Embed Size (px)
Citation preview

500 Proceedings ofthe Royal Society ofMedicine 20
Tabk SPigmentation and prognosis
Degree of Died withpigmentation Number secondariesNone 9Slight 9 1Marked 30 6
Table 6Maignat molanomata arising in nIevi
Follow-up Died withIn years Number secondaries1 1 12 13 24 35 26 27 212
Table 7Malignant melanomata arising in novi:Treatment
Died with7Treatment Number secondariesLocal excision 6Local excision 4 1and radio-therapyEnucleation 3Exenteration 1
figures are not statistically significant. Therelationship between pigment content of thesetumours and prognosis is also not statisticallysignificant (Table 5).
Melanoma arising in a navus: Fourteen tumours inthis series were assumed to arise in a congenitalnaevus. It is usually difficult or even impossible tomake a histological diagnosis of a malignantmelanoma arising in a nevus, as in most casesthere are no remaining nests of benign nxvuscells, and in some cases a frank malignantmelanoma may be composed of cells difficult todistinguish from nivus cells. I consider, however,that the history of a pigmented lesion since birthor childhood at the site of the malignant melan-oma is good presumptive evidence of the origin ofthe malignant tumour from a navus. In thepresent series of malignant melanomata of nevusorigin there was only one death attributable to thetumour and this is contrary to Reese's opinionthat these tumours are highly malignant. Halfthese tumours ofnevus origin have been followedup five years or more (Table 6). With only onedeath in this group of malignant melanomata it isimpossible to draw conclusions about theefficacy of one form of treatment over another(Table 7).
The results of this follow-up study demonstratethat the localized malignant melanoma of thelimbus is a diagnosis useful in assessing the man-agement and prognosis of these tumours, whichbehave in a less malignant manner than similarmelanomata of the skin. These results show thatadequate local excision is the treatment of choicein the majority of cases, that enucleation of theaffected eye is seldom justified, and that orbitalexenteration need only be considered in excep-tional circumstances, when the tumour is verylarge or when there have been repeated recur-rences. I would like to stress, however, that thesestatistics indicate a trend, they do not necessarilyindicate the correct management of a particularpatient.
Acknowledgments: My thanks are due to ProfessorNorman Ashton for his continuous help andencouragement throughout this study, and tothe Medical Illustration Department of theInstitute of Ophthalmology for the preparationof the figures.REFERENCESAsh J F (1950) Amer. J. Ophthal. 33, 1203LedermanM(1962) In: System of Ophthalmology. Ed. W S Duke-Elder.London; 7, 772Lister A (1952) Trans. ophthal. Soc. U.K. 71,97ReebM J (1963) Treatment ofLid and Epibulbar Tumours.
Springfield, Ul.; p 179Reese A B (1963) Tumours ofthe Eye. 2nd ed. New York; p 330Verhoeff FH& LonngR G (1903) Arch. Ophthal., N. Y. 32,97Wybar K C (1962) Int. Ophthal. Clin. 2, 657
MrDW Hill, Dr C T Dollery,Dr J V Hodge and Dr D J Scott(Postgraduate Medical School, London)
Fluorescein Studies of the Choroidal Circulation'
The retinal circulation has been studied byphotographing circulating fluorescein injectedthrough an intravenous catheter. There is amoderate background fluorescence from theretinal capillaries, but the choroidal circulation isnot seen because of the overlying retina. Whenthe retinal pigment epithelium is disrupted bydisease choroidal fluorescence can be seen. Anumber of instances have been encountered dur-ing other studies, of which four-are presented inthis preliminary report: a patient with secondarychoroidal sclerosis, two siblings with retinitispigmentosa, and a patient with a macular scar.'This work was supported by a grant from the Medical ResearchCouncil

Section ofOphthalmology
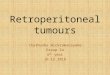
Fig 1 Fluorescein photograph of the normal fundus, inthe early venous phase of retinal circulation. The uppertemporal arteriole (right arrow) is almost empty, thevein (left arrow) full offluorescein. Many of the vesselsshow laminar flow. There is a fine mottled backgroundfluorescencefrom the retinal capillaries
Fig 2 Fluorescein photograph of the right eye ofa managed 62 with secondary choroidal sclerosis. Earlyvenous phase ofthe retinal circulation, arterioles b?com-ingpale and veins showing laminarflow. Above the opticdisc a retinal vein (arrow) crosses superficially to thetortuous choroidal vessels. Below the disc a dark area(arrow) due to masking by an island of intact retina;laterally patches ofmasking by pigment may be seen
All these patients were studied by the usualtechnique of fluorescein retinal photography(Dollery et al. 1962), serial photographs beingtaken during the passage of the dye through theeye. The appearance of the choroidal circulationdepended on the extent of disease as well as the
rig 3 riuorescein pnotograpn oj tme injerotemporatregion of the right eye of a man aged 20 with retinitispigmentosa. Arterial phase of the retinal circulation,first injection of.fluorescein. Above can be seen a retinalarteriole; below, the interlacing vertical lines (arrows)of vessels of the arterial side ofthe choroidal circulation
-ig 4 Fluorescein photograph of the right eye of a girlaged 15 with retinitis pigmentosa. Arterial phase Ofthe retinal circulation. Heavy mottled backgroundfluorescence with some vessels visible. Above the opticdisc there is an irregular dark area (arrows) whichfilled a few seconds later
timing of the photograph; the cases of retinitispigmentosa both showed a bright rrottled back-ground fluorescence (Fig 4) in contrast to thefainter evanescent fluorescence of the retinalcapillaries (Fig 1). The patient with secondarychoroidal sclerosis, a man aged 62, who had lost
21 501

502 Proceedings of/the Royal Society of Medicine 22
the vision of one eye as a result of illness fourteenyears previously, showed ophthalmoscopic evi-dence of severe choroidal damage; the back-ground fluorescence was slight but a tortuouspattern of vessels deep to the retinal vessels wasseen (Fig 2).The sequence of circulation in the choroid was
not as definite as that in the retina. An arterialphase with interlacing meridianally disposedvessels was seen in one patient (Fig 3); this wasquickly replaced by general mottled fluorescencewhich faded slowly outlasting the retinal circula-tion. Late in the sequence large empty choroidalvessels appeared as dark silhouettes against thefading choroidal fluorescence. Superimposition ofthe photographs in the sequence and the pre-liminary colour transparency by means of draw-ings, showed that the late phase silhouettescorresponded in many instances with tortuousred choroidal vessels seen ophthalmoscopically;in a few instances vessels seen in the choroidalarterial phase corresponded in position with thesilhouettes. At present these silhouetted vesselscannot be assigned to an anatomical category.A regional abnormality was demonstrated (Fig
4): an area of delayed filling was seen during theretinal arterial phase but a few seconds later, onreaching the retinal venous phase, it had dis-appeared and was indistinguishable from the restof the choroid. The patient with a fine pigmentedscar at the macula showed an exact image of it inthe fluorescein photographs, brightly fluorescentwith the pigment casting a dark shadow.
In the case of secondary choroidal sclerosis(Fig 2) the depth of the vessels and their appear-ance confirm the impression that they arechoroidal. The two patients with retinitis pig-mentosa (Figs 3 & 4) are less obvious cases ofchoroidal fluorescence, but the masking effect ofintact retina at the macula, the prolonged dura-tion of fluorescence, and the late appearance ofidentifiable choroidal vessels in silhouette leavelittle doubt. Atrophy, migration and proliferationof the retinal pigment epithelium are acceptedfeatures of retinitis pigmentosa and choroidalsclerosis (Duke-Elder 1940). Aggregrations ofpigment mask the fluorescence, but between theclumps it is brighter, suggesting that the pigmentepithelium is the most important factor in themasking of choroidal fluorescence by normalretina.
These cases demonstrate the pattern ofchoroidal fluorescence in generalized and localchoroidoretinal disease, they indicate that circu-lation is more prolonged in the choroid than theretina, and show that regional delay in filling mayoccur. The choroid in all these cases is diseased sothat the behaviour of normal choroid cannot beinferred; however, the results are sufficientlyinteresting to encourage further studies.
Acknowledgment: We are most grateful to Mrs MEngel for the care with which she has processedthe films and prepared the illustrations.REFERENCESDoliery C T, Hodge J V & Engel M(1962) Brit. med. J. ii, 1210Duke-Elder W S(1940) Textbook ofOphthalmology. London; 3, 2409, 2776
Dr W Campbell (Queen Victoria Hospital, EastGrinstead) read a paper entitled Macro-dacryo-cystography (see Campbell W, 1964, Brit. J.Radiol. 37, 1).
Mr A I Friedmann (Royal Eye Medical Ophthal-mology Unit, Lambeth Hospital, London) demon-strated a New Perimeter(see Friedmann A I, 1962,Trans. ophthal. Soc. U.K., 82, 381).
Meeting December 121963
In a discussion on Social Aspects of Ocular Dis-ability the following papers were read:
The Assessment and Placing of theVisually HandicappedMiss I D R Gregory
The Placing of the Partially-sightedSchool LeaverMrsM C Clark
Temporary Ocular DisabilityMrM J Roper-Hall
The Role of the AlmonerMissD Collis