Embed Size (px)
Citation preview

Resuscitation 45 (2000) 181–187
Termination of recent-onset atrial fibrillation/flutter in theemergency department: a sequential approach with intravenous
ibutilide and external electrical cardioversion
Hans Domanovits a,*, Martin Schillinger a, Jana Thoennissen a, Mariam Nikfardjam b,Karin Janata a, Martin Brunner c, Anton N. Laggner a
a Department of Emergency Medicine, Vienna General Hospital, Uni6ersity of Vienna, Medical School, Waehringer Guertel 18-20/6D,1090 Vienna, Austria
b Department of Cardiology, Vienna General Hospital, Uni6ersity of Vienna, Medical School, Waehringer Guertel 18-20/6D,1090 Vienna, Austria
c Department of Clinical Pharmacology, Vienna General Hospital, Uni6ersity of Vienna, Medical School, Waehringer Guertel 18-20/6D,1090 Vienna, Austria
Accepted 15 March 2000
Abstract
Safety and effectiveness are the goals in treating patients with arrhythmias. In an open prospective study, we observed theefficacy and safety of up to 2 mg intravenous ibutilide, a new class III antiarrhythmic agent in haemodynamically stable patientspresenting in the emergency department (ED) with symptoms of recent-onset (B48 h) atrial fibrillation/flutter. Arrhythmiatermination within 90 min, haemodynamic parameters and proarrhythmic effects were assessed. Non-responders to the ibutilideinfusion underwent external electrical cardioversion. We included 51 patients. In 31 patients therapeutic intervention withintravenous ibutilide was successful within 90 min (61%). In another seven patients conversion to sinus rhythm occurred after 90min without any other intervention (14%). Blood pressure remained stable and no relevant proarrhythmic effects were observed.The 13 patients who did not respond to ibutilide treatment underwent successful external electrical cardioversion. The overallconversion rate was 100%. Forty-seven patients (92%) were discharged within a median of 9 h and managed as outpatients. Inconclusion, in haemodynamically stable patients with recent-onset atrial fibrillation/flutter intravenous ibutilide and externalelectrical cardioversion for conversion to sinus rhythm turned out to be effective and safe. The short duration of admission makesthis strategy attractive for use in the ED. © 2000 Elsevier Science Ireland Ltd. All rights reserved.
Keywords: Atrial fibrillation/flutter; Electrical cardioversion; Emergency department; Intravenous ibutilide; Safety
www.elsevier.com/locate/resuscitation
1. Introduction
Atrial fibrillation, a common arrhythmia [1–3]may cause various haemodynamic complications.The association with chronic heart failure [2] andsubsequent cardioembolic events [4] leads to fre-quent hospitalisation [5] and considerable eco-nomic burden. Acute atrial fibrillation is the most
common form of paroxysmal supraventriculartachycardia in patients, who present to the emer-gency department (ED) [6,7]. Most of these pa-tients are admitted to the hospital to excludeserious underlying cardiac pathology as a causefor the arrhythmia and assessment for significantcomplications [8]. If patients experience adversesigns and symptoms clinicians should prepare forimmediate electrical cardioversion [9]. A quick,effective and safe treatment in haemodynamicallystable patients facilitating immediate discharge tohome from the ED and further evaluation on anoutpatient basis may help to reduce time of hospi-
* Corresponding author. Tel.: +43-1-40400-1964; fax: +43-1-40400-3953.
E-mail address: [email protected] (H. Do-manovits).
0300-9572/00/$ - see front matter © 2000 Elsevier Science Ireland Ltd. All rights reserved.PII: S 0 3 0 0 -9572 (00 )00180 -5

H. Domano6its et al. / Resuscitation 45 (2000) 181–187182
tal stay and costs. In haemodynamically stablepatients for acute conversion of atrial fibrillation/flutter, besides electrical cardioversion [10], severalantiarrhythmic agents [11–18] may be used. Un-fortunately unsatisfactory efficacy and proarrhyth-mic effects limit their applicability [1]. Recentlyibutilide, a new class III antiarrhythmic agentwhich works rapidly and is short acting, hasproven to be effective for conversion of atrialfibrillation and flutter to sinus rhythm [19–26].Efficacy for conversion ranges from 50 to 70%[20]. Therefore, further effort to improve conver-sion rates with safe and cost effective strategies iswarranted.
The aim of this study was to determine if pa-tients presenting to the ED with an episode ofrecent-onset atrial fibrillation/flutter can be man-aged effectively and safely using a sequential ap-proach with intravenous ibutilide and externalelectrical cardioversion.
2. Methods
2.1. Study design
In an open, non-randomised, prospective studypatients presenting with symptoms of recent-onset(B48 h duration) atrial fibrillation/flutter in theED of a 2200-bed university teaching hospitalwere included.
2.2. Inclusion and exclusion criteria
Patients, who are 18 years, with stable haemo-dynamic status and normal serum electrolytes (K\3.5 and Mg \0.7 mmol/l) were eligible. Weexcluded patients who did not strictly meet inclu-sion criteria and those who had a previous historyof or who actually suffered from a severe conges-tive heart failure, severe depressed ventricularfunction, tachyarrhythmia inducing haemody-namic instability, symptomatic bradycardia, sicksinus syndrome, sinoatrial block, second degree orcomplete atrioventricular block without protectionof an implanted pacemaker, myocardial infarctionwithin the last month, ventricular tachycardia andsevere hepatic disorders which may influencemetabolism or excretion of ibutilide. Patients witha known hypersensitivity to ibutilide or hypersen-sitivity to related drugs and patients receiving
treatment with other class III or class I an-tiarrhythmics were excluded. Female patients dur-ing pregnancy or lactation were not eligible.Informed consent was obtained from the patientsto participate in the study.
2.3. Definition of the endpoint
The primary criterion for the efficacy of ibu-tilide treatment was the termination of arrhythmiawithin 90 min after intravenous infusion. Separateconversion rates for atrial fibrillation, atrial flutterand atrial fibrillation/flutter were calculated.Safety was judged by changes in haemodynamicparameters (systolic blood pressure B80 mmHgand heart rate B50 beats per min) and the follow-ing ECG changes: temporary or persistent appear-ance of sinus bradycardia (heart rate B50 beatsper min), ventricular pauses (]2 s), first degreeAV — block (PQ time \0, 20 s), new bundlebranch block, torsades de pointes, non-sustainedventricular tachycardia, sustained ventriculartachycardia and corrected QT time prolongationover ]440 ms. Non-responders to intravenousibutilide underwent external electrical cardiover-sion using short term anaesthesia. The cumulativeconversion rate of arrhythmia to sinus rhythm wascalculated.
2.4. Monitoring and treatment
Initially a detailed medical history together withconcomitant medication was recorded and atwelve lead ECG was obtained. Chest X-ray and atransthoracic echocardiogram for exclusion ofsevere underlying cardiac disease or presence ofthrombus was performed in all patients. Afterinclusion, patients were placed on a monitor (HPSeries 600 Monitor, Product No. M-1166A,Hewlett-Packard, Paolo Alto, CA, USA) for con-tinuous ECG, non-invasive blood pressure, heartrate and pulse oxymetry monitoring. For preven-tion of conversion associated embolic events everypatient was treated by a combined administrationof at least 5000 IU of unfractioned heparin and100 IU/kg body weight of low molecular weightheparin (dalteparin). Clinical signs and symptomswere observed repetitively until 4 h after conver-sion to sinus rhythm with special attention toadverse events. All patients were continuouslymonitored for proarryhthmic effects for at least 4

H. Domano6its et al. / Resuscitation 45 (2000) 181–187 183
h after conversion to sinus rhythm with eithermethod or until normalisation of prolonged QTcinterval.
As first step, 1 mg of ibutilide was given intra-venously as an infusion over 10 min. The infusionwas stopped earlier if conversion to sinus rhythmoccurred during this interval. After 10 min intervala second infusion of 1 mg ibutilide over 10 minwas started if the arrhythmia persisted. Patientswith QT time prolongation (QTc]440 ms) afterapplication of the first mg ibutilide and those witha body weight B70 kg were not given a secondmg of ibutilide, they were electrically cardiovertedfor safety reasons. A complete twelve lead ECGand blood pressure were recorded before the ad-ministration of ibutilide and after the infusion at10, 20, 90 min and 4 h as well as immediately afterconversion to sinus rhythm. Heart rate wasderived from the ECG recordings.
In the second step, ibutilide non-responders un-derwent external electrical cardioversion. Foranaesthesia, fentanyl 0.1 mg in combination withup to 15 mg midazolam and/or 200 mg propofolwas administered intravenously. External electricalcardioversion was started with 200 J, with thepaddles in basal and apical position. The energywas increased if required up to 360 J maximum.After successful electrical cardioversion, patientswere continuously monitored for at least 4 h andwere discharged if they remained in sinus rhythmand were clinically stable.
2.5. Statistics
Continuous data are presented as median andthe 25th and 75th percentile (IQR). Percentagesare calculated for frequencies.
3. Results
A total of 51 patients were included in thestudy, comprising 42 males (82%) and 9 females(18%). The median age was 61 years (total range25–87 years). Thirty-four patients (67%) had ahistory of cardiovascular disease or other abnor-mal cardiovascular findings (Table 1). Atrial fibril-lation was present in 42 patients (82%), 6 patientshad atrial flutter and 3 patients had atrialfibrillation/flutter.
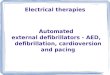
The treatment algorithm and response to treat-ment is shown in Fig. 1. In the first step, anintravenous infusion with 1 mg ibutilide over 10min was started in 51 patients, in 6 of thesearrhythmia converted to sinus rhythm prior tocompletion of 1 mg ibutilide administration andthe infusion was therefore stopped by administer-ing less than 1 mg. Twenty-six patients receivedmore than 1 mg (maximum 2 mg in 22 patients).Three patients with QT time prolongation afterapplication of the first mg ibutilide (QTc]440ms) and 4 patients with body weight B70 kg werenot given a second mg of ibutilide.
The cumulative conversion rate to sinus rhythmwas 41% after 30 min, 57% after 60 min and 61%(31 patients) within 90 min after intravenous ap-plication of ibutilide, 25 of 42 patients (60%) withatrial fibrillation converted to sinus rhythm; 4 of 6patients (67%) with atrial flutter; and 2 of 3 pa-tients (67%) with fibrillation/flutter. Later on, be-fore external electrical cardioversion wasattempted as the second step of the regimen, an-other 7 patients converted to sinus rhythm withoutany other intervention. The median heart rateoverall decreased from 132 (IQR 118–150) to 77(IQR 66–105) beats per min, but none of thepatients developed bradycardia; blood pressure re-mained stable (Fig. 2). In the group of ibutilideresponders (n=38) median heart rate decreasedfrom 133 (IQR 121–150) to 73 beats per min (IQR61–83). There was also a measurable reduction ofmedian heart rate in the group of patients who didnot convert to sinus rhythm after ibutilide infusion
Table 1Cardiovascular findings in 51 patients presenting with atrialfibrillation/flutter
Number ofpatients, n (%)
Hypertension 17 (33)9 (18)Val6ular heart disease5 (10)Prosthetic heart valve8 (16)Coronary artery disease3 (6)History of myocardial infarction
Cardiomyopathy 3 (6)2 (4)Pacemaker
Pre-existing incomplete right bundle 6 (12)branch block (QRSB0.12)
Pre-existing complete right bundle branch 1 (2)block (QRS\0.12)
3 (6)Pre-existing left bundle branch block(QRS\0.12)

H. Domano6its et al. / Resuscitation 45 (2000) 181–187184
Fig. 1. Treatment algorithm and response of the different steps; using a sequential approach of arrhythmia termination withibutilide and external electrical cardioversion in 51 patients with atrial fibrillation/flutter.
(n=13) from a median of 120 (IQR 115–129) to104 beats per min (IQR 101–110). Oxygen satura-tion remained within the range of 95–100% in allpatients. We did not observe any seriousproarrhythmic effects of ibutilide. ECG changeswithin 4 h after intravenous ibutilide are shown inTable 2. The most common ibutilide associatedeffect was an intermittent right bundle branchblock in 11 patients (22%). In 10 patients (20%) atemporary QTc time prolongation ]440 ms wasrecorded (maximum 480 ms in one patient). Noother adverse events of any kind were registered.
In the second step external electrical cardiover-sion was performed in 13 patients who did notrespond to ibutilide infusion. Atrial arrhythmiawas successfully terminated in all 13 patients.Thecumulative conversion rate of the sequential regi-men was 100% at 17 h after inclusion. Forty-sevenpatients (92%) were managed as outpatients at theED and discharged after median 9 h (IQR 5.5–16.5). Four patients (8%) were transferred to an-other ward for further observation due tounderlying disease (cerebrovascular disease, car-diomyopathy, valvular heart disease), all with sta-ble sinus rhythm.
Fig. 2. Blood pressure and heart rate within 4 h after ibutilideinfusion in 51 patients with atrial fibrillation/flutter. Datapresented as median and range from the 25th to the 75thpercentile (whiskers); [heart rate in beats per minute, fullcircle (); systolic blood pressure in mmHg, diamonds (");diastolic blood pressure in mmHg, squares ()].

H. Domano6its et al. / Resuscitation 45 (2000) 181–187 185
Table 2Proarrhythmic ECG changes within 4 h after intravenousibutilide infusion
Number ofpatients, n (%)
Intermittent complete right bundle 11 (22)branch block (QRS\0.12)
Temporary QTc time prolongation 10 (20)(]440 ms)
PQ time prolongation (\0.20 s) 1 (2)Sinus bradycardia (heart rate B50 beats 0
per min, ventricular pause (]2 s)Torsades de pointes, non sustained or 0
sustained ventricular tachycardia
tients receiving ibutilide cardiac output, pul-monary artery or capillary wedge pressure, bloodpressure, or heart rate were not significantly differ-ent from patients receiving placebo [31]. However,these patients were haemodynamically stable andin sinus rhythm. We observed a steady decrease ofmean heart rate after ibutilide infusion, which is inline with previously published data [24]. Heart ratenormalised in patients with successful conversionto sinus rhythm. In patients with ongoing arrhyth-mia a reduction of ventricular rate could be ob-served after ibutilide infusion. We foundprolongation of QTc in 10 of our patients (20%),which has been described previously in patientstreated with ibutilide [34]. Prolongation of repolar-isation is known to be associated with other classIII antiarrhythmic drugs [32,33]. We did not ob-serve serious proarrhythmia, in particular poly-morphic ventricular tachycardia and torsades depointes, in our patients compared withproarrhythmic events in 3–9% of patients treatedwith ibutilide described by others [20,22,34]. It hasbeen suspected that patients with marked impair-ment of left ventricular function are at higher riskfor proarrhythmic complications [34]. Exclusion ofpatients with severely depressed ventricular func-tion and the small number of patients includedmight explain the absence of serious proarrhyth-mic effects in our study. Thus, no conclusions canbe drawn with regard to the occurrence ofproarrhythmia in haemodynamically unstable pa-tients from our results. However, as proarrhyth-mia with hemodynamic deterioration may occur,adequate equipment and trained physicians in per-forming cardioversion/defibrillation are essentialfor an ED [35]. Most of the adverse events ofibutilide however occur in less than 1 h[20,22,24,29,30] and not more than 4 h of observa-tion is usually recommended. Thus, the short andrapid action and good tolerance seem to suggestibutilide an alternative to electrical cardioversionfor conversion of atrial fibrillation/flutter.
There are several reasons to attempt pharmaco-logical cardioversion of atrial fibrillation as initialstep; first it obviates the requirements of sedationor short term intravenous anaesthesia needed forelectrical methods. Second, electrical cardioversionis anticipated as a most unpleasant event by mostof the patients, which many preferably wouldavoid. Third, a delay after food ingestion to avoid
4. Discussion
We have evaluated a new sequential approachwith intravenous ibutilide and external electricalcardioversion for patients presenting with recent-onset atrial fibrillation/flutter in the ED. In thispatient series, the two step treatment regimen withintravenous ibutilide and external electrical car-dioversion for conversion of recent-onset atrialfibrillation/flutter resulted in a 100% success rate.
During the first therapeutic step with ibutilideinfusion arrhythmia was terminated in 61% of thepatients within 90 min. The efficacy compares wellwith results published in the literature [21,24]. Therapidity of action [20–22,24,27] and relativelyshort duration of effect [28] make ibutilide an idealcandidate for acute care. The conversion rate wassimilar in patients with atrial fibrillation, atrialflutter and atrial fibrillation/flutter. Others re-ported a significantly higher success rate for atrialflutter [22,29]. In seven patients arrhythmia termi-nation occurred more than 90 min after ibutilideinfusion. We interpret these cases of conversion asnot directly ibutilide associated, but conversionmay have been facilitated by the drug. Sponta-neous conversion is more probable. We found thatsystolic and diastolic blood pressure remained sta-ble during and after ibutilide administration inpatients with preserved left ventricular function asreported previously [19,30]. There is only one mul-ticenter, randomised, placebo controlled, study ad-dressing the acute haemodynamic effects ofintravenous ibutilide in 47 patients with or withoutreduced left ventricular ejection fraction. In pa-

H. Domano6its et al. / Resuscitation 45 (2000) 181–187186
aspiration of gastric contents is not required withthe drug treatment.
External electrical cardioversion, as step two,was successful in all 13 patients whose atrial fibril-lation/flutter was not converted by intravenousibutilide. In published series, success rate variesfrom about 70 to 95% [10]. Other authors reportedthat pre-treatment with ibutilide facilitates electri-cal cardioversion [34,36] and is associated with areduction in the mean energy required for defibril-lation [34]. Maybe the electrical cardioversion suc-cess rate in our study was influenced bypre-treatment with ibutilide. We did not observeany adverse events associated with electrical car-dioversion. However, electrical cardioversion isknown to be associated with thromboembolicevents, hypotension, ventricular dysrhythmias,pulmonary oedema, and pacemaker malfunction[37].
4.1. Limitations
Our results, obtained in a single centre in arelatively small number of patients need validationin larger number of patients. We did not includepatients whose recent episode of atrial fibrillation/flutter had lasted for more than 48 h. Sufficientanticoagulation for at least 3 weeks or exclusion ofcardiac embolism sources by transesophagealechocardiography prior to cardioversion would benecessary for this patient group. Thus, we do notknow the effectiveness of this approach for pa-tients with atrial fibrillation/flutter \48 h dura-tion. Because of the study design we do not knowhow many patients had spontaneous conversion tosinus rhythm. The rate of spontaneous cardiover-sion within 90 min has not been defined, but wewould expect a rate far below 60%.
4.2. Clinical implication
In haemodynamically stable patients, the se-quential management with ibutilide and externalelectrical cardioversion resulted in an excellentconversion rate of recent-onset (B48 h) atrialfibrillation/flutter to stable sinus rhythm. The ma-jority of patients could be managed as outpatientsin the ED and discharged after a median of 9 h,thus helping to save health care resources. Thistreatment strategy seems to be attractive for use inthe ED.
Acknowledgements
We thank Dr Marcus Mullner for critical reviewof the manuscript.
References
[1] Anderson JL. Acute treatment of atrial fibrillation andflutter. Am J Cardiol 1996;78(Suppl 8A):17–21.
[2] Camm AJ, Obel OA. Epidemiology and mechanism ofatrial fibrillation and flutter. Am J Cardiol1996;78(Suppl 8A):3–11.
[3] Kannel WB, Abbott RD, Savage DD, McNamara PM.Epidemiologic features of atrial fibrillation: the Fram-ingham study. New Engl J Med 1982;306:1018–22.
[4] Wolf PA, Dawber TR, Thomas HE, Kannel WB. Epi-demiologic assessment of chronic atrial fibrillation andrisk of stroke: the Framingham study. Neurology1978;28:973–7.
[5] Bialy D, Lehmann MH, Schumacher DN, Steinman RT,Meissner MD. Hospitalization for arrhythmias in theUnited States: importance of atrial fibrillation. J AmColl Cardiol 1992;19:41A.
[6] Connors S, Dorian P. Management of supraventriculartachycardia in the emergency department. Can J Cardiol1997;13(Suppl A):19A–24A.
[7] Mulcahy B, Coates WC, Henneman PL, Lewis RJ. Newonset atrial fibrillation: when is admission medicallyjustified? Acad Emerg Med 1996;3(2):114–9.
[8] Friedman HZ, Goldberg SF, Bonema JD, Cragg DR,Hauser AM. Acute complications associated with newonset atrial fibrillation. Am J Cardiol 1991;3:114–9.
[9] Guidelines for cardiopulmonary resuscitation and emer-gency cardiac care. J Am Med Assoc 1992;268:2171–302.
[10] Falk RH, Podrid PJ. Electrical cardioversion of atrialfibrillation. In: Falk RH, Podrid PJ, editors. AtrialFibrillation. Mechanisms and Management. New York,NY: Raven Press, 1992:181–95.
[11] Suttorp MJ, Singma JH, Lie-A-Huen L, Mast EG.Intravenous flecainide versus verapamil for acute con-version of paroxysmal atrial fibrillation or flutter tosinus rhythm. Am J Cardiol 1989;63:693–6.
[12] Donovan KD, Cobb DJ, Coombs LJ, Lee K-Y, WeekesJW, Murdock CJ, Clarke GM. Revision of recent-onsetatrial fibrillation to sinus by intravenous flecainide. AmJ Cardiol 1991;67:137–41.
[13] Fenster P, Comess KA, Marsh R, Katzenberg C, HagerWD. Conversion of atrial fibrillation to sinus rhythm byacute intravenous procainamide. Am Heart J1983;106:501–4.
[14] Chapman MJ, Moran JL, O’Fathartaigh ML, PeisachAR, Cunningham DM. Management of atrial tach-yarrhythmias in the critically ill: a comparison of intra-venous procainamide and amiodarone. Intensive CareMed 1993;19:48–52.
[15] Fujiki A, Yoshida S, Tani M, Inoue H. Efficacy of classI antiarrhythmic drugs in converting atrial fibrillation

H. Domano6its et al. / Resuscitation 45 (2000) 181–187 187
unassociated with organic heart disease and their rela-tion to atrial electrophysiologic characteristics. Am JCardiol 1994;74:282–3.
[16] Madrid AH, Moro C, Marin-Huerta E, Mestre JL,Novo L, Costa A. Comparison of flecainide and pro-cainamide in cardioversion of atrial fibrillation. EurHeart J 1993;14:1127–31.
[17] Capucci A, Villani GQ. Propafenone oral loading doseplus digitalis in converting atrial fibrillation to sinusrhythm: a placebo controlled multicenter trial. Circula-tion 1995;92:1–775.
[18] Sung RJ, Tan HL, Karagounis L, Hanyok JJ, Falk R,Platia E, Des G, Hardy LA. Intravenous sotalol for thetermination of supraventricular tachycardia and atrialfibrillation and flutter: a multicenter, randomized, dou-ble-blind, placebo controlled study. Am Heart J1995;129:739–48.
[19] Stambler BS, Wood MA, Ellenbogen KA. Antiarrhyt-mic actions of intravenous ibutilide compared with pro-cainamide during human atrial flutter and fibrillation.Circulation 1997;96:4298–306.
[20] Ellenbogen KA, Stambler BS, Wood MA, Saager PT,Wesley RC, Meissner MD, Zoble RG, Wakefield RK,Perry KT, VanderLugt JT. Efficacy of intravenous ibu-tilide for rapid termination of atrial fibrillation andatrial flutter: a dose–response study. J Am Coll Cardiol1996;28:130–6.
[21] Ellenbogen KA, Clemo HF, Stambler BS, Wood MA,VanderLugt JT. Efficacy of ibutilide for termination ofatrial fibrillation and flutter. Am J Cardiol1996;78(Suppl 8A):42–5.
[22] Stambler BS, Wood MA, Ellenbogen KA, Perry KT,Wakefield LK, VanderLugt JT. Efficacy and safety ofrepeated intravenous doses of ibutilide for rapid conver-sion of atrial flutter and fibrillation. Circulation1996;94:1613–21.
[23] Murray KT. Ibutilide. Circulation 1998;97:493–7.[24] Volgman AS, Carberry PA, Stambler BS, et al. Conver-
sion efficacy and safety of intravenous ibutilide andcompared with intravenous procainamid in patients withatrial flutter or fibrillation. Am J Cardiol 1998;31:1414–9.
[25] Buchanan LV, Turcotte VM, Kabell GG, Gibson JK.Antiarrhythmic and electrophysiologic effects of ibu-tilide in a chronic canine model of atrial flutter. JCardiovasc Pharmacol 1993;33:10–4.
[26] Nabih MA, Prcevski P, Fromm BS, Lavine SJ, ElnabtityM, Munir A, Steinmann RT, Meissner MD, Lehmann
MH. Effect of ibutilide, a new class III agent, on sus-tained atrial fibrillation in a canine model of acuteischemia and myocardial dysfunction induced by mi-croembolisation. PACE 1993;16:1975–83.
[27] Vos MA, Golitsyn SR, Stangl K, Ruda MY, Van WijkL, Harry JD, Perry KT, Touboul P, Steinbeck G,Wellens HJJ. Superiority of ibutilide (a new class IIIagent) over DL-sotalol in converting atrial flutter andatrial fibrillation. Heart 1998;79:568–75.
[28] Naccarelli GV, Lee KS, Gibson JK, VanderLugt J.Electrophysiology and pharmacology of ibutilide. Am JCardiol 1996;78(Suppl 8A):12–6.
[29] Abi-Mansour P, Carberry PA, McCowan RJ, HenthornRW, Dunn GH, Kimberly TP. Conversion efficacy andsafety of repeated doses of ibutilide in patients withatrial flutter and atrial fibrillation. Am Heart J1998;136:632–42.
[30] Kowey PR, VanderLugt JT, Luderer JR. Safety andrisk/benefit analysis of ibutilide for acute conversion ofatrial fibrillation/flutter. Am J Cardiol 1996;78(Suppl8A):46–52.
[31] Stambler BS, Beckman KJ, Kadish AH, Camm JA,Ellenbogen KA, Perry KT, VanderLugt JT. Acutehemodynamic effects of intravenous ibutilide in patientswith or without reduced left ventricular function. Am JCardiol 1997;80:458–63.
[32] Van Gelder IC, Brugemann J, Crijins HJ. Current treat-ment recommendations in antiarrhythmic therapy.Drugs 1998;55:331–46.
[33] Singh BN. Antiarrhythmic actions of amiodarone: aprofile of a paradoxical agent. Am J Cardiol1996;78:41–53.
[34] Oral H, Souza JJ, Michaud GF, Knight BP, Goyal R,Strickberger A, Morady F. Facilitating transthoraciccardioversion of atrial fibrillation with ibutilide pretreat-ment. New Engl J Med 1999;340:1849–54.
[35] Domanovits H, Paulis M, Nikfardjam M, Holzer M,Stuhlinger HG, Hirschl MM, Laggner AN. Sustainedventricular tachycardia in the emergency department.Resuscitation 1999;42:19–25.
[36] Wesley RC, Farkhani F, Morgan D, Zimmermann D.Ibutilide: enhanced defibrillation via plateau sodium cur-rent activation. Am J Physiol 1993;264:H1269–74.
[37] Bjerkelund O, Orning OM. An evaluation of DC shocktreatment of atrial arrhythmias: immediate results andcomplications in 437 patients with long term results inthe first 290 of these. Acta Med Scand 1968;184:481–91.
..






















![Check List Cardioversion I.gallastegi[1]](https://img.dokumen.tips/doc/110x75/55cf8e57550346703b912349/check-list-cardioversion-igallastegi1.jpg)