Embed Size (px)
Citation preview

453
28 Pandemic p reparedness and r esponse Jonathan S. Nguyen-Van-Tam 1 and Joseph Bresee 2 1 Health Protection and Infl uenza Research Group , University of Nottingham Medical School , City Hospital , Nottingham , UK
2 Epidemiology and Prevention Branch, Infl uenza Division , Centers for Disease Control and Prevention , Atlanta , GA , USA
Historical c ontext of h ealth e mergency p lanning and r esponse
Ancient h istory
Early historical accounts of outbreaks of infectious diseases have not only described the clinical and path-ologic features in humans, but also the complex inter-actions between such outbreaks and human society. The etiology of the Plague of Athens, 430–427 BC, is unknown, but the historian and writer Thucydides clearly describes the breakdown of social order, dis-ruption of military operations, spontaneous social distancing, abandonment of normal burial rites in the face of massive population mortality, person-to-person transmission (often associated with care of the sick), excess mortality among physicians, and spread to neighboring territories; from which we can con-clude that there was no organized response to this severe epidemic [1] . Nevertheless, the acquisition of immunity after recovery from infection is clearly documented, along with the observation that such individuals could safely care for the sick without risk of personal harm, suggesting early insight into how an organized response could prove advantageous.
The re-emergence of bubonic plague ( Yersinia pestis ) or “Black Death” in Europe in 1345 produced the fi rst notions that the impact of infectious diseases could be mitigated through organized response. The city of Venice implemented quarantine measures in
1374 by holding ships offshore for 40 days and through the isolation of affected families [2] .
Local and n ational c oordination
Possibly the fi rst recognition that there should be an overall coordinated response to outbreaks or epidem-ics of infectious diseases came in 1493 when the Italian city of Florence established a board of offi cials charged with responding to such incidents. Under its auspices, public gatherings were at one point banned to prevent spread the spread of plague from Rome. During the sixteenth century permanent health com-mittees were established in many European cities, whose purpose was to monitor and control the spread of infectious diseases [3] .
Supra- n ational c oordination
Besides the need for an organized local response to infectious diseases, clear recognition of the need for a coordinated supra-national response resulted in the fi rst International Sanitary Conference in Paris, 1851, the objective of which was to harmonize quarantine regulations across European nations. Subsequently, an Offi ce for International Public Hygiene ( OIHP ) was established in 1907; but it was in the aftermath of World War II that the World Health Organization ( WHO ) was founded in 1948.
Textbook of Infl uenza, Second Edition. Edited by Robert G. Webster, Arnold S. Monto, Thomas J. Braciale, and Robert A. Lamb.© 2013 John Wiley & Sons, Ltd. Published 2013 by John Wiley & Sons, Ltd.

CHAPTER 28
454
a clear reminder that the last pandemic virus had emerged almost 30 years previously and of the endur-ing threat to humans from the avian infl uenza reser-voir in wild birds [7] . While effi cient spread of A(H5N1) infection from person-to-person has not occurred to date, the emergence of a different novel zoonosis, severe acute respiratory syndrome ( SARS ) in late 2002, provided a different perspective, with effi cient person-to-person transmission and rapid international spread via the medium of air travel [8] . When infl uenza A(H5N1) re-emerged in South-East Asia in 2003 [9] , and the virus became endemic in poultry fl ocks in several, mainly South-East Asian, countries it became clear that substantial efforts were needed to improve global infl uenza pandemic preparedness.
Although little pandemic preparedness had been undertaken anywhere in the world prior to 2004, a few countries had developed pandemic preparedness plans earlier; for example, the United Kingdom ’ s fi rst national plan was published in 1997, and the fi rst WHO pandemic plan came out in 1999. However, the now familiar, whole-of-society, multisectoral approach was most clearly established upon publica-tion of the second WHO pandemic plan and its asso-ciated checklist in 2005 [10,11] .
Pandemic p reparedness p rinciples and a ssumptions p rior to 2009
Pandemic preparedness is predicated on the emer-gence of an infl uenza virus that is suffi ciently novel that large sections of the global population have no pre-existing immunity. In addition, the virus must be readily transmissible from person-to-person and cause clinical illness. Based on the experience in 1918 when the case–fatality rate due to the pandemic A(H1N1) virus was about 2.5%, and the 63% case–fatality rate observed due to A(H5N1) between 2003 and 2008, it was assumed by many authorities that a pandemic virus would be more virulent than seasonal infl uenza. However, the pandemic viruses of 1957 and 1968 infl icted a far lower case fatality of around 0.1% [12] , leaving a wide range of uncertainty for planners. The data on clinical attack rates in the pandemics of the twentieth century offered more con-sistent estimates around 25–30% [13] . Similarly, the literature on geographic spread of past pandemics revealed that in both 1957 and 1968 effective global
Preparedness and r esponse to p andemics of the t wentieth c entury
During the 1918 pandemic, well-organized responses were seen throughout the world, mainly coordinated at national (governmental) level. In almost all juris-dictions the focus was on public health measures such as respiratory etiquette, case isolation, quarantining of contacts, school closures, limitation or prohibition of public gatherings, and border closures; most of these with limited evidence of effectiveness [4] . This emphasis may have arisen in part due to the absence of antiviral drugs and antibiotics and lack of under-standing about the etiology of infl uenza, forcing a reliance on simple preventive measures.
By 1957, infl uenza vaccines had been available for more than a decade and the focus in national responses, especially in the United States and United Kingdom had switched towards vaccination, with healthcare and “essential” workers prioritized in both countries. However, vaccine arrived too late to be maximally effective and was in short supply com-pared to population size [5] . None whatsoever was available in resource-poor countries. The same prin-ciples were followed in 1968 although vaccine was slightly more widely available.
Although it is not possible to comment in detail on the A(H1N1) swine infl uenza incident at Fort Dix, United States, in 1976 (see Chapter 2 ), this was a pandemic “false alarm” that resulted in a massive vaccination campaign during which 25% of the US population was vaccinated ( > 40 million persons), before the program was halted due to an excess of cases of Guillain–Barré syndrome temporally associ-ated with the vaccine. The program did, however, adhere to the important principle of early vaccine intervention, although the pandemic threat never fi nally materialized. Unfortunately, it also did much to undermine public confi dence in the organized gov-ernmental response to infl uenza threats.
Modern d ay p andemic p reparedness
Emergence of p andemic p reparedness a ctivities
In 1997 an outbreak of highly pathogenic avian infl u-enza A(H5N1) in humans in Hong Kong resulted in 18 cases of whom six died [6] . The incident served as
PANDEMIC PREPAREDNESS AND RESPONSE
455
operational plans can be established and tested. Although widely different formats and approaches may be pursued, all require fi rm political support and dedicated fi nancial resources. As countries are hetero-geneous in terms of how they are organized adminis-tratively (e.g., centralized versus federal systems, including health services and the extent to which these lie in the private or public sectors), many dif-ferent approaches to pandemic preparedness exist but all are underpinned by specifi c common elements described below.
Specifi c e lements of p andemic p reparedness
Planning for e pidemiologic m onitoring and s urveillance of a p andemic
A fundamental requirement for an effective pandemic response is the ability to conduct appropriate disease and viral surveillance, and to gather additional data required for decision-making from targeted fi eld investigations. The establishment of the WHO World Infl uenza Center in 1947 (now the Global Infl uenza Surveillance and Response System ; GISRS ), was a response to concerns that new pandemic strains be detected as quickly as possible [14,15] . The 1957 A(H2N2) pandemic was the fi rst in which both virus and disease were identifi ed and monitored during its global spread [5] . Since that time, ensuring robust surveillance systems has been a centerpiece of all pandemic plans [16] .
Even so, the global capacity to conduct viral and disease surveillance capable of detecting and monitor-ing an emergent pandemic remained limited during the decades following the A(H2N2) pandemic. During this period, the primary goal shaping expan-sion of global infl uenza surveillance was to gather and characterize infl uenza viruses in support of sea-sonal vaccine production [15] . National surveillance systems that produced data on risk groups, seasonal-ity, and disease burden were mostly confi ned to high-income countries in Asia, Europe, Oceania, and North America. For most countries, laboratory capacity to detect potential pandemic viruses, and the ability to detect and investigate clusters of respiratory illnesses remained inadequate [17] . Interest in infl u-enza surveillance for pandemic readiness increased
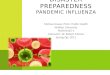
spread from an epicenter in South-East Asia occurred in under 6 months [13] . However, in 2003 SARS spread from Hong Kong to Vietnam, Singapore, and Canada in just 3 weeks, illustrating the potential for modern day air passenger movement to accelerate substantially international spread of a novel respira-tory infection (Table 28.1 ).
The purpose of pandemic preparedness is to plan, organize, and coordinate activities that will be neces-sary to respond to all aspects of a pandemic. A national pandemic plan should serve as an overarch-ing strategy, beneath which sub-national and local
Table 28.1. Basic epidemiologic and virologic assumptions in pandemic preparedness prior to 2009.
Epicenter
• Unknown • On basis of loci of 1957 and 1968 pandemics and
endemicity of A(H5N1) in poultry, considered most likely to be South-East Asia
Subtype
• Unknown • Most worrisome possibility: A(H5N1) due to high
case–fatality rate of sporadic human cases • Other possibilities: A(H7N7), A(H7N2), A(H9N2),
A(H2N2)
Case–fatality rate
• Unknown • Planning ranges from 2.5% (1918-like) to 0.1%
(1968-like) • CFR for avian infl uenza A(H5N1) noted to be circa
60% – assumption this would fall if virus became transmissible between humans
Attack rates
• Clinical attack rate 25–35% (cumulative) • Serologic attack rates roughly twofold higher • Highest attack rates in younger age groups
Transmissibility and spread
• Global spread within 6 months of emergence • International travel restrictions unlikely to slow
spread • Reproductive number R 0 : 1.2–2.0 • Up to three separate pandemic waves over 18-month
period

CHAPTER 28
456
identifi cation of these specifi c data needs, and design-ing and exercising plans to collect them are crucial.
International h ealth r egulations
In 2005, all WHO Member States agreed to become legally bound to a group of regulations intended to ensure that the international community would detect, respond, and share information on acute public health events posing an international health risk and which might require a coordinated interna-tional response [20] . These regulations, the Interna-tional Health Regulations ( IHR ) (2005) came into effect in June 2007. Human infl uenza caused by a new subtype is specifi cally listed as a disease that must be reported under the IHR agreement. IHR (2005) has served as a powerful catalyst for improved sur-veillance and response particularly relevant to coun-tries at higher risk for A(H5N1) outbreaks [21] . Countries are now required to be able to detect infl u-enza viruses, and refer suspicious isolates to WHO collaborating laboratories for further characteriza-tion. Countries also responded by improving pro-cesses to investigate outbreaks and communicate the results to WHO. Following the implementation of IHR (2005) there was a marked increase in data and isolates sent to GISRS. The ability of countries world-wide to detect fi rst cases of A(H1N1)pdm09 and to share epidemiologic data and laboratory samples with WHO was, in part, the result of IHR implemen-tation [21] .
Planning for u se of a ntivirals
The use of antiviral drugs remains a cornerstone of many countries ’ pandemic plans. Because of the time required to create and distribute a pandemic vaccine, antivirals that can treat or prevent infl uenza are attractive tools to limit disease complications, and perhaps infl uenza transmission during a pandemic. Pandemic antiviral strategies have been based on pro-fi les of the available medications, models of potential effects of various approaches, programmatic require-ments, and resources available.
Currently, two classes of antivirals are licensed for treatment or prophylaxis of infl uenza A: the M2 channel blockers (or adamantanes) and the neurami-nidase inhibitor s ( NAI s). While two adamantanes are currently licensed, the propensity of infl uenza A
following the 1997 avian infl uenza A(H5N1) out-break among humans in Hong Kong and was further galvanized by the SARS outbreak and re-emergence of A(H5N1) in 2003.
While all pandemic plans contain substantially similar surveillance goals, the specifi c objectives of surveillance (or uses of surveillance data) will vary between countries and potentially change during the course of a pandemic [16,18] . During the interpan-demic period, surveillance systems must be suffi -ciently sensitive and comprehensive to identify the emergence of a pandemic strain as early as possible, thereby triggering a public health response. Countries also must be able to test reliably for infl uenza and have access to laboratories that can characterize potentially novel infl uenza A strains. During the last decade, growth of WHO ’ s global laboratory surveil-lance network, GISRS, which now includes 123 coun-tries, and the expansion of reverse transcriptase polymerase chain reaction ( RT-PCR ) testing in clini-cal and public laboratories, has dramatically improved the speed with which a future pandemic strain will be detected and confi rmed. Interpandemic surveillance is also used to establish baselines against which pan-demic infl uenza can be compared (for instance, to assess severity). Once a pandemic virus has emerged, disease surveillance must be suffi ciently robust to monitor the geographic spread, changes in epidemio-logic features, severity or impact in a community, and the effect of public health interventions [19] . Viral surveillance systems should monitor changes in the virus that may make medical interventions less effective (e.g., mutations that confer antiviral resist-ance) or would guide vaccine and diagnostic test development.
Strong seasonal infl uenza surveillance systems are critical as foundations for pandemic surveillance. The stress on human and health resources during a pan-demic mainly precludes development of new systems or enrollment of new surveillance sites once a pan-demic has started. Rather, modifi cation of seasonal surveillance systems to provide more timely data (e.g., daily rather than weekly) or more information (e.g., fi ner age strata, additional clinical data) is preferred. Even so, some information needed for a pandemic response is not likely to be available from routine seasonal surveillance. For instance, systems that monitor healthcare delivery or hospital bed availabil-ity may be important for surge planning. Advance

PANDEMIC PREPAREDNESS AND RESPONSE
457
Programs to deliver antivirals during a pandemic are complex given the dispersed geographic nature of pandemic illness (compared with delivery of antibiot-ics following a point-source anthrax exposure, for instance). Planners should exercise distribution and administration in advance of a pandemic. In addition, because effective treatment requires early administra-tion after illness onset, strategies to ensure easy access to treatment in all localities within a country are criti-cal. Antiviral stockpiling and use during a pandemic is complex and expensive, but can result in substan-tial public health benefi ts [27] . A global considera-tion continues to be the equitable distribution of antivirals.
Planning for u se of p andemic v accines
While vaccines are the best tool for the prevention of infl uenza, they will not be available early in a pandemic unless production techniques are vastly improved or a “universal” vaccine is developed. The current steps in producing infl uenza vaccines, whether live, attenuated, or inactivated, require several months, and cannot be initiated until a suitable pan-demic vaccine seed strain is produced following the emergence of a novel virus. Because it is unlikely that seasonal vaccines will provide adequate protection against a newly emergent pandemic strain, planning for pandemic vaccines has taken two approaches: the creation of vaccines based on the pandemic virus once detected; and creation and stockpiling of “pre-pandemic” vaccines based on assumptions about future pandemic strains [28] .
The optimal antigenic match between a pandemic strain and vaccine will be achieved by creating vac-cines specifi cally against the new pandemic strain. This approach is taken in the production of seasonal vaccine and has been used in each pandemic since 1957, but requires several months to progress from strain characterization to vaccine delivery [29] . As a result, vaccination is not currently a viable strategy for mitigating spread or limiting disease at the start of a pandemic.
An approach to reduce the time from pandemic detection to vaccine delivery is to produce and stock-pile pre-pandemic vaccines during the interpandemic period, designed to protect against strains thought to represent a pandemic risk. Many countries and WHO undertook the creation of vaccine stockpiles
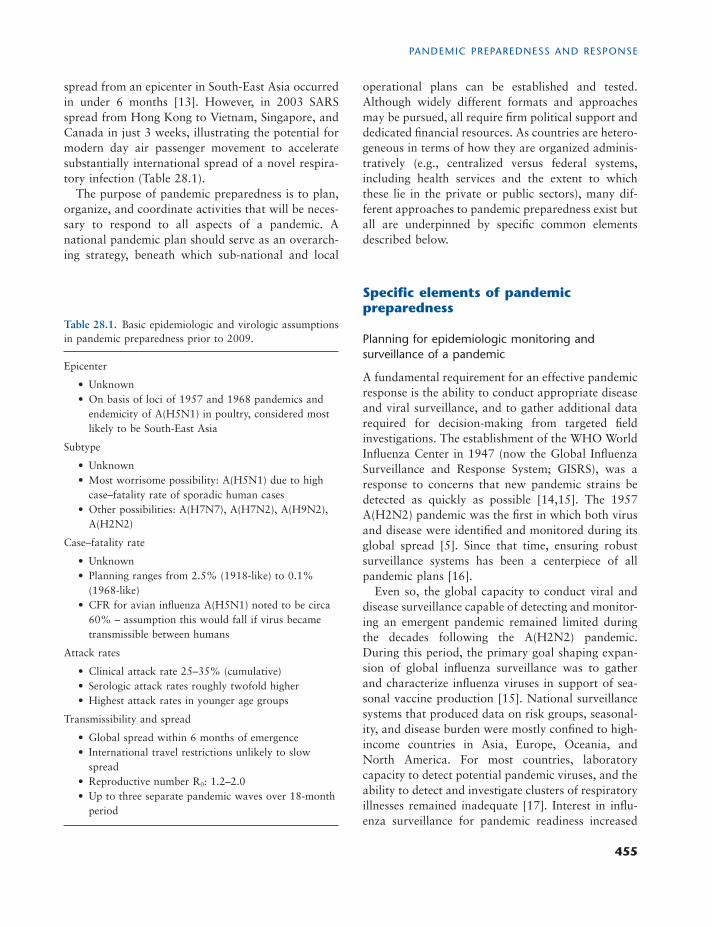
viruses to develop rapid resistance to these agents has limited enthusiasm for including them in pandemic plans [22] . Most plans have focused on use of NAIs, of which two are widely available – oseltamivir and zanamavir. NAIs have been incorporated into national, international, and private stockpiles and were used widely during the 2009 pandemic [23] . Zanamavir use has been more limited than oseltamivir because of its narrower age indication, contraindication for use among persons with some respiratory conditions, and relative complexity of administration. While oseltami-vir resistance was observed in A(H1N1) viruses circu-lating before the 2009 pandemic, resistance among currently circulating viruses (including A(H1N1)pdm09) and A(H5N1) remains uncommon [24] . Even so, the reliance of pandemic plans on NAIs, together with the threat of rapidly developing resistance during a pandemic or the emergence of a resistant pandemic strain, highlight the importance of additional antiviral choices. In addition, the diffi culty of administering oral or inhaled medications to severely ill persons has led to increased testing and emergency use of intrave-nous NAIs. The anticipated worldwide licensure of second generation NAIs should offer options for intravenous administration to severely ill patients and “once only” dosing (Table 28.2 ).
Because NAIs are effective in both treating and preventing infl uenza, a variety of pandemic approaches has been proposed. While strategies that emphasize prophylaxis could produce reductions in overall illness rates [25] , and better preserve critical infra-structures (e.g., prophylaxis of healthcare workers), they require far larger stockpiles for effective imple-mentation than do treatment-based approaches. Most countries ’ plans, therefore, focus on treatment of ill persons, with prophylaxis reserved for specifi c, limited circumstances (e.g., high-risk household members) [18,26] . In some high-income countries, such as the United Kingdom and United States, with large stockpiles, all persons suspected of having a pandemic illness were recommended to be treated. Other countries with more limited stockpiles have chosen to target specifi c groups, either to maximize reduction of severe disease (e.g., persons at high risk for severe infl uenza) or safeguard critical national infrastructure ( CNI ) resiliency. Because decisions on the use of scarce resources have public, political, sci-entifi c, and ethical implications, these deliberations should be systematic and transparent.
CHAPTER 28
458
Table 28.2. Summary of characteristics of drugs licensed for use against infl uenza.
Class M2 channel blockers (adamantanes)
Neuraminidase inhibitors (NAIs)
Agent Amantadine Rimantadine Zanamivir Oseltamivir Peramivir Laninamivir
Trade name(s) Lysovir®, Symadine®
Flumadine® Relenza® Tamifl u® Rapiacta® Peramifl u®
Inavir®
Infl uenza activity A viruses only A viruses only A and B viruses A and B viruses
A and B viruses A and B viruses
Route of administration
Oral Oral Oral inhalation (dry powder)
Oral Intravenous Oral inhalation (dry powder)
Use for treatment Yes Yes Yes Yes Yes a Yes
Use for prophylaxis
Yes Yes Yes Yes No No b
Pandemic application
Unreliable choices for pandemic application due to propensity for rapid emergence of resistance Adverse event profi le for amantadine unfavorable compared with NAIs
Highly suitable provided patient can operate delivery device and make suffi cient inspiratory effort to inhale dry powder Twice daily dosing (treatment) necessitates good compliance Large pack size increases warehousing space for stockpiles
Highly suitable general choice; available in capsules and pediatric suspension Twice daily dosing (treatment) necessitates good compliance Risk of resistance emergence (H275Y mutation) in viruses of N1 moiety
Unsuitable for use in ambulatory care Most suitable and possibly “best choice” in severely ill (ventilated) patients who cannot be given zanamivir and who can only be given oseltamivir by nasogastric instillation
Similar use issues as for zanamivir Once and only dosing offers “fi re and forget” simplicity; may be useful in low compliance populations (e.g., homeless) or situations where facilities or living conditions are basic (military, refugee settings, etc.)
a Intravenous route of administration makes it most suitable for use in hospital for severely ill patients. b Not yet licensed for prophylaxis (April 2012); theoretically likely to be effective for post-exposure prophylaxis. Source: Adapted with permission from Van-Tam J, Lim WS. Pharmaceutical interventions. In: Pandemic Infl uenza , 2nd edn. J. Van-Tam and C. Sellwood, editors. 2012, Wallingford: CABI, p. 123.

PANDEMIC PREPAREDNESS AND RESPONSE
459
potency. The drawbacks of the approach are several. First, because a person would receive a vaccine designed well before the identifi cation of a pandemic strain, the risk that the pandemic strain will be anti-genically different is relatively high; so, reduced pro-tection or priming might be conferred. Second, the ethical implications of exposing a person to a vaccine for which there is currently minimal risk of wild-type virus exposure must be resolved. Finally, policies for the use of these vaccines, such as target groups, must be settled. While some countries have licensed A(H5N1) vaccines that could be used for such pur-poses, no pre-pandemic vaccination program has so far been implemented.
Planning for u se of a ntibiotics and p neumococcal v accines
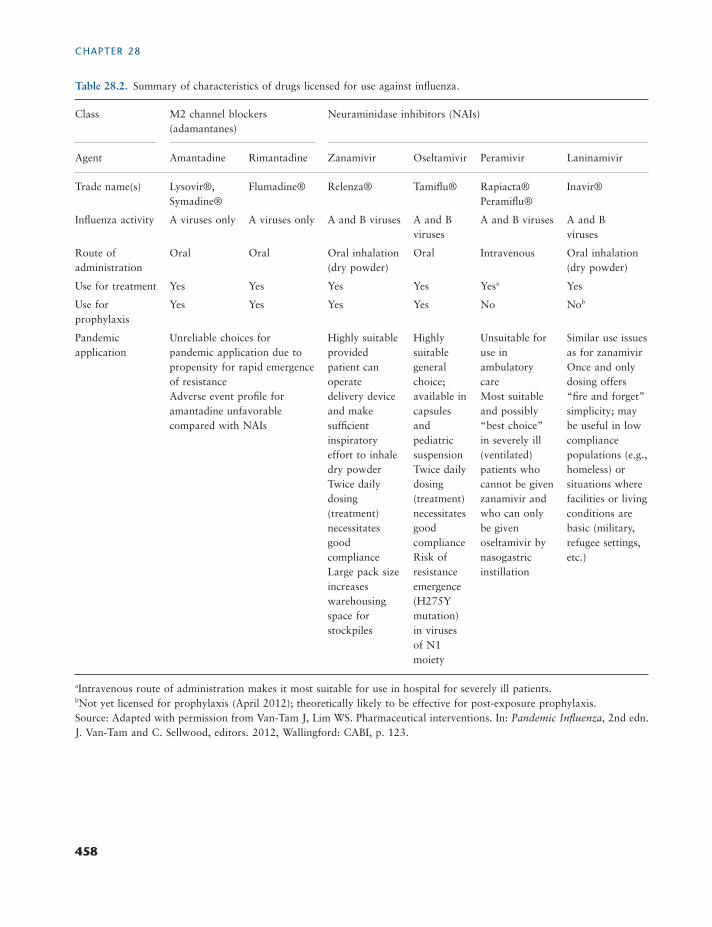
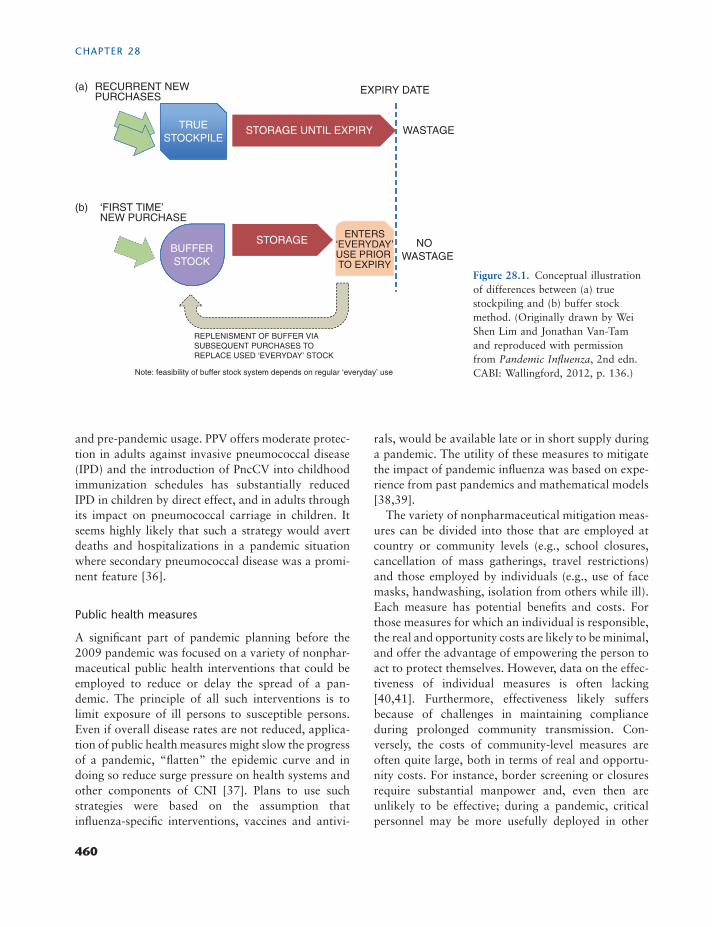
Although antiviral drugs and infl uenza vaccines dom-inate the pharmaceutical responses to pandemic infl u-enza, there is a strong temporal association between infl uenza activity and bacterial pneumonia, the most common pathogens being (in numerical order) Strep-tococcus pneumoniae (the pneumococcus) , Haemo-philus infl uenzae and Staphylococcus aureus . It has been estimated that 15–20% of pandemic infl uenza cases develop secondary bacterial pneumonia [33] , therefore, given an infl uenza clinical attack rate of 25–50%, planning for antibiotic stockpiles to cover up to 10% of the population seems reasonable [34] . The precise choice of agents should be driven by local and national surveillance data on antimicrobial resist-ance. However, there should be a planning assump-tion around the need to cover the three major etiologic organisms named above using empirical therapy, because demand for laboratory diagnostic services is likely to exceed supply and the emphasis will be on timely intervention. Because antibiotics are used year round in large numbers, true stockpiling may not be necessary if buffer stocks are introduced into the routine supply chain (Figure 28.1 ); this approach allows for gradual variations in the types and propor-tions of antibiotics held in response to changes in patterns of resistance [35] .
It has also been suggested that pneumococcal polysaccharide vaccines ( PPV ) and pneumococcal conjugate vaccines ( PncCV ) may form part of a coherent pandemic response strategy, most likely achieved through routine immunization programs
and conducted extensive testing of avian infl uenza A(H5N1) vaccines in the last decade for this purpose [30] . Stockpiles of monovalent A(H5N1) vaccines (some adjuvanted) against clades 1, 2.1, 2.2, and 2.3 viruses were created and are maintained by several countries. Use of stockpiled vaccines has been pro-moted to limit disease or delay spread among the fi rst countries affected, or to provide early vaccination of high-risk groups. However, stockpiling of vaccines in advance of a pandemic carries the inherent risk that the pandemic strain will be antigenically different from stockpiled vaccines, limiting their usefulness. Even so, the prospect of early prevention through vaccination, particularly in a severe pandemic, has maintained interest in this approach.
A challenge to pandemic vaccination is to ensure suffi cient quantity to meet demand, particularly if protection were to require two doses or high antigen content per dose. This challenge has been addressed in two ways. Several adjuvanted vaccines have been developed, both for pandemic use (e.g., A(H5N1) and A(H1N1) monovalent vaccines) and in seasonal cam-paigns (trivalent) (see Chapter 20) [29] . Adjuvants enhance immune responses in recipients, and can gen-erate greater heterotypic protection against drifted strains. Adjuvant can also be stockpiled to be mixed with pandemic antigen. A second approach to ensure adequate pandemic vaccine supply is to increase global production capacity [31] . Because most vaccine stockpiles and manufacturing capacity exist in high-income countries, concerns about the equitable access to vaccines during a pandemic has led to a concerted program to increase global vaccine supply and pro-duction capacity. The WHO Global Action Plan for Infl uenza Vaccines is designed to help ensure greater global availability of pandemic vaccines by increasing the number of manufacturers in mid- and low-income countries. As a result of the program, which began in 2005, global vaccine production has risen from 350 million doses in 2006 to more than 900 million doses in 2009. Eleven manufacturers in non-high-income settings are developing or producing vaccines [32] .
Finally, consideration has been given to vaccinating with stockpiled vaccines before the emergence of a pandemic [28] . This approach would ensure that a person receives a vaccine prior to exposure, and would be primed for later boosting with a pandemic vaccine when available. Such a strategy would also allow for use of stockpiled vaccines before loss of
CHAPTER 28
460
rals, would be available late or in short supply during a pandemic. The utility of these measures to mitigate the impact of pandemic infl uenza was based on expe-rience from past pandemics and mathematical models [38,39] .
The variety of nonpharmaceutical mitigation meas-ures can be divided into those that are employed at country or community levels (e.g., school closures, cancellation of mass gatherings, travel restrictions) and those employed by individuals (e.g., use of face masks, handwashing, isolation from others while ill). Each measure has potential benefi ts and costs. For those measures for which an individual is responsible, the real and opportunity costs are likely to be minimal, and offer the advantage of empowering the person to act to protect themselves. However, data on the effec-tiveness of individual measures is often lacking [40,41] . Furthermore, effectiveness likely suffers because of challenges in maintaining compliance during prolonged community transmission. Con-versely, the costs of community-level measures are often quite large, both in terms of real and opportu-nity costs. For instance, border screening or closures require substantial manpower and, even then are unlikely to be effective; during a pandemic, critical personnel may be more usefully deployed in other
and pre-pandemic usage. PPV offers moderate protec-tion in adults against invasive pneumococcal disease ( IPD ) and the introduction of PncCV into childhood immunization schedules has substantially reduced IPD in children by direct effect, and in adults through its impact on pneumococcal carriage in children. It seems highly likely that such a strategy would avert deaths and hospitalizations in a pandemic situation where secondary pneumococcal disease was a promi-nent feature [36] .
Public h ealth m easures
A signifi cant part of pandemic planning before the 2009 pandemic was focused on a variety of nonphar-maceutical public health interventions that could be employed to reduce or delay the spread of a pan-demic. The principle of all such interventions is to limit exposure of ill persons to susceptible persons. Even if overall disease rates are not reduced, applica-tion of public health measures might slow the progress of a pandemic, “fl atten” the epidemic curve and in doing so reduce surge pressure on health systems and other components of CNI [37] . Plans to use such strategies were based on the assumption that infl uenza-specifi c interventions, vaccines and antivi-
Figure 28.1. Conceptual illustration of differences between (a) true stockpiling and (b) buffer stock method. (Originally drawn by Wei Shen Lim and Jonathan Van-Tam and reproduced with permission from Pandemic Infl uenza , 2nd edn. CABI: Wallingford, 2012, p. 136.)
EXPIRY DATERECURRENT NEW PURCHASES
TRUE
STOCKPILESTORAGE UNTIL EXPIRY
(a)
(b)
WASTAGE
‘FIRST TIME’ NEW PURCHASE
BUFFER
STOCK
STORAGEENTERS
‘EVERYDAY’ USE PRIOR TO EXPIRY
NO
WASTAGE
REPLACE USED ‘EVERYDAY’ STOCK
REPLENISMENT OF BUFFER VIA
SUBSEQUENT PURCHASES TO
Note: feasibility of buffer stock system depends on regular ‘everyday’ use

PANDEMIC PREPAREDNESS AND RESPONSE
461
then falls, perhaps repeatedly over one to three sepa-rate waves as in 1918–1919. 2. The need to mount such a response with poten-tially lower staff availability due to sickness absence, mortality, and potentially refusal to work during a severe pandemic threat. 3. The requirement to maintain care provision in “mission critical” noninfl uenza areas, for example the handling of trauma cases, severe bacterial infections, emergency surgery, obstetric services, and coronary care. 4. To minimize the risk that healthcare becomes part of the problem (as opposed to part of the solution) through nosocomial spread of pandemic infl uenza.
The impact on healthcare demand during a pan-demic will depend upon the clinical attack rate and the propensity of the novel virus to cause severe infec-tion that cannot be managed through self-care (or informal care provided by family members) and over-the-counter remedies, that is the requirements for ambulatory (primary) care, hospital admission, and critical care (ventilatory support). Sensible ranges for such indices can be estimated from previous pandem-ics but cannot be accurately predicted, emphasizing the need for adequate surveillance data that also cover secondary and tertiary care settings. Modeling data support the fact that the impact on healthcare during a pandemic is likely to be concentrated into a typical epidemic wave of about 12 weeks, during which almost one-quarter of total associated health-care demand might fall in a single concentrated 1-week period at the peak [43] . Therefore, the ability of interventions such as the early use of antiviral drugs and public health measures to “fl atten” the peak of healthcare demand (even if this broadens the period of time affected) would be an important factor [38] . Supply issues focus principally on availability and planned usage of antiviral drugs alongside other “pandemic consumables,” notably antibiotics for the treatment of secondary bacterial pneumonias [33] , oxygen, and personal protective equipment for healthcare workers. It is clear from a recent meta-analysis that healthcare workers are at increased risk of infl uenza infection compared with nonhealth workers [44] , emphasizing the need for well-planned and rehearsed infection control procedures that reduce the risks of nosocomial spread and protect staff. In this area one critical defect remains the inad-equacy of understanding about modes of infl uenza
parts of the response. Like individual measures, high quality data on the effectiveness of community inter-ventions are sparse. Because of the diffi culty with estimating the true value and costs of the interven-tions, developing consensus on which and when to implement them has proved challenging.
Planning must also account for changing needs during a pandemic [16,26,37] . For instance, while handwashing and cough etiquette are equally reason-able at any time, the value of other mitigation meas-ures is likely to change over time. A good example of this time dependency relates to school closures. School closures are intended to mitigate local com-munity spread early in a local outbreak but work best when schools are closed before the introduction of the virus into the school-aged population [42] .
Another principle is that the actual tools employed will depend on the severity and the epidemiologic features of the pandemic [4,26] . Because of the high costs and disruption caused by some interventions, they might be relegated to the most severe pandemics, while others would be used in even mild pandemics, where the cost–benefi t is more favorable. Similarly, features of a pandemic such as age-specifi c attack rate or complication rate might result in targeting meas-ures to the affected age groups. Finally, pandemic models have repeatedly demonstrated that public health measures should be used in combination to be maximally effective [37,38] . WHO and national gov-ernments have developed plans for “targeted,” “layered” containment and mitigation strategies. As each measure, along with the use of vaccines and antivirals, is imperfect, plans rely on the additive effects of employing several at any time.
Health s ector p reparedness i ssues
In its 2005 plan and checklist, WHO drew specifi c attention to the fact that health services will be at the forefront of any national response to pandemic infl u-enza from the earliest stages when fi rst human cases are recognized through to the peak of disease activity in a given country, and thereafter into the decline and recovery phases of the response [10,11] . The impor-tant underpinning requirement is to plan for respond-ing to four interrelated threats: 1. The need to provide surge capacity as the number of patients requiring care for pandemic infl uenza rises

CHAPTER 28
462
agencies and between tiers within organizations (e.g., primary and secondary care) and rehearse interaction at critical interfaces; to identify lessons and gaps in capability which can then be rectifi ed; to reinforce training and identify training gaps [50] . Both desktop and command post exercise formats have been used for pandemic preparedness. In the former, players from participating agencies assemble in one place for a typical period of 1–2 days and play out in theory what might happen in practice, using specially designed scenarios and “compressed time”; in the
transmission [45,46] and the effectiveness of specifi c interventions such as face masks and respirators [47] .
Business c ontinuity and p reservation of c ritical n ational i nfrastructures
Besides the likely impact on healthcare systems, it is clear that the mortality and morbidity of a severe pandemic would have a major macroeconomic and societal impact justifying a whole-of-society multisec-toral response. In addition, it seems likely that the disease effects such as workplace absenteeism, supply chain disruption, and threats to social order might be compounded by intervention effects of public health measures related to travel restrictions, social distanc-ing measures, and school closures whether imple-mented formally by governments or informally by private citizens [48,49] . In light of such considera-tions, planning for the maintenance of business func-tions and preservation and maintenance of CNI has become an integral part of pandemic preparedness; however, not all national pandemic plans offer the same degree of emphasis on this point. While the emergency planning movement has been driven to a large extent by the threat posed by “big-bang” inci-dents such as terrorist attacks and sudden impact natural disasters (e.g., earthquakes) where the dura-tion is generally short (days to weeks) and mutual aid is possible, a pandemic represents a “rising tide” inci-dent that will last for an extended period (months). In addition, their global nature makes it far less likely that mutual aid will be available, locally, nationally or internationally (Table 28.3 ).
Exercises, s imulations, and d rills
Although there is a long history of using exercises, simulations, and drills to maintain and improve oper-ational effi ciency in the military, their use in civilian settings has been largely confi ned to police, fi re, rescue, and ambulance services. However, events such as the 9/11 terrorist attack, anthrax letters in 2001, the SARS outbreak in 2003, and the 7/7 London bombings in 2005 have highlighted the benefi ts of rehearsing a wider mobilization of the healthcare system to address an emergency situation. The objec-tives of pandemic healthcare exercises are: to develop multiagency links with relevant nonhealthcare organ-izations; clarify roles and responsibilities between
Table 28.3. Civilian organizations for consideration under pandemic planning arrangements for Critical National Infrastructure (CNI).
Emergency services a
• Police and security forces • Fire authorities • Ambulance services • Maritime and Coastguard Agencies
Local and regional government tiers
• Principal local, municipal, and regional authorities • Port Health Authorities
Health bodies
• Primary care providers • Hospitals • Public health and environmental authorities • Burial services
Utilities
• Electricity distributors and transmitters • Gas distributors • Water and sewage services • Telephone service providers (fi xed and mobile)
Transport
• Rail networks and operating companies (passenger and freight)
• Urban mass transportation systems • Airport operators • Harbor authorities • Public highways agencies • Food distributors • Fuel distributors
a Military personnel may feature as part of national pan-demic arrangements but are usually subject to their own contingency plans.

PANDEMIC PREPAREDNESS AND RESPONSE
463
available) to frontline healthcare workers, and many circumstances related to potential rationing or priori-tization of healthcare [51] . In the 2009–2010 pan-demic, few ethical issues were raised because the A(H1N1)pdm09 virus was of generally low severity; however, it is clear that the unexpectedly high demand for intensive care beds that ensued would have created ethical issues over the allocation of scarce resources had the pandemic virus been even slightly more severe. WHO and several individual countries (France, New Zealand, Switzerland, United Kingdom) have recognized the ethical issues that might be raised by pandemic preparedness and response. In the United Kingdom a Committee of Ethical Aspects of Pan-demic Infl uenza ( CEAPI ) was formed and met regu-larly from 2006 to 2009.
Communications
The 2009–2010 pandemic highlighted the importance of communication in pandemic response activities. Although some issues were well anticipated, for example the use of antiviral drugs and vaccines, several others such as the mildness of the A(H1N1)pdm09 virus, the fact that it was not A(H5N1), the epicenter (Mexico), and lack of clarity about severity in the early stages placed authorities “on the back foot.”
Communication between the authorities, the pub-lic, and other stakeholders such as frontline health-care workers should be planned for and the role of the media anticipated. Abraham and Pople [52] sug-gest that principles of the approach should be: 1. Building and maintenance of trust between author-ities and the public – this depends on establishing the authorities as knowledgeable, competent and fair with transparent, early communication of facts. Once trust is lost, the management of an outbreak becomes diffi cult. 2. Early release of information – even if this is bad news or there is uncertainty. In the latter case, the public also needs to be prepared for the fact that the situation and the response might change as more information becomes available. 3. Transparency – sharing dilemmas and challenges with the public and communicating the rationale for decisions, even if these change over time. 4. Listening to the public and maintaining media relations – communication during a health crisis should not be seen as a one-way fl ow of information.
latter, players participate from their normal place of duty which is especially useful for testing communica-tion between agencies and facilities. Examples of complex exercises that took place before the 2009–2010 pandemic include Exercise Common Ground (2006) in the European Union, Exercise Cumpston (2006) in Australia, and Exercise Winter Willow (2007) in the United Kingdom.
Ethical and l egal c hallenges
It has long been recognized that a severe infl uenza pandemic will apply stress to the whole of society, especially healthcare systems, and that under such extraordinary pressures ethical issues will emerge. However, the fi rst of these relates to pandemic pre-paredness itself. While it is relatively easy for high-income countries to undertake such activities (e.g., improving infl uenza surveillance and stockpiling anti-viral drugs), in low-income countries with large and immediate unresolved health challenges (e.g., sanita-tion, childhood vaccination, and maternal mortality), the decision to divert scarce resources into planning for an event whose future timing is uncertain raises ethical issues [51] . Nevertheless, under Article 12 of the United Nations International Covenant on Eco-nomic, Social and Cultural Rights (1966) and the International Health Regulations (2005), a duty of international cooperation and assistance has been established in the context of the prevention, treat-ment, and control of epidemic diseases and the WHO has a prominent role in coordinating international pandemic preparedness.
It is also recognized that many of the public health measures that are proposed for a severe pandemic may infringe personal liberty; for example, restric-tions on domestic and international movement, restriction on social and mass gatherings, workplace and school closures, quarantine arrangements and isolation. These might be enacted voluntarily, but if enforced by the state then the ethical dimensions of such decisions (which may not necessarily be wrong) will require consideration [51] .
In the area of healthcare, many issues are poten-tially raised such as the obligation of healthcare workers to provide care during a time of increased danger to themselves, the principle of reciprocity in terms of the employer ’ s duty to provide personal pro-tective equipment, antiviral drugs and vaccine (when

CHAPTER 28
464
shared the information with WHO, enabling the offi -cial declaration of a pandemic [56] . The expanded global laboratory capacity also produced timely data on antigenic and genetic viral characteristics which informed treatment and vaccine policies. Finally, the ability to confi rm the virus quickly and report through the IHR and GISRS mechanisms provided situational awareness to the public, health systems, public health offi cials, media, and politicians which informed the response and fostered trust among stakeholders [21] . Another notable product of enhanced surveillance was the rapid understanding developed regarding risk groups and age distribution [57] . These data led to policies that targeted these groups for prevention and control strategies [58] . The pandemic also high-lighted the value of data on severely ill persons, which has accelerated countries ’ adoption of surveillance systems focusing on severe acute respiratory illness ( SARI ). SARI surveillance provides countries with limited resources data on disease occurrence, severity, and provides a platform for virus and clinical data collection to inform control policies [58] .
However, some aspects related to the collection and communication of epidemiologic data were problem-atic [19] . First, use of the data to understand and articulate the severity of the pandemic was diffi cult and led to some confusion among public partners. In the United States, the Pandemic Severity Index ( PSI ) which was developed in 2006 to assess and commu-nicate severity was quickly abandoned after the start of the pandemic [37] . The PSI was diffi cult to calcu-late with suffi cient precision given the data available early in the pandemic, and mortality alone did not capture the potential impact of the pandemic [53] . WHO developed a plan based on comparison of the pandemic to past pandemics, while many individual countries had poorly developed severity and risk assessment frameworks and instead relied on WHO assessments [19] . Another source of confusion was that the ability to track laboratory-confi rmed cases early in the pandemic led to an expectation that public health authorities would provide the same regular disease counts throughout the pandemic. When countries transitioned to aggregate reporting, more general statements regarding the levels of disease, or modeled estimates, confusion among public and political leaders ensued [54,59] .
The pandemic response did provide opportunities to employ and study the effects of nonpharmaceutical
In modern societies the media is powerful and there should be investment in planning how to communi-cate with them, how to answer queries and rebut false information.
During the 2009–2010 pandemic it became clear that social media networks (e.g., Facebook® and Twitter®) are potentially important in terms of both reaching new audiences with public health informa-tion and the rapid promulgation of rumors and misinformation. The power of these tools was not fully appreciated prior to 2009 but needs to be fully taken account of in future pandemic preparedness activities.
The 2009–2010 p andemic r esponse
In spring 2009, a novel A(H1N1)pdm09 strain emerged that was of swine origin and had a collection of genes not identifi ed previously in humans or animals [53] . During the few weeks following the initial detection, the virus spread rapidly worldwide, causing the fi rst infl uenza pandemic since the emer-gence of A(H3N2) in 1968. The response to the 2009–2010 pandemic at local, national, and interna-tional levels highlighted the benefi ts and shortcom-ings of the pandemic preparedness activities reviewed in the previous sections.
Most reviews have pointed to epidemiologic and virologic surveillance and dissemination of data as a success during the pandemic, although early informa-tion was imprecise with high variability. Some keys to successes in this area are informative. First, the presence of existing surveillance structures that moni-tored seasonal infl uenza incorporated into pandemic planning allowed for a fairly seamless transition from seasonal to pandemic monitoring [9,54] . The response benefi ted from recent efforts to strengthen global sur-veillance, and led to further expansion of surveillance capacity; 138 National Infl uenza Centers now partici-pate in global data sharing, and increasing numbers of countries report epidemiologic data along with viral data [55] . An additional WHO Collaborating Center in China has been added which will make viral characterization and pandemic confi rmation more timely and representative, and further expansion is planned. On 11 June, only weeks after the fi rst iden-tifi cation of the virus, 74 countries had confi rmed illness using laboratory tests in their country and

PANDEMIC PREPAREDNESS AND RESPONSE
465
infl uenza vaccines resulted in vaccine delivered too late for the fi rst peaks of disease in many countries, limiting the demand for the vaccine in some places, and value of the vaccine in general. Countries that had used seasonal infl uenza vaccines routinely had fewer prob-lems with delayed delivery and distribution. Low-income countries where infl uenza vaccine programs were not routine relied more heavily on donations of vaccine, and had little vaccine before January 2010 [61] . While some countries reached target vaccine coverage goals, vaccine uptake in most was less than expected due to some skepticism about the need for vaccine in a “mild” pandemic and concerns over its safety. Improving the vaccine response for the next pandemic will build upon the lessons learned in 2009–2010. Building pandemic vaccine production, delivery and monitoring on solid seasonal vaccine programs is critical, but reaching low and middle-income countries to a greater extent will require expansion of seasonal programs to more countries and increasing global production capacity [31,32] .
The absence of signifi cant antiviral resistance of the pandemic strain to NAIs enabled governments and healthcare systems to employ antivirals according to their pandemic plans. Most responses used antivirals for treatment and focused on methods to ensure early treatment of ill persons, such as by removing the requirement for laboratory confi rmation and by allowing the dispensing of drug via telephone triage, obviating the delay caused by a clinic visit. Where antivirals were used as prophylaxis, it was often in subsets of high-risk persons with likely exposure or in early community outbreaks as a delaying tactic [49,60] . The scarcity of antivirals feared in the plan-ning stages was not a signifi cant factor that shaped the response in countries with stockpiles, although many resource-poor countries had little access to anti-virals drugs. In the United States, while the national stockpile was deployed, antivirals were widely avail-able and often obtained through the usual healthcare delivery systems. Despite the general availability of antiviral drugs and absence of widespread shortages, the need for licensed intravenous preparations for the treatment of severely ill persons was a clear lesson from the pandemic. While some preparations were available, they generally required special approvals which delayed treatment.
In general, pandemic planning and exercises con-ducted in the years before the emergence of the
mitigation and containment efforts. However, be-cause the pandemic virus lacked the severity of 1918, the full range of mitigation and containment tools was not employed or employed in limited fashion. For instance, the countries initially affected – Mexico, United States and Canada – almost immedi-ately abandoned “containment”-style interventions in favor of community mitigation strategies [19] . So, the quenching strategy conceived of in pre-pandemic planning phases was not possible. Communities fo-cused on early case treatment with antiviral drugs, reducing transmission through voluntarily decreasing exposures (e.g., requesting ill persons to stay home, voluntary school closures), rather than contact trac-ing and enforced isolation or quarantine. The United Kingdom, Australia, and many other countries em-ployed “delaying” strategies which included active case fi nding and treatment with antiviral drugs, bor-der restrictions, voluntary quarantine or close follow-up of contacts, and household post-exposure prophylaxis (United Kingdom) [19,25,60] . Most countries abandoned these approaches once transmis-sion was confi rmed within the country because of the high costs of manpower to administer the programs compared with the diminishing value once that point was reached. The appreciation that the pandemic was not a severe 1918-like scenario, which was planned for by most countries, meant that most national responses principally involved the health sector rather than requiring a broad whole-of-government approach. When responses did involve institutions outside of the health sector, public and political ac-ceptance was often low. An example was the diffi culty encountered when school closures were recommend-ed as a community mitigation measure in the United States [54] .
Because of the emergence of an A(H1N1) pandemic virus, rather than an A(H5N1) virus, pre-pandemic vaccine stockpiles were not put to use in the response. Even so, the rapid production and approval of pan-demic vaccines was a notable success in the public health response [61] . The vast experience in making seasonal vaccines, together with substantial amount of planning involving public and private partners, was critical to this success. After the production, building on infrastructure used in seasonal campaigns to evalu-ate the effectiveness and safety of the vaccines and monitor coverage allowed for rapid and reliable data. However, the inherent time constraints in making

CHAPTER 28
466
2008. Thus, although it is clear that planning prior to 2009 lacked fl exibility to deal with a range of milder scenarios [63] , severe scenarios remain equally valid.
Although political support for pandemic prepared-ness and the eventual response in 2009–2010 had been strong in many countries, there was a degree of pandemic fatigue by mid-2010 when the WHO declared the pandemic over and perhaps a sense among the unwary that pandemics are easy to cope with. Subsequently, the continuing global fi nancial crisis has focused political attention on pressures to control or reduce public spending which, in turn, has somewhat dampened enthusiasm for investment in activities such as pre-pandemic vaccination (where skeptics can argue the choice of vaccine–A(H5N1) – turned out to be wrong) and the establishment or replenishment of antiviral drug stockpiles. However, this attitude is not universal; for example, the UK Cabinet Offi ce continues to rank pandemic infl uenza as its highest civil emergency threat due to natural events in terms of both likelihood (at some point) and potential impact [63] .
Aside from political issues the biggest “forward lesson” from the 2009–2010 pandemic undoubtedly relates to vaccination. The considerable manufactur-ing success of producing pandemic vaccines within 6 months of the fi rst signs of a pandemic crisis did not alter the fact that in epidemiologic terms, this was too late to be of maximum benefi t and reinforces the pressing need for improved cross-reactive vaccines that can be produced and administered in advance of a crisis [29] . Sadly, the global vaccination response to A(H1N1)pdm09 also highlighted inequities in both the distribution and timing of delivery of vaccines that remain to be addressed.
Acknowledgments
Any views expressed in the Work by contributors employed by the United States government at the time of writing do not necessarily represent the views of the United States government, and the contributor ’ s contribution to the Work is not meant to serve as an offi cial endorsement of any statement to the extent that such statement may confl ict with any offi cial position of the United States government.
H1N1pdm09 virus resulted in real benefi ts to com-munities affected. Areas of the pandemic response that built on systems used in interpandemic periods, such as surveillance, communications, and vaccine programs, generally fared well during the pandemic. Activities that were initiated during the pandemic or were diffi cult to exercise were often less effective. The importance of exercising the response compo-nents of national plans cannot be overstated; coun-tries with true operational plans generally fared better than those with strategic plans that had not been tested operationally. While an international group of experts that reviewed WHO ’ s response to the pan-demic was generally complementary, it noted that the world remained ill-prepared for a severe pan-demic [21] .
The f uture of p andemic p reparedness
The experiences of 2009–2010 have served to remind public health authorities and the public that infl uenza pandemics remain totally unpredictable in terms of their timing, origin, epicenter, and severity. Although these facts were well understood long before, the natural tendency was to plan for the possible emer-gence of an A(H5N1) related pandemic threat, poten-tially of avian origin and indeed few experts would have bet against that scenario. It is therefore hardly surprising that although pandemic preparedness activity had generally proven useful, there was a widespread acknowledgment that pre-2009 plans lacked fl exibility for dealing with less severe scenar-ios, which now needs to be addressed [63] . Neverthe-less, although the 2009–2010 pandemic was not of mainly avian origin, not of the A(H5) hemagglutinin subtype, did not emerge in South-East Asia, and was generally mild, the degree of diffi culty experienced in the response related mainly to communications, vaccine logistics, and intensive care capacity rein-forces the worth of pandemic preparedness activity [62] and the potential for massive disruption in a severe pandemic. However, many nonhealth compo-nents of the national plans were not tested in 2009. Most experts agree that the pandemic threat posed by infl uenza viruses in the animal kingdom, notably A(H5N1), A(H7N7), A(H7N2), A(H9N2), and A(H2N2), has neither increased nor decreased since
PANDEMIC PREPAREDNESS AND RESPONSE
467
15. Hampson AW . Surveillance for pandemic infl uenza . J Infect Dis . 1997 ; 176 ( Suppl. 1 ): S8 – 13 .
16. World Health Organization . Pandemic Infl uenza Prepar-edness and Response . WHO Publication, 2009 . p. 1 – 58 .
17. Oshitani H , Kamigaki T , Suzuki A . Major issues and challenges of infl uenza pandemic preparedness in devel-oping countries . Emerg Infect Dis . 2008 ; 14 ( 6 ): 875 – 80 .
18. US Department of Health and Human Services . HHS Pandemic Infl uenza Plan . 2005 . Available from: http://www.flu.gov/planning-preparedness/federal/hhspandemicinfl uenzaplan.pdf (accessed 19 February 2013).
19. Nicoll A , Ammon A , Amato Gauci A , Ciancio B , Zucs P , Devaux I , et al. Experience and lessons from surveil-lance and studies of the 2009 pandemic in Europe . Public Health . 2010 ; 124 ( 1 ): 14 – 23 .
20. World Health Organization . International Health Regu-lations: (2005) . 2nd ed . Lyon, France : World Health Organization ; 2008 . p. 1 .
21. World Health Organization . Implementation of the International Health Regulations (2005): Report of the Review Committee on the Functioning of the Interna-tional Health Regulations (2005) in relation to Pan-demic (H1N1) 2009. Geneva, Switzerland : World Health Organization ; 2011 . p. 1 . Available from: http://apps.who.int/gb/ebwha/pdf_fi les/WHA64/A64_10-en.pdf (accessed 25 February 2013).
22. Monto AS . Vaccines and antiviral drugs in pandemic preparedness . Emerg Infect Dis . 2006 ; 12 ( 1 ): 55 – 60 .
23. Greene SK , Shay DK , Yin R , McCarthy NL , Baxter R , Jackson ML , et al. Patterns in infl uenza antiviral medi-cation use before and during the 2009 H1N1 pandemic, Vaccine Safety Datalink Project, 2000–2010 . Infl uenza Other Respi Viruses . 2012 ; 6 : 143 – 51 .
24. Hurt AC , Hardie K , Wilson NJ , Deng YM , Osbourn M , Gehrig N , et al. Community transmission of oseltamivir-resistant A(H1N1)pdm09 infl uenza . N Engl J Med . 2011 ; 365 ( 26 ): 2541 – 2 .
25. Pebody RG , Harris R , Kafatos G , Chamberland M , Campbell C , Nguyen-Van-Tam JS , et al. Use of antiviral drugs to reduce household transmission of pandemic (H1N1) 2009, United Kingdom . Emerg Infect Dis . 2011 ; 17 ( 6 ): 990 – 9 .
26. Department of Health Pandemic Infl uenza Preparedness Team . UK Infl uenza Pandemic Preparedness Strategy . 2011 . London, UK. p. 1 – 70 . Available from: http://www.dh.gov.uk/prod_consum_dh/groups /dh_digitalassets/documents/digitalasset/dh_131040.pdf (accessed 19 February 2013).
27. Muthuri SG , Myles PR , Venkatesan S , Leonardi-Bee J , Nguyen-Van-Tam JS. Impact of neuraminidase inhibitor treatment on outcomes of public health importance during the 2009–2010 infl uenza A(H1N1) pandemic: a
References
1. Thucydides. The Peloponnesian War (Introduction by Finley MI; Translation by Warner R.) . London : Penguin Books ; 1972 .
2. Simpson WJ . A Treatise on Plague Dealing with the Historical, Epidemiological, Clinical, Therapeutic and Preventive Aspects of the Disease . Cambridge : Cam-bridge University Press ; 1905 .
3. Cipolla CM . Cristofano and the Plague: A Study in the History of Public Health in the Age of Galileo . Berkeley : University of California Press ; 1973 .
4. Bell DM , G. World Health Organization Writing . Non-pharmaceutical interventions for pandemic infl uenza, national and community measures . Emerg Infect Dis . 2006 ; 12 ( 1 ): 88 – 94 .
5. Henderson DA , Courtney B , Inglesby TV , Toner E , Nuzzo JB . Public health and medical responses to the 1957–58 infl uenza pandemic . Biosecur Bioterror . 2009 ; 7 ( 3 ): 265 – 73 .
6. Tam JS . Infl uenza A (H5N1) in Hong Kong: an over-view . Vaccine . 2002 ; 20 ( Suppl. 2 ): S77 – 81 .
7. Horimoto T , Kawaoka Y . Pandemic threat posed by avian infl uenza A viruses . Clin Microbiol Rev . 2001 ; 14 ( 1 ): 129 – 49 .
8. Abdullah AS , Tomlinson B , Cockram CS , Thomas GN . Lessons from the severe acute respiratory syndrome out-break in Hong Kong . Emerg Infect Dis . 2003 ; 9 ( 9 ): 1042 – 5 .
9. Peiris JS , Yu WC , Leung CW , Cheung CY , Ng WF , Nicholls JM , et al. Re-emergence of fatal human infl u-enza A subtype H5N1 disease . Lancet . 2004 ; 363 ( 9409 ): 617 – 9 .
10. World Health Organization . WHO global infl uenza pre-paredness plan. The role of WHO and recommenda-tions for national measures before and during pandemics . 2005 . Available from: http://www.who.int/csr/resources/publ i ca t ions / in f luenza /WHO_CDS_CSR_GIP_2005_5.pdf (accessed 19 February 2013).
11. World Health Organization . WHO checklist for infl u-enza pandmeic preparedness . 2005 . Available from: http://www.who.int/csr/resources/publications/infl uenza/WHO_CDS_CSR_GIP_2005_4/en/ (accessed 19 February 2013).
12. Taubenberger JK , Morens DM . 1918 Infl uenza: the mother of all pandemics . Emerg Infect Dis . 2006 ; 12 ( 1 ): 15 – 22 .
13. Nguyen-Van-Tam JS , Hampson AW . The epidemiology and clinical impact of pandemic infl uenza . Vaccine . 2003 ; 21 ( 16 ): 1762 – 8 .
14. Payne AM . The infl uenza programme of WHO . Bull World Health Organ . 1953 ; 8 ( 5–6 ): 755 – 74 .
CHAPTER 28
468
41. Aledort JE , Lurie N , Wasserman J , Bozzette SA . Non-pharmaceutical public health interventions for pan-demic infl uenza: an evaluation of the evidence base . BMC Public Health . 2007 ; 7 : 208 .
42. Cauchemez S , Ferguson NM , Wachtel C , Tegnell A , Saour G , Duncan B , et al. Closure of schools during an infl uenza pandemic . Lancet Infect Dis . 2009 ; 9 ( 8 ): 473 – 81 .
43. Department of Health . Pandemic fl u: a national frame-work for responding to an infl uenza pandemic . 2007 . Available from: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_080734 (accessed 19 February2013).
44. Kuster SP , Shah PS , Coleman BL , Lam PP , Tong A , Wormsbecker A , et al. Incidence of infl uenza in healthy adults and healthcare workers: a systematic review and meta-analysis . PLoS ONE . 2011 ; 6 ( 10 ): e26239 .
45. Brankston G , Gitterman L , Hirji Z , Lemieux C , Gardam M . Transmission of infl uenza A in human beings . Lancet Infect Dis . 2007 ; 7 ( 4 ): 257 – 65 .
46. Tellier R . Review of aerosol transmission of infl uenza A virus . Emerg Infect Dis . 2006 ; 12 ( 11 ): 1657 – 62 .
47. Bin-Reza F , Lopez Chavarrias V , Nicoll A , Chamberland ME . The use of masks and respirators to prevent trans-mission of infl uenza: a systematic review of the scientifi c evidence . Infl uenza Other Respi Viruses . 2012 ; 6 ( 4 ): 257 – 67 .
48. Blank PR , Szucs TD . Socio-economic impact . In: Van-Tam J , Sellwood C , editors. Pandemic Infl uenza, 2nd edn . Wallingford : CABI ; 2012 . p. 173 – 80 .
49. Nicoll A , Lopez Chavarrias V . National and interna-tional public health measures . In: Van-Tam J , Sellwood C , editors. Pandemic Infl uenza , 2nd edn . Wallingford : CABI ; 2012 . p. 152 – 63 .
50. Simpson J . The role of exercises in pandemic prepared-ness . In: Van-Tam J , Sellwood C , editors. Pandemic Infl u-enza , 2nd edn . Wallingford : CABI ; 2012 . p. 97 – 103 .
51. Gadd EM . Ethical issues related to pandemic prepared-ness and response . In: Van-Tam J , Sellwood C , editors. Pandemic Infl uenza , 2nd edn . Wallingford : CABI ; 2012 . p. 181 – 8 .
52. Abraham T , Pople D . Pandemic communications . In: Van-Tam J , Sellwood C , editors. Pandemic Infl uenza , 2nd edn . Wallingford : CABI ; 2012 . p. 189 – 97 .
53. Centers for Disease Control and Prevention (CDC) . Swine infl uenza A (H1N1) infection in two children – Southern California, March–April 2009 . Morb Mortal Wkly Rep . 2009 ; 58 : 400 – 2 .
54. Presidential Advisors on Science and Technology . Report to the President on US preparations for 2009-H1N1 infl uenza, Executive Offi ce of the President . 2009 . p. 1 – 86 .
55. World Health Organization . Global Infl uenza Surveil-lance and Response System (GISRS) . 2012 . Available
systematic review and meta-analysis in hospitalized patients . J Infect Dis. 2013 ; 207 ( 4 ): 553 – 63 .
28. Jennings LC , Monto AS , Chan PK , Szucs TD , Nichol-son KG . Stockpiling prepandemic infl uenza vaccines: a new cornerstone of pandemic preparedness plans . Lancet Infect Dis . 2008 ; 8 ( 10 ): 650 – 8 .
29. Carrasco P , Leroux-Roels G . Pandemic vaccines . In: Van-Tam J , Sellwood C , editors. Pandemic Infl uenza , 2nd edn . Wallingford : CABI ; 2012 . p. 139 – 51 .
30. El Sahly HM , Keitel WA . Pandemic H5N1 infl uenza vaccine development: an update . Expert Rev Vaccines . 2008 ; 7 ( 2 ): 241 – 7 .
31. World Health Organization . Global pandemic infl uenza action plan to increase vaccine supply . WHO Publica-tion, 2006 . Available from: http://www.who.int/csr/resources/publications/influenza/WHO_CDS_EPR_GIP_2006_1/en/index.html (accessed 25 February 2013).
32. Friede M , Palkonyay L , Alfonso C , Pervikov Y , Torelli G , Wood D , et al. WHO initiative to increase global and equitable access to infl uenza vaccine in the event of a pandemic: supporting developing country production capacity through technology transfer . Vaccine . 2011 ; 29 ( Suppl. 1 ): A2 – 7 .
33. Brundage JF . Interactions between infl uenza and bacte-rial respiratory pathogens: implications for pandemic preparedness . Lancet Infect Dis . 2006 ; 6 : 303 – 12 .
34. Gupta RK , George R , Nguyen-Van-Tam JS . Bacterial pneumonia and pandemic infl uenza planning . Emerg Infect Dis . 2008 ; 14 ( 8 ): 1187 – 92 .
35. Van-Tam J , Lim WS . Pharmaceutical interventions . In: Van-Tam J , Sellwood C , editors. Pandemic Infl uenza , 2nd edn . Wallingford : CABI ; 2012 . p. 122 – 38 .
36. Crowe S , Utley M , Walker G , Grove P , Pagel C . A model to evaluate mass vaccination against pneumococcus as a countermeasure against pandemic infl uenza . Vaccine . 2011 ; 29 ( 31 ): 5065 – 77 .
37. Centers for Disease Control and Prevention (CDC) . Interim Pre-pandemic Planning Guidance: Community Strategy for Pandemic Infl uenza Mitigation in the United States – Early, Targeted, Layered Use of Nonp-harmaceutical Interventions , US Department of Health and Human Services. 2007 . p. 1 – 97 .
38. Ferguson NM , Cummings DA , Fraser C , Cajka JC , Cooley PC , Burke DS . Strategies for mitigating an infl u-enza pandemic . Nature . 2006 ; 442 ( 7101 ): 448 – 52 .
39. Markel H , Lipman HB , Navarro JA , Sloan A , Michalsen JR , Stern AM , et al. Nonpharmaceutical interventions implemented by US cities during the 1918–1919 infl u-enza pandemic . JAMA . 2007 ; 298 ( 6 ): 644 – 54 .
40. Cowling BJ , Zhou Y , Ip DK , Leung GM , Aiello AE . Face masks to prevent transmission of infl uenza virus: a sys-tematic review . Epidemiol Infect . 2010 ; 138 ( 4 ): 449 – 56 .

PANDEMIC PREPAREDNESS AND RESPONSE
469
60. Australia Government, Department of Health and Ageing . Review of Australia ’ s Health Sector Response to Pandemic (H1N1) 2009: Lessons Identifi ed . 2011 : Canberra. Available from: http://www.fl upandemic.gov.au/internet/panflu/publishing.nsf/Content/review-2011/$File/lessons%20identifi ed-oct11.pdf (accessed 19 February 2013).
61. Partridge J , Kieny MP ; World Health Organization H1N1 infl uenza vaccine Task Force. Global production of seasonal and pandemic (H1N1) infl uenza vaccines in 2009–2010 and comparison with previous estimates and global action plan targets . Vaccine . 2010 ; 28 ( 30 ): 4709 – 12 .
62. Hashim A , Jean-Gilles L , Hegermann-Lindencrone M , Shaw I , Brown C , Nguyen-Van-Tam J . Did pandemic preparedness aid the response to pandemic (H1N1) 2009? A qualitative analysis in seven countries within the WHO European Region . J Infect Public Health . 2012 ; 5 : 286 – 96 .
63. Cabinet Offi ce . National Risk Register of Civil Emer-gencies 2012 edition . 2012 . Available from: http://www.cabinetoffice.gov.uk/resource-library/national-risk-register (accessed 19 February 2013).
from: http://www.who.int/infl uenza/gisrs_laboratory/en/ (accessed 19 February 2013).
56. World Health Organization . World now at the start of 2009 infl uenza pandemic . 2009 . Available from: http://www.who.int/mediacentre/news/statements/2009/h1n1_pandemic_phase6_20090611/en/index.html (accessed 19 February 2013).
57. Van Kerkhove MD , Vandemaele KA , Shinde V , Jaramillo-Gutierrez G , Koukounari A , Donnelly CA , et al. Risk factors for severe outcomes following 2009 infl uenza A (H1N1) infection: a global pooled analysis . PLoS Med . 2011 ; 8 ( 7 ): e1001053 .
58. Centers for Disease Control and Prevention . Interim results: infl uenza A (H1N1) 2009 monovalent and sea-sonal infl uenza vaccination coverage among health-care personnel – United States, August 2009–January 2010 . MMWR Morb Mortal Wkly Rep . 2010 ; 59 ( 12 ): 357 – 62 .
59. World Health Organization . WHO global technical consultation: global standards and tools for infl uenza surveillance . 2011 . Available from: http://www.who.int/infl uenza/resources/documents/technical_consultation/en/index.html (accessed 19 February 2013).