Embed Size (px)
Citation preview
The Ankle
Anatomy &
INJURIES
Bone Stability
• Tibia, Fibula, Talus
• Form the “Ankle Mortise”
• Very stable joint
• Most injured joint

Difference in Stability
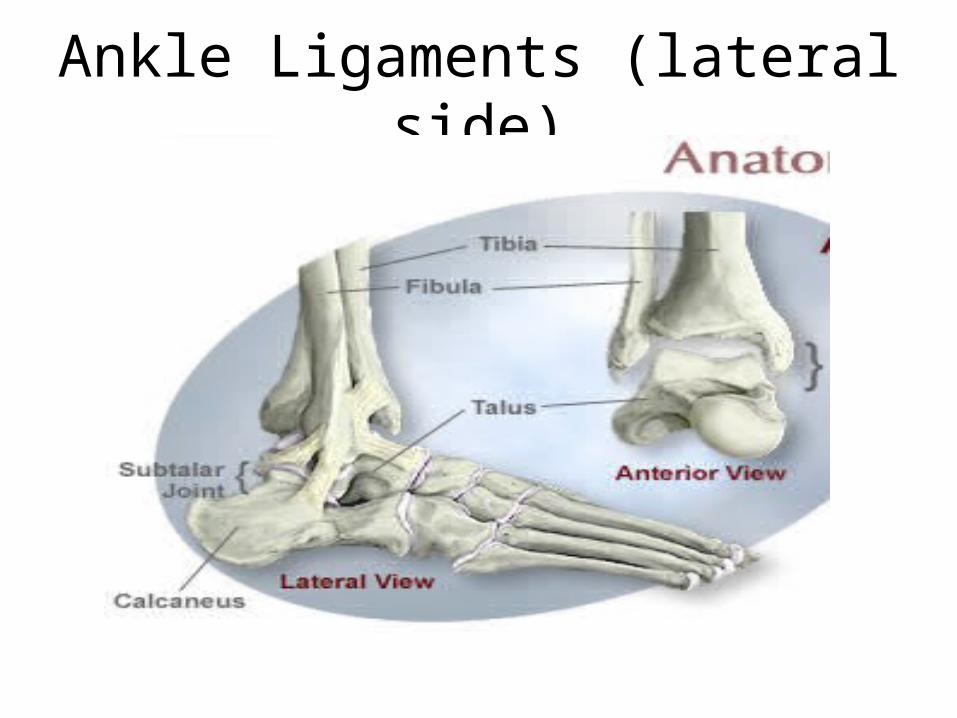
Ankle Ligaments (lateral side)
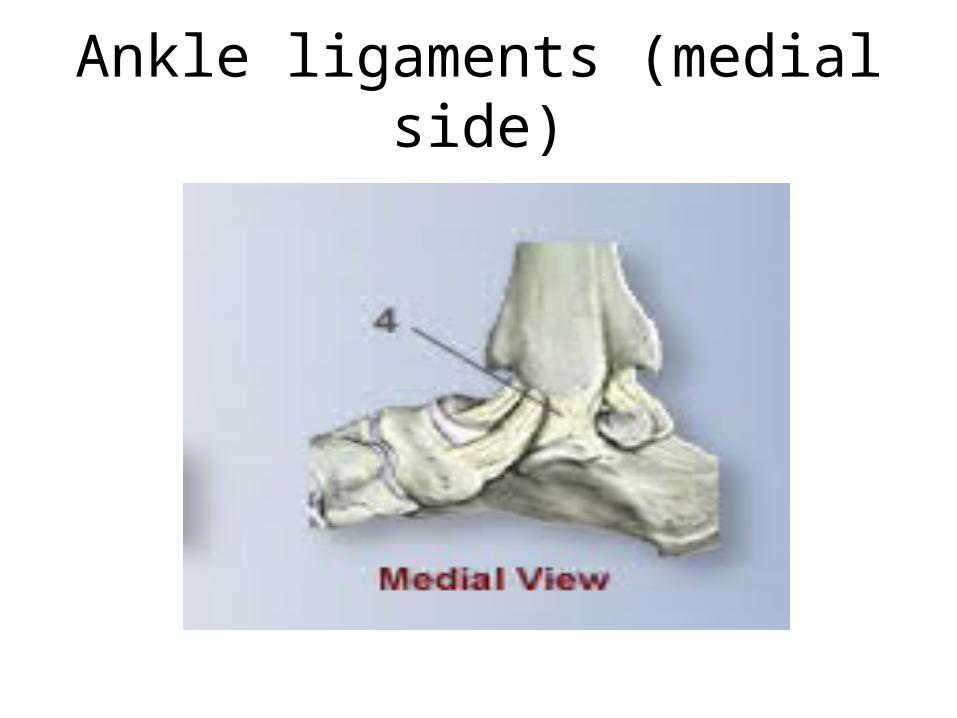
Ankle ligaments (medial side)
Ankle Muscles
• Extensor / Flexor digitorum
• Extensor / Flexor hallux
• Tibialis Anterior – Dorsiflex and invert
• Tibialis Posterior – Plantarflex and invert
• Peroneal longus/brevis – Plantarflex and evert
• Gastrochnemius/soleus – Plantarflex

Ankle Injuries
• Sprains
• Strains
• Contusions
• Fractures
• Dislocations / Subluxations
• Tendonitis
• Bursitis
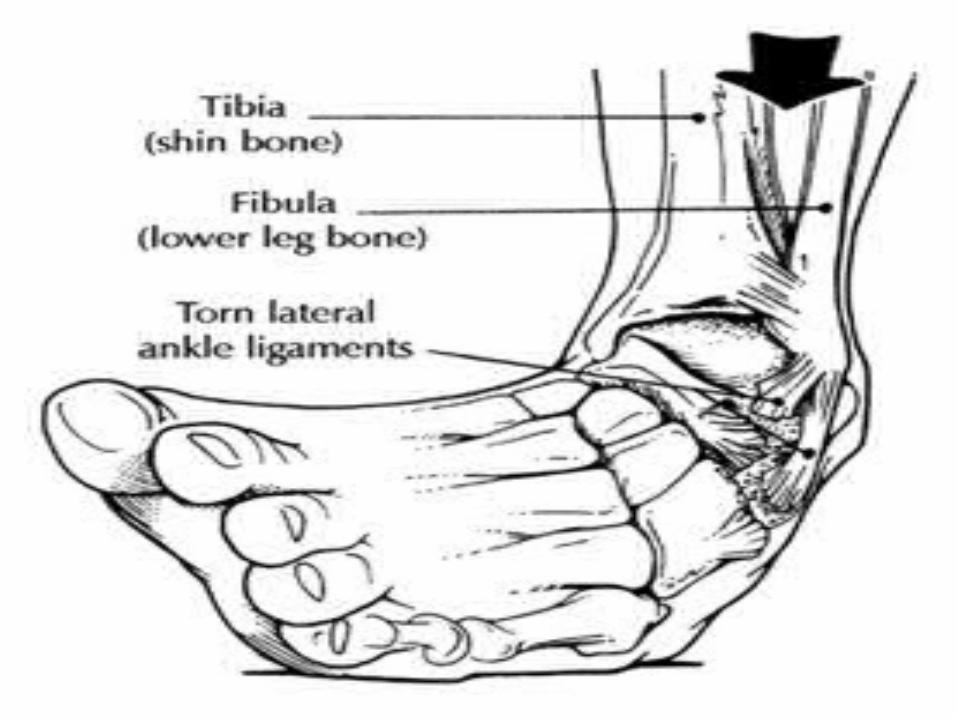
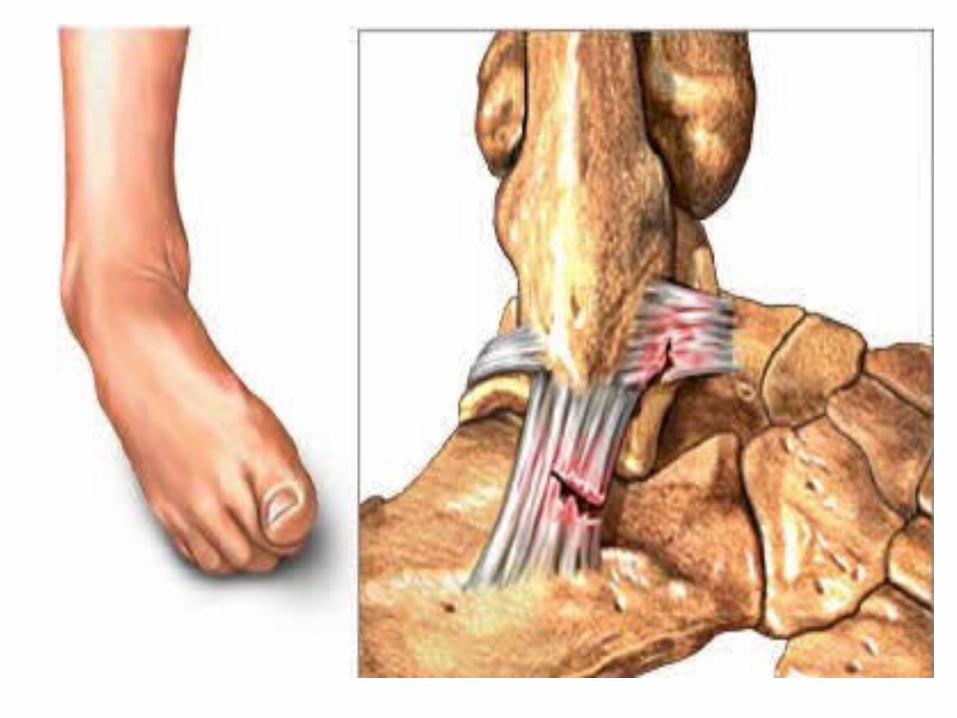
Inversion Sprains
• Most common sports injury
• Plantarflexion and Inversion
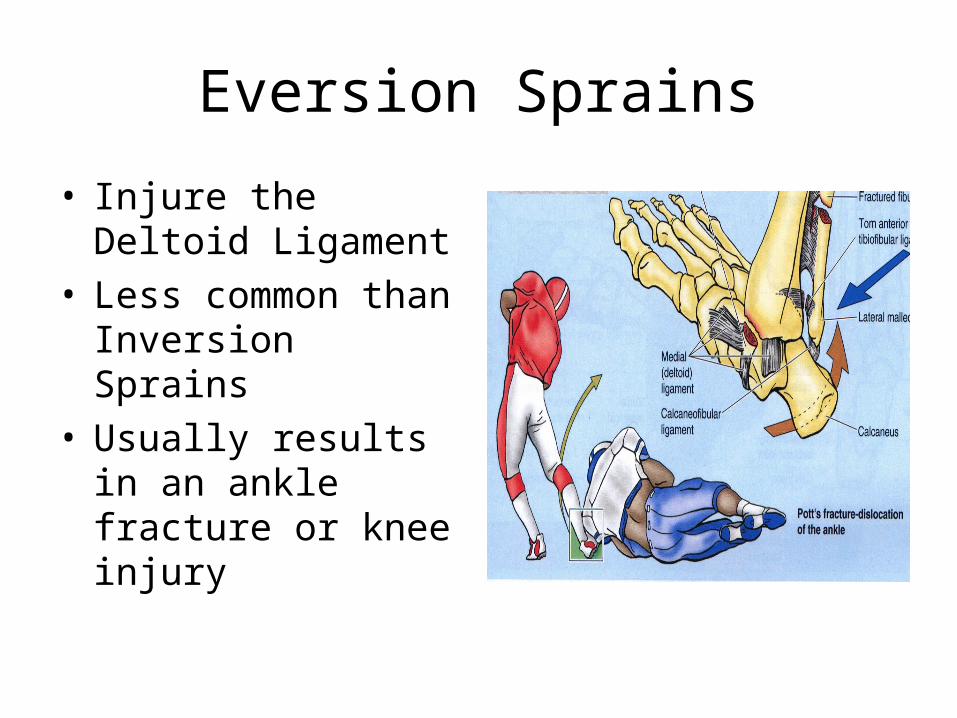
Eversion Sprains
• Injure the Deltoid Ligament
• Less common than Inversion Sprains
• Usually results in an ankle fracture or knee injury

“High Ankle Sprain”
• Syndesmotic Joint
• Tibiofibular ligaments
• Injury mechanism – ankle external rotation
• Very long recovery time
• Difficult rehab (weight bearing)

Kicking injuries?


Running Injuries
Lifting Injuries
Contact Sport Injuries

Care for Ankle Injuries
• R – rest
• I - ice
• C – compression
• E - elevation

Ankle Rehabilitation
• Decrease Swelling• Increase ROM
– Passive / Active ROM
• Increase Strength– Isometric followed by isotonic
• Increase Weight Bearing• Increase Achilles Flexibility• Increase Function• Return to Activity





























