Embed Size (px)
Citation preview

235
Systemic and Regional Hemodynamics inPatients With Salt-Sensitive Hypertension
Toshiro Fujita, Katsuyuki Ando, and Etsuro Ogata
Twenty-two patients with normal plasma renln and essential hypertension were classified as"salt-sensitive" (SS) (n=9) or "non-salt-sensitive" (NSS) (n=13) from an increase in meanblood pressure with changes in sodium intake from 25 to 250 meq/day. With the high sodiumdiet, the SS patients gained more weight (/?<0.05), retained more sodium (/><0.05), and hada greater increase in cardiac output (/?<0.05). Despite the markedly increased cardiac output,systemic vascular resistance did not change with sodium loads in the SS patients, whereas theNSS patients had a significant decrease in systemic vascular resistance. Thus, the greaterincrease in blood pressure with sodium loads in SS patients can be attributed not only to anincrease in cardiac output, possibly resulting from greater sodium retention, but also toinappropriately elevated systemic vascular resistance. Concomitant with a greater increase incardiac output, the SS patients had a greater increase in forearm blood flow with sodiumloading than the NSS patients (p<0.02). In contrast, blood flow to the kidney and the liver wasnot significantly changed in either group; renal (p<0.05) and hepatic (/><0.01) vascularresistance increased significantly in SS patients but remained unchanged in NSS patients.Thus, evidence presented suggests that the greater increase in blood pressure with sodium loadsseems to be characterized by a very inhomogenous distribution of local flow and resistance inSS patients; renal and hepatic blood flow remains essentially unchanged and skeletal muscleblood flow receives almost all of the increase in cardiac output Moreover, systemic vascularresistance changes did not reflect the resistance of individual beds because vasoconstrictionappeared in the kidney and the splanchnic area but was masked by prominent vasodilation inthe skeletal muscle. Because this hemodynamic pattern is similar to the pattern evoked duringdefense reaction, it is suggested that sympathetic overactivity on a selective basis might beinvolved in the impaired renal function for sodium excretion and the increase in blood pressurewith sodium loads in SS patients. (Hypertension 1990,16:235-244)
It is widely believed that excessive sodium intakeplays a role in the development of hypertensionin humans.1 However, the mechanisms by which
excess salt intake increases blood pressure in humansare not clear.2^
In previous studies, patients with hypertensionwere classified as salt-sensitive (SS) or non-salt-sensitive (NSS) as estimated from the rise in bloodpressure with the increase in sodium intake.4'5 On ahigh salt diet, the SS hypertensive patients retainedmore sodium and gained more weight, with a greaterincrease in cardiac output, than did the NSSpatients.5 Thus, the elevation of blood pressure withsalt loading in the SS patients was attributed to the
From the Fourth Department of Internal Medicine, Universityof Tokyo, Tokyo, and the Department of Internal Medicine,University of Tsukuba, Ibaraki, Japan.
Address for correspondence: Toshiro Fujita, MD, the FourthDepartment of Internal Medicine, University of Tokyo, School ofMedicine, 3-28-6 Mejirodai, Bunkyo-ku, Tokyo 112, Japan.
Received February 21,1989; accepted in revised form April 24,1990.
increased cardiac output, possibly by sodium reten-tion. Because glomerular filtration rate was almostnormal in the SS patients, there are considerablepossibilities that the impaired renal function forsodium excretion, the most characteristic finding inSS hypertension, might be due not only to morpho-logical but also to functional changes in the kidney.Although a number of factors control the renalhandling of sodium, neural mechanisms are impor-tant in the renal function for sodium excretion andthe resultant development of hypertension. In ratswith deoxycorticosterone acetate (DOCA)-salthypertension, a model of salt-dependent hyperten-sion, the increased sympathetic activity in the kidneymight contribute, through sodium retention,6-7 to thedevelopment of hypertension. Accordingly, we5'8-9
and recently GUI et al10 have hypothesized that thepersistence of autonomic "drive" in the SS patientsmight play an important role in the impaired renalfunction for sodium excretion and the resultantincreases in cardiac output and blood pressure with
by guest on June 30, 2018http://hyper.ahajournals.org/
Dow
nloaded from
236 Hypertension Vol 16, No 3, September 1990
sodium loads. This hypothesis was supported by thestudies of Campese et al11 and Koolen and VanBrummelen12 that reported higher plasma norepineph-rine concentrations during salt loading in SS hyperten-sive patients as compared with the NSS patients.
In general, autonomic activation in essential hyper-tension is not generalized but is regional.1314 Becausethe sympathetic nervous system is the key factor inregulating vasoconstrictor tone, it is not equal in thedifferent organs15; a defense reaction triggered, forexample, by mental arithmetic induced a peculiarhemodynamic pattern of increased vascular resistancein the kidney and the splanchnic area and a decreasedvascular resistance in the skeletal muscle vascular bed,suggesting increased sympathetic tone on a selectivebasis.16-17 Thus, the degree of sympathetic tone in thedifferent tissues can be estimated indirectly by mea-suring the change in blood flow and the resistance ofindividual beds. Consequently, if there are abnormalresponses of the sympathetic nervous system tosodium loading in the SS patients, the pattern ofchanges in regional blood flow with sodium loading inthe SS patients should differ from that in the NSSpatients. Interestingly, the recent study of Lawton etal18 showed that dietary salt loading in borderlinehypertensive subjects produced enhanced renal vaso-constriction during standing, suggesting that salt load-ing might unmask the increased renal sympathetictone and then cause exaggerated reflex vasoconstric-tor responses. However, only a few studies haveexamined changes in blood flow in the different organsduring salt loading in SS hypertensive patients. In thepresent study, therefore, we studied the changes insystemic and regional hemodynamics with sodiumloads in patients with SS hypertension to furtherassess the role of the sympathetic nervous system invascular resistance changes and blood pressureincreases with sodium loads.
MethodsTwenty-two patients with essential hypertension
(15 men, seven women) were studied. These patientshad mild-to-moderate hypertension, with casual(morning) clinic blood pressure from 150 to 180mm Hg systolic and 90 to 115 mm Hg diastolic.Patients with primary aldosteronism, pheochromocy-toma, renal vascular disease, diabetes mellitus, orCushing's syndrome were excluded by complete his-tory and physical examination, urinalysis, rapid-sequence intravenous pyelograms, plasma potassiumand creatinine, plasma renin activity, aldosteroneand norepinephrine, and 24-hour urinary 17-hydroxycorticosteroids, metanephrine, and vanillylmandelic acid. There was no evidence of cardiacfailure or of liver damage in any of the patients, andnone had "malignant" hypertension. The electrocar-diogram investigation was done to detect left ventric-ular hypertrophy. A subject was considered to have apositive family history of hypertension if either orboth parents had hypertension. This information, tolearn of a "probable genetic background of hyperten-
sion" (World Health Organization workshop19), wasobtained by questioning the subjects. Twenty-two unse-lected hypertensive patients were entered into thestudy. All subjects read and signed an informed consentoutlining the details of the tests to be performed.
ProtocolAll antihypertensive medications had been discon-
tinued at least 2 weeks before admission. Eachsubject was maintained on a constant activity patternand adhered to a daily constant diet containing 25meq sodium and 70 meq potassium (low sodiumdiet). Patients were studied for 4 days with this dietto which 140 meq NaQ was added each day (normalsodium diet). Then, the low sodium diet alone wasgiven for 3 days, followed by 6 days of the low sodiumdiet to which 225 meq NaCl was added each day(high sodium diet). On the first day of the low sodiumdiet, 40 mg furosemide was injected intravenously.
Body weight was measured each morning at 7:00AM after the patient had voided. Daily urine collec-tions were made from admission to discharge toassess urinary sodium and creatinine excretion and todetermine both creatinine clearance and the com-pleteness of urine collection. Urine collections had tobe complete, as judged by a daily creatinine excretionwithin 10% of the mean for the entire admission.Every 4 hours throughout the study, after the patienthad been supine for 5 minutes or longer, bloodpressure was measured by sphygmomanometer.Mean blood pressure, calculated for every 4-hourreading (day and night) as diastolic pressure plus onethird of pulse pressure, for the third day of the lowsodium diet and the sixth day of the high sodium dietwas a statistical comparison of the effects of dietarysodium on blood pressure. As in previous studies,4-5
patients whose average mean blood pressure valueon day 6 of the high sodium regimen exceeded by10% or more that on the third day of the low sodiumdiet were classified as SS, those whose average meanblood pressure decreased, did not change, orincreased by less than 10%, as NSS (Figure 1).
With the patient supine, blood was drawn from allsubjects on the last day of the normal sodium diet,the furosemide plus low sodium diet, and the highsodium diet for hematocrit, plasma sodium, andplasma potassium determinations. Plasma and urinesodium and potassium concentrations were mea-sured with a flame photometer, and plasma andurinary creatinine was measured by an autoanalyzermethod. Radioimmunoassay was used to measureplasma renin activity and aldosterone.20'21 Normalrenin essential hypertension, present in all cases, wasdefined as plasma renin between 2.5 and 15 ngangiotensin I/ml/hr in a sample drawn from thesubjects after they had been in an upright position for2 hours and after balance had been achieved with a165 meq sodium intake after oral administration of40 mg furosemide.
The hemodynamic studies were performed on thethird day of the low sodium diet and on the sixth day
by guest on June 30, 2018http://hyper.ahajournals.org/
Dow
nloaded from

Fujita et al Hemodynaraics In Salt-Sensitive Patients 237
28|
2 0 '
Q.m(0 16O
10
N88
Low Na High Na
FIGURE 1. Graph showing increase in mean blood pressure(BP) with a change from the low (25 meq/day) to the high(250 meq/day) sodium diet for each patient. Mean±SEM forsalt-sensitive (SS) and non-salt-sensitive (NSS) patients areindicated on right side of figure. *p<0.001 (unpaired t test).
of the high sodium diet. The patients were studied inthe resting state in an air-conditioned laboratory,with ambient temperature ranging from 24° C to27° C. Cardiac output was determined by dye dilution(indocyanine green) as previously described.20-2* Car-diac output was measured at least 20 minutes aftereach patient had rested supine in the morning, butnot before the subject was subjectively relaxed andhad a stable pulse rate. Cardiac index was expressedas liters per minute per meters squared. Systemicvascular resistance (SVR) was calculated as the ratioof mean blood pressure to cardiac index, expressed inunits of dynes-second-centimeter^-meters squared.
Forearm blood flow (FBF) was measured by aplethysmographic technique, as described previous-ly.22 Changes in forearm blood volume were deter-mined by means of a mercury-in-rubber strain-gaugeplethysmograph23 placed on the mid forearm. Withthe subject comfortable in the supine position and hisarms supported at a 45° angle from the long axis of thebody, a strain-gauge was mounted so that its maximaltension was less than 10 g, to prevent the gauge fromobstructing even the superficial veins beneath it. Toeliminate the vessels in the hand from these determi-nations, a sphygmomanometric cuff 7 cm wide wasplaced around the wrist and inflated to a level exceed-ing systolic arterial pressure just before each venousocclusion. A sphygmomanometric cuff 13 cm wide wasplaced around the upper arm, and forearm venousocclusion was produced by suddenly inflating this cuffto a pressure below the diastolic arterial pressure (40mm Hg),24 using a tank of compressed air to provide aconstant pressure source. FBF was taken as the aver-age of 4-8 flow measurements made at 15-secondintervals. Calculation of FBF was done independentlyby two of the authors from the copied records, and theaverage value was used for statistical analysis. Theblood pressure was measured in the other arm with a
sphygmomanometer. FBF, expressed as milliliters per100 milliliters forearm volume per minute, was calcu-lated from the change in forearm circumference dur-ing venous occlusion. Forearm vascular resistance(FVR) was calculated by dividing mean blood pres-sure (mmHg) by forearm blood flow (ml/100 mlforearm volume/min); these values are expressed as"units" throughout this report.
In this method of FBF measurements, a within-observer variability is 2.8%, and a between-observervariability is 3.6%. Under these experimental condi-tions, repeated FBF measurements (on two differentdays) in a separate group of 10 normal subjects whensodium intake remained constant gave a 13.2±15.8%variation coefficient.
Renal blood flow (RBF) was determined by thesingle injection clearance of iodine-131 para-aminohippurate ("'I-PAH)25 on the basis of themodel proposed by Sapirstein et al.26 The fastingpatients were recumbent for 30 minutes before theinjection of mI-PAH. 131I-PAH (60 Ci/1.73 m2) wasinjected intravenously and heparinized blood samples(5 ml) were drawn at 5, 10, 15, 20, 30, 40, 50, and 60minutes after injection. Renal plasma flow was calcu-lated as proposed by Sapirstein et al.26 This value wascorrected for hematocrit and body surface area, andRBF was expressed in milliliters per minute per metersquared. Renal vascular resistance (RVR) was calcu-lated as the ratio of mean blood pressure to RBF(expressed in units of dynes-sec-cnT^m2).
In a group of 10 normal subjects in whom duplicatedeterminations of 131I-PAH clearance were obtainedby this method on two different days while thesubjects were maintained on the same diet, the meanestimated RBF was l,106±54 ml/min/m2. The abso-lute day-to-day variation was 40 ±44 ml/min/m2, anaverage of 3.6±4.0%.
131I-PAH clearance was compared in a group ofseven normal subjects on a high (250 meq/day) versusa low (25 meq/day) sodium diet. There was a signif-icant increase (163±36 ml/min/m2,/?<0.01, by pairedt test) in 131I-PAH clearance with salt loading(l,076±41 versus 913±46 ml/min/m2). The resultsobtained provide evidence that the method for mea-surement of RBF, as performed in our laboratory, issignificantly sensitive enough to detect small changesin blood flow.
In the present study, indocyanine green was usedto estimate hepatic blood flow (HBF).27 A bolus ofindocyanine green (50 mg) was rapidly injected intoan antecubital vein and a 2 ml sample of blood wasdrawn at 4, 6, 8,10,12,14,16,18, 20, and 22 minutesafter the injection. Indocyanine green concentrationsin the serum were estimated with a Beckman DU-2spectrophotometer (Beckman Instruments, Inc.,Irvine, Calif.) at a wavelength of 805 nm. Concentra-tions were read off a standard calibration curveprepared with solutions of known concentrations ofthe dye made up in pooled human serum. The values,when plotted against time on semilogarithmic paper,fell in a straight line. This exponential disappearance
by guest on June 30, 2018http://hyper.ahajournals.org/
Dow
nloaded from

238 Hypertension Vol 16, No 3, September 1990
permitted extrapolation back to zero time.28 Opticaldensity units were converted to plasma concentra-tions by reference to standard curves of dye in plasmaconstructed with each dye lot and found to be linear inthe concentration range used in these studies. Plasmavolume was estimated from the volume of distributionof indocyanine green, which was calculated as theratio of the amount of dye injected (mg) to extrapo-lated concentration at zero time (mg/ml). Fractionalclearance was calculated using the method of leastsquares for the natural logarithmic values of the serumconcentration. Subsequently, the fractional clearancewas multiplied by the plasma volume to obtain plasmaclearance of indocyanine green. This value was cor-rected for hematocrit to obtain the total blood clear-ance, that is, HBF (expressed in ml/min/m2). Hepaticvascular resistance (HVR) was calculated as ratio ofmean blood pressure to HBF (expressed in units ofdynes-sec-cm~5-m2.)
The absolute average difference in paired indocy-anine green measurements on a single sample on thesame run is less than 1%. The internal standards varyby 1% or less on different days. In a group of ninenormal subjects in whom duplicate determinations ofindocyanine green clearance were obtained by thismethod on two different days while they were ingest-ing the same diet, the mean estimated HBF was1,116±76 ml/min/m2. The absolute day-to-day varia-tion was 52±66%, an average of 4.7±5.9%.
Statistical Analysis
Mean±SEM and correlation coefficients were cal-culated by the standard statistical method. Regres-sion analyses were carried out by the least-squaresmethod. Differences in means between two groupswere assessed by Student's t test. Ap value less than0.05 was accepted as statistically significant.
ResultsNine patients fell into the SS group and 13 into the
NSS group by our criteria (Figure 1). Their distribu-tion by age and sex is given in Table 1. There was nosignificant difference in age, sex distribution, orknown duration of hypertension. Also, there were nosignificant differences in systolic and diastolic bloodpressure levels, in secondary effects of hypertensionas revealed by serum creatinine, or in the incidenceof left ventricular hypertrophy or retinopathy (Table1). Indexes of the state of the renin-angiotensin-aldosterone system and plasma and urinary electro-lytes also did not differ when external sodium balancehad been achieved on a low sodium diet (Table 2).
The average mean blood pressure values for the SSpatients taking the normal sodium diet, the low sodiumdiet, and the high sodium diet were 111±2,101 ±2, and116±2 mm Hg, respectively (Table 3). Correspondingaverages of mean blood pressure values for the NSSpatients were 110±3, 104±2, and 110±2 mmHg,respectively. The mean decrement of mean blood pres-sure between the normal sodium and low sodium dietswas significantly (p<0.05) greater in the SS than in the
TABLE 1. Clinical Data
Variables
NumberAge (yr)
Gender (female: male)Prior drug therapyFamily history positiveDuration of hypertension (yr)Left ventricular hypertrophyRetinopathyBlood pressure (mm Hg)
Highest recordedSystolicDiastolic
AdmissionSystolicDiastolic
StudySystolicDiastolic
Serum creatinine (mg/dl)
Salt-sensitive
948±44=55/95/9
7.8+.0.65/94/9
166±5113±3
152±3100+2
147±293±21.0±0.1
Non-salt-sensitive
1344±33:10
10/1311/13
73+1.36/135/13
165±5112±2
151+299+2
146±492±21.0±0.1
Values are mean±SEM.
NSS patients (-8.9+1.5% versus -5.5±0.8%). Also,the mean increment of mean blood pressure withsodium loading differed significantly (p<0.01)between the SS and NSS groups (14.8±1.5% versus6.2±0.7%) (Figure 1).
Sodium BalanceUrinary sodium during the normal sodium diet was
not significantly different in either group, as shown inFigure 2. On the third day of sodium restriction,urinary sodium decreased equally in both groups(Table 2 and Figure 2). On the last day of the high
Table 2. Physiological Variables
Variables
Weight (kg)Plasma renin activity
(ng Ang tyml/hr)Plasma aldosterone (ng/dl)Sodium concentration, serum
(meq/1)Potassium concentration, serum
(meq/1)Sodium excretion
(meq/24 hr)Potassium excretion
(meq/24 hr)Creatinine clearance
(mVmin/1.73 m2)
Salt-sensitive
63.7±2.6
6.4±1.919.8±3.2
139±2
4.2±0.1
25±6
65±7
113±12
Non-salt-sensitive
66.5±2.7
8.9±1.124.2±5.8
138±2
4.2±0.1
28±4
62±6
110±14
Values are mean±SEM. Data refer to values obtained whenbalance had been achieved with a 25 meq sodium intake. Bloodsamples were obtained between 7:00 and 8:00 AM with subjects ina recumbent position. Ang I, angiotensin I.
by guest on June 30, 2018http://hyper.ahajournals.org/
Dow
nloaded from

Fujita et al Hemodynamlcs in Salt-Sensitive Patients 239
TABLE 3. Systemic and Regional Hemodynamlcs in Salt-Sensitive and Non-Salt-Stnsltive Hypertensive Patients
Hemodynamic measurements
Systolic blood pressure (mm Hg)Diastolic blood pressure (mm Hg)Mean blood pressure (mm Hg)Heart rate (beats/min)Cardiac index (1/min/m2)Systemic vascular resistance (units)Forearm blood flow (ml/100 ml/min)Forearm vascular resistance (units)Hepatic blood flow (ml/min/m2)Hepatic vascular resistance (units)Renal blood flow (ml/min/m2)Renal vascular resistance (units)
Salt-sensitive
Low Na
133±285±2
101±269±23.4±0.4
2,674±2693.0±0.3
37.6±3.41,135±97
7.8±0.7726±4212.5±0.7
HighNa
153±3*98±2*
116±2*65±24.0±0.4*
2,469±2043.8±0J*
31.7±2.9*l,029±82
9.2±0.6*751±3113.6±0.7*
Non-salt-sensitive
Low Na
134±389±2
104±272±23.1±0.2
2,891 ±1972.8±0.3
41.7±3.31,200±77
7.3 ±0.5896±4110.4±0.6
HighNa
146±4'92±2*
110±2't67±2|3.4±0.2*
2,682±176'2.7±0.1§
41.0±1.5§l,190±76
7.7±0.5
9O6±43t10.8±0.6f
'/><0.01 versus patients on the low sodium diet, by paired t test1p<0.05 versus salt-sensitive patients, by unpaired t test.ip<Q.QS versus patients on the low sodium diet, by paired t test£ versus salt-sensitive patients, by unpaired t test
sodium diet, urinary sodium was quite close betweenthe SS and NSS patients (248 ±14 meq/day versus250 ±13 meq/day, respectively) despite the signifi-cantly (/><0.05) higher level of blood pressure in theSS than in the NSS patients (116±2 mm Hg versus110±2 mm Hg, respectively) (Table 3 and Figure 2).Therefore, the slope of the blood pressure/urinarysodium excretion curve for the kidneys of the SShypertensive patients apparently decreased as com-pared with that of the NSS patients (Figure 2).
An estimate of the mean cumulative sodium reten-tion (intake sodium minus urinary sodium) over the 6days of the high sodium diet was 204 ±32 meq in theSS patients and 125±26 meq (/><0.05) in the NSSpatients; the SS patients retained significantly moresodium over the 6 days of high sodium diet than had
~ 300o
O
oX111Eo0}
200NSS .SS
90 100 110 120
Mean Blood Pressure (mmHg)
FIGURE 2. Line graph showing relation between mean bloodpressure and measured 24-hour urinary sodium excretion forsame period. Slope of renal function curve obtained innon-salt-sensitive (NSS) patients (n=13) (o) was steepercompared with that in salt-sensitive (SS) patients (n=9) (•) .
the NSS patients. These differences in sodium excre-tion could not be explained by a difference in filteredsodium load as estimated by creatinine clearance andserum sodium concentration (Table 2). Body weightchanges showed the anticipated increase from thedata on external sodium balance by 0.7±0.1 kg in theNSS patients and 1.2±0.2 kg (p<0.05) in the SSpatients. Concomitantly, the SS patients had agreater increase in plasma volume than the NSS ones(693+157 versus 195±135 ml,p<0.05).
Systemic HemodynamicsThe average cardiac indexes for the SS patients on
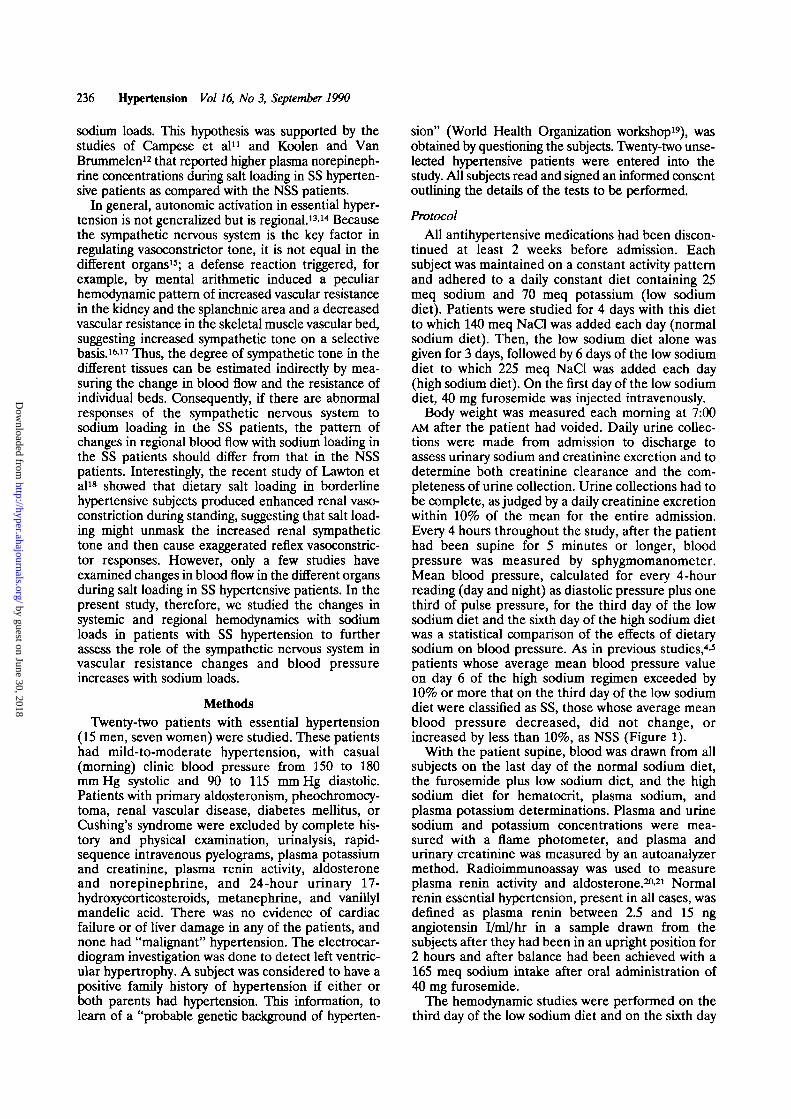
the low sodium and high sodium diets were 3.4±0.4and 4.0±0.4 1/min/m2, respectively (/?<0.01, by pairedt test) (Table 3). Corresponding averages of cardiacindex were 3.1 ±0.2 and 3.4±0.2 1/min/m2 (p<0.01, bypaired t test) for the NSS patients on the low sodiumand the high sodium diets, respectively (Table 3). Themean increments of cardiac output between the lowsodium and the high sodium diets, calculated for eachpatient, differ significantly between the groups(19.4±4.5% versus 9.5±1.5%,/><0.05) (Figure 3). Incontrast, there was no significant change of SVR withsodium loads in the SS patients (-5.2±3.9%, NS),although SVR was significantly decreased in the NSSpatients (-7.0±1.4%,/><0.01) (Figure 3).
Regional HemodynamicsThe average FBF for the SS patients on the low
sodium and high sodium diets were 3.0±0.3 and3.8 ±0.3 ml/100 ml/min, respectively (/?<0.05, bypaired t test) (Table 3). Corresponding averages ofFBF were 2.8 ±0.3 and 2.7 ±0.1 ml/100 ml/min (NS,by paired t test) for the NSS patients on the lowsodium and the high sodium diets, respectively. Themean increments of FBF between the low sodiumand the high sodium diets, calculated for eachpatient, differed significantly between the groups
by guest on June 30, 2018http://hyper.ahajournals.org/
Dow
nloaded from
240 Hypertension Vol 16, No 3, September 1990
OO
25"
20"
16-
1 0 -
5 --3B
- 1 0 } -
- 2 0 -
m
-261-
SS NSSFIGURE 3. Bar graph showing percent changes in cardiacoutput (%&CO) and systemic vascular resistance (%hSVR)with sodium load in salt-sensitive (SS) (n=9) and non-salt-sensitive (NSS) (n=13) patients. Despite the markedlyincreased CO, SVR remained unchanged with sodium load inSS patients, but it decreased significantly in NSS patients.*p<0.01 (paired t test); §p<0.05 (versus NSS, by unpaired ttest).
(31.9±8.6% versus 1.6±7.3%, p<0.02) (Figure 4).Thus, FBF in those patients on the high sodium dietwas significantly greater in those that were SS than inthose that were NSS (3.8+0.3 versus 2.7+0.1 ml/100ml/min, p<0.01); FBF in those patients on the low
o
OOm"ocoo>CD
a.mOc
40 -
30 -
20 -
10
§ -10-O<D
%
40
30
20
10
- - 1 0
FBF HBF RBF
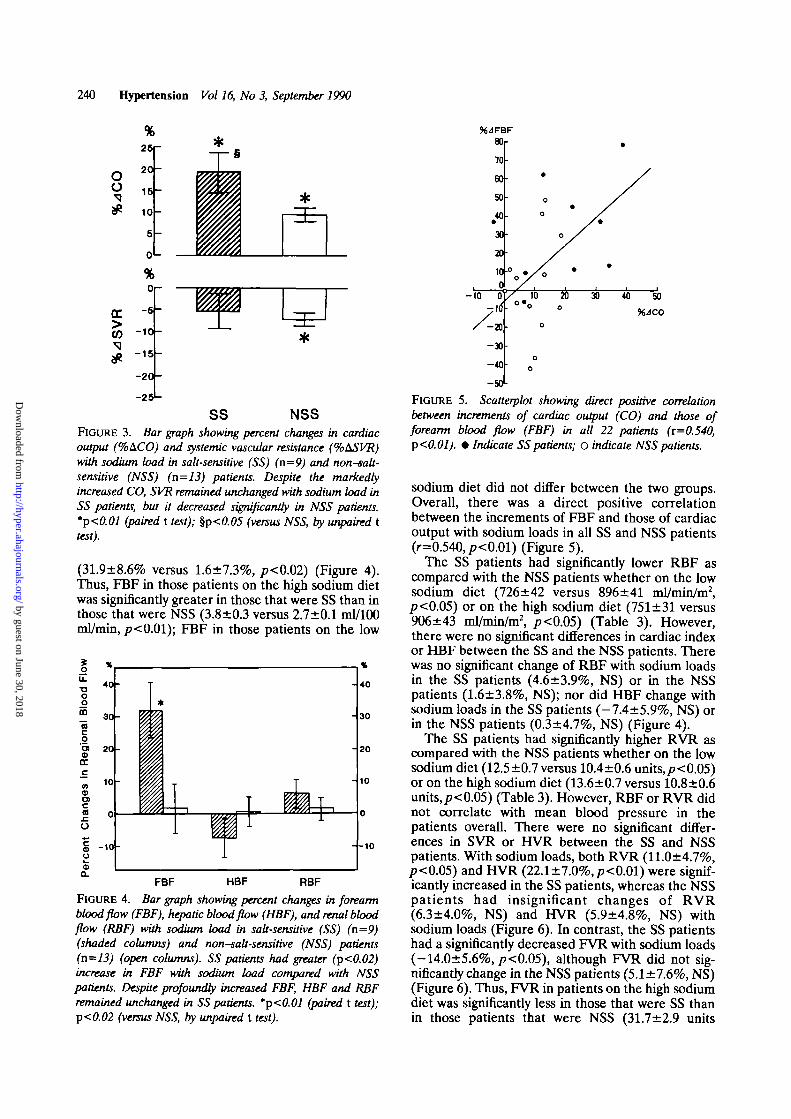
FIGURE 4. Bar graph showing percent changes in forearmblood flow (FBF), hepatic blood flow (HBF), and renal bloodflow (RBF) with sodium load in salt-sensitive (SS) (n=9)(shaded columns) and non-salt-sensitive (NSS) patients(n=13) (open columns). SS patients had greater (p<0.02)increase in FBF with sodium load compared with NSSpatients. Despite profoundly increased FBF, HBF and RBFremained unchanged in SS patients. *p<0.01 (paired t test);p<0.02 (versus NSS, by unpaired t test).
FIGURE 5. Scatterplot showing direct positive correlationbetween increments of cardiac output (CO) and those offorearm blood flow (FBF) in all 22 patients (i=0.540,p<0.01). • Indicate SS patients; o indicate NSS patients.
sodium diet did not differ between the two groups.Overall, there was a direct positive correlationbetween the increments of FBF and those of cardiacoutput with sodium loads in all SS and NSS patients(r=0.540,/j<0.01) (Figure 5).
The SS patients had significantly lower RBF ascompared with the NSS patients whether on the lowsodium diet (726 ±42 versus 896+41 ml/min/m2,p<0.05) or on the high sodium diet (751±31 versus906±43 ml/min/m2, p<0.05) (Table 3). However,there were no significant differences in cardiac indexor HBF between the SS and the NSS patients. Therewas no significant change of RBF with sodium loadsin the SS patients (4.6±3.9%, NS) or in the NSSpatients (1.6±3.8%, NS); nor did HBF change withsodium loads in the SS patients (-7.4±5.9%, NS) orin the NSS patients (0.3+4.7%, NS) (Figure 4).
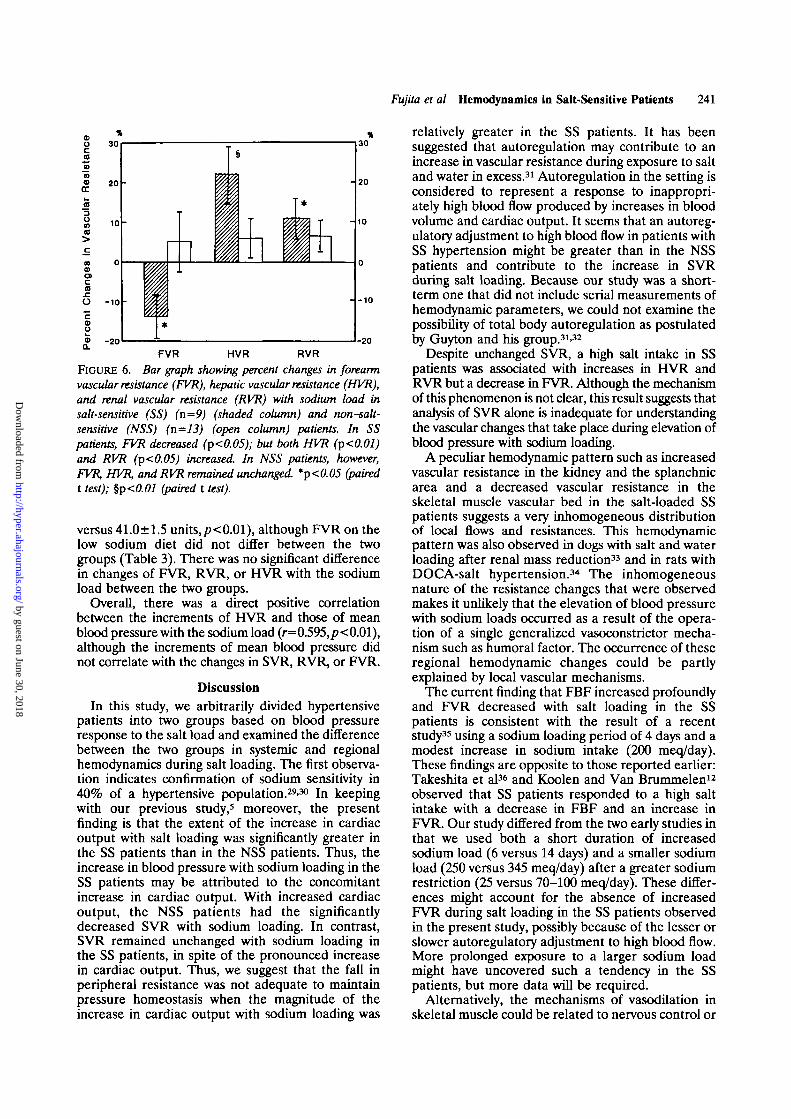
The SS patients had significantly higher RVR ascompared with the NSS patients whether on the lowsodium diet (12.5±0.7 versus 10.4±0.6 units, £< 0.05)or on the high sodium diet (13.6±0.7 versus 10.8+0.6units, p<0.05) (Table 3). However, RBF or RVR didnot correlate with mean blood pressure in thepatients overall. There were no significant differ-ences in SVR or HVR between the SS and NSSpatients. With sodium loads, both RVR (11.0±4.7%,P<0.05) and HVR (22.1±7.0%,/><0.01) were signif-icantly increased in the SS patients, whereas the NSSpatients had insignificant changes of RVR(6.3±4.0%, NS) and HVR (5.9±4.8%, NS) withsodium loads (Figure 6). In contrast, the SS patientshad a significantly decreased FVR with sodium loads(-14.0±5.6%, p<0.05), although FVR did not sig-nificantly change in the NSS patients (5.1 ±7.6%, NS)(Figure 6). Thus, FVR in patients on the high sodiumdiet was significantly less in those that were SS thanin those patients that were NSS (31.7±2.9 units
by guest on June 30, 2018http://hyper.ahajournals.org/
Dow
nloaded from
Fujita et al Hemodynamics in Salt-Sensitive Patients 241
oca1?toeo
CC
3OmCD
aCDacaO -10 •ca>u<5a. - 2 0 -20
FVR HVR RVR
FIGURE 6. Bar graph showing percent changes in forearmvascular resistance (FVR), hepatic vascular resistance (HVR),and renal vascular resistance (RVR) with sodium load insalt-sensitive (SS) (n=9) (shaded column) and non-salt-sensitive (NSS) (n=13) (open column) patients. In SSpatients, FVR decreased (p<0.05); but both HVR (p<0.01)and RVR (p<0.05) increased In NSS patients, however,FVR, HVR, and RVR remained unchanged *p<0.05 (pairedt test); %p<0.01 (paired t test).
versus 41.0±1.5 units,p<0.01), although FVR on thelow sodium diet did not differ between the twogroups (Table 3). There was no significant differencein changes of FVR, RVR, or HVR with the sodiumload between the two groups.
Overall, there was a direct positive correlationbetween the increments of HVR and those of meanblood pressure with the sodium load (r=0.595,/?<0.01),although the increments of mean blood pressure didnot correlate with the changes in SVR, RVR, or FVR.
DiscussionIn this study, we arbitrarily divided hypertensive
patients into two groups based on blood pressureresponse to the salt load and examined the differencebetween the two groups in systemic and regionalhemodynamics during salt loading. The first observa-tion indicates confirmation of sodium sensitivity in40% of a hypertensive population.29-30 In keepingwith our previous study,5 moreover, the presentfinding is that the extent of the increase in cardiacoutput with salt loading was significantly greater inthe SS patients than in the NSS patients. Thus, theincrease in blood pressure with sodium loading in theSS patients may be attributed to the concomitantincrease in cardiac output. With increased cardiacoutput, the NSS patients had the significantlydecreased SVR with sodium loading. In contrast,SVR remained unchanged with sodium loading inthe SS patients, in spite of the pronounced increasein cardiac output. Thus, we suggest that the fall inperipheral resistance was not adequate to maintainpressure homeostasis when the magnitude of theincrease in cardiac output with sodium loading was
relatively greater in the SS patients. It has beensuggested that autoregulation may contribute to anincrease in vascular resistance during exposure to saltand water in excess.31 Autoregulation in the setting isconsidered to represent a response to inappropri-ately high blood flow produced by increases in bloodvolume and cardiac output. It seems that an autoreg-ulatory adjustment to high blood flow in patients withSS hypertension might be greater than in the NSSpatients and contribute to the increase in SVRduring salt loading. Because our study was a short-term one that did not include serial measurements ofhemodynamic parameters, we could not examine thepossibility of total body autoregulation as postulatedby Guyton and his group.31'32
Despite unchanged SVR, a high salt intake in SSpatients was associated with increases in HVR andRVR but a decrease in FVR. Although the mechanismof this phenomenon is not clear, this result suggests thatanalysis of SVR alone is inadequate for understandingthe vascular changes that take place during elevation ofblood pressure with sodium loading.
A peculiar hemodynamic pattern such as increasedvascular resistance in the kidney and the splanchnicarea and a decreased vascular resistance in theskeletal muscle vascular bed in the salt-loaded SSpatients suggests a very inhomogeneous distributionof local flows and resistances. This hemodynamicpattern was also observed in dogs with salt and waterloading after renal mass reduction33 and in rats withDOCA-salt hypertension.34 The inhomogeneousnature of the resistance changes that were observedmakes it unlikely that the elevation of blood pressurewith sodium loads occurred as a result of the opera-tion of a single generalized vasoconstrictor mecha-nism such as humoral factor. The occurrence of theseregional hemodynamic changes could be partlyexplained by local vascular mechanisms.
The current finding that FBF increased profoundlyand FVR decreased with salt loading in the SSpatients is consistent with the result of a recentstudy35 using a sodium loading period of 4 days and amodest increase in sodium intake (200 meq/day).These findings are opposite to those reported earlier:Takeshita et al36 and Koolen and Van Brummelen12
observed that SS patients responded to a high saltintake with a decrease in FBF and an increase inFVR. Our study differed from the two early studies inthat we used both a short duration of increasedsodium load (6 versus 14 days) and a smaller sodiumload (250 versus 345 meq/day) after a greater sodiumrestriction (25 versus 70-100 meq/day). These differ-ences might account for the absence of increasedFVR during salt loading in the SS patients observedin the present study, possibly because of the lesser orslower autoregulatory adjustment to high blood flow.More prolonged exposure to a larger sodium loadmight have uncovered such a tendency in the SSpatients, but more data will be required.
Alternatively, the mechanisms of vasodilation inskeletal muscle could be related to nervous control or
by guest on June 30, 2018http://hyper.ahajournals.org/
Dow
nloaded from
242 Hypertension Vol 16, No 3, September 1990
to some physical or functional characteristic of thisvascular bed. During the initial stage of salt loading,high and low pressure mechanoreceptors are stimu-lated, prompting reflex alterations in the effectorsegments of the circulation. Abboud et al37 foundthat carotid and cardiopulmonary baroreceptors pro-duced nonuniform regional vascular responses dur-ing venous pooling by lower body suction: cardiopul-monary baroreceptors exert the predominantinfluence on FVR but appear to have only minorinfluence on splanchnic vascular resistance. There-fore, it might be that some of these reflexes affectmore particularly the skeletal muscle vascular bedduring salt loading. Otherwise, skeletal muscle vaso-dilation might actively be effected by sympatheticcholinergic vasodilators.
How important a role are these regional hemody-namic changes likely to play in the process of increas-ing cardiac output and blood pressure with sodiumloading in the SS patients? On the basis of animalexperiments,38 it seems likely that arteriolar vasodi-lation of muscles is analogous to opening an arterio-venous fistula. In contrast to the short time constantfor venous drainage of the skeletal muscles, thesplanchnic bed has a long time constant for venousdrainage. If such is the case in humans, there is aconsiderable possibility that a redistribution of localflows and resistances with vasoconstriction in thesplanchnic bed and an increase in muscle blood flow,which was observed in the salt-loaded SS patients,might contribute to the profound increase in cardiacoutput through a faster average venous return to theheart by means of the shorter time constant pathway.It is suggested that skeletal muscle blood flowreceives almost all of the increase in cardiac outputwith sodium loads in the SS patients to maintain highcardiac output. Moreover, the selective vasoconstric-tion in the splanchnic bed during salt loading maycontribute to the rise in blood pressure, not only byincreased vascular resistance but also by increasedcardiac output, through increased central blood vol-ume via splanchnic venous constriction.
The present finding that the SS patients retainedmore sodium and gained more weight during the highsodium-diet period suggests that the SS patientshave an impaired renal function for sodium excretiondespite a normal glomerular filtration rate, which isconsistent with previous studies.510'39-41 Because theSS patients had significantly lower RBF and higherRVR than did the NSS patients, it is suggested thatthe abnormality of renal hemodynamics in the SSpatients might be involved in the impaired renalability to excrete sodium in the urine. To account forthe observation that the SS patients had lower RBFthan the NSS patients, one might speculate that theSS patients had suffered from more severe organdamage due to hypertension than the NSS ones.However, the evidence does not support such asuggestion, as there were no significant differences insystolic and diastolic blood pressure or secondaryeffects of hypertension, as revealed by creatinine
clearance and the incidence of left ventricular hyper-trophy. In addition, the variances of mean bloodpressure (67.6 versus 80.0, F=1.18, NS) were quiteclose between the SS and NSS patients. Finally, therewere no significant correlations of mean blood pres-sure with RBF or RVR in all the patients. Thus, theincreased RVR and reduced RBF in the SS patientsdid not appear to be a consequence of hypertension.
Although many extrarenal factors regulate renalvascular tone, neural mechanisms may play an impor-tant role in the control of renal sodium handling.42
Several investigators demonstrated that long-termintrarenal infusion of low dose norepinephrine indogs caused not only the decreased RBF but alsoresulted in an increasingly higher arterial pressurelevel with progressive increases in sodium intakeassociated with the shifted renal function curve.43'44
In previous studies, patients with SS hypertensionhad inappropriately high levels of plasma norepi-nephrine during sodium loading5-10-12 and greaterincrements of plasma norepinephrine duringstanding11 compared with the NSS patients, thussuggesting the persistence of autonomic "drive" inthe sodium-loaded patients with SS hyperten-sion.5-10-12 Therefore, it can be speculated that theincreased sympathetic activity with salt loading maycontribute to the decreased RBF through increasedrenal vascular resistance and thus induce theimpaired renal function for sodium excretion in SSpatients. In general, autonomic activation in essen-tial hypertension is regional rather than general-ized,13-14 so that the measurement of total plasmanorepinephrine and tests for generalized activationare inadequate.45-4* In the present study, we mea-sured regional blood flows to further assess changesin the sympathetic activity in individual vascular bedswith salt loading. As a result, salt loading caused adefenselike hemodynamic pattern of increased RVRand HVR and decreased FVR in the SS patients,which might reflect an increased neurogenic tone inthe renal and splanchnic area on a selective basis.47-48
Interestingly, Koepke and DiBona49 demonstratedthat high sodium intake could not only enhance therenal sympathetic nerve activity but also antinatri-uretic responses to air stress in the spontaneouslyhypertensive rat, which might be dependent on acentrally mediated facilitation of sympathetic neuraloutflow to the kidney. Accordingly, Lawton et al18
also demonstrated that salt loading caused an exag-gerated renal vasoconstrictor and antinatriureticresponse to standing in young patients with essentialhypertension. Therefore, there is a considerable pos-sibility that an augmented centrally mediated outflowto the kidney could mediate the altered renovascularresponse to sodium loading, and thus shift thesodium-loaded renal function curve to the higherpressure levels, resulting in sodium retention andblood pressure rise with sodium loading in patientswith SS hypertension. However, further studies arenecessary to clarify the primary cause of impaired
by guest on June 30, 2018http://hyper.ahajournals.org/
Dow
nloaded from

Fujita et al Hemodynamics in Salt-Sensitive Patients 243
renal hemodynamics and blood pressure rise withsodium loading in patients with SS hypertension.
References1. Dahl LK, Love RA: Evidence for relationship between
Na(chloride) intake and human essential hypertension. ArchIntern Med 1954;94:525-531
2. Mark AL, Lawton WJ, Abboud FM, Fitz AE, Conner WE,Heistad DD: Effects of high and low sodium intake on arterialpressure and forearm vascular resistance in borderline hyper-tension. Ore Res 1973;36/37(suppl I):I-194-I-198
3. Dustan HP, Bravo EL, Tarazi RC: Volume-dependent essen-tial and steroid hypertension. Am J Cardiol 1973;31:606-615
4. Kawasaki T, Delea CS, Bartter FC, Smith H: The effect ofhigh-sodium and low-sodium intakes on blood pressure andother related variables in human subjects with idiopathichypertension. Am J Med 1978;64:193-198
5. Fujita T, Henry WL, Bartter FC, Lake CR, Delea CS: Factorsinfluencing blood pressure in salt-sensitive patients withhypertension. Am J Med 1980;69:334-344
6. Katholi RE, Naftilan AJ, Oparil S: Importance of renalsympathetic tone in the development of DOCA-salt hyperten-sion in the rat. Hypertension 1980;2:266-273
7. Fujita T, Sato Y: Changes in renal and central noradrenergicactivity with potassium in DOCA-salt rats. Am J Physiol1984;246:F670-F675
8. Fujita T, Noda H, Ando K: Sodium susceptibility and potas-sium effects in young patients with borderline hypertension.Circulation 1984;69:468-476
9. Fujita T, Sato Y, Ando K; Role of sympathetic nerve activityand natriuresis in the antihypertensive actions of potassium inNad hypertension. Jpn Ore J 1983;47:1227-1231
10. Gill JR, Gullner HG, Lake CR, Lakatua DJ, Lan G: Plasmaand urinary catecholamines in salt-sensitive idiopathic hyper-tension. Hypertension 1988;11:312-319
11. Campese VM, Romoff MS, Levitan D, Saglikes Y, FriedlerRM, Massry SG: Abnormal relationship between sodiumintake and sympathetic nervous system activity in salt-sensitivepatients with essential hypertension. Kidney Int 1982;21:317-378
12. Koolen MI, Van Brummelen P: Adrenergic activity andperipheral hemodynamics in relation to sodium sensitivity inpatients with essential hypertension. Hypertension 1984;6:820-825
13. Floras J, Jones JV, Hassan MO, Osikowska BA, Sever PS,Slight P: Failure of plasma norepinephrine to consistentlyreflect sympathetic activity in humans. Hypertension 1986;8:641-649
14. Folkow B, DiBona GF, Hjemdahl P, Thoren PH, Wallin BG:Measurement of plasma norepinephrine concentrations inhuman primary hypertension: A word of caution on theirapplicability for assessing neurogenic contributions. Hyperten-sion 1983^:399-403
15. Green HD, Kepchar JH: Control of peripheral resistance inmajor systemic vascular beds. Physiol Rev 1959;39:617-686
16. Forsyth RP: Regional blood-flow changes during 72-houravoidance schedules in the monkey. Science 1971;173:546-548
17. Brod J, Fencl V, Hejl Z, Jirka J: Circulatory changes under-lying blood pressure elevation during acute emotional stress(mental arithmetic) in nonnotensive and hypertensive sub-jects. Clin Sd 1959;18:269-279
18. Lawton WJ, Christine A, Sinkey CA, Fitz AE, Mark AL:Dietary salt produces abnormal renal vasoconstrictorresponses to upright posture in borderline hypertensive sub-jects. Hypertension 1988;ll:529-536
19. WHO workshop on methodology of hypertension: Cationicmarkers determination. Hypertension 1982;4:916-917
20. Fujita T, Ando K, Noda H, Sato Y, Yamashita N, YamashitaK: Hemodynamic and endocrine changes associated withcaptopril in diuretic-resistant hypertensive patients. Am J Med1982;73:341-347
21. Ando K, Fujita T, Ito Y, Noda H, Yamashita K; The rote ofrenal hemodynamics in the antihypertensive effects of capto-pril. Am Heart J 1986;lll:347-352
22. Fujita T, Ito Y, Noda H, Sato Y, Ando K, Kangawa K, MatsuoH: Vasodilator actions of a-human atrial natriuretic peptideand high Ca2+ effects in normal man. / Clin Invest 1987;80:832-840
23. Whitney RJ: The measurement of volume changes in humanlimbs. / Physiol 1953;121:l-27
24. Folkow B, Grimby G, Thulesius O: Adaptive structuralchanges of the vascular walls in hypertension and their rela-tion to the control of the peripheral resistance. Acta PhysiolScand 1958;44:255-272
25. Messerli FH, De Carvalho JGR, Christie B, Frohlich ED:Systemic and regional hemodynamic in low, normal and highcardiac output borderline hypertension. Circulation 1978;58:441-448
26. Sapirstein LA, Vidt DG, Mandel MJ, Hanusek G: Volumes ofdistribution and clearances of intravenously injected creati-nine in the dog. Am J Physiol 1955;181:330-336
27. Messerli FH, Nowaczynski W, Honda M, Gencst J, BoucherR, Kuchel O, Rojo-Ortega JM: Effects of angiotensin II onsteroid metabolism and hepatic blood flow in man. Ore Res1977;40:204-207
28. Wiegand BD, Ketterer SG, Rapaport E: The use of indocya-nine green for the evaluation of hepatic function and bloodflow in man. Am J Digest Dis 1960^:427-436
29. Skrabal F, Herholz H, Neumayr M, Hamberger L, Ledochow-ski M, Spore H, Hortnagl H, Schwarz S, Schonitzer D: Saltsensitivity in humans is linked to enhanced sympatheticresponsiveness and to enhanced proximal tubular reabsorp-tion. Hypertension 1984;6:152-158
30. Weinberger MH, Luft FC, Grim CE, Fineberg NS: Definitionsand characteristics of sodium sensitivity and blood pressureresistance. Hypertension 1986;8(suppl II):II-127-II-134
31. Coleman TG, Granger HJ, Guyton AC: Whole-body circula-tory autoregulation and hypertension. Ore Res 1971 ;28/29(suppl II):II-76-n-87
32. Guyton AC, Coleman TG, Cowley AW, Scheel KW, ManningRD, Norman RA: Arterial pressure regulation: Overridingdominance of the kidneys in long-term regulation and inhypertension. Am J Med 1972^2:584-594
33. Liard JF: Regional blood flows in salt loading hypertension inthe dog. Am J Physiol 1981;240:H361-H367
34. Yates MS, Hiley CR: Distribution of cardiac output in dif-ferent models of hypertension in the conscious rat. PflugersArch 1979;379:219-222
35. Sullivan JM, Ratts TE: Sodium sensitivity in human subjects.Hemodynamic and humoral correlates. Hypertension 1988;11:717-723
36. Takeshita A, Imaizumi T, Ashihara T, Nakamura M: Charac-teristics of responses to salt loading and deprivation in hyper-tensive subjects. Ore Res 1982^1:457-464
37. Abboud FM, Eckberg DL, Johannsen UJ, Mark AL: Carotidand cardiopulmonary baroreceptor control of splanchnic andforearm vascular resistance during venous pooling in man. /Physiol 1979;286:173-184
38. Caldini P, Permutt S, Waddell JA, Riley RL: Effect ofepinephrine on pressure, flow, and volume relationship in thesystemic circulation of dogs. Ore Res 1974;34:606-623
39. Luft FC, Weinberger MH, Grim CE: Sodium sensitivity andresistance in nonnotensive humans. Am J Med 1982;72:726-736
40. Hollenberg NK, Moore T, Shoback D, Redgrave J, RabinoweS, Williams GH: Abnormal renal sodium handling in essentialhypertension. Relation to failure of renal and adrenal modu-lation of responses to angiotensin II. Am J Med 1986;81:412-418
41. Dustan HP, Valdes G, Bravo EL, Tarazi RC: Excessivesodium retention as a characteristic of salt-sensitive hyperten-sion. Am J Med Sci 1986;292:67-74
42. DiBona GF: Neurogenic regulation of renal tubular sodiumreabsorption. Am J Physiol 1977;233:F73-F81
by guest on June 30, 2018http://hyper.ahajournals.org/
Dow
nloaded from

244 Hypertension Vol 16, No 3, September 1990
43. Cowley AW Jr, Lohmeier TE: Changes in renal vascularsensitivity and arterial pressure associated with sodium intakeduring long-term intrarenal norepinephrine infusion in dogs.Hypertension 1979;l:549-558
44. Katholi RE, Carey RM, Ayers CR, Vaughan ED, Yancey MR,Morton CL: Production of sustained hypertension by chronicintrarenal norepinephrine infusion in conscious dogs. Cut Res1977;40(suppl I):I-18-I-26
45. Goldstein DS, McCarty R, Polinsky RJ, Kopin LI: Relation-ship between plasma norepinephrine and sympathetic neuralactivity. Hypertension 1983^:552-559
46. Brown MJ, Jenner DA, Allison DJ, Dollery CT: Variation inindividual organ release of noradrenaline measured by animproved radioenzymatic technique: Limitation of peripheral
venous measurements in the assessment of sympathetic ner-vous activity. Clin Sci 1981;61:585-590
47. Brod J: Hemodynamic basis of acute pressor reactions andhypertension. Br Heart J 1963;25:227-245
48. Brod J, Fencl V, Heji Z, Jirka J: General and regionalhemodynamic pattern underlying essential hypertension. ClinSci 1962;23:339-349
49. Koepke JP, DiBona GF: High sodium intake enhances renalnerve and antinatriuretic responses to stress in spontaneouslyhypertensive rats. Hypertension 1985;7:357-363
KEY WORDS • sodium • sympathetic nervous systemvascular resistance • blood pressure
by guest on June 30, 2018http://hyper.ahajournals.org/
Dow
nloaded from

T Fujita, K Ando and E OgataSystemic and regional hemodynamics in patients with salt-sensitive hypertension.
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 1990 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension doi: 10.1161/01.HYP.16.3.235
1990;16:235-244Hypertension.
http://hyper.ahajournals.org/content/16/3/235World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOffice. Once the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertension Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 30, 2018http://hyper.ahajournals.org/
Dow
nloaded from
![Hemodynamic and Systemic Effects of Albumin in Patients ...crease in the cardiac index from compensated cirrhosis to decompensated cirrhosis and hepatorenal syndrome [36–38]. Hemodynamic](https://img.dokumen.tips/doc/110x75/60a53321dd87fd6c8d2ff281/hemodynamic-and-systemic-effects-of-albumin-in-patients-crease-in-the-cardiac.jpg)



























