Embed Size (px)
Citation preview

Malena Cohen-Cymberknoh, M.D.Pediatric Pulmonology and CF Center
Hadassah-Hebrew University Medical Center
Jerusalem, Israel
Annual CF Israeli ConferenceEin Gedi, November 11th 2016
Targeting inflammation in CF:
…is it safe?

M. Cohen-Cymberknoh et al, Thorax 2013; J.M. Courtney et al, Journal of CF 2004; Chmiel et al, Cold Spring Harb Perspect Med.
2013
• Airway disease in CF is characterized by chronic
infection and an inflammatory response dominated
by a neutrophil infiltrate
Airway inflammation in Cystic fibrosis
• Intense bronchial
neutrophilic inflammation
and release of proteases
and oxygen radicals
perpetuate the vicious
cycle and progressively
damage the airways

Triggers of inflammation in CF airway cells
Cohen-Cymberknoh M et al. Thorax 2013
Extracellular triggers
Intracellular triggers

Intracellular triggers of inflammation in
CF airway cells
Cohen-Cymberknoh M, et al. Thorax 2013
IL-10
Peroxisome proliferator-
activated receptor-gamma
(PPARgamma)
Thiazolidinediones or glitazones
High dose Ibuprofen -
IL-10
Protease/Anti-
protease balance
Alpha-1 antitrypsin
Oxidant/
Antioxidant balance Glutathione

Anti-inflammatory therapies evaluated in “preclinical” studies in CF
IL-10 and Interferon-γ
• Administration of IL-10 to infected mice showed beneficial effects on airway
inflammation. Although, till now, no trial showed any clinical relevant effect
(Chmiel et al AJRCCM 1999)
• Interferon-γ aerosolized did not improve pulmonary function, reduce
sputum bacterial density, or affect inflammatory sputum markers (Moss et al Ped Pulm 2005)
• There is a reciprocal relationship between anti-
inflammatory (IL-10) and pro-inflammatory (IL-6 and IL-8)
cytokine production by the CF epithelial cells
(Bonfield et al J Allergy Clin Immunol. 1999)

Anti-inflammatory therapies evaluated in
Clinical trials in CF
Chmiel, Konstan and Elborn, Cold Spring Harb Perspect Med. 2013
(Alpha-1 antitrypsin)

Alpha-1-antitrypsin (rAAT)
• A large multicenter trial did not shown any beneficial effects
(Bilton et al, Ped Pulm. 1999)
• Reduction in NE concentration by rAAT does not alter
bacterial loading in the sputum of CF patients
(Moore Br J Biomed Sci. 2004)
• Nebulized rAAT is safe and well-tolerated, but has a limited
effect on NE activity and other markers of inflammation
(Martin, Ped Pulm 2006)
• rAAT inhalation reduces airway inflammation in CF patients,
although, no effect on lung function was observed
(Griese M, ERJ 2007)

Systemic Corticosteroids
• Can slow lung function decline and improve weight gain, however
significant side effects were reported
• Glucose intolerance, growth impairment, and cataract formation were
shown with alternate-day oral corticosteroids treatment
• Growth deficits persisted after therapy discontinuation
• Other known toxicities- osteopenia, osteoporosis, and skeletal muscle
weakness
• For patients with CF without asthma or ABPA, the CFF recommends
against the chronic use of oral corticosteroids to improve lung function and
to reduce exacerbations
Matthews NEJM 1980; Auerbach Lancet 1985; Eigen J of Ped 1995; Lai et al 2000; Flume et al 2007; Mogayzel
AJRCCM 2013
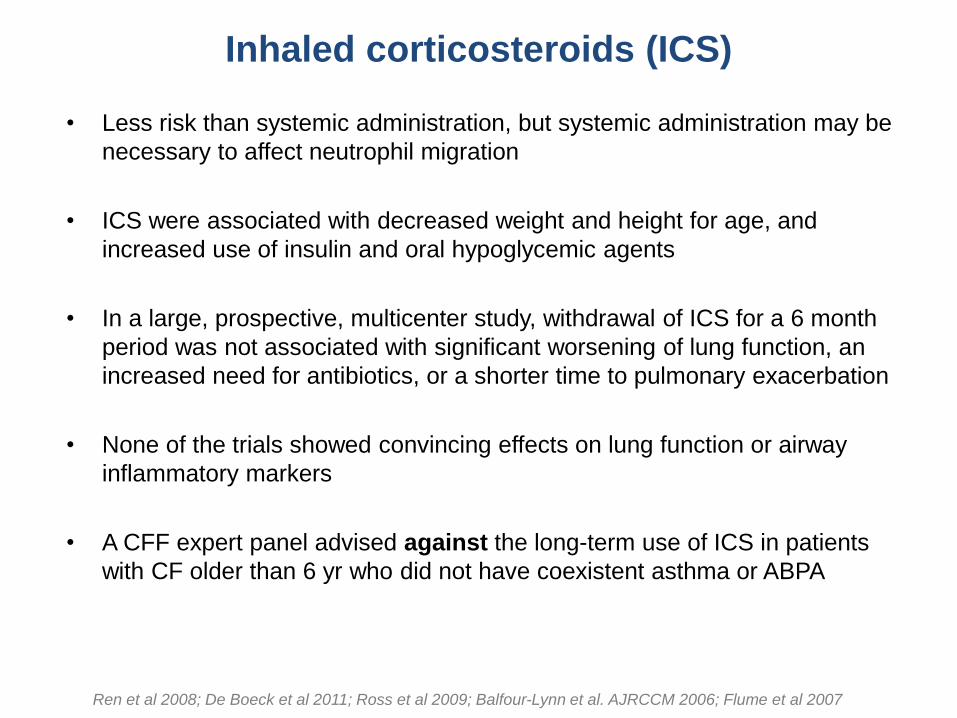
Inhaled corticosteroids (ICS)
• Less risk than systemic administration, but systemic administration may be
necessary to affect neutrophil migration
• ICS were associated with decreased weight and height for age, and
increased use of insulin and oral hypoglycemic agents
• In a large, prospective, multicenter study, withdrawal of ICS for a 6 month
period was not associated with significant worsening of lung function, an
increased need for antibiotics, or a shorter time to pulmonary exacerbation
• None of the trials showed convincing effects on lung function or airway
inflammatory markers
• A CFF expert panel advised against the long-term use of ICS in patients
with CF older than 6 yr who did not have coexistent asthma or ABPA
Ren et al 2008; De Boeck et al 2011; Ross et al 2009; Balfour-Lynn et al. AJRCCM 2006; Flume et al 2007
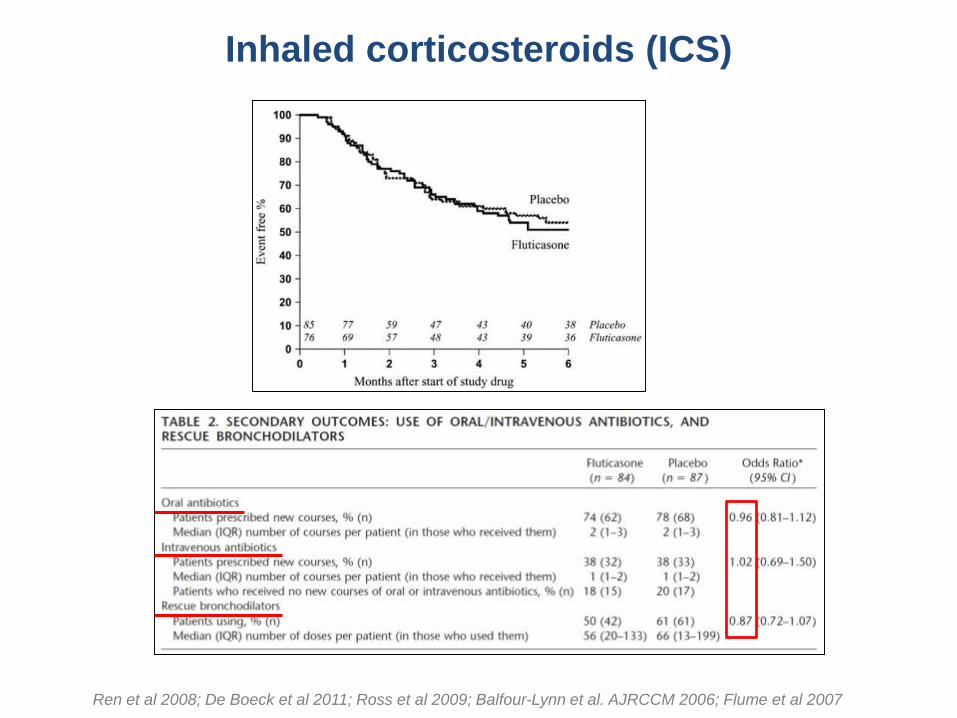
Inhaled corticosteroids (ICS)
Ren et al 2008; De Boeck et al 2011; Ross et al 2009; Balfour-Lynn et al. AJRCCM 2006; Flume et al 2007

• CXCR2 receptor antagonist can inhibit the
recruitment and activation of neutrophils
and other inflammatory cells into the CF
lung
• Blood levels of fibrinogen, CRP and
CXCL8 (IL-8) increased after treatment
• No changes in lung function or respiratory
symptoms
• Safe but not useful as an anti-
inflammatory drug in CF patients

Glutathione
• The oxidant–antioxidant imbalance may be exacerbated by
abnormalities in CFTR (Linsdell and Hanrahan 1998)
• Because decreased lung concentrations of glutathione have been
shown in CF patients (Roum J Appl Physiol 1993; Kettle et al ERJ 2014), it seems
logical to augment its concentration in the CF lung
• Treatment with aerosolized glutathione can reduced superoxide
production by inflammatory cells (Roum et al 1993)
• However, subjects treated with inhaled glutathione had no
detectable change in BAL markers of oxidative stress (Bishop et al 2005;
Hartl 2005)

Glutathione

• Randomized, double-blind, placebo-controlled trial evaluated inhaled glutathione
in subjects with CF ≥8 yrs of age
• FEV1- primary endpoint- not difference between the 2 groups
• Did not reduce number of pulmonary exacerbations, nor better scores for quality
of life
• No changes in markers of oxidation, proteolysis, or inflammation
• Inhaled glutathione did not shown clinically relevant improvements in CF patients
Griese et al, Am J Respir Crit Care Med. 2013

Griese et al, Am J Respir Crit Care Med. 2013
Placebo
GSH
• Inhaled glutathione could not affect parameters of oxidative stress such as
myeloperoxidase, ascorbic acid, uric acid and others
(Griese et al, AJRCCM 2004; Hartl Free Radic Biol Med 2005)
• No substantial effect on lung function parameters (Griese et al AJRCCM 2013)
• Since neutrophils release both oxidants and proteases causing harm to the
pulmonary tissue (Hartl, Journal of CF 2012), advanced therapeutic approaches may
consider inhibiting oxidants and proteases simultaneously
“Targeting proteases is not a real “success story” in
CF lung disease yet”
A. Hector, M. Griese, D. Hartl, ERJ 2014
Editorial

Available medications used for other inflammatory disorders
Hydroxychloroquine
o Increases intracellular pH and was evaluated in a small 28-d study in CF
o The drug was well tolerated, but there was no change in sputum inflammatory
markers (Williams et al Ped Pulm Suppl2008)
Methotrexate
o Data from studies were largely negative, intolerable adverse event profile
and increased need for IV antibiotics (Oermann, Ped Pulm Suppl 2007; Konstan, Ped Pulm Suppl 2008; Williams, Ped Pulm Suppl 2008 )
Simvastatin
o A trend toward increased eNO, but not effect on sputum inflammatory markers
(Kraynack, Ped Pulm Suppl 2008)
Pioglitazone- Inhibits NF-κB activity
o A 28-d clinical trial did not show a beneficial effect on sputum inflammatory
mediators (Konstan Ped Pulm Suppl. 2009)
These compounds are no longer being actively investigated

• Is a humanized monoclonal Fab fragment that targets a P. aeruginosa
virulence factor
• No improvement compared to placebo, in the time to need for antibiotics
2014
KB001-A
Eicosanoid modulators
• LTB4, a potent neutrophil chemoattractant, is present in high
concentrations in the CF airway (Konstan et al 1993)
• A CF trial was terminated early because of a statistically
significant increase in pulmonary-related serious adverse events
in adults receiving BIIL 284 BS (amelubant) -LTB4 receptor
antagonist (Konstan et al Ped Pulm 2005)
• Probable the inhibitory effect of BIIL 284 BS on the LTB4 pathway
is too potent, resulting in impaired antimicrobial defenses and
increasing the risk of an exacerbation
• ….Care must be taken when selecting an anti-inflammatory
agent for future clinical trials (Konstan et al Ped Pulm 2005)

“…..the outcome of this trial provides a cautionary tale for the administration
of potent anti-inflammatory compounds to individuals with chronic infections,
as the potential to significantly suppress the inflammatory response
may increase the risk of infection-related adverse events”
Konstan et al, J Cyst Fibros. 2014
After 420 patients were randomized, the trial was terminated due to
significant increase in pulmonary related serious adverse events
A substantial reduction in PMN activity at the site of infection in the lung due
to LTB4 receptor antagonism increased bacterial proliferation which
might explain why circulating counts of PMN were observed to be
significantly elevated

Azithromycin
There is a combined effect of both immunomodulatory, anti-inflammatory and anti-infective properties
Azithromycin can inhibit
neutrophil recruitment and
oxidative burst, as well as
proinflammatory
cytokine production
Verleden AJRCCM 2006; Tsai AJRCCM 2004; Culic Eur J Pharmacol 2002, Saiman JAMA 2003; Mogayzel AJRCCM 2013

Azithromycin- cont.
• The CFF recommends the chronic use of Azithromycin in patients with Pseudomonas
to improve lung function and reduce exacerbations
• In patients “without” Pseudomonas the chronic use of Azithromycin “should be
considered” to reduce exacerbations
Azithromycin use for 24 weeks may not significantly affect pulmonary function in children
without pseudomonas infection
• Remember! ….Azithromycin was associated with
Increase incidence of nausea and vomiting
Increase antibiotic resistance with chronic use (Staph, NTM)
• Azithromycin is useful but not ideal therapy as an anti-inflammatory drug
Tramper-Stranders, Pediatr Infect Dis J. 2007; Saiman L, JAMA 2010; Taylor-Cousar, Journal of Inflammation Research 2010

Pulmozyme (recombinant Dnase)
Modest reductions in sputum neutrophil elastase activity
Over a 3-year period, rhDNase prevented an increase in several markers of airway inflammation, as measured in BAL, not observed in untreated patients
Could have a positive impact on airway inflammation either by reducing levels of proinflammatory mediators in the short term or by preventing an increase in inflammation that might occur over years
Shah PL, Eur Respir J 1996; Paul K, Am J Respir Crit Care Med 2004; Ratjen Ped Pulm 2005

Pulmozyme (recombinant Dnase)

Anti-inflammatory drugs

(High dose) Ibuprofen
• The first 4-year trial showed less decline in PFT’s in patients <13 yrs. of age,
but no significant effect in adults (Konstan NEJM 1995)
• The second 2-year trial, in Canada, 6-18 y.o patients, reduction in the annual
rate of decline in FVC but not effect in FEV1 % predicted (Lands J Pediatr 2007)
• Doses: 20-30 mg/kg, a concentration of 50-100 mcg/ml is required to inhibit
neutrophil migration, >100 mcg associated to adverse effects
• Some reports about acute severe nephrotoxicity with concomitant use of IV
aminoglycosides (Lands 2007)
• Ibuprofen may be contraindicated for those who are at increased risk because
of GER, history of gastrointestinal ulcerations, or abnormal gastrointestinal
motility or anatomy (Mackey BMC Pediatr. 2004)
…..almost ALL CF patients…….

• Ibuprofen and other NSAIDs interfere with the intrarenal
production of PgE2 and prostacyclin, which cause renal
vasodilatation in the presence of reduced circulating volume
• Four children with CF had transient renal failure caused by the
IV administration of an aminoglycoside while maintenance
treatment with ibuprofen was continued
A 16-y.o girl patient- nausea and vomiting developed 6 six days after the commencement of
IV tobramycin for exacerbation. Oliguria developed the next day. The ibuprofen and
tobramycin were discontinued. The patient died 9 days later of lung disease; minimal
tubule-interstitial nephritis was seen at autopsy
A 23 mo. old baby required 9 days of peritoneal dialysis after the concomitant use of IV
gentamicin and ibuprofen
Kovesi et al, 1998

High dose Ibuprofen- recommendations
For individuals with CF, between 6-17 yrs, with FEV1 > 60% pred, the CFF recommends the chronic use of oral ibuprofen, at a peak plasma concentration of 50–100 mg/ml, to slow the loss of lung function
For individuals with CF >18 yrs. the evidence is insufficient to recommend for or against the chronic use of ibuprofen
Konstan NEJM 1995; Lands 2007; Konstant Curr Opin Pulm Med 2008; Mogayzel et al AJRCCM 2013

Ibuprofen- recommended, but,
……who uses it..?
• “…nonetheless, ibuprofen has not been widely adopted, largely
because of the logistic challenges associated with the need to
establish the dose in each patient with a 3-h pharmacokinetic test
and the concerns related to adverse effects of the drug”
(Konstan Curr Opin Pulm Med 2008)
• Based on U.S. CF Foundation Patient Registry data, ibuprofen use
is associated with gastrointestinal bleeding; the occurrence is
rare, but… (Konstan AJRCCM 2007)
• “…However, concerns about potential adverse effects have
limited the use of high-dose ibuprofen in CF patients” (Lands, Pharmaceuticals 2010)

CTX-4430 Acebilustat-
LTB4 antagonist
• A small-molecule drug that blocks the enzyme
LTA4 hydrolase, diminishing the production of LTB4,
accompanied by reductions in biomarkers inflammation
……….but………remember…….
• One trial in adults receiving a specific LTB4 receptor antagonist was
terminated early because of increase in pulmonary-related serious adverse
events (Konstan et al Ped Pulmon. 2005)
• Another study using LTB4 antagonist, after 420 patients were randomized,
the trial was terminated (phase 2) due to significant increase in pulmonary
related serious adverse events (Konstan Journal of CF 2014)
(phase 2)

Other anti-inflammatory drugs in
Phase Two and One
GS-5745 is an antibody that may reduce inflammation in the lungs, leading to
improved lung function in people with CF

Other anti-inflammatory drugs in
Phase Two and One
May increase the production of anti-
inflammatory molecules while
reducing the production of pro-
inflammatory molecules

Other anti-inflammatory drugs in
Phase Two and One
• LAU-7b, an oral compound, a form of the retinoid fenretinide
• May help reduce the inflammatory response in the CF lungs

Other anti-inflammatory drugs in
Phase Two and One
A compound designed to block the function of neutrophil elastase

Methods of assessing inflammation in the CF airways
M. Cohen-Cymberknoh et al. Thorax 2013

Methods of assessing inflammation in the CF airways
M. Cohen-Cymberknoh et al. Thorax 2013
It is crucial to standardize
measures of inflammation across
studies
We need more useful and more
dynamic biomarkers of
pulmonary function!!!

To conclude…
• No consensus as to
what the inflammation pathways are
how they may interact with the basic defect in CF
• We need more preclinical models of CF lung disease
• Recognizing that inhibiting inflammation could suppress the
inflammatory response and impair innate immunity, it is critically
important to consider the risk of infection-related adverse events (Konstan, Journal of CF 2014)
• “Targeting inflammation in CF remains an attractive therapeutic
approach, but optimizing anti-inflammatory effects while
minimizing any detrimental impact on host defense remains a
key challenge” (Sagel, Journal of CF 2014)

Thank You!