Embed Size (px)
Citation preview

Medical Education 1988, 22, I 1-14
Teaching school health to undergraduate medical students
V. O ’ H A R A t , J . C . V A N C E S & D. M c M I L L A N S
tDivision of Child Health, Department of Health, State Government of Queensland, Fortitude Valley, Queensland and $University Department of Child Health, Matev Children’s Hospital, South Brisbane, Queensland
Summary-This paper describes a teaching pro- gramme for final- (sixth-) year undergraduate medical students during their 10-week term in child health. Students attend schools on two occasions and are actively involved in the physi- cal, educational and emotional assessment of children. The advantages of the programme include active participation by the students, con- tact with children in a less threatening environ- ment, learning new skills in the assessment of children, and knowledge of common screening procedures. Student evaluation of the pro- gramme has been positive.
Key words: paediatrics/*educ; *education, medical, undergraduate; teaching/methods; school health services; curriculum; Australia
Introduct ion
As the management ofacute medical disorders in children has improved, an increasing proportion of the paediatrician’s time is taken up with the care of children with what has been called the ‘new morbidity’ (Haggerty et al . 197s). This includes behavioural, psychological and educa- tional problems. It is also important for general practitioners to be aware of these problems because they may be persistently overlooked when children present with relatively minor acute medical disorders such as upper respiratory tract infections.
Correspondence: Dr J. C. Vance, University Department of Child Health, Mater Children’s Hospi- tal, South Brisbane, Queensland 4101, Australia.
In 1979, the Department ofch i ld Health in the Faculty ofMedicine at the University of Queens- land changed its curriculum to include visits to schools. During these visits, medical students were active participants in the assessment of the children.
Description of the programme
The State Department of Health, Queensland, Australia, has had a School Health programme for 75 years. At the present time children in year I
(age 5-6) and year 7 (age 11-12) are routinely examined by school health nurses who visit each school in their allocated area. Children from other years are seen only on referral from parents, child or teachers. Each nurse is responsi- ble for 8000-10 ooo children in a year. This includes all children from years 1-7.
Parents are notified when the nurse is visiting the school and complete information on immu- nization, past medical and surgical history and any particular problems which the parents may wish to be evaluated. Once this information is obtained from the parents, the child in year 1 is then examined with particular emphasis on the following features: growth (height and weight as compared with standardized percentile charts [National Health and Medical Research Council 19821); vision, including strabismus; hearing; postural deformities; and development of speech, language and fine motor skills. Children in year 7 are assessed for growth, hearing, visual acuity and colour defective vision (for boys) and scoliosis (for girls).
At the University of Queensland, students
I 1
I 2 I/. O’Hara et a1
attend their course in child health in their sixth (final) year. Students could elect to do their course a t either of the major paediatric hospitals in Brisbane (Royal Children’s Hospital or Mater Children’s Hospital). The term lasts 10 weeks full time. The teaching programme at the Mater Children’s Hospital consists of a series oflectures and case presentations, attendance at ward rounds, out-patient clinics, casualty, visits to specialty hospitals (for example, for cardiac pro- blems or for children with handicapping condi- tions) and community-based government health services for children. The latter consist ofvisits to schools and child health clinics. All students would be rostcred to either of these facilities and some would attend both. Students were rostered for this community work for a maximum of 4 half-days a term.
Other community-based teaching occurred in the third year of the course, when students visited the home of a handicapped child and interviewed the parents and, if appropriate, the child. In the fifth year, students were rostered to 4 weeks of community practice.
In 1979, it became possible for students at the Mater Children’s Hospital to visit schools. This was done with the approval and cooperation of the Director of School Health (VO’H). Students were rostered twice to attend the schools in groups of four. Their visits lasted 3 hours (half a day). Parents of the children at the schools were informed that their children would be examined by medical students under the supervision of a
paediatrician from the university UCV). Stu- dents, during their first visit, saw children in year I (aged 5-6) at a school in a lower-class area close to the hospital. During their second visit, stu- dents examined children in year 7 (aged I 1-12) in a middle-class area.
Students were instructed by the school health nurse and the paediatrician how to test for vision and hearing defects, how to measure the children, test for colour defective vision and scoliosis. A developmental assessment was also made. Students checked the information sup- plied by the parents and then examined the children using standardized printed forms. Any difficulties in using the equipment o r doing the examination were resolved after discussion with the nurse or paediatrician. Students were then required to present their findings to the paediatri- cian for discussion about diagnosis and future management. Problems which were detected were referred to the parents who then attended their own doctor for follow-up. Children with related learning or behaviour problems were dis- cussed with the child’s teacher so that students could appreciate the importance of cooperation between the medical profession and educational- ists. Students saw on average two or three children in a 3-hour session.
Students detected several problems in children which had previously not been recognized by the parents or their general practitioner. For children in year I these included visual and hearing defects, speech and developmental problems and
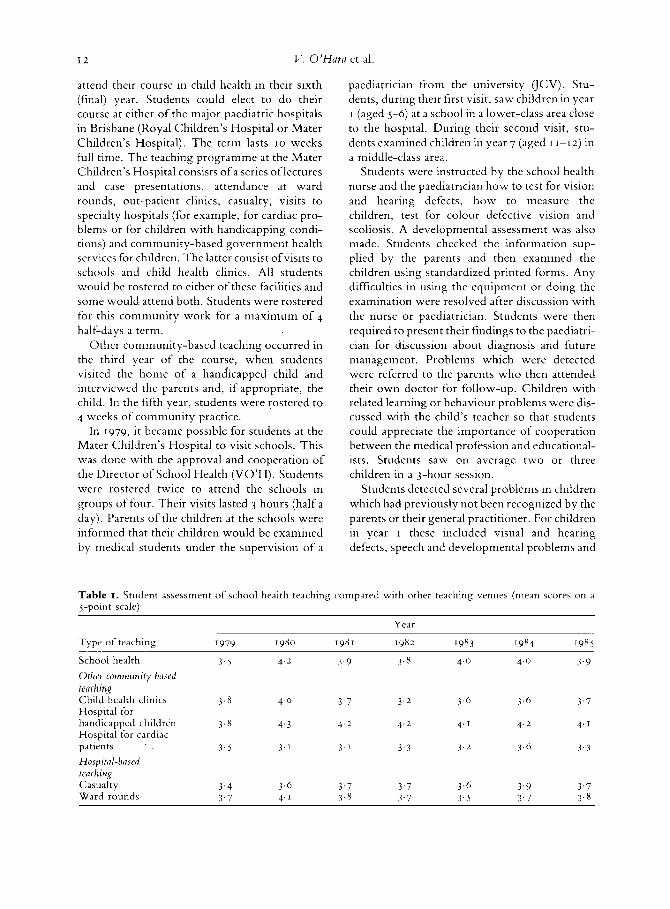
Table I . Student assessment of school health teaching compared with other teaching venues (mean scores on a 5-point scale)
Year
Type of teaching I979 1980 19x1 1982 I983 1984 1985
School health 3 . 5 4.2 3.9 3.8 4 . 0 4.0 3.9 Orher cornrnunity based fearhing Child health clinics 3.8 4- 0 3 . 7 3 .2 3 . 6 3.6 3.7 Hospital for handicapped children 3.8 4.3 4.2 4.2 4.1 4 .2 4. J
Hospital for cardiac patients 3.5 3 . ’ 3 . I 3 .3 3 .2 3.6 3 .3 Hospitul-based teathin2 Casualty 3 .4 3.6 3.7 3.7 3.6 3.9 3.7 Ward rounds 3.7 4.1 3.8 3.7 3 . 5 3.7 3 . 8

Teaching school health to undevgvaduates 13
disorders of growth. For children in year 7, scoliosis was the most common condition detected.
Over the years, students have been asked to evaluate these sessions using a 5-point scale. The points on the scale are excellent, very good, good, fair and no value, with a high score indicat- ing a better assessment by the student. Table I
shows the mean scores for the teaching in school health and compares these scores with others obtained from other small-group teaching ses- sions such as casualty and ward rounds and visits to other community facilities such as child health clinics ‘and hospitals for handicapped children and cardiac patients. The scores for school health compare favourably with the scores for these other teaching venues.
Discussion
A system of teaching medical students about school health has been described. The advantages of such a programme are many. Students are introduced to a group of apparently normal healthy children in their own environment. Most of the students’ previous contact with children is in hospital where they have an acute or chronic illness and are in a strange environment. Students are therefore more likely to experience the way children of that age normally behave in a school setting. Students are exposed to the concept of screening for paediatric diseases. They learn that children may have unsuspected health problems which could hinder the child’s medical arid educational growth. Students’ previous experi- ence ofscreening for paediatric diseases would be limited to knowledge of neonatal screening pro- cedures for phenylketonuria, hypothyroidisni and galactosaemia. The students learn and prac- tise new skills, such as vision and hearing screen- ing, and interpretation of height and weight measurements on percentile charts. They make contact with a state government health service and come to understand the referral system of children once a problem has been detected, its advantages and limitations. These are helpful in future paediatric specialization or general prac- tice. Finally, they have first-hand contact with another professional group caring for children- teachers. Students are able to discuss on the spot children with behaviour, learning or medical
problems, and, in consultation, decisions con- cerning the child’s future care can often be made.
Previous reports have described programmes in which paediatric interns, residents and fellows in ambulatory paediatrics have attended school health programmes as part of their postgraduate training. The emphasis for each programme has mainly involved the assessment of behavioural and psychological problems in children as they related to the school setting. A review of post- graduate paediatric and family medicine pro- grammes showed that there were deficiencies in what was taught to residents (Collins & Graham 1980). Very few took up electives in school health. There were variations in the emphasis of training programmes for these two departments. For example, only 86% of family medicine and 82% of paediatric programmes surveyed taught hearing and vision screening. There was no men- tion of the assessment of growth or orthopaedic problems.
Resident medical officers have been actively involved as part of the school health team in the diagnosis and management of behaviour pro- blems (Novak ef a / . 1978; Rockowitz & Hamniar 1978; Mok et al. 1983) and health education classes for students (Bass et al. 1982).
Only two reports describe visits to schools by medical students. One discussed demonstration to medical students of children who had been referred to the school health doctor (Grant 1965). Students in this report attended in pairs and were also able to attend the child’s class and talk to his teachers. Students were given hand-out material on the various aspects of school health. They usually only visited once.
The other study (Chilton 1982) also described students observing the school health nurse in the performance ofher duties. The author felt that it was important to give students exposure to the school health programme because many will not have more formal contact after graduation. Understanding the referral system and the types of problems faced is also important.
This present study goes one step further. Not only do students observe how to examine the children in their schools, but they actively par- ticipate in the assessment process by performing all components of the examination. They therefore become familiar with the techniques of examination and their pitfalls. Students therefore

I4 V . O’Hara et a1
acquire new skills as well as knowledge which is useful in their subsequent career as paediatricians or family practitioners.
Acknowledgements
We give thanks to the head teachers ofthe schools we have visited, West End, Coorparoo, Camp Hill, Grecnslopcs, White’s Hill and East Brisbane Primary Schools and the many school health nurses and children who have been involved with the programme over the last 8 years.
References
Bass J . , Mehta K., Chartor J . & Hickey J . (1982) Pediatric residents as health educators: the reactions of children. Journal of School Health 52, 422-4.
Chilton L. (1982) Are physicians educable? Teaching medical students about school health. Journal of School Health 52, 479-82.
Collins T.R. K. Graham D. (1980) School health educa-
tion in family medicine and pediatrics. Journal of Family Practice 11, 583-8.
Grant W. (1965) The school physician as an active member of the school staff. Paediatric Clinics of North America 12, 1057-70.
Haggerty R.J., Roghmann K.J. & Pless I.B. (1975) Child Health and the Community. John Wiley and Sons, New York.
Mok J. , MacLean S. & Langton M. (1983) O n e year’s experience in community child health. Health Bulletin 41, 177-80.
National Health and Medical Research Council Can- berra (1982) Growth C h a m . National Health and Medical Research Council, Australia.
Novak S.F., Rockowitz R.J. &- Zastowny T. (1978) Evaluation of training in school health for pediatri- cians. Journal of Medical Education 53. 837-40.
Rockowitz R.J. & Hammar S.L. (1978) Mini-groups for school children; preventive self-help groups that teach physicians. Journal qf School Health 48, I 19 20.
Received 3 February 1987; ediforinl comments to authors 6 March 1987; accepted for publication 14 May I987





























