally,6-‘4 distally based muscle flapsi5.16 and free flaps.“,” Although recon- struction by a free flap transfer is superior to other methods of reconstruction, as it can provide well- vascularised tissue of any size with minimal donor site morbidity, 1,17.‘8 one has to consider the disadvan- tages of reconstruction by a free flap (lengthy procedure, sophisticated equipment, well-trained microsurgical team, high cost) for small to moder- ate defects.
In 1992, Masquelet et a1.19 reported a flap, based on reverse flow through the anastomosis between the median superficial sural artery and the lowermost perforator from the peroneal artery, for the recon- struction of moderate defects of distal parts of the leg.
The first major series of 21 flaps was reported by Hasegawa et al.” who also named them distally based superficial sural artery flaps, for the reconstruc- tion of similar defects, with almost no complications.
The purpose of this paper is to present our experi- ence with a distally based superficial sural flap for the reconstruction of the lower one third of the leg in a series of 21 patients.
Anatom)>
The blood supply to the skin of the lower leg is provided by direct cutaneous vessels arising from the popliteal artery or its branches, musculocutaneous perforators and septocutaneous vessels arising from the deeply situated major arteries.21.22 All the vessels extend and anastomose above the fascia in transverse and longitudinal directions forming rich vascular networks. Perforators from the suprafascial vascular network ramify in the subcutaneous tissue, forming subdermal and dermal vascular networks.
The median superficial sural artery is the largest among the direct cutaneous arteries (medial, median and lateral superficial sural arteries). It pierces the fascia cruris in the lower two thirds of the posterior calf, following and nourishing the medial sural nerve.23 During its suprafascial course, the artery gives off several cutaneous branches to the overlying skin. In its distal part, behind the lateral malleolus, the artery anastomoses with septocutaneous perfor- ators from the peroneal artery, either directly or through the interlacing suprafascial network.” There are three to five peroneal septocutaneous vessels arising from the peroneal artery in the posterolateral septum, the major one being constant and located about 5 cm above the tip of the lateral malleolus.19,24 This distal anastomosis between the peroneal artery and the median superficial sural artery is a pivot point for the distally based superficial sural flap elevated from the lower two thirds of the posterior calf.
Patients and methods
Twenty-one patients with moderate skin defects and exposed tendon, joint or bone in the lower one third of the leg and foot were treated with distally based superficial sural flaps over a period of 14 months, from June 1994 to October 1995, at the Al-Babtain Center for Plastic, Reconstructive Surgery and Burns, Kuwait.
The mean age of the patients was 20 years (range 4485 years). The female to male ratio was 1 :2. Table 1 summarises the causes of the defects. The majority of the patients had defects due to trauma. The size of the flap varied from 3 x 4 cm to 20 x 8 cm. In 18 patients the flap was fasciocutaneous and in 3 cases it was a fascial flap covered with skin graft. Defects over the heel were covered in 8 cases, lateral malleolus in 2 cases, medial malleolus in 1 case, dorsum of the foot and anterior ankle region in 8
383

384
Table 1 Clinical details
British Journal of Plastic Surgery
Case Age no. (years) Sex
1 38 2 21 3 8 4 16 5 85 6 5
I 18 8 6
9 23 10 40
11 12 13 14
15 6
16 45 17 30 18 6
19
20 21
9
19 23
M M F M M M
F M
M M
F M M M
F
M F M
F
M M
Cause of Site of Flap size Associated defect defect (cm) problems Complications
Neurotrophic ulcer L. heel Pressure sore R. lat. malleolus Trauma R. lat. malleolus Trauma L. medial heel Diabetic gangrene R. heel Trauma Dorsum of L. foot
Trauma L. medial heel Trauma R. lateral foot
12x8 3x4 4x5 6x4 8x5 8x5
(fascia) 6x4 9x4
Postburn contrature Dorsum of L. foot 15 x 10 Trauma R. lower leg 11 x8
Trauma R. anterior ankle 3x4 Postburn contracture Dorsum of L foot 9x5 Trauma Dorsum of L. foot 9x6 Trauma Dorsum of L. foot 11x6
Trauma L. anterior ankle 1x5
Trauma R. heel Trauma R. heel Trauma Dorsum of L. foot
Trauma Dorsum of L. foot
Trauma R. heel Bedsore L. heel
5x3 8x7 5x3
(fascia) 20 x 8 (fascia)
8x7 7x5
No No No No No No No No Diabetes mellitus Failed No No
Fracture OS calcis Amputated 4th, 5th toes
No Fractures tibia and fibula, chronic renal failure, hypertension No No No Fractures metatarsals, open joints, fractures tibia and fibula Fractures tibia and fibula, mid third No Fracture OS calcis No
No Partial loss of distal skin No No
No No No No
No
No No No
Shaved bones No
Fracture OS calcis No No No
cases, lateral side of foot in 1 case and lower tibia in 1 case.
8 patients had underlying fractures. One of the patients had had diabetes mellitus for 30 years and one had chronic renal failure with uremia and hypertension.
Operative technique
The operative technique is very well described in previous publications.‘9,20,24 We describe it briefly here, highlighting some of the important operative steps. After marking of the axis of the flap, which is the course of the medial sural nerve, the flap is outlined according to the size of the defect and distance from it, along the posterior lower two thirds of the leg. The pivot point is 5 cm above the lateral malleolus, the location of the lowermost perforator from the peroneal artery. The pedicle, which contains the small saphenous vein, sural nerve and median superficial sural artery, is exposed through a zig-zag incision and raised with a small cuff of fascia around it, up to the level of the outlined flap. The distal and lateral margins of the flap are incised through the skin and deep fascia. At the distal end of the flap, the median superficial sural artery, small saphenous vein and medial sural nerve are divided and the vessels ligated. The deep fascia is sutured to the skin island and elevated from the muscles, making sure that the vessels and the nerve are included in the flap. The pedicle is freed to the level above the lowermost peroneal perforator in the posterolateral intermuscu-
lar septum. If the flap easily reaches the defect, it is not necessary to visualize the main perforator. However, in cases where a longer pedicle is needed for the coverage of more distant defects, the posterior intermuscular septum is entered and the peroneal perforator itself mobilised, which gives some additional length to the pedicle.
The flap is transferred to the defect either through a skin tunnel or by incising the skin bridge. The flap donor site is closed directly, if it is less than 3-4 cm wide, otherwise a skin graft is applied. If a thinner flap is required or cosmesis of the posterior calf is to be preserved, a flap of fascia alone can be raised and covered with a skin graft.
Results
18 flaps survived completely. In two cases, where the flap was used to resurface the dorsum of the foot and toes, necrosis of the distal part of skin only occurred. The necrotic part of the skin was debrided and the fascia covered with a split thickness skin graft. In one case, the flap failed completely. This patient was an 85year-old male, with a history of uncontrolled diabetes for 30 years and with diabetic gangrene over the heel. He had undergone femoropo- pliteal bypass surgery prior to the reconstruction of the heel defect. After debriding the flap and part of the calcaneum, satisfactory granulation tissue was obtained to support the skin graft. Venous congestion and long lasting oedema of the flap were noticed in two cases.
Distally based superficial sural flap 385
Case reports
Case 1
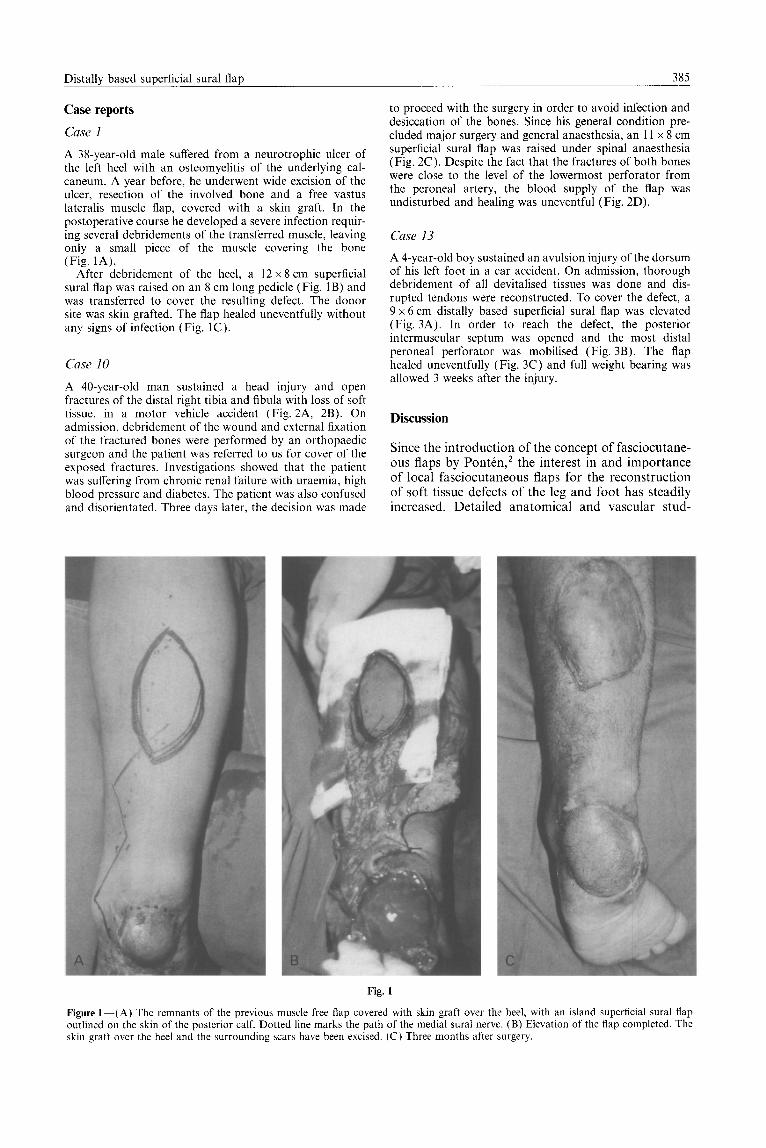
A 3%year-old male suffered from a neurotrophic ulcer of the left heel with an osteomyelitis of the underlying cal- caneum. A year before, he underwent wide excision of the ulcer, resection of the involved bone and a free vastus lateralis muscle flap, covered with a skin graft. In the postoperative course he developed a severe infection requir- ing several debridements of the transferred muscle, leaving only a small piece of the muscle covering the bone (Fig. 1A).
After debridement of the heel, a 12 x 8 cm superficial sural flap was raised on an 8 cm long pedicle (Fig. 1 B) and was transferred to cover the resulting defect. The donor site was skin grafted. The flap healed uneventfully without any signs of infection (Fig. 1C ).
Case 10
A 40-year-old man sustained a head injury and open fractures of the distal right tibia and fibula with loss of soft tissue, in a motor vehicle accident (Fig. 2A, 2B). On admission, debridement of the wound and external fixation of the fractured bones were performed by an orthopaedic surgeon and the patient was referred to us for cover of the exposed fractures. Investigations showed that the patient was suffering from chronic renal failure with uraemia, high blood pressure and diabetes. The patient was also confused and disorientated. Three days later, the decision was made
to proceed with the surgery in order to avoid infection and desiccation of the bones. Since his general condition pre- cluded major surgery and general anaesthesia, an 11 x 8 cm superficial sural flap was raised under spinal anaesthesia (Fig. 2C). Despite the fact that the fractures of both bones were close to the level of the lowermost perforator from the peroneal artery, the blood supply of the flap was undisturbed and healing was uneventful (Fig. 2D).
Case 13
A 4-year-old boy sustained an avulsion injury of the dorsum of his left foot in a car accident. On admission, thorough debridement of all devitalised tissues was done and dis- rupted tendons were reconstructed. To cover the defect, a 9 x 6 cm distally based superficial sural flap was elevated (Fig. 3A). In order to reach the defect, the posterior intermuscular septum was opened and the most distal peroneal perforator was mobilised (Fig. 3B). The flap healed uneventfully (Fig. 3C) and full weight bearing was allowed 3 weeks after the injury.
Discussion
Since the introduction of the concept of fasciocutane- ous flaps by PontCn,’ the interest in and importance of local fasciocutaneous flaps for the reconstruction of soft tissue defects of the leg and foot has steadily increased. Detailed anatomical and vascular stud-
Fig. 1
Figure l-(A) The remnants of the previous muscle free flap covered with skin graft over the heel, with an island superficial sural flap outlined on the skin of the posterior calf. Dotted line marks the path of the medial sural nerve. (B) Elevation of the flap completed. The skin graft over the heel and the surrounding scars have been excised. (C) Three months after surgery.

386 British Journal of Plastic Surnerv
Fig. 2
Figure2-(A) Skin defect on the anterior side of the right lower leg, with exposed tibia1 fracture. (B) X-ray showing fractures of the tibia and fibula. (C) 11 x 8 cm distally based sural flap elevated on narrow pedicle. (D) Healed flap, one month after the injury.
ies19,21,22 have shown rich suprafascial vascular com- munications between longitudinally oriented direct arteries and deep main arteries through musculo- and septocutaneous perforators. Furthermore, after pass- ing through the fascia, the septocutaneous perforators have a radial pattern of branches which anastomose in transverse and longitudinal directions with similar
perforators arising above and below in the same septum, forming a longitudinal anastomotic arcade.22 These vascular connections between the fascia and the skin on one side and the main arteries on the other, via septo- and musculocutaneous perforators, make each of the perforators a potential pivot point for a pedicle, provided it is constant.25 This enables

Distallv based sunerficial sural flan 387
Fig. 3
Figure 3-(A) Defect of the skin after debridement and reconstruction of the lacerated tendons. The distally based superficial sural flap has been elevated. (B) The posterior intermuscular septum opened and the lowermost perforator from the peroneal artery mobilised (tape placed under the perforator). (C) Good contour of the flap, 3 weeks after surgery.
surgeons to design flaps with pedicles based not only proximally,3.4 as originally described by Ponten, but also distally6~14,19,20.24,26 or even in a transverse direc- tion.5 Distally based flaps are, in our opinion, superior to the proximally based flaps for reconstruction of the lower third of the leg due to their better arc of rotation and their donor sites being more suitable for skin grafting. Two types of distally based flaps have been described. One, based on perforators from one of the three major arteries,lzm14 which has the major disadvantage of requiring division of the trunk artery, and the other one, based on one or more perforators and their suprafascial connections.
Various types of distally based flaps have been reported, based on perforators from the posterior tibia1 artery,’ the peroneal artery6,‘0,“~‘9,20~24~26 or both’.’ and raised as island, peninsular, de-epi- thelialised turn-over flaps’,” or turn-over fasciosub- cutaneous flaps.’
In this paper, we report on the flap originally described by Masquelet et a1.19 in 1992 and sub- sequently used by Hasegawa et a1.20 and Hyakusoku et a1.24 The flap is similar to one described by Donski and Fogdestam‘j except that it is pivoted on a huge and constant anastomosis from the peroneal artery, located more distally. This gives an additional length to the pedicle and increases the rotation of the flap. Due to the anastomosis between the peroneal artery perforator and the longitudinally oriented median superficial sural artery, this type of flap could be considered an axial pattern flap.
Shalaby26 described a flap based on the same peroneal perforator but with the skin island taken more laterally, overlying the posterolateral intermus-
cular septum. The vascular axis of this flap is an anastomotic arcade formed by longitudinal connec- tions between neighbouring septocutaneous vessels in the same septum. 22 The flap has a short pedicle and although rotation of 180 degrees is possible, there is concern about the resulting twisting of the pedicle. It seems that this flap is more suitable for covering defects above rather than below the ankle joint. The posterolateral malleolar flap described by Oberlin et a12’ is a peninsular flap with its pivot point at the tip of the lateral malleolus. It is obvious that the major peroneal perforator, which is the base of our flap, has to be sacrificed. The vascularity of the posterolateral malleolar flap is provided by smaller peroneal perforators nourishing the medial sural nerve and by the skin pedicle. Lacking a strong arterial input, the flap is relatively short and can only be used for cover of defects around the lateral mal- leolus and the posterior heel, with unsightly dog-ears in cases with major rotation of the flap.
The distally based lateral supramalleolar flap, reported also by Masquelet et al.,” derives its vascu- larity through the anterior branch of the peroneal artery at approximately the same level as in our flap. Tedious dissection, a shorter pedicle and a less favour- able flap donor site for skin grafting make this flap, in our opinion, inferior to a distally based superficial sural flap for cover of defects of the lower leg.
In our series of 21 patients we had one complete failure and two partial failures of skin only, in the distal part. As mentioned earlier, complete failure happened in an 85-year-old diabetic patient who had femoropopliteal bypass surgery prior to the recon- struction of his heel defect. Since then, a Doppler is

388 British Journal of Plastic Surgery
routinely used in all patients who may have under- lying vascular disease or injury to the bones in the distal third of the leg. The Doppler is useful for marking of the pivot point of the flap preoperatively, but is not compulsory in otherwise healthy patients. Although the perforator is constant and can be easily traced, we could not asses the patency of the com- munications with the median superficial sural artery and the perforator with the Doppler.
Partial failure in the most distal part of the flap occurred in two cases, in which the dorsum of the foot and the toes were covered. In both cases the flap was extended to the proximal third of the calf in order to reach the defect. The partial flap failure confirms the opinion of Masquelet” that the flap is safe only if taken in the lower two thirds of the posterior leg along the suprafascial course of the median superficial sural artery. In similar cases after- wards, additional length of the pedicle was gained through sufficient mobilisation of the peroneal perfor- ator rather than through extension of the flap proximally.
Three patients in our series had fractures of both the tibia and fibula, two in the lower third and one in the middle third. There was no vascular compro- mise of the flap in any of these patients.
The advantages of the distally based superficial sural flap are: easy, quick and safe surgery in one stage, preservation of major arteries and minimal morbidity for the patient. Due to its long and narrow pedicle, with its vascular axis including the largest direct artery of the posterior calf and the strongest peroneal perforator at its pivot point, the distally based superficial sural flap has the widest range of rotation among other similar flaps with superior vascularity.
The major disadvantage is an unsightly scar over the posterior calf in cases where a skin island is included in the flap and the sacrifice of the sural nerve. The problem of ugly scars could be solved by raising only a fascial flap and covering it with skin graft as we did in three cases. An alternative is subsequent partial excision of the grafted donor area, thus reducing it to a linear scar. Although some authors6s24 reported sparing the sural nerve during elevation of similar flaps, we found it too risky for the blood supply of the flap and unnecessary.
We believe that the distally based superficial sural flap is an excellent choice for covering uncomplicated defects of the lower tibia, ankle region and dorsum of the foot where thin, pliable skin is needed. Having the deep fascia included in the flap makes the flap durable and suitable for the coverage of heel defects, as well. For severely infected wounds with loss of bones or osteomyelitic cavities requiring well vascu- larised, bulky flaps, priority should be given to a free tissue transfer.
Acknowledgement
We are extremely grateful to Prof. Christopher J. Ford for helping us in the correction of the manuscript.
References
1. Serafin D, Georgiade NG, Smith D. Comparison of free with pedicled flaps for coverage of defects of leg or foot. Plast Reconstr Surg 1911; 59: 492-9.
2. Ponttn B. The fasciocutaneous flap: its use in soft tissue defects of the lower leg. Br J Plast Sure 1981: 34: 215-20.
3. Tolhurst DE, Haeseker B, Zeem& RJ.‘The development of the fasciocutaneous flap and its clinical applications. Plast Reconstr Surg 1983; 71: 597-605.
4. Barclay TL, Cardoso E, Sharpe DT, Crockett DJ. Repair of lower leg injuries with fascia-cutaneous flaps. Br J Plast Surg 1982; 35: 127-32.
5. Thatte RL, Laud N. The use of the fascia of the lower leg as a roll-over flap: its possible clinical applications in recon- structive surgery. Br J Plast Surg 1984; 37: 88892.
6. Donski PK, Fogdestam I. Distally based fasciocutaneous flap from the sural region. Stand J Plast Reconstr Surg 1983; 17: 191-6.
7. Amarante J, Costa H Reis J, Soares R. A new distally based fasciocutaneous flap of the leg. Br J Plast Surg 1986; 39: 338-40.
8. Gumener R, Zbrodowski A, Montandon D. The reversed fasciosubcutaneous flap in the leg. Plast Reconstr Surg 1991; 88: 1034-41.
9. Carriquiry CE. Heel coverage with a deepithelized distally based fasciocutaneous flap. Plast Reconstr Surg 1990; 85: 116-9.
10. Numanoglu A, Esemenli T, Uzunismail A, Bas L. The ‘lazy-V de-epithelialised turn-over fasciocutaneous flap in the recon- struction of skin defects after tendo Achilles repair. Br J Plast Surg 1992; 45: 550-3.
11. Masquelet A, Beveridge J, Romana C, Gerber C. The lateral supramalleolar flap. Plast Reconstr Surg 1988; 81: 74-81.
12. Yoshimura M, Imura S, Shimamura K, Yamauchi S, Nomura S. Peroneal flap for reconstruction in the extremity: prelimi- nary report. Plast Reconstr Surg 1984; 74: 402-9.
13. Wee JTK. Reconstruction of the lower leg and foot with the reverse-pedicled anterior tibia1 flap: preliminary report of a new fasciocutaneous flap. Br J Plast Surg 1986; 39: 327-37.
14. Hong G, Steffens K, Wang FB. Reconstruction of the lower leg and foot with the reverse pedicled posterior tibia1 fasciocutaneous flap. Br J Plast Surg 1989;42: 512-16.
15. Fayman MS, Orak F, Hugo B, Berson SD. The distally based split soleus muscle flap. Br J Plast Surg 1987; 40: 20-6.
16. Magee WP, Gilbert DA, McInnis WD. Extended muscle and musculocutaneous flaps. Clin Plast Surg 1980; 7: 57-65.
17. Swartz WM. Mears DC. The role of free-tissue transfers in lower extremity reconstruction. Plast Reconstr Surg 1985; 76: 364-13.
18. Rajacic N, Lari AR, Khalaf ME, et al. Free flaps for the treatment of avulsion injuries in the feet. J Pediatr Orthop 1994; 14: 522-5.
19. Masquelet AC, Romana MC, Wolf G. Skin island flaps supplied by the vascular axis of the sensitive superficial nerves: anatomic study and clinical experience in the leg. Plast Reconstr Surg 1992; 89: 1115-20.
20. Hasegawa M, Torii S, Katoh H, et al. The distally based superficial sural artery flap. Plast Reconstr Surg 1994; 93: 1012-20.
21. Haertsch P. The blood supply to the skin of the leg: a post- mortem investigation. Br J Plast Surg 1981; 34: 470-7.
22. Carriquiry C, Costa MA, Vasconez LO. An anatomic study of the septocutaneous vessels of the leg. Plast Reconstr Surg 1985; 76: 354461,
23. Fachinelli A, Masquelet A, Restrepo J, et al. The vascularized sural nerve. Int J Microsurg 1981; 3: 57-62.
24. Hyakusoku H, Tonegawa H, Fumiiri M. Heel coverage with a T-shaped distally based sural island fasciocutaneous flap. Plast Reconstr Surg 1994; 93: 872-6.
25. Masquelet A. The posterolateral malleolar flap of the ankle: a distally based sural neurocutaneous flap-Report of 14 cases (Discussion). Plast Reconstr Surg 1995; 96: 406-7.
26. Shalabv HA. The distallv based neroneal island flan. Br J Plast Surg 1995; 48: 2336. - _
27. Oberlin C, Azoulay B, Bhatia A. The posterolateral malleolar flap of the ankle: a distally based sural neurocutaneous flap- Report of 14 cases. Plast Reconstr Surg 1995; 96: 400-5.

Distally based superficial sural flap 389
The Authors
Nebojsa Rajacic MD, Assistant Professor, Department of Surgery, Faculty of Medicine, Kuwait University.
Consultant Plastic Surgeon, Al-Babtain Center for Plastic, Reconstructive Surgery and Burns
Maber Darweesb MB BS, Registrar in Plastic Surgery. Kolady Jayakrisbnan MB BS, Registrar in Plastic Surgery. Raj Kumar Gang MB BS, FRCS, Senior Registrar in Plastic
Surgery.
Correspondence to Nebojsa Rajacic MD, Assistant Professor, Department of Surgery, Faculty of Medicine, Kuwait University, P.O. Box 24923 Safat, 13110 Kuwait.
Paper received 24 November 1995. Accepted 17 April 1996, after revision.
Al-Babtain Center for Plastic, Reconstructive Surgery and Burns, Kuwait University, Kuwait.
Sinisa Kojic MD, Specialist in Plastic Surgery, Medical Center, Foca-Srbinje, Bosnia and Herzegovina.





![Hyperbaric oxygen therapy and surgical delay …the dorsum of the foot, the medial and lateral arches, and all regions of the heel. The reverse sural flap [3,4] is raised from the](https://img.dokumen.tips/doc/110x75/5f7b32540d8f777e9871b889/hyperbaric-oxygen-therapy-and-surgical-delay-the-dorsum-of-the-foot-the-medial.jpg)























