Embed Size (px)
Citation preview
Focus on Dementia | Testing the 8 Pillars Model | Perspective of staff | V 22.11.2015 Page 1
TESTING THE 8 PILLARS’ MODEL OF COMMUNITY SUPPORT
SUPPORTING PEOPLE WITH DEMENTIA IN THE COMMUNITY:
THE PERSPECTIVE OF STAFF
Eileen Moir and Michelle Miller
October 2015
Focus on Dementia | Testing the 8 Pillars Model | Perspective of staff | V 22.11.2015 Page 2
Contents
Page Foreword Executive summary Introduction Approach Findings Conclusions
3 5 6 6 8
12
Focus on Dementia | Testing the 8 Pillars Model | Perspective of staff | V 22.11.2015 Page 3
FOREWORD
About Focus on Dementia Focus on Dementia is a partnership improvement programme which brings together and maximises the skills, expertise and knowledge of improvement professionals, policy practitioners and the third sector in order to support the continuing transformation and modernisation of dementia services in Scotland. In supporting the implementation of the dementia strategy, the programme is testing Alzheimer Scotland’s 8 pillar model. 8 Pillar Model of Comprehensive Integrated Support The 8 pillar model was developed by Alzheimer Scotland based on best available evidence and following wide consultation which included people with dementia and carers. It is a comprehensive integrated approach to supporting people with dementia, their families and carers. The model includes the introduction of a dementia practice co-ordinator, who will ensure access to all pillars of support as appropriate to each individual. Other pillars include support for carers, personalised support, community connections, environment, mental health care and treatment, general health care and treatment and therapeutic interventions. Testing the Model An improvement collaborative has been established nationally to support the test sites (health and social care partnerships) to inform the testing of this model in practice, and associated improvements, to share data, progress, challenges and opportunities. This is being achieved through a series of learning sessions, action learning sets, webinars and through targeted improvement support. A key aspect of the work is understanding the experience of staff in working with the 8 Pillars’ Model. The attached report is an important contribution to this work in providing qualitative data to inform the design of improvements to support the implementation of the 8 pillar model. An external evaluation of the Focus on Dementia 8 pillar testing work is underway and will re-visit staff experience to understand any further implications and impact of this as the testing is taken forward across the five test sites. Acknowledgements The Focus on Dementia team are grateful to practitioners for taking time away from their busy work schedules and to project managers for coordinating this process. The candid views expressed in the focus group conversations help us to understand better what it is like for practitioners at the beginning of the testing phase and what might be done to address some of the barriers to improvement nationally as well as locally. We would also like to thank Alzheimer’s Scotland for their administrative support in transcribing the focus group conversations. Eileen Moir and Michelle Miller Focus on Dementia
Focus on Dementia | Testing the 8 Pillars Model | Perspective of staff | V 22.11.2015 Page 4
EXECUTIVE SUMMARY
This report presents the findings from a series of focus groups held with staff from the five test sites in the early part of 2015. The aim was to:
Learn about the experience of staff within the context of the 8 Pillars programme
Identify what might be experienced as enablers and conversely, what might hinder progress.
Three focus groups were held with staff between January and March 2015. Twenty staff attended the three focus groups. Between 3-5 practitioners attended from each test site. Emotional Touchpoints and photo-elicitation were the methods used to seek views in relation to four Touchpoints - knowing the person; decision-making; driving things forward and working with the system. The data was initially themed according to the four Touchpoints and the three improvement aims of the project - improving experience, improving safety and improving coordination. A final stage involved organising the data according to the level in the system to which the experiences related – individual; service/project; organizational or national level. Six themes were identified under each of the four outcome levels as per the table above. These were: 1) There is a high level of commitment demonstrated by practitioners working with people with
dementia and their carers in the community (Individual level) 2) The relationship between practitioners, the person with dementia and their carer/s is the
essence of person-centred care (Individual level)
3) Although the Dementia Practice Coordinator (DPC) is responsible for coordinating care and services for people with dementia, in some instances practitioners felt they had little control over delivery (Service level)
4) The integration of health and social care services services going on in the background added
to the uncertainty and complexity of testing the 8 pillars model in some test sites (Service level) 5) Although there were mixed views about being part of the national testing programme,
practitioners were hopeful that things would get better for people with dementia and their carers (Organisational level).
6) Messages for Scottish Government and the national improvement support team (National
level) Each test site is different in character and approach and as such there was a broad spectrum of views expressed across the focus groups. Emotional Touchpoints provided an extraordinary richness and depth of data. However, the approach may not have been structured enough for this context. Health and social care services across Scotland were in the midst of transitioning into Health and Social Care Partnerships. Responses to the Touchpoints were wide ranging making it difficult to extrapolate views about the 8 Pillars’ testing from staff experience of the integration of health and social care per se. Moreover, the uncertainty relating to the ‘shaky foundations’ typical of systemic change can make innovation more difficult. This appears to have coloured the perceptions of some practitioners. The progress they have made in the first half of the project is a credit to their tenacity
Focus on Dementia | Testing the 8 Pillars Model | Perspective of staff | V 22.11.2015 Page 5
Success in meeting personal outcomes at the interface between the practitioner and the person with dementia and their carers will only be achieved, and sustained, if there is a commitment to delivery at every level within the system. Exploring staff experience within the context of the four system levels in Fig 1 has illuminated where some of the enablers and barriers lie. This gives rise to a number of questions for consideration by the local test sites in association with national improvement support team. 1. What are seen to be the main bottle-necks in relation to service delays and how might they be
addressed? 2. What might be needed to help practitioners feel more empowered in fulfilling the DPC role? 3. What is ‘in scope’ and ‘out of scope’ in relation to the role of a DPC? 4. To what extent has the distraction of the health and social care integration influenced how the
changes have been managed in test sites? 5. Building on the previous question, what opportunities has the integration of health and social
care brought to the 8 Pillars’ testing programme? The findings along with these questions should inform improvement activity within the test sites and guide the work of the 8 Pillars National Team during this final stage of testing.
Focus on Dementia | Testing the 8 Pillars Model | Perspective of staff | V 22.11.2015 Page 6
1. INTRODUCTION An important part of testing the 8 Pillars' model of community support for people with dementia is to understand the experiences of staff. This, along with the experience of carers, formed the qualitative data plan which complemented the quantitative data being collected from each site. It was important to understand how it was for staff before the full introduction of the 8 Pillars model and again when the changes had begun to bed down; approximately a year later. This report presents the findings from a series of focus groups held with staff from the five test sites in the early part of 2015. The focus groups were held at an early stage in the testing process. They also took place against the backdrop of the integration of health and social care which is one of Scotland's major programmes of reform. Health and social care integration is about ensuring that those who use services get the right care and support whatever their needs, at any point in their care journey. It aims to transform the way health and social care services are provided in Scotland and drive real change that improves people’s lives. The integration of health and social care is arguably one of the most fundamental set of changes affecting staff in parts of the NHS and local authorities in Scotland in recent years. Scotland has also lived through a period of prolonged austerity. The focus groups were therefore a microcosm of what was taking place in the wider system. 1.1 Brief Review of the Literature There is very little in the literature about staff experience of supporting people with dementia and their carers live well in the community. Perhaps understandably most published studies focus on the experiences and outcomes for people with dementia and their carers. However, as Churchill (2015) points out
‘Great patient experience cannot be delivered at the expense of staff experience. In fact … good staff experience generates good patient experience’
Some studies consider the efficacy of case management which is similar to the concept of Dementia Care Coordination; the cornerstone of the 8 Pillars’ Model. Of particular note is a study by Prince et al in the World Alzheimer’s Report 2013. They looked at the evidence base for case management and found moderate evidence for a beneficial effect on quality of care, quality of life (clients), and satisfaction with services. Important to success was seen to be (a) a single point of contact, (b) case management targeted on those with particularly complex health and social care needs and (c) delivered within the context of a ‘high degree of functional integration between agencies, particularly health and social care’. These success factors provide helpful markers when considering staff experience in the 8 Pillars test sites. 2. APPROACH Three focus groups were held with staff between January and March 2015. One was held in Glasgow for those staff from the central belt sites – Glasgow, Midlothian and North Lanarkshire. The other two were held in Highland and Moray respectively. Project Managers from each site were invited to nominate staff who were already designated Dementia Practice Coordinators (DPC) or who supported people in the community with Advanced dementia. Twenty staff attended the three focus groups. Between 3-5 practitioners attended from each test site.
Focus on Dementia | Testing the 8 Pillars Model | Perspective of staff | V 22.11.2015 Page 7
Most of the focus group attendees worked directly with people with dementia but there were others supporting the 8 Pillars testing such as project managers and a senior manager. The range of titles is captured below. • CPN (7) • Social Worker (2) • Practice Team Leader, Alzheimer’s Scotland • Day Unit Staff Nurse • Social Work Carers Development Worker • Care Manager • AHP Dementia Consultant • Service Manager, Dementia Practice • DPC/8 Pillars Project Manager • Post Diagnostic Support Link Worker • Memory Clinic Nurse • 8 Pillars Project Manager • Senior Manager The aim was to learn about the experience of staff within the context of the 8 Pillars programme. The national 8 Pillar’s improvement support team also wanted to identify what might be experienced as enablers and conversely, what might hinder progress. 2.1 Method Emotional Touchpoints and photo-elicitation were the methods used. Emotional Touchpoints is a method that helps us to tap into the meaning of an experience in a structured way. It focuses on particular points in the ‘experience’ under the spotlight (Touchpoints) and asks people to select from a range of emotional words that sum up what the experience felt like. The practitioner, is also invited to sum up why they felt that way and if appropriate what would help to make the experience better. A set of 14 Touchpoints were identified by the study team. Following a teleconference with programme managers, four core Touchpoints were selected from the original list. These were: 1. Knowing the person 2. Decision-Making 3. Driving things forward 4. Working with the system The conversations during the focus group were recorded and transcribed verbatim within the bounds of confidentiality. All identifying markers were removed from the transcriptions to ensure a degree of anonymity for both the practitioners and the test sites. 2.2 Analysis of Data The data was initially themed according to the four Touchpoints and the three improvement aims of the project - improving experience, improving safety and improving coordination. The data did not always relate to one specific aim so a degree of judgement was required. The next stage involved organising the data according to the level in the system to which the experiences related. The four levels of the outcomes as articulated by Ailsa Cook and Emma Miller provided a useful framework. The levels are set out in Fig 1 below.
Focus on Dementia | Testing the 8 Pillars Model | Perspective of staff | V 22.11.2015 Page 8
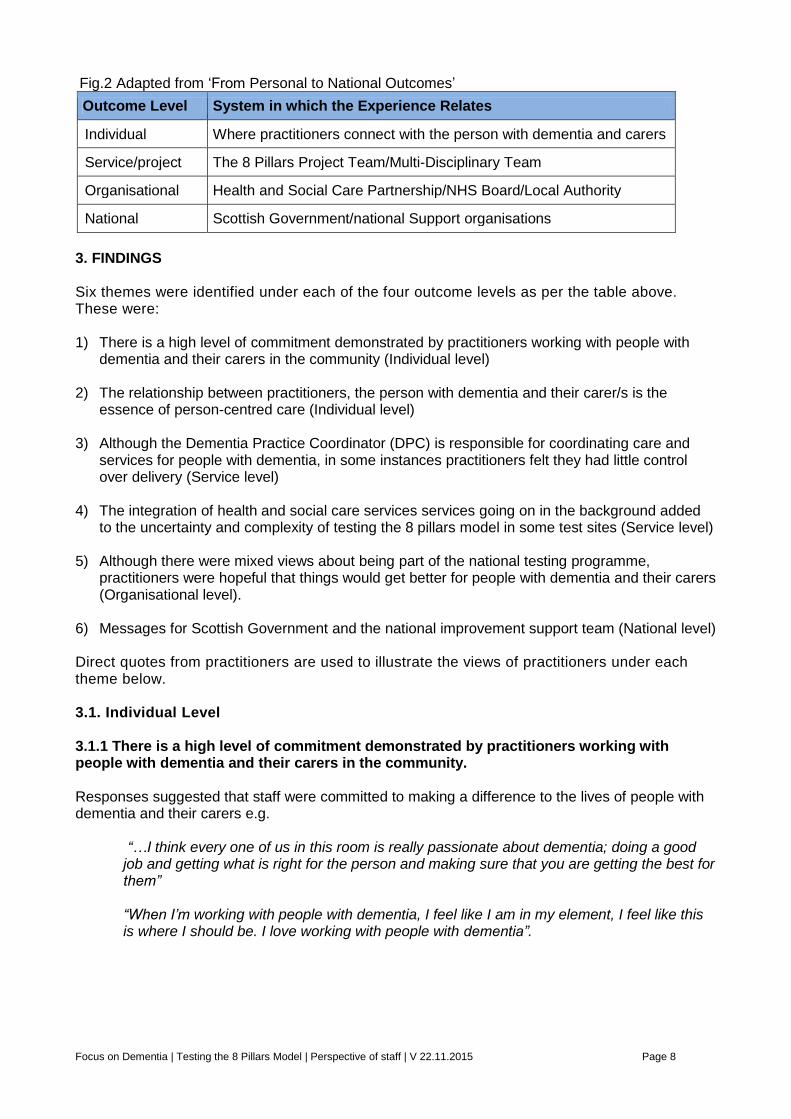
Fig.2 Adapted from ‘From Personal to National Outcomes’
Outcome Level System in which the Experience Relates
Individual Where practitioners connect with the person with dementia and carers
Service/project The 8 Pillars Project Team/Multi-Disciplinary Team
Organisational Health and Social Care Partnership/NHS Board/Local Authority
National Scottish Government/national Support organisations
3. FINDINGS Six themes were identified under each of the four outcome levels as per the table above. These were: 1) There is a high level of commitment demonstrated by practitioners working with people with
dementia and their carers in the community (Individual level) 2) The relationship between practitioners, the person with dementia and their carer/s is the
essence of person-centred care (Individual level) 3) Although the Dementia Practice Coordinator (DPC) is responsible for coordinating care and
services for people with dementia, in some instances practitioners felt they had little control over delivery (Service level)
4) The integration of health and social care services services going on in the background added to the uncertainty and complexity of testing the 8 pillars model in some test sites (Service level)
5) Although there were mixed views about being part of the national testing programme,
practitioners were hopeful that things would get better for people with dementia and their carers (Organisational level).
6) Messages for Scottish Government and the national improvement support team (National level) Direct quotes from practitioners are used to illustrate the views of practitioners under each theme below. 3.1. Individual Level 3.1.1 There is a high level of commitment demonstrated by practitioners working with people with dementia and their carers in the community. Responses suggested that staff were committed to making a difference to the lives of people with dementia and their carers e.g.
“…I think every one of us in this room is really passionate about dementia; doing a good job and getting what is right for the person and making sure that you are getting the best for them” “When I’m working with people with dementia, I feel like I am in my element, I feel like this is where I should be. I love working with people with dementia”.
Focus on Dementia | Testing the 8 Pillars Model | Perspective of staff | V 22.11.2015 Page 9
3.1.2 The relationship between practitioners and their carer/s is the essence of person-centred care The responses indicated that relationships are central to connecting well with people with dementia and their carers and considerable investment is made by staff e.g.
“You never fail to be overwhelmed by what you’re told. People open up to me about things
they haven’t shared with their families and friends”
“…Getting to know the person breaks down the barriers. People with dementia pick up on your body language and how you are working with them.
The emotional impact of the work was a feature in a number of the focus group conversations e.g.
“We’re on an emotional rollercoaster and we rely heavily on each other for support….. You’re getting beaten down and it doesn’t matter how much you do, you’re ‘treading treacle’. Then you’ll get a phone call from a carer saying ‘I just wanted to phone and say thanks because you made things so different for us’ and you go back up again”
The way that team members support each other shone through each of the conversations. This appeared to make all the difference in sustaining each other.
“There’s a trust as well. It’s never needed to be said or anything; a trust and a bond” There was however, some evidence of strained relationships within teams especially across agencies. This may be more to do with cultural and philosophical differences rather than issues between individual staff members. For example the differences in the way health and social care are funded may be a factor in creating some of this tension i.e. the NHS being seen as ‘free at the point of delivery’ with open access whereas access to local authority social care seen to be limited for a variety of reasons.
“It’s really difficult not to (criticise) and I don’t do it, but sometimes I have to bite my tongue and say "we’re all doing our best. “I feel let down by services. We know what people need but it’s not always there for them”
3.2 Service/Project Level 3.2.1 Although the DPC is responsible for coordinating care and services for people with dementia, in some instances practitioners felt they had little control over delivery Assessment came up a number of times in terms of the extensive nature of the process and the frustration when the agreed outcomes couldn’t always be achieved e.g.
“It’s frustrating doing assessment and identifying needs and knowing that you can put things in place but there are waiting lists or funding restrictions – factors that make it difficult – e.g. for day centre”
“I often hear myself saying that we’ll have to wait until crisis to happen before we can do anything about this, which you never used to; we were more proactive. This is down to resources”
Focus groups practitioners often used phrases that reflected a sense of stuckness which prevented them from moving forward on behalf of clients e.g.
“We’re supposed to be acting on his behalf and we are stuck between a rock and a hard place”
Focus on Dementia | Testing the 8 Pillars Model | Perspective of staff | V 22.11.2015 Page 10
“I think my social work colleagues feel the exact same because they want to do their best as well but they are constrained by finances and budgets”.
We have got to prioritise; I get that. But I think prioritising resources is a bigger deal than they are giving it credit for. For example, the agenda around delayed discharge and reducing that. They justify prioritising this for homecare to get people out of hospital, but what about anticipatory care and prevention agendas?”
3.2.2 The integration of health and social care services going on in the background added to the uncertainty and complexity of testing the 8 pillars model in some test sites The 8 Pillars model encourages partner agencies to work together in service of people with dementia and their carers. The Dementia Practice Coordinator role is central to supporting partnership working in the community context for people with complex care needs. Practitioners referred to factors in their respective systems which helped and hindered the testing process e.g.
“It is a difficult time for us at the moment because we are going through integration and everybody is feeling a bit uneasy. I think it adds pressures and it isn’t clear who you should speak to about certain things, they may no longer be there or their role may have changed. From the project’s point of view it has been frustrating”
However, some practitioners reflected on how they were using the 8 Pillars process to influence change from the bottom up e.g.
“The DPC role will help to show the changes required in the system. We’re pushing the boundaries. We’re testing this and learning about what needs to change to allow this to happen. We’ve now got better co-ordination with the GPs”
3.3. Organisational Level 3.3.1 Although there were mixed views about being part of the national testing programme practitioners were hopeful that things would get better for people with dementia and their carers. Overall, practitioners were enthusiastic about being part of a test site. They saw it as providing permission to push at the boundaries and make improvements e.g. .
“I feel that the introduction of the dementia practice coordinator role has been welcomed as the one ‘go to person’, someone who can take forward your concerns and make arrangements” “I feel fortunate to be part of the process of 8 pillars testing and liaising with other services to make sure people have as good a package is possible” “Not to blow our own trumpets but (when you met with the carers) you were trying to get a sense of before and after. The people we picked for interviews were very much ‘before’, who haven’t had that support. I think if we had picked people who had, you’d be blown away”
However, some practitioners shared their worries about testing the 8 Pillars model e.g.
“On paper it looks good but now I’m a bit more despondent and worried about how this will be implemented as I don’t have buy-in from everyone to move this forward” “I think the biggest risk of this model is that it isn’t deliverable now and it isn’t sustainable in the future”
Focus on Dementia | Testing the 8 Pillars Model | Perspective of staff | V 22.11.2015 Page 11
“As a DPC I’m anxious about the reality of managing on a day to day basis”
The issue of commissioning was raised on a number of occasions and was seen by some practitioners as a stumbling block e.g.
“8 Pillars’ co-ordination as a vehicle could really help if only we could commission services for the individual. But that’s where the role is difficult”
Despite the concerns highlighted about the model the determination of some practitioners shone through. They were perhaps a little less focused on the model and more on its potential as a vehicle for improvement e.g.
“We changed our system because we were so concerned about younger people with dementia. We did this as a test. We get in there early to avoid crises. We were signposting at an early stage” “I feel hopeful that this might bring a bit of investment and support solutions to the problems we’re finding”
Some of the issues raised by practitioners were more personal and reflected the complex nature of testing the 8 Pillars model within the context of wider systemic change.
“There is a fear of the unknown, what is going to happen to me? How is it (the generic Dementia Practice Coordinator role) going to affect me and my professional role? I’m coming towards the end of my career but if I was younger I would certainly scared about where my profession would be heading”
3.4. National Level 3.4.1 Messages for Scottish Government, Policy Makers and the National Support Team A number of practitioners reflected that were pleased to be part of the solution. They particularly valued being part of a national improvement collaborative where they could share concerns, ideas and progress with others. Having their voice heard was important.
“I feel fortunate to be part of something which is continually trying to improve. There’s a lot of negativity around but I feel fortunate that the Government and bigger agencies are continually working to improve things for people with dementia. I’ve just recently qualified and so will still be in the system for the next 30-40 years. It will be great to be part of the continuing changes to make things better for people with dementia in the years to come” “I’m relieved we’re having conversations like this and that we are being listened to at a higher level and can make positive changes and progress” “Thank God it’s happening! It’s a good model and we’re testing and optimistic that this should be a better future for younger people with dementia and we hope there will be a more streamlined equitable access. Relived we’re doing this”
Conversely, some practitioners raised concerns about the possibility of tunnel vision with such an emphasis on dementia and that other conditions may become side-lined or subordinated, particularly where people had other long term conditions.
“One of my concerns is that we overlook other things which affect old people, like delirium or depression”. With 2/3 general hospital beds occupied by people over 65 with about 2/3 of those people experience delirium, dementia and/or depression and not enough is done for them”
Focus on Dementia | Testing the 8 Pillars Model | Perspective of staff | V 22.11.2015 Page 12
Some of the comments related to issues surfaced through testing the 8 Pillars Model which need to be considered in a national context.
“I think we perhaps still underestimate the inability of the very complex health and social care system to meet people’s needs in a very person centered way”. “The optimism needs to be tempered by a sense of realism that actually, this is always going to be complicated. The demand for things for people and families affected by dementia is always going to outstrip supply” “It feels like you are steering people down (the road of) what you’ve got rather than what they need”
Other policy imperatives were sometimes seen to get in the way of progress in testing the 8 Pillars Model. The inflexibility of systems was seen by some practitioners to limit their ability to find solutions to address the delays in services.
“The role is fine if the systems allow you to do that. But if the systems are not there to support you then you’re bumping up against it” “Part of the problem is that delayed discharge and moving people out of hospital will always get priority over people in the community who are waiting for care. That’s the issue with targets”
Finally, one practitioner reflected on the situation internationally and could see the progress that Scotland was making in that context.
“I’ve been fortunate to meet with other countries in Europe and UK and when you look at what we’ve achieved in Scotland with the dementia strategy and associated activities, in comparison with other countries it’s night and day. I met 2 women from Cyprus and they were developing services (to the whole of Cyprus – about half a million population) and there are two for the whole island. Some of the things she was describing made me appreciate what we have in Scotland”
4. CONCLUSIONS
Each test site is different in character and approach and as such there was a broad spectrum of views expressed across the focus groups. Emotional Touchpoints provided an extraordinary richness and depth of data. However, the approach may not have been structured enough for this context. Health and social care services across Scotland were in the midst of transitioning into Health and Social Care Partnerships. Responses to the Touchpoints were wide ranging making it difficult to extrapolate views about the 8 Pillars’ testing from staff experience of the integration of health and social care per se. Moreover, the uncertainty relating to the ‘shaky foundations’ typical of systemic change can make innovation more difficult. This appears to have coloured the perceptions of some practitioners. The progress they have made in the first half of the project is a credit to their tenacity. In the attempt to maintain anonymity the data from the three focus groups were brought together in one report. This means that not all of the issues raised would have been applicable across all test sites. Care was taken to select a cross section of quotes from each of the focus groups. Notwithstanding, test site managers may have found it more helpful to have a report relating to their own test sites. This is something to be considered if the focus groups are repeated. .
Focus on Dementia | Testing the 8 Pillars Model | Perspective of staff | V 22.11.2015 Page 13
The responses suggest that the sense of responsibility practitioners feel towards supporting people with dementia and their carers make any delays in service delivery difficult to contend with. This can lead to feelings of guilt and frustration. Success in meeting personal outcomes at the interface between the practitioner and the person with dementia and their carers will only be achieved, and sustained, if there is a commitment to delivery at every level within the system. Exploring staff experience within the context of the four system levels in Fig 1 has illuminated where some of the enablers and barriers lie. This gives rise to a number of questions for consideration by the local test sites in association with national improvement support team. 1) What are seen to be the main bottle-necks in relation to service delays and how might they be
addressed? 2) What might be needed to help practitioners feel more empowered in fulfilling the DPC role? 3) What is ‘in scope’ and ‘out of scope’ in relation to the role of a DPC? 4) To what extent has the distraction of the health and social care integration influenced how the
changes have been managed in test sites? 5) Building on the previous question, what opportunities has the integration of health and social
care brought to the 8 Pillars’ testing programme? The findings along with these questions should inform improvement activity within the test sites and guide the work of the 8 Pillars National Team during this final stage of testing.