Embed Size (px)
Citation preview

Techniques of Mandibular and Techniques of Mandibular and Maxillary AnesthesiaMaxillary Anesthesia
Dr. Mumena C.HDr. Mumena C.H

IntroductionIntroduction
Choice of anesthesiaChoice of anesthesia Mandibular techniqueMandibular technique Maxillary techniqueMaxillary technique

Choice of LAChoice of LA
3 Important factors;3 Important factors;– Specific nerve to be blocked,Specific nerve to be blocked,– Onset of action,Onset of action,– Duration action,Duration action,

Duration of actionDuration of action
The duration of action of LA may vary from The duration of action of LA may vary from 30min to 180 minutes or longer,30min to 180 minutes or longer,
Duration is related to dosage, increasing dosage Duration is related to dosage, increasing dosage increases duration,increases duration,
Duration can be increased by adding Epinephrine Duration can be increased by adding Epinephrine (vasoconstrictor) to the local anaesthesia,(vasoconstrictor) to the local anaesthesia,
Duration of action differs for different agentsDuration of action differs for different agents NB. Read the properties of each agent.NB. Read the properties of each agent.

Nerve to be blockedNerve to be blocked
Small nerves are in general easier to be Small nerves are in general easier to be block than larger onces,block than larger onces,
Nerve endings and cutaneous nerves are Nerve endings and cutaneous nerves are easily and quickly blocked by low easily and quickly blocked by low concentration of drug given by infiltration,concentration of drug given by infiltration,

Onset of actionOnset of action
Depending on the type of operation, e.g Depending on the type of operation, e.g acute pain then rapid onset required,acute pain then rapid onset required,

Review Anat. Trigeminal nerveReview Anat. Trigeminal nerve
55thth cranial nerve. cranial nerve. Major sensory of the face, mouth and nasal cavity.Major sensory of the face, mouth and nasal cavity. Motor and proprioceptive innervation to muscles of Motor and proprioceptive innervation to muscles of
mastication.mastication. Origin-Origin-
– Sensory neurons-upper part of pons,Sensory neurons-upper part of pons,– Motor neurons-inferior surface of ponsMotor neurons-inferior surface of pons
3 divisions 3 divisions • Ophthalmic, Ophthalmic, • maxillary, and maxillary, and • mandibular).mandibular).
Successful practice of dentistry is based on blockade of the Successful practice of dentistry is based on blockade of the various branches of these nerves.various branches of these nerves.

Mandibular nerveMandibular nerve
33rdrd and largest branch of trigeminal nerve. and largest branch of trigeminal nerve. Composed of Composed of
– motor and sensory roots.motor and sensory roots. Exits craniumExits cranium
– foramen ovaleforamen ovale.. Motor innervation to the muscles of mastication.Motor innervation to the muscles of mastication.

Mandibular nerveMandibular nerve
Sensory to mandibular teeth and gingiva, lower Sensory to mandibular teeth and gingiva, lower lip, cheek, anterior two thirds of the tongue, lip, cheek, anterior two thirds of the tongue, auricle and skin over temporal region.auricle and skin over temporal region.
Braches – Braches – – Inferior alveolar nerve,Inferior alveolar nerve,– Lingual nerveLingual nerve– Buccal nerveBuccal nerve– Mental nerveMental nerve– Incisive nerveIncisive nerve

Inferior alveolar nerve block in DentalInferior alveolar nerve block in Dental
Inferior alveolar nerve together with lingual Inferior alveolar nerve together with lingual nerve are anesthetized by the same or different nerve are anesthetized by the same or different injections.injections.
Lingual nerve Lingual nerve – mucous membrane of the floor of mouth, mucous membrane of the floor of mouth,
anterior 2/3 of tongue and lingual gingiva.anterior 2/3 of tongue and lingual gingiva. I.A.n I.A.n
– mandibular teeth and surrounding hard and mandibular teeth and surrounding hard and soft tissue up to the midline, exception soft tissue up to the midline, exception buccal soft tissues in the molar area.buccal soft tissues in the molar area.

Inferior alveolar nerve block in Inferior alveolar nerve block in DentalDental
Anatomical landmarks Anatomical landmarks – anterior border of ramus, external and internal anterior border of ramus, external and internal
oblique ridges, the coronoid notch, retromolar oblique ridges, the coronoid notch, retromolar triangle and pterygomandibular ligament.triangle and pterygomandibular ligament.
Target area for injectionTarget area for injection– mandibular foramen located in the mid-portion mandibular foramen located in the mid-portion
of ramus and 1 cm above the occlusal plane. of ramus and 1 cm above the occlusal plane. » Sometimes found in the area between mid-portion Sometimes found in the area between mid-portion
of ramus and posterior 1/3 of ramus.of ramus and posterior 1/3 of ramus.

Inferior alveolar nerve block in Dental Inferior alveolar nerve block in Dental cont…cont…
Several technique elaborated Several technique elaborated – difficulty of locating mandibular foramen hence LA failure.difficulty of locating mandibular foramen hence LA failure.
There is two techniques:There is two techniques: Traditional technique, Traditional technique,
– Direct techniqueDirect technique
– Indirect technique Indirect technique
Alternative technique;Alternative technique;– High ramus –neck of condyle approach (Gow-gates High ramus –neck of condyle approach (Gow-gates
technique) and technique) and
– Tuberosity approach (Akinos technique)-Tresmus.Tuberosity approach (Akinos technique)-Tresmus.

Inferior alveolar Nerve Block Inferior alveolar Nerve Block AnesthesiaAnesthesia
Lower success rate than Maxillary anesthesia - Lower success rate than Maxillary anesthesia - approx. 80-85 %approx. 80-85 %
Related to bone densityRelated to bone density Less access to nerve trunks Less access to nerve trunks Most commonly performed techniqueMost commonly performed technique Has highest failure rate (15-20%)Has highest failure rate (15-20%) Success depends on depositing solution within 1 mm Success depends on depositing solution within 1 mm
of nerve trunkof nerve trunk

Inferior Alveolar Nerve BlockInferior Alveolar Nerve Block
Not a complete mandibular nerve block.Not a complete mandibular nerve block. Requires supplemental buccal nerve blockRequires supplemental buccal nerve block May require infiltration of incisors or May require infiltration of incisors or
mesial root of first molarmesial root of first molar

Inferior Alveolar Nerve BlockInferior Alveolar Nerve Block
Nerves anesthetizedNerves anesthetized
Inferior AlveolarInferior Alveolar
MentalMental
Incisive Incisive
LingualLingual

Inferior Alveolar Nerve BlockInferior Alveolar Nerve Block
Areas AnesthetizedAreas Anesthetized– Mandibular teeth to midlineMandibular teeth to midline
– Body of mandible, inferior ramus Body of mandible, inferior ramus – Buccal mucosa anterior to mental foramenBuccal mucosa anterior to mental foramen– Anterior 2/3 tongue & floor of mouthAnterior 2/3 tongue & floor of mouth– Lingual soft tissue and periosteumLingual soft tissue and periosteum

Inferior Alveolar Nerve BlockInferior Alveolar Nerve Block
IndicationsIndications– Multiple mandibular teethMultiple mandibular teeth
– Buccal anterior soft tissueBuccal anterior soft tissue– Lingual anesthesiaLingual anesthesia

Inferior Alveolar Nerve Block Inferior Alveolar Nerve Block
ContraindicationsContraindications– Infection/inflammation at injection siteInfection/inflammation at injection site
– Patients at risk for self injury (eg. children)Patients at risk for self injury (eg. children)

Inferior Alveolar Nerve BlockInferior Alveolar Nerve Block
10%-15% positive aspiration10%-15% positive aspiration

Inferior Alveolar Nerve BlockInferior Alveolar Nerve Block
Supplemental injectionSupplemental injection– Periodontal ligament injection (PDL)Periodontal ligament injection (PDL)
– IntraseptalIntraseptal

Inferior Alveolar Nerve Block Inferior Alveolar Nerve Block
Target AreaTarget Area– Inferior alveolar nerve, near mandibular foramenInferior alveolar nerve, near mandibular foramen
LandmarksLandmarks– Coronoid notchCoronoid notch
– Pterygomandibular raphePterygomandibular raphe– Occlusal plane of mandibular posterior teeth Occlusal plane of mandibular posterior teeth
(molars).(molars).

Inferior Alveolar Nerve BlockInferior Alveolar Nerve Block
PrecautionsPrecautions– Do not inject if bone not contactedDo not inject if bone not contacted
– Avoid forceful bone contactAvoid forceful bone contact– Avoid use of cold agentsAvoid use of cold agents

Inferior Alveolar Nerve BlockInferior Alveolar Nerve Block
Failure of AnesthesiaFailure of Anesthesia– Injection too lowInjection too low
– Injection too anteriorInjection too anterior– Accessory innervationAccessory innervation
-Mylohyoid nerve-Mylohyoid nerve
-contralateral Incisive nerve innervation-contralateral Incisive nerve innervation

Inferior Alveolar Nerve BlockInferior Alveolar Nerve Block
ComplicationsComplications– HematomaHematoma
– TrismusTrismus– Facial paralysis (Inject into parotid gland).Facial paralysis (Inject into parotid gland).
Inferior Alveolar Nerve BlockInferior Alveolar Nerve Block
General hints: TechniqueGeneral hints: Technique– Apply topicalApply topical
– Area of insertionArea of insertion::
» medial ramus, mid-coronoid notch,medial ramus, mid-coronoid notch,
» level with occlusal plane (1 cm above),level with occlusal plane (1 cm above),» 3/4 posterior from coronoid notch to 3/4 posterior from coronoid notch to
pterygomandibular raphepterygomandibular raphe» advance to bone (20-25 mm)advance to bone (20-25 mm)

Traditional technique of inferior alveolar Traditional technique of inferior alveolar nerve block-Direct techniquenerve block-Direct technique
Palpate the oblique ridge in the oral vestibule with index Palpate the oblique ridge in the oral vestibule with index finger.finger.– Follow it posteriorly to where it ascends as sharp anterior border Follow it posteriorly to where it ascends as sharp anterior border
of the ramus of mandible.of the ramus of mandible. Move the finger to the temporal crest (internal oblique Move the finger to the temporal crest (internal oblique
line) of the mandible and is left in this position.line) of the mandible and is left in this position. The finger is now in the retromolar fossa with the finger The finger is now in the retromolar fossa with the finger
nail backwards.nail backwards.

Traditional technique of inferior alveolar Traditional technique of inferior alveolar nerve block-Direct techniquenerve block-Direct technique
Draw an imaginary line from point between Draw an imaginary line from point between the occlusal surfaces of the two premolars the occlusal surfaces of the two premolars in the opposite quadrant to the midpoint of in the opposite quadrant to the midpoint of the fingernail.the fingernail.
This imaginary line when extended This imaginary line when extended posteriorly ends just above the mandibular posteriorly ends just above the mandibular foramen.foramen.
Therefore the syringe needle will be Therefore the syringe needle will be directed along this line.directed along this line.

Traditional technique of inferior alveolar Traditional technique of inferior alveolar nerve block-Indirect techniquenerve block-Indirect technique
After locating the injection site the syringe is held After locating the injection site the syringe is held parallel to the mandibular occlusal plane on the parallel to the mandibular occlusal plane on the same side as the tooth to be blocked.same side as the tooth to be blocked.
The needle is directed approximately 1 cm (with The needle is directed approximately 1 cm (with the syringe) above the mandibular arch. the syringe) above the mandibular arch.
Aspirate the needle and inject 0.5 ml of LA for Aspirate the needle and inject 0.5 ml of LA for lingual nerve.lingual nerve.
Then move the syringe to the other side of the arch Then move the syringe to the other side of the arch over the opposite premolars teeth.over the opposite premolars teeth.

Alternative technique-Alternative technique-
More reliable.More reliable.– Gow gates technique;Gow gates technique;
• Also known as high ramus- neck of condyle approach.Also known as high ramus- neck of condyle approach.• Penetration into the oral mucosa is along the medial border of the Penetration into the oral mucosa is along the medial border of the
mandibular ramus lateral to the pterygomandibular depression, but mandibular ramus lateral to the pterygomandibular depression, but medial to the temporalis muscle tendon.medial to the temporalis muscle tendon.
• The needle inserted along a line extending from the corner of the The needle inserted along a line extending from the corner of the mouth opposite the site of injectionmouth opposite the site of injection
• The needle should be 25G and usually 1in long.The needle should be 25G and usually 1in long.• The needle should advanced until bone is contacted and then The needle should advanced until bone is contacted and then
withdrawn 1 mm.withdrawn 1 mm.• Anesthetic solution deposited after negative aspirationAnesthetic solution deposited after negative aspiration







Alternative technique- cont…Alternative technique- cont…
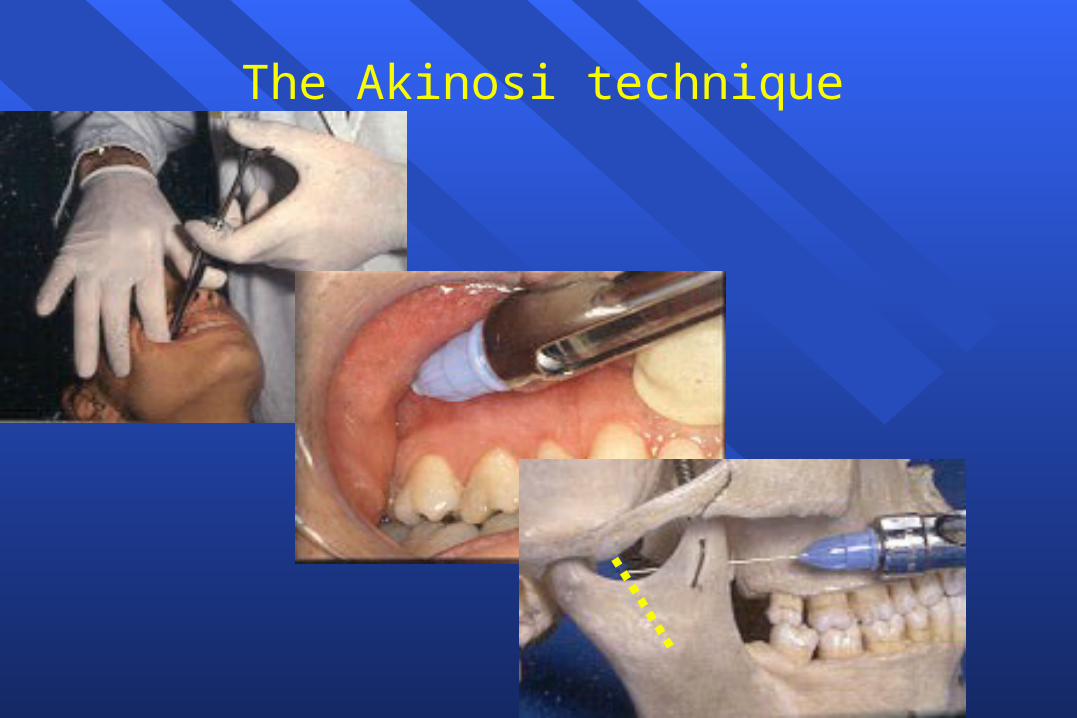
– Akinos technique;Akinos technique;» Also known as Tuberosity approach.Also known as Tuberosity approach.
» This technique is useful where patient has intense This technique is useful where patient has intense trismus.trismus.
» Mucosa is penetrated along the medial surface of the Mucosa is penetrated along the medial surface of the mandibular ramus.mandibular ramus.
» The mouth is kept closed (teeth in occlusion) with The mouth is kept closed (teeth in occlusion) with the cheek and muscles of mastication relaxed.the cheek and muscles of mastication relaxed.
» The same needle side.The same needle side.
» The depth of penetration is 1 ½ inches.The depth of penetration is 1 ½ inches.
The Akinosi technique

The Akinositechnique

Avoiding self-inflicted traumaAvoiding self-inflicted trauma
reduce area of soft tissue anaesthesiareduce area of soft tissue anaesthesia– intraligamentary anaesthesiaintraligamentary anaesthesia
– intra-osseous anaesthesiaintra-osseous anaesthesia
– palatal approaches to pulppalatal approaches to pulp




Intraligamentary anaesthesia
pulp
dentine
intraligamentaryinjection
gingiva
pdl
alveolus

Intraligamentary anaesthesia
pulp
dentine
intraligamentaryinjection
gingiva
alveolus

Intraligamentary anaesthesia
pulp
dentine
intraligamentaryinjection
gingiva
alveolus

Intraligamentary anaesthesia
pulp
dentine
intraligamentaryinjection
gingiva
alveolus

Intraligamentary and intra-osseous anaesthesia
pulp
dentine
intra-osseousinjection
intraligamentaryinjection
alveolus
gingiva

Intraligamentary and intra-osseous anaesthesia
pulp
dentine
intra-osseousinjection
intraligamentaryinjection
alveolus
gingiva

Success of intraligamentary Success of intraligamentary anaesthesia depends on:anaesthesia depends on:
toothtooth– least successful with lower incisorsleast successful with lower incisors
solutionsolution– dependent upon vasoconstrictor concentrationdependent upon vasoconstrictor concentration


self-aspirating
} aspirating
non-aspirating


syringe
needle
cartridge
basal diaphragm aspirating nipple
aspiration force
diaphragm deformation
basal diaphragmrecoils

Force
Time
initial aspiration force
subsequentforce

Buccal nerve blockBuccal nerve block
Anterior branch of Mandibular nerve (V3)Anterior branch of Mandibular nerve (V3) Provides buccal soft tissue anesthesia adjacent to Provides buccal soft tissue anesthesia adjacent to
mandibular molarsmandibular molars Not required for most restorative proceduresNot required for most restorative procedures Buccal is blocked by the injection in the buccal Buccal is blocked by the injection in the buccal
mucosa right to the 3mucosa right to the 3rdrd molar just above the molar just above the occlusal plane.occlusal plane.

Buccal Nerve BlockBuccal Nerve Block
IndicationsIndicationsAnesthesia required - mucoperiosteum buccal Anesthesia required - mucoperiosteum buccal
to mandibular molarsto mandibular molars ContraindicationsContraindications
Infection/inflammation at injection siteInfection/inflammation at injection site

Buccal Nerve BlockBuccal Nerve Block
AdvantagesAdvantages
Technically easyTechnically easy
High success rateHigh success rate
DisadvantagesDisadvantages
DiscomfortDiscomfort

Buccal Nerve BlockBuccal Nerve Block
AlternativesAlternatives
Buccal infiltrationBuccal infiltration
PDLPDL
IntraseptalIntraseptal

Buccal Nerve BlockBuccal Nerve Block
LandmarksLandmarks
Mandibular molarsMandibular molars
Mucobuccal foldMucobuccal fold

Buccal Nerve BlockBuccal Nerve Block
ComplicationsComplications
Hematoma (unusual)Hematoma (unusual)
Positive aspirationPositive aspiration
0.7 %0.7 %
Long Buccal Nerve BlockLong Buccal Nerve Block
Technique;Technique;– Apply topicalApply topical
– Retract the cheek Retract the cheek
– Insert the needle distal to the tooth with the syringe Insert the needle distal to the tooth with the syringe horizontal into the buccal fold.horizontal into the buccal fold.
– About 0.5 ml of LA solution is injected.About 0.5 ml of LA solution is injected.
– The barrel of the needle should be facing downwards. The barrel of the needle should be facing downwards.



Mental nerve blockMental nerve block
Mental nerve exits mandible through mental Mental nerve exits mandible through mental foramen.foramen.
The foramen is located between root apices The foramen is located between root apices of 1of 1stst and 2 and 2ndnd premolrs. premolrs.
Technique; Technique; – Insert the needle at an angle to the bony canal Insert the needle at an angle to the bony canal
towards the mental foramen.towards the mental foramen.– Inject 1-1.5 ml LA solution, another injection is Inject 1-1.5 ml LA solution, another injection is
required in the lingual gingiva and mucosa. required in the lingual gingiva and mucosa.

Mental Nerve BlockMental Nerve Block
Provides sensory innervation to buccal soft Provides sensory innervation to buccal soft tissue anterior to mental foramen, lip and tissue anterior to mental foramen, lip and chin chin
Mental Nerve BlockMental Nerve Block
IndicationIndication
Need for anesthesia in innervated areaNeed for anesthesia in innervated area
ContraindicationContraindication
Infection/inflammation at injection siteInfection/inflammation at injection site

Mental Nerve BlockMental Nerve Block
AdvantagesAdvantages
Easy, high success rateEasy, high success rate
Usually atraumaticUsually atraumatic
DisadvantageDisadvantage
HematomaHematoma

Mental Nerve BlockMental Nerve Block
AlternativesAlternatives
Local infiltrationLocal infiltration
PDLPDL
IntraseptalIntraseptal
Inferior alveolar nerve blockInferior alveolar nerve block
Gow GatesGow Gates

Mental Nerve BlockMental Nerve Block
ComplicationsComplications
FewFew
HematomaHematoma
Positive aspirationPositive aspiration
5.7 %5.7 %





Incisive Nerve BlockIncisive Nerve Block
Terminal branch of IAN Terminal branch of IAN Originates in mental foramen and proceeds Originates in mental foramen and proceeds
anteriorlyanteriorly
Good for bilateral anterior anesthesia Good for bilateral anterior anesthesia
Not effective for anterior lingual anesthesia Not effective for anterior lingual anesthesia

Incisive Nerve BlockIncisive Nerve Block
Nerves anesthetizedNerves anesthetized
IncisiveIncisive
MentalMental

Incisive Nerve BlockIncisive Nerve Block
Areas AnesthetizedAreas Anesthetized
Mandibular labial mucous membranesMandibular labial mucous membranes
Lower lip / skin of chinLower lip / skin of chin
Incisor, cuspid and bicuspid teethIncisor, cuspid and bicuspid teeth

Incisive Nerve BlockIncisive Nerve Block
IndicationIndication
Anesthesia of pulp or tissue required Anesthesia of pulp or tissue required anterior to mental foramenanterior to mental foramen
ContraindicationContraindication
Infection/inflammation at injection siteInfection/inflammation at injection site

Incisive Nerve BlockIncisive Nerve Block
AdvantagesAdvantages
High success rateHigh success rate
Pulpal anesthesia w/o lingual anesthesiaPulpal anesthesia w/o lingual anesthesia
DisadvantagesDisadvantages
Lack of lingual or midline anesthesiaLack of lingual or midline anesthesia

Incisive Nerve BlockIncisive Nerve Block
ComplicationsComplications
HematomaHematoma
Positive aspirationPositive aspiration
5.7 %5.7 %

Maxillary nerveMaxillary nerve
Foramen rotundumForamen rotundum Courses Courses
– pterygopalatine fossa & infraorbital canal.pterygopalatine fossa & infraorbital canal. Exit the face through infraorbital foramen.Exit the face through infraorbital foramen. Supply Supply
– sensory innervation-maxillary teeth, gingiva, maxillary sinus, sensory innervation-maxillary teeth, gingiva, maxillary sinus, hard & soft palate, lower eyelid, side of the nose, upper lip, hard & soft palate, lower eyelid, side of the nose, upper lip, mucous membrane of nasopharynx, and skin over the anterior mucous membrane of nasopharynx, and skin over the anterior temporal region.temporal region.
Necessary to block one or more of nerve or branches listed Necessary to block one or more of nerve or branches listed above.above.
3 branches: Posterior, middle & anterior superior alveolar 3 branches: Posterior, middle & anterior superior alveolar nervesnerves

Maxillary nerve cont…Maxillary nerve cont…
Posterior superior alveolar nerve-all molars except Posterior superior alveolar nerve-all molars except mesiobuccal root of 1mesiobuccal root of 1stst molar. molar.
Technique-Technique-– Dry area with gauze,Dry area with gauze,– Apply topical anesthesiaApply topical anesthesia– Insert palpating finger into muccobuccal fold of maxilla till Insert palpating finger into muccobuccal fold of maxilla till
contacts the zygomatic arch at it juncture with maxillary bone.contacts the zygomatic arch at it juncture with maxillary bone.– Cheek retracted gentle laterally,Cheek retracted gentle laterally,– Mouth partially opened.Mouth partially opened.– Long needle 1 5/8 inches inserted through maxillary mucosa at 45Long needle 1 5/8 inches inserted through maxillary mucosa at 4500
angle to all 3 planes of orientation.angle to all 3 planes of orientation.– Advance needle slowly in this orientation.Advance needle slowly in this orientation.– This ensure deposition of LA soln in close proximity to the nerve This ensure deposition of LA soln in close proximity to the nerve
as it enters its foramina.as it enters its foramina.

Maxillary nerve cont…Maxillary nerve cont…
– Avoids contact with the ptrygoid plexus of veins.Avoids contact with the ptrygoid plexus of veins.– Needle should be advanced to a depth of one half to two thirds of the Needle should be advanced to a depth of one half to two thirds of the
dental needle.dental needle.– Inject slowly two thirds of LA soln after negative aspiration.Inject slowly two thirds of LA soln after negative aspiration.– Withdraw needle the remaining one third may be used to block Withdraw needle the remaining one third may be used to block
mesiobuccal root of 1mesiobuccal root of 1stst molar. molar. Middle superior alveolar nerve-located within the maxilla.Middle superior alveolar nerve-located within the maxilla.
– Innervate mesiobuccal root of 1Innervate mesiobuccal root of 1stst molar, premolars, antral lining molar, premolars, antral lining corresponding to these teeth and buccal alveolar bone and soft tissues corresponding to these teeth and buccal alveolar bone and soft tissues in this area.in this area.
– Technique;Technique;• Retract cheek mucosa after preparation as described previously.Retract cheek mucosa after preparation as described previously.• 1 to 1 5/8 inches needle should be used.1 to 1 5/8 inches needle should be used.• Orient needle so that it conforms to the maxilla curvature in this area. Orient needle so that it conforms to the maxilla curvature in this area.

Maxillary nerve cont…Maxillary nerve cont…
• Advance slowly to a depth where whereby its tip approximates the Advance slowly to a depth where whereby its tip approximates the level of the apices of the premolar teeeth.level of the apices of the premolar teeeth.
• Inject slowly following negative aspiration.Inject slowly following negative aspiration.• LA diffuses through the maxilla blocking the MSAn. LA diffuses through the maxilla blocking the MSAn.
Anterior superior alveolar nerve (ASAn)- supply Anterior superior alveolar nerve (ASAn)- supply canine, lateral and central incisors, buccal alveolar canine, lateral and central incisors, buccal alveolar bone, and soft tissues in this region.bone, and soft tissues in this region.– Technique;Technique;
• 1 to 1 5/8 inches needle.1 to 1 5/8 inches needle.• Needle inserted and advanced slowly along the long canine Needle inserted and advanced slowly along the long canine
eminence,eminence,• Until tip approximates the level of the apex of canine tooth.Until tip approximates the level of the apex of canine tooth.• Inject slowly after negative aspiration.Inject slowly after negative aspiration.

Maxillary nerve cont…Maxillary nerve cont…
Greater palatine nerve (GPn)- exit into the hard palate Greater palatine nerve (GPn)- exit into the hard palate though greater palatine foramen located at level of 1 cm though greater palatine foramen located at level of 1 cm above margin of palatal gingiva and between 2above margin of palatal gingiva and between 2ndnd and 3 and 3rdrd molar.molar.– Technique; Technique;
» Insert the needle slightly anterior to the greater palatine (depression Insert the needle slightly anterior to the greater palatine (depression btn 2btn 2ndnd & 3 & 3rdrd Molars) foramen and perpendicular to the hard palate. Molars) foramen and perpendicular to the hard palate.
» The needle advanced to contact the bone.The needle advanced to contact the bone.» Withdraw 2mm and approximately one fourth of a dental cartilage Withdraw 2mm and approximately one fourth of a dental cartilage
(0.5 ml) injected.(0.5 ml) injected. Nasopalatine nerve (NPn)- enters oral cavity through Nasopalatine nerve (NPn)- enters oral cavity through
incisive foramen, located in the midline of the anterior incisive foramen, located in the midline of the anterior hard palate directly beneath incisive papilla.hard palate directly beneath incisive papilla.– Technique; insert a needle into the incisive papilla at an angleTechnique; insert a needle into the incisive papilla at an angle

Maxillary nerve cont…Maxillary nerve cont…
– To the midline and advanced until the rim of the foramen is To the midline and advanced until the rim of the foramen is contacted.contacted.
– Needle withdrawn 1-2 mm and one fourth of a dental cartilage Needle withdrawn 1-2 mm and one fourth of a dental cartilage injected following negative aspiration.injected following negative aspiration.
Infra-orbital block; exits via infra orbital firamen,Infra-orbital block; exits via infra orbital firamen,– Technique; foramen located in vertical line with the pt’s pupil as Technique; foramen located in vertical line with the pt’s pupil as
he looks straight ahead.he looks straight ahead.– Palpate the foramen, retract the cheek to expose the buccal Palpate the foramen, retract the cheek to expose the buccal
vestibule adjacent to the bicuspids.vestibule adjacent to the bicuspids.– Insert the needle between bicuspids and parallel to their long axes.Insert the needle between bicuspids and parallel to their long axes.– Penetrate far to enough to reach infra orbital foramen.Penetrate far to enough to reach infra orbital foramen.– Following negative aspiration deposit LA. Following negative aspiration deposit LA. – It is possible to produce unilateral analgesia of I, C, P, and It is possible to produce unilateral analgesia of I, C, P, and
mesiobuccal root of 1mesiobuccal root of 1stst molar. molar.

Palatal access

I hope L.A is the bridge to Effective I hope L.A is the bridge to Effective surgical procedures.surgical procedures.
BEST OF LUCKYBEST OF LUCKY





























