Embed Size (px)
Citation preview

ava i l ab l e a t www.sc i enced i r ec t . com
C l i n i ca l Immuno logy
www.e l sev i e r . com/ loca te /yc l im
Clinical Immunology (2010) 135, 99–107
T and B cells target identical regions of thenon-collagenous domain 1 of type VII collagenin epidermolysis bullosa acquisitaRalf Müller a,⁎, Christiane Dahler a, Christian Möbs a, Elke Wenzel a,Rüdiger Eming a, Gerald Messer b, Andrea Niedermeier a,b, Michael Hertl a,⁎
a Department of Dermatology and Allergology, Philipps University Deutschhausstrasse 9, D-35033 Marburg, Germanyb Department of Dermatology and Allergology, Ludwig-Maximilians University Munich, Germany
Received 6 August 2009; accepted with revision 23 December 2009Available online 25 January 2010
Abbreviations: Auto-ab, autoantiblous skin disorder intensity score; BMZBP, bullous pemphigoid; Col VII, typelinked immunosorbent assay; ELISPOTassay; IA, immunoadsorption; IIF, inPBS, phosphate-buffered saline; Rtx,dodecyl sulfate-polyacrylamide gel elskin.⁎ Corresponding authors. M. Hertl is
6421 58 65729. R. Müller, Departmentand Venerology University of Lübeck,10), D-23538 Lübeck, Germany. Fax: +
E-mail addresses: Ralf.Mueller@[email protected] (M. Hertl).
1521-6616/$ – see front matter © 200doi:10.1016/j.clim.2009.12.010
KEYWORDSEpidermolysis bullosa;Collagen VII;Autoantibody;T cell;Epitope;Immunoadsorption;Rituximab;ELISA;ELISPOT;Immunoblot
Abstract Epidermolysis bullosa acquisita (EBA) is a severe immunobullous disease and is causedby IgG against type VII collagen (Col VII) of anchoring fibrils. In this study, utilizing ELISA andimmunoblot, 13/15 EBA sera but 0/20 bullous pemphigoid sera and 0/30 healthy control serashowed IgG reactivity with distinct recombinant subregions of the non-collagenous domain 1(NC1) of Col VII. In two EBA patients, IgG titers against Col VII-NC1 were grossly correlated toclinical disease activity. Moreover, Col VII-reactive T cells were identified in a representativeEBA patient which recognized identical subdomains of Col VII-NC1. These findings stronglysuggest that (1) the Col VII-NC1 ELISA is a powerful tool for making the diagnosis of EBA, (2) ColVII-specific IgG grossly relates to disease activity and (3) IgG reactivity is associated with T cellrecognition of identical subdomains of Col VII-NC1.© 2009 Elsevier Inc. All rights reserved.
ody; ABSIS, autoimmune bul-, basement membrane zone;VII collagen; ELISA, enzyme-, enzyme-linked immunospotdirect immunofluorescence;rituximab; SDS-PAGE, sodiumectrophoresis; SSS, salt split
to be contacted at fax: +49of Dermatology, AllergologyRatzeburger Allee 160 (Haus49 451 500 5162.sh.de (R. Müller),
9 Elsevier Inc. All rights reserv
edIntroduction
Epidermolysis bullosa acquisita (EBA) is a rare chronicsubepidermal bullous disease of the skin and mucousmembranes with an incidence of 0.17–0.26 per millionpeople in Western Europe [1,2,3]. It is characterized by IgGautoantibodies (auto-ab) against the 290 KDa type VIIcollagen (Col VII), a major component of anchoring fibrilsin the lamina densa of the dermo-epidermal basementmembrane zone (BMZ) [4,5]. Epitopes recognized by themajority of EBA sera have been mapped to the non-collagenous (NC) 1 domain of Col VII [5,6,7]. The Col VII-NC1 region has been shown to directly interact with the β3-chain of laminin 332 (formerly laminin 5) which provides a
.

100 R. Müller et al.
direct linkage between the anchoring fibrils of the dermisand components of the BMZ [8]).
The pathogenic relevance of IgG against Col VII is supportedby compelling evidence. IgG auto-ab from EBA patients wereshown to recruit and activate leukocytes in vitro, resulting indermal-epidermal separation of cryosections of human skin[9,10]. Many of the key features of EBA have been successfullyreproduced indistinct animalmodels [11]. Thepassive transferof Col VII-reactive IgG from EBA sera into neonatal micereproduces the pathologywith a subepidermal loss of adhesionand the appearance of tense blisters [12–14]. Moreover, activeimmunization of SJL mice with murine Col VII-NC1 leads to theinduction of pathogenic auto-ab resulting in a severe blisteringphenotype reminiscent of EBA [15].
The aim of the present study was to screen the sera of acohort of EBA patients for IgG reactivity with distinctsubdomains of the immunodominant Col VII-NC1 regionutilizing a recently developed highly sensitive and specificELISA and immunoblot analysis with the identical humanCol VIIrecombinants. Additionally, we used ELISPOT technology tomonitor autoreactive T cell responses against the Col VII-NC1domain in a well-characterized EBA patient. Our findingsdemonstrate that the majority of EBA sera show IgG reactivitywith Col VII-NC1 and that the titers of Col VII-specific IgG auto-ab seem to relate to the clinical activity of EBA. Moreover,autoreactive T cells from a selected EBA patient recognizedepitopes within the same regions of the Col VII-NC1 domainwhich were targeted by IgG auto-ab. These observationssupport the concept that the NC1 domain of Col VII harboursmajor epitopes for autoreactive T and B cells in EBA.
Materials and methods
Characterization of the patients' sera
Sera from a total of 15 patients with EBA were analyzed forIgG reactivity against Col VII. The clinical suspicion of EBAwith a variable phenotype ranging from tense blisters of theoral mucosa and additional mucosal surfaces to tense blisters
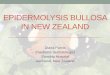
Figure 1 Baculovirus-derived non-collagenous domain 1 (NC1) ofthe two NC1 and NC2 subregions that are interrupted by a triple heliVII and is larger than the COOH-terminal Col VII-NC2 domain (A). The6×His tag at the NH2 terminus followed by the antigenic epitopes atof the NC1 domain (aa17-610), Col VII-NC1(2) the mid portion of the Nthe NC1 domain (aa611-1253) (B). The purified Col VII-NC1 recombreacted with a monoclonal anti-E tag antibody: lane 1, Col VII-NC1(1)is the molecular weight marker.
with atrophy and milia cyst formation or a more bullouspemphigoid (BP)-like inflammatory phenotype was con-firmed by (1) histopathology (subepidermal blister withscarring), (2) direct immunofluorescence (DIF) with lineardeposits of IgG and complement factor 3 (C3) along thedermal-epidermal BMZ, and (3) circulating IgG auto-abreactive with the dermal side of saline-split human skin(SSS) as previously described [16]. Among the 15 studiedpatients, 3 (patients 7–9) showed the inflammatory, BP-likeEBA phenotype while the majority of the patients showed themechano-bullous EBA phenotype. The control group con-sisted of a total of 30 age-matched individuals who did notexhibit a specific bullous skin disorder. Patients and controlsgave written consent to participate in this study which wasadherent to the Declaration of Helsinki Guidelines and whichwas approved by the local Ethics Committee.
The extent of cutaneous and mucosal involvement of theEBA and BP patients during the observation periodwas assessedby a recently established scoring system, the autoimmunebullous skin disorder intensity score (ABSIS), which waspreviously introduced by our group and applied for the clinicalfollow-up of patients with EBA [17,18]. Oral mucosal involve-ment was included in a modified form of the mucosal ABSISranging from 0 (no lesions) to 11 (maximum extent) [18].
Cloning of recombinant Col VII proteins
The sequences of human Col VII-NC1(1) (aa17–610), Col VII-NC1(2) (aa273–857) and Col VII-NC1(3) (aa611–1253) (Fig. 1A)were amplified using the following primers: for Col VII-NC1 (1)(aa17–610), forward 5′-T CCCGGGTACCTTCTAGAAGAGGCGCCC CGA GTG-3′; reverse 5′-CAG GAA AGG ATC AGA TCT ATCTGA CAC CAC AAC CCG-3′; for Col VII NC1 (2) (aa273–857),forward 5′-T CCC GGG TAC CTT CTA GAA GAG CGG CAG GAGGTG AAC-3′; reverse 5′-CAG GAA AGG ATC AGA TCT CGG CGTAGTGACAACAAT-3′; for Col VII NC1 (3) (aa611–1253), forward5′-T CCC GGG TAC CTT CTA GAA GCA ACG CGA GTG AGG GTG-3′; reverse 5′-CAG GAA AGG ATC AGA TCT CTT TGG ACA ATACAC TGG-3′.
type VII collagen (Col VII) recombinant proteins. Col VII containscal region; the NC1 domain is located at the NH2-terminus of ColCol VII-NC1 recombinants of this study are composed of an E tag/the COOH end. Col VII-NC1(1) contains the NH2-terminal portionC1 domain (aa273-857) and Col VII-NC1(3) the COOH-terminus ofinants were transferred to nitrocellulose membranes and were; lane 2, Col VII-NC1(2); lane 3, Col VII-NC1(3). Shown on the left

101Type VII collagen and epidermolysis bullosa acquisita
Full-length cDNA of Col VII-NC1 (HNC1-pcDNA3; kind giftfrom G. Meneguzzi, Nice) was used as a template andamplification was performed with Triple Master PolymeraseMix (Eppendorf, Hamburg, Germany). The amplified cDNAswere digested with restriction enzymes XbaI and BglII andligated in the modified transfer vector pAcGP67EHN using T4-Ligase (Promega,Mannheim,Germany), as described [19]. Theligated vector was transfected inE. coli XL10 gold (Stratagene,Amsterdam, the Netherlands), cloned and amplified. Theisolated plasmids were checked for inserts of the correct sizeby sequencing (Sequiserve, Vaterstetten, Germany).
Expression and purification of Col VII-NC1recombinant proteins
The baculovirus transfer vectors pAcGP67EHN, containing thesequences of defined non-collagenous regions of Col VII, wereco-transfected with linearized baculo gold bright virus DNA (BDBiosciences, Heidelberg, Germany) in SF21 insect cells usingbaculo gold transfection buffer A and B set (BD Biosciences,Heidelberg, Germany). For high baculovirus titers, the recom-binant baculoviruseswere amplified in SF21 insect cells. For theproduction of recombinant CollVII-NC1 proteins, High-Fiveinsect cells were inoculated with recombinant baculovirus asdescribed [19]. Recombinant proteins were purified fromculture supernatants by affinity chromatography and graduallydialyzed against PBS [19]. Protein concentrations weredetermined by a commercial kit (DC Protein Assay, Bio-Rad,Munich, Germany) according to a modified protocol by Lowry.
ELISA utilizing Col VII-NC1 fragments
ELISA experiments were performed with the affinity-purified recombinant proteins according to a recently
Table 1 Detection of IgG autoantibodies against the Col VII-NC1 dELISA and immunoblot analysis.
EBA–patient ELISA
IIF Col VII–NC1(1) Col VII–NC1(2) Col VII–
aa17–610 aa273–857 aa611–
1 + + + +2 + + + −3 + − − +4 + − + +5 + + + +6 + + − −7 + − − +8 + − − +9 − − − +10 + − − −11 + − − −12 + − − −13 + − − −14 + − − +15 + − − −
EBA patients, except for patients 7–9 with the inflammatory type of EBindirect immunofluorescence microscopy (IgG reactivity with theimmunosorbent assay ColVII-NC1, non-collagenous domain 1 of human
described protocol [19]. Each well of the 96-well polysty-rene plates was coated with 2 pmol of the recombinantproteins Col VII-NC1(1), Col VII-NC1(2), and Col VII-NC1(3),respectively. Sera of 15 EBA patients, 20 BP patients and 30healthy controls (diluted at 1:50) were reacted withimmobilized recombinant proteins. IgG binding was visual-ized by a horseradish peroxidase (HRP)-labeled goat anti-human IgG (1:5000, Dako, Hamburg, Germany) (1 h at roomtemperature) and ABTS (Calbiochem, Schwalbach, Ger-many) reactivity (30 min at room temperature) wasmeasured at an optical density (OD) of 405 nm. Sampleswere run at least in duplicate and the results wereexpressed as median values.
Immunoblot analysis
Equal amounts of recombinant Col VII-NC1 proteins wereseparated by 10% SDS-PAGE and visualized by Coomassiestaining or were electrophoretically transferred to nitrocel-lulose and blocked with milk powder in PBST as previouslydescribed [19]. We used the primary monoclonal mouse anti-E-Tag ab (1:2000) (GE-Healthcare, Freiburg, Germany) andthe secondary HRP-labeled monoclonal anti mouse ab(1:2000) (Dako, Hamburg, Germany), to verify molecularweight and immunoreactivity. Specific bands of human ColVII-NC1(1) (aa17–610), Col VII-NC1(2) (aa273–857) and ColVII-NC1(3) (aa611–1253) were detected at ca. 69, 67 and 74kDa, respectively (Fig. 1B). Thus, affinity purification led tosubstantial amounts of intact and fully immunoreactive ColVII-NC1 components. To detect the IgG reactivity of patientssera, the sera were diluted 1:200, incubated overnight at8°C and IgG binding was visualized by a HRP-labeled goatanti-human IgG (Dako, Hamburg, Germany), followingenhanced chemoluminescence (Millipore, Germany).
omain in patients with epidermolysis bullosa acquisita (EBA) by
Western blot
NC1(3) Col VII–NC1(1) Col VII–NC1(2) Col VII–NC1(3)
1253 aa17–610 aa273–857 aa611–1253
+ + ++ + +− − +− − ++ + ++ − −− − −− − +− − −+ − −− − ++ − −− − −− − +− − −
A, all the other patients had the mechano-bullous type of EBA IIIF,dermal side of saline-split human skin) ELISA, enzyme linkedtype VII collagen.

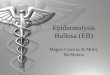
Figure 2 IgG reactivity of epidermolysis bullosa acquisita (EBA) serawith thenon-collagenous domain1 of typeVII collagen (Col VII-NC1) byenzyme-linked immunosorbent assay (ELISA) and immunoblot analysis. IgG reactivity of the sera from patients with EBA, bullous pemphigoid(BP) and healthy control individuals with the Col VII-NC1 recombinants was analysed by ELISA and immunoblot analysis. By ELISA, 10/15 EBAsera showed IgG reactivity against at least one of the Col VII-NC1 recombinants, i.e., Col VII-NC1(1) (aa17–610), Col VII-NC1(2) (aa273–857),or Col VII-NC1(3) (aa611–1253) (A). In contrast, none of the BP or control sera showed IgG reactivitywith the Col VII-NC1 recombinants (B–C).The interrupted lines indicate the cut-off value of the ELISA which was set at 0.376 (OD at 405 nm) as evaluated by maximization of Youdenindex. By immunoblot analysis, 11/15 of the EBA sera were IgG reactive with at least one of the Col VII–NC1 recombinants (D).
102 R. Müller et al.
Enzyme-linked immunosorbent spot assay (ELISPOT)
Frozen peripheral blood mononuclear cells (PBMC) werethawed and cultured in 24-well-plates (Nunc, Langenselbold,Germany) at a concentration of 1×106/ml in mediumconsisting of RPMI-1640 (Lonza, Basel, Switzerland) and10% pooled human serum, 100 U/ml penicillin, 100 μg/ml
Figure 3 Relationship of IgG reactivity against the non-collagenouin two patients with epidermolysis bullosa acquisita (EBA). Two patiewith regard to clinical activity determined by the autoimmune bulloCol VII-NC1 which was measured by ELISA. Patient 1 initially receivestarting at 0 month (A) which did not lead to a marked improvemobservation period (A). Accordingly, IgG against the Col VII-NC1 recoagain thereafter, so did the IgG autoantibody titers by indirect immtreatment with IA followed by Rtx and showed a clinical improvementmonth observation period (B). IgG against the Col VII-NC1 recombinastayed below the initial serum concentrations during the entire obs
streptomycin and 2 mM L-glutamine (all PAA Laboratories,Pasching, Austria). PBMC were stimulated with 10 μg/ml ofthe respective Col VII-NC1 protein or left unstimulated. Onday 3, IL-2 (10 U/ml; Roche, Mannheim, Germany) and IL-7(10 ng/ml; Miltenyi Biotech, Bergisch-Gladbach, Germany)was added for in vitro expansion of Col VII-NC1-specific Tcells. After 7 days, PBMCs were restimulated with the
s domain 1 of type VII collagen (Col VII-NC1) with disease activitynts with severe EBA were monitored over a period of 9–16 monthsus skin disorder intensity score (ABSIS) and IgG reactivity againstd immunoadsorption (IA) treatment followed by rituximab (Rtx)ent of EBA (as visualized by the ABSIS score) over the entirembinants NC1(1), NC1(2) and NC1(3) decreased initially and roseunofluoresence microscopy (IIF). Patient 2 also received initialwhich was apparent by a decrease of the ABSIS over the entire 9-nts was reduced initially and showed a distinct increment whichervation period (B).

103Type VII collagen and epidermolysis bullosa acquisita

104 R. Müller et al.
appropriate Col VII-NC1 construct (10 μg/ml). After platecoating with anti-human IFNγ, anti-IL-5 or anti-IL-10 mAbs,respectively, overnight at 4°C, 2×105 PBMC/well were addedand incubated for 20 h at 37°C in a humidified atmospherecontaining 5% CO2. ELISPOT analysis was performed accord-ing to the manufacturer's protocol (BD Biosciences, Heidel-berg, Germany). Cytokine-producing spots were countedautomatically using an ELISPOT plate reader (A.EL.VIS,Hannover, Germany) and the median number of spots wasdetermined in triplicate after subtracting the spots of theunstimulated wells from the Ag-stimulated wells.
Results
Baculovirus-derived Col VII-NC1 recombinant proteins
Recombinant overlapping proteins that represented distinctregions of the NC1 domain of Col VII, i.e., NC1(1) (aa17–610),NC1(2) (aa273–857) and (NC1(3) (aa611–1253) were pro-duced in a baculovirus expression system and were affinity-purified over Nickel agarose (Fig. 1A). Confirmation of therecombinant proteins was performed by immunoblot analysiswith a monoclonal ab against the E-tag (Fig. 1B) and byimmunoreactivity with EBA sera (not shown).
Detection of Col VII-NC1-specific IgG in EBA sera byELISA and immunoblot
Among the 15 EBA sera studied, fourteen sera showed dermalIgG reactivity on SSS while one serum showed a combinedepidermal/dermal reactivity pattern (Table 1). In contrast, allof 20 investigated BP sera showed IgG reactivity with theepidermal side of SSS and IgG against type XVII collagen/BPantigen 2 (BP180) and/or BPantigen 1 (BP230) by ELISA. Sera ofhealthy controls (n=30) did not show IgG reactivity by IIF and/or ELISA. IgG reactivity against the Col VII-NC1 recombinants ofsera from patients with EBA, BP and the healthy individualswas analyzed by ELISA (Figs. 2A–C) as previously described[20,21]. A total of 10/15 EBA sera showed IgG reactivitywith atleast one of the Col VII-NC1 recombinants (Fig. 2A) while 0/20BP sera showed IgG reactivity (Fig. 2B). Moreover, none of the30 healthy control sera showed IgG reactivity to Col VIII-NC1(Fig. 2C). The observed IgG response was specific since none ofthe Col VII-reactive EBA sera showed IgG reactivity againstbaculovirus-derived desmoglein 3, an unrelated desmosomalprotein which was expressed and purified in an identicalmanner (not shown).
Of the 10 reactive EBA sera, two showed reactivity with allthe three Col VII-NC1 recombinant constructs (Pat 1 and Pat 5),one EBA serum reacted with Col VII-NC1(1) and Col VII-NC1(2)(Pat 2) while another EBA serum showed IgG reactivity againstCol VII-NC1(2) and Col VII-NC1(3) (Pat 4). Moreover, 6 EBA serawere only reactive with a single Col VII recombinant, i.e. oneserum with Col VII-NC1(1) only (Pat 6), and five sera with ColVII-NC1(3), respectively (Fig. 2A and Table 1).
Immunoblot analysis of the EBA sera with the identical ColVII-NC1 recombinants led to similar findings. A total of 11/15(73%) EBA sera showed IgG reactivity by immunoblot analysiswith at least one of the three Col VII-NC1 fragments (Fig. 2D).Three EBA sera (Pat 1, Pat 2, Pat 5) were IgG reactive with allthree Col VII-NC1 proteins, while eight EBA sera were only
reactive with a single Col VII protein (NC1(1): Pat 6, Pat 10,Pat 12; NC1(3): Pat 3, Pat 4, Pat 8, Pat 11, Pat 14)) (Fig. 2Dand Table 1). Based on the findings with Col VII-ELISA andimmunoblot analysis, the majority of the EBA sera (i.e., 13/15, 87%) showed IgG reactivity with an epitope within theCOOH-terminal stretch/part (aa611–1253) of the Col VII-NC1domain.
Col VII-NC1-specific IgG reactivity and correlationwith the clinical severity of EBA
Among the patients studied, two EBA patients presentedwith extensive skin lesions and received treatment withimmunoadsorption (IA) and rituximab (Rtx),as recentlydescribed [17]. In these patients, serum samples werecollected over a period of 120 weeks and were analyzed forIgG reactivity against the Col VII-NC1 recombinants by ELISA.As shown in Figs. 3A–B, Col VII-NC1-specific IgG titers werehighest at month 0 prior to treatment with IA and Rtx whichreflects the highest disease activity expressed by the ABSIS.Patient 1 did not show a pronounced clinical improvementupon treatment with IA followed by Rtx as shown by apersisting ABSIS and a gradual increase of Col VII-NC1-specific IgG and IIF reactivity (Fig. 3A). In contrast, EBApatient 2 showed a good clinical response to IA/Rtx which isvisible by the gradual decline of the ABSIS and IgG reactivityagainst Col VII-NC1 (as well as IIF reactivity) which remainedbelow the initial concentration at month 0 (Fig. 3B).
Ex vivo detection of Col VII-NC1-specific T helper cells
ELISPOT analysis revealed cytokine-producing spots upon exvivo stimulation of PBMC of an EBA patient with Col VII-NC1.In vitro stimulation of PBMC from an EBA patient showed IL-5-secreting T cells (as a typical T helper 2-associated cytokine)reactive with the Col VII-NC1(1) and-NC1(2) recombinantsand to a minor extent to Col VII-NC1(3) (Fig. 4A). Moreover,IFN-γ-secreting T cells (with IFN-γ considered as a cytokinesecreted by Th1 cells) were similarly detected against all theCol VII-NC1 recombinants (Fig. 4A). Finally, IL-10-secreting Tcells reactive with the Col VII-NC1 recombinants weredetected at lower frequencies. Thus, T cell reactivity againstCol VII was directed against several regions throughout theNC1 domain (Fig. 4A).
Subsets of Col VII-NC1-reactive Th cells of a patient withmechano-bullous EBA were monitored longitudinally(Fig. 4B). The patient was initially (at month 0) treatedwith four cycles of IA followed by Rtx which was given fourtimes over a month i.v. at 375 mg/m2 and the patient wasfollowed up thereafter over a period of 25 months. Inaddition, the patient also received mycophenolate 2 g/dayfor at least 6 months. Immediately after treatment with IA/Rtx, there was a marked decrease of all the T cell subsetswhich was accompanied by strongly reduced Col VII-specificIgG auto-ab and a clinical response which is reflected by adecrease of the ABSIS (Fig. 4C). When the patient experi-enced a clinical relapse at month 15 (which was associatedwith an elevated ABSIS), the frequencies of Col VII-specificTh cells were also increased. Upon re-treatment with Rtx,ABSIS and auto-ab concentrations showed a decline as did thefrequencies of Col VII-specific T cells. In this patient, the

Figure 4 Detection of type VII collagen (Col VII)-NC1-specific T helper (Th) cell responses in a patient with epidermolysis bullosaacquisita (EBA) by enzyme-linked immunospot (ELISPOT) assay. By ELISPOT analysis, IL-5-secreting Th2 cells and IFN-γ-secreting Th1cells were detected upon ex vivo stimulation of peripheral blood mononuclear cells from an EBA patient with recombinant proteinsrepresenting distinct portions of the Col VII-NC1 domain, i.e., Col VII-NC1(1),-NC1(2), and-NC1(3) (Methods section). An IL-10-secreting T cell subset responsive to Col VII-NC1 was also identified. Expressed is the number of cytokine-producing cells per 200,000peripheral blood mononuclear cells (A). A patient with EBA received initial treatment with immunoadsorption (IA) followed byrituximab (Rtx) and was monitored over a period of 25 months with regard to T cell reactivity, Col VII-Nc1-specific IgG and clinicalactivity expressed by the autoimmune bullous skin disorder intensity score (ABSIS) (B–C). Frequencies of Th1, Th2 and IL-10+T cellsresponsive to Col VII-NC1 were expressed as numbers of cytokine-producing spots (per 200,000 PBMC). Frequencies of Th1, Th2 and IL-10+T cells responsive to Col VII-NC1 dropped significantly upon treatment with IA/Rtx over the entire observation period (pb 0.05) (B).In addition, IgG autoantibodies against Col VII-NC1 were initially decreased and remained at an intermediate level below the initialserum concentration (C). Moreover, clinical activity which was visualized by ABSIS showed an excellent response to IA/Rtx and, after arelapse at month 20, to a second cycle of Rtx (C). Thus, T cell reactivity against Col VII-NC1 was closely related to the clinical activityfollowed by a delayed response of Col VII-specific IgG.
105Type VII collagen and epidermolysis bullosa acquisita

106 R. Müller et al.
extent of the IgG auto-ab response to Col VII did not strictlyfollow the observed clinical improvement.
Discussion
The present study shows for the first time that both,autoreactive T and B cells from patients with EBA, a severeautoimmune bullous skin disorder, target identical regionswithin the NC1 domain of Col VII, the autoantigen of EBA.Utilizing a recently developed ELISA with baculovirus-derived Col VII-NC1 recombinants, we were able to demon-strate that the majority (87%) of the studied EBA sera showedIgG reactivity with distinct subdomains of the immunodomi-nant Col VII-NC1 region. Specifically, the majority of the EBAsera showed IgG reactivity against the COOH-terminus of ColVII-NC1 which encompasses aa611–1253. This IgG auto-abprofile of the EBA sera was also verified in independentstudies utilizing Western blot analysis with defined Col VII-NC1 recombinants. Moreover, peripheral blood T cells froman EBA patient recognized identical regions within the entireCol VII-NC1 domain. The Col VII-specific autoreactive T cellssecreted Th1-and Th2-like cytokines upon ex vivo stimulationwith recombinant human Col VII while a minority of the Tcells also secreted the immunosuppressive cytokine, IL-10.These observations are in line with previous studies whichdemonstrated that patients with unrelated autoimmunebullous disorders, such as pemphigus vulgaris, BP, pemphi-goid gestationis and linear IgA bullous dermatosis, show Tand B cell reactivity against similar or identical epitopes ofthe major autoantigens, desmoglein 3 or BP180/BP230,respectively [22–27]. By ELISPOT assay, a previous studydetected mixed autoreactive Th1 and Th2 responses inpatients with pemphigus vulgaris and BP [28].
These findings extend previous observations that the NC1domain is the immunodominant region of Col VII and stronglysuggest that autoreactive T cells provide help to Col VII-specific B cells for the production of pathogenic IgG auto-abin EBA as shown in pemphigus and BP [29].
Specifically, the ELISA assay established here proved to behighly sensitive and specific in identifying IgG auto-ab in thestudied EBA sera. The detection of Col VII NC1-specific IgGwas specific since sera from patients with unrelated skinconditions, such as BP or from healthy donors did not showIgG reactivity. The remaining EBA sera (3/15, i.e., 20%) thatdid not show IgG reactivity against Col VII-NC1 may targetepitopes of Col VII other than the NC1 domain. Moreover, thetiters of anti-Col VII-NC1 IgG were found to grossly reflectdisease severity in individual EBA patients. Immunoblotanalysis utilizing the identical Col VII-NC1 recombinantsseemed to be less sensitive than the ELISA but showed thesame pattern of Col VII-NC1-specific auto-ab profiles whichsupports the specificity of the Col VII ELISA.
Our findings extend previous studies by Chen et al. whodeveloped an ELISA with human Col VII-NC1 recombinantprotein derived from an eukaryotic expression system [30].In their study, all of 24 EBA sera showed specific IgGreactivity with the Col VII-NC1 domain by ELISA while neitherhealthy donors nor patients with unrelated disorders such asBP or pemphigus showed specific IgG reactivity. In contrastto the previous study with full-length Col VII-NC1 recombi-nant protein, we were able to identify the COOH-terminal
portion of Col VII-NC1 (aa611–1253) as the major target ofIgG auto-ab even though the NH2-terminal subdomains werealso recognized by several EBA sera. A prospective study witha larger cohort of EBA patients may help to clarify whetherIgG reactivity against distinct subdomains of Col VII-NC1 is amore specific and sensitive marker of disease activity thanIgG reactivity against Col VII.
Therapeutic interventions are at times most unsatisfactorydue to the clinical heterogeneity of EBA. Specifically, the“classical” presentation, i.e., the mechano-bullous variantwhich is characterized by skin fragility of the acral surfaces andoral mucosa is extremely hard to treat [31]. While the mildmanifestation of mechano-bullous EBA mimicks porphyriacutanea tarda, the severe form carries features of dystrophicEB, a hereditary disorder associated with scarring, cicatrizingalopecia,milia formation and nail dystrophy. By ELISAwith ColVII-NC1, we were able to establish the diagnosis of EBA in sucha patient as shown in Fig. 3A. Despite treatment with IAfollowed by the B cell depleting ab, Rtx, the patient did notimprove significantlywhich is also reflected by the persistenceof Col VI-specific IgG auto-ab (Fig. 3A). A second patient with aclinical variant of EBA which is reminiscent of BP showed amuchmore favorable clinical outcome to IA and Rtx treatmentwhich was associated with a decrease of Col VII-NC1-specificIgG auto-ab (Fig. 3B). Monitoring T cell reactivity against ColVII-NC1may be of help as a sensitivemarker of disease activityin EBA as shown in Fig. 4C.
A patient with EBA showed an excellent clinical responseto treatment with IA followed by Rtx which was reflected bya decrease of the ABSIS, a clinical parameter which wasrecently introduced in EBA [17]. The frequencies of Col VII-specific Th2 and Th1 cells were directly correlated with theABSIS (Fig. 4B), while the titers of Col VII-specific IgG showeda more delayed course (Fig. 4C).
Thus, the present ELISA with Col VII-NC1 is sensitive andspecific in detecting Col VII NC1-reactive IgG in EBA.Moreover, the successful detection and quantification ofautoreactive T cells by ELISPOT assay in a single patient withEBA may be helpful in identifying more refined diseaseactivity markers in EBA once these findings are substantiatedin greater patient cohorts. Thus, EBA adds up to the list ofwell-characterized autoimmune bullous skin disorders, suchas pemphigus and BP whose auto-ab-mediated immunepathogenesis is presumably regulated by autoreactive T cells.
Acknowledgments
We are grateful to Dr. Guerrino Meneguzzi for the generousgift of Col VII cDNA (HNC1-pcDNA3) and to Prof. LeenaBruckner-Tuderman and Dr. Silke Hofmann for EBA sera.This study was supported by grants from the DeutscheForschungsgemeinschaft (He 1602/8-1, to MH) and theBundesministerium für Bildung und Forschung (01 GN 0973to RE and MH).
References
[1] M. Chen, D. Hallel-Halevy, C. Nadelman, D.T. Woodley,Epidermolysis bullosa acquisita, in: M Hertl (Ed.), AutoimmuneDiseases of the Skin, Springer, Wien, 2005, pp. 109–132.
[2] K.B. Yancey, The pathophysiology of autoimmune blisteringdiseases, J. Clin. Invest. 115 (2005) 825–828.

107Type VII collagen and epidermolysis bullosa acquisita
[3] D.T. Woodley, J. Remington, M. Chen, Autoimmunity to type VIIcollagen: epidermolysis bullosa acquisita, Clin. Rev. AllergyImmunol. 33 (2007) 78–84.
[4] D.T. Woodley, E.J. O'Keefe, M.J. Reese, G.L. Mechanic, R.A.Briggaman, W.R. Gammon, Epidermolysis bullosa acquisitaantigen, a new major component of cutaneous basementmembrane, is a glycoprotein with collagenous domains, J.Invest. Dermatol. 86 (1986) 668–672.
[5] W.R. Gammon, D.F. Murrell, M.W. Jenison, K.M. Padilla, P.S.Prisayanh, D.A. Jones, R.A. Briggaman, S.W.D. Hunt, Auto-antibodies to type VII collagen recognize epitopes in afibronectin-like region of the noncollagenous (NC1) domain,J. Invest. Dermatol 100 (1993) 618–622.
[6] J.C. Lapiere, D.T. Woodley, M.G. Parente, T. Iwasaki, K.C.Wynn, A.M. Christiano, J. Uitto, Epitope mapping of type VIIcollagen: identification of discrete peptide sequences recog-nized by sera from patients with acquired epidermolysisbullosa, J. Clin. Invest. 92 (1993) 189–1831.
[7] T. Tanaka, F. Furukawa, S. Imamura, Epitope mapping forepidermolysis bullosa acquisita autoantibody by molecularlycloned cDNA for type VII collagen, J. Invest. Dermatol. 102(1994) 706–709.
[8] M. Chen, M.P. Marinkovich, J.C. Jones, E.A. O'Toole, Y.Y. Li, D.T.Woodley, NC1 domain of type VII collagen binds to the beta3chain of laminin 5 via a unique subdomain within the fibronectin-like repeats, J. Invest. Dermatol. 112 (1999) 177–183.
[9] C. Sitaru, A. Kromminga, T. Hashimoto, E.B. Bröcker, D.Zillikens, Autoantibodies to type VII collagen mediateFcgamma-dependent neutrophil activation and induce der-mal-epidermal separation in cryosections of human skin, Am. J.Pathol 161 (2002) 301–311.
[10] I. Shimanovich, S. Mihai, G.J. Oostingh, T.T. Ilenchuk, E.B.Bröcker, G. Opdenakker, D. Zillikens, C. Sitaru, Granulocyte-derived elastase and gelatinase B are required for dermal-epidermal separation induced by autoantibodies from patientswith epidermolysis bullosa acquisita and bullous pemphigoid, JPathol 204 (2004) 519–527.
[11] C. Sitaru, Experimental models of epidermolysis bullosaacquisita, Exp. Dermatol. 16 (2007) 520–531.
[12] D.T. Woodley, C. Chang, P. Saadat, R. Ram, Z. Liu, M. Chen,Evidence that anti-type VII collagen antibodies are pathogenicand responsible for the clinical, histological, and immunolog-ical features of epidermolysis bullosa acquisita, J. Invest.Dermatol. 124 (2005) 958–964.
[13] D.T. Woodley, R. Ram, A. Doostan, P. Bandyopadhyay, Y.Huang, J. Remington, Y. Hou, D.R. Keene, Z. Liu, Z.M. Chen,Induction of epidermolysis bullosa acquisita in mice by passivetransfer of autoantibodies from patients, J. Invest. Dermatol.126 (2006) 1323–1330.
[14] C. Sitaru, S.Mihai, C.Otto,M.T.Chiriac, I.Hausser, B.Dotterweich,H. Saito, C. Rose, A. Ishiko, D. Zillikens, Induction of dermal-epidermal separation in mice by passive transfer of antibodiesspecific to type VII collagen, J. Clin. Invest. 115 (2005) 870–878.
[15] C. Sitaru, M.T. Chiriac, S. Mihai, J. Büning, A. Gebert, A. Ishiko,D. Zillikens, Induction of complement-fixing autoantibodiesagainst type VII collagen results in subepidermal blistering inmice, J. Immunol. 177 (2006) 3461–3468.
[16] W.R. Gammon, C. Kowalewski, T.P. Chorzelski, V. Kumar, R.A.Briggaman, E.H. Beutner, Direct immunofluorescence studiesof sodium chloride-separated skin in the differential diagnosisof bullous pemphigoid and epidermolysis bullosa acquisita, J.Am. Acad. Dermatol. 22 (1990) 664–670.
[17] A. Niedermeier, R. Eming, M. Pfütze, C.R. Neumann, C.Happel, K. Reich, M. Hertl, Clinical response of severemechanobullous epidermolysis bullosa acquisita to combinedtreatment with immunoadsorption and rituximab (anti-CD20monoclonal antibody), Arch. Dermatol. 143 (2007) 192–198.
[18] M. Pfütze, A. Niedermeier, M. Hertl, R. Eming, Introducing anovel autoimmune bullous skin disorder intensity core (ABSIS)in pemphigus, Eur. J. Dermatol. 17 (2007) 4–11.
[19] R. Müller, V. Svoboda, E. Wenzel, S. Gebert, N. Hunzelmann, H.H. Müller, M. Hertl, IgG reactivity against non-conformationalNH-terminal epitopes of the desmoglein 3 ectodomain relatesto clinical activity and phenotype of pemphigus vulgaris, Exp.Dermatol. 15 (2006) 606–614.
[20] S. Hofmann, S. Thoma-Uszynski, T. Hunziker, P. Bernard, C.Koebnick, A. Stauber, G. Schuler, L. Borradori, M. Hertl, Severityand phenotype of bullous pemphigoid relate to autoantibodyprofile against the NH2-and COOH-terminal regions of the BP180ectodomain, J. Invest. Dermatol. 119 (2002) 1065–1073.
[21] S. Thoma-Uszynski, W. Uter, S. Schwietzke, S. Hofmann, T.Hunziker, P. Bernard, R. Treudler, C.C. Zouboulis, G. Schuler, L.Borradori, M. Hertl, BP230-and BP180-specific auto-antibodies inbullous pemphigoid, J. Invest. Dermatol. 122 (2004) 1413–1422.
[22] M.S. Lin, S.J. Swartz, A. Lopez, X. Ding, M.A. Fernandez-Vina,P. Stastny, J.A. Fairley, L.A. Diaz, Development and charac-terization of desmoglein-3 specific T cells from patients withpemphigus vulgaris, J. Clin. Invest. 99 (1997) 31–34.
[23] M.S. Lin, M.A. Gharia, S.J. Swartz, L.A. Diaz, G.J. Giudice,Identification andcharacterization of epitopes recognized by Tlymphocytes and autoantibodies from patients with herpesgestationis, J. Immunol. 162 (1999) 4991–4997.
[24] M.S. Lin, C.L. Fu, M. Olague-Marchan, M.K. Hacker, D. Zillikens,G.J. Giudice, J.A. Fairley, Autoimmune responses in patientswith linear IgA bullous dermatosis: both autoantibodies and Tlymphocytes recognize the NC16A domain of the BP180molecule, Clin. Immunol. 102 (2002) 310–319.
[25] L. Büdinger, L. Borradori, C. Yee, R. Eming, S. Ferencik, H.Grosse-Wilde, H.F. Merk, K.B. Yancey, M. Hertl, Identificationand characterization of autoreactive T cell responses to bullouspemphigoid antigen 2 in patients and healthy controls, J. Clin.Invest. 102 (1998) 2082–2089.
[26] C.M. Veldman, K.L. Gebhard, W. Uter, R. Wassmuth, J.Grötzinger, E. Schultz, M. Hertl, M, T cell recognition ofdesmoglein 3 peptides in patients with pemphigus vulgaris andhealthy individuals, J. Immunol. 172 (2004) 3883–3892.
[27] S. Thoma-Uszynski, W. Uter, S. Schwietzke, G. Schuler, L.Borradori, M. Hertl, Autoreactive T and B cells from bullouspemphigoid (BP) patients recognize epitopes clustered in distinctregions of BP180 and BP230, J. Immunol. 176 (2006) 2015–2023.
[28] R. Eming, L. Büdinger, R. Riechers, O. Christensen, H. Bohlen,R. Kalish, M. Hertl, M, Frequency analysis of autoreactive T-helper 1 and 2 cells in bullous pemphigoid and pemphigusvulgaris by enzyme-linked immunospot assay, Br. J. Dermatol.143 (2000) 1279–1282.
[29] M. Hertl, R. Eming, C. Veldman, T cell control in autoimmunebullous skin disorders, J. Clin. Invest. 116 (2006) 1159–1166.
[30] M. Chen, L.S. Chan, X. Cai, E.A. O'Toole, J.C. Sample, D.T.Woodley, Development of an ELISA for rapid detection of anti-type VII collagen autoantibodies in epidermolysis bullosaacquisita, J. Invest. Dermatol. 108 (1997) 68–72.
[31] D. Hallel-Halevy, C. Nadelman, M. Chen, D.T. Woodley,Epidermolysis bullosa acquisita: update and review, Clin.Dermatol. 19 (2001) 712–718.