Embed Size (px)
Citation preview

R
R
St
PF
RCPp
0d
evue des Maladies Respiratoires (2011) 28, e76—e93
Disponible en ligne sur
www.sciencedirect.com
EVIEWS
wallowing disorders, pneumonia and respiratoryract infectious disease in the elderly�,��
F. Puisieuxa,∗, C. D’Andreab, P. Baconnierc,D. Bui-Dinhd, S. Castaings-Pelete, B. Crestani f,B. Desruesg, C. Ferronh, A. Franco i, J. Gaillat j,H. Guenardk, B. Housset l, C. Jeandelm, G. Jebrakf,A. Leymarie-Saddlesn, E. Orvoen-Frijao, F. Piettep,G. Pinganaudd, J.-Y. Salleq, D. Strubel r,J.-M. Vernejouxs, B. de Wazières t, S. Weil-Engereru,Intergroupe PneumoGériatrie SPLF—SFGG placé sousl’égide de la Société de pneumologie de languefrancaise (SPLF) et de la Société francaise degériatrie et gérontologie (SFGG)
a Service de gériatrie, hôpital des Bateliers, CHRU de Lille, 23, rue des Bateliers,59037 Lille cedex, Franceb Service de gérontologie, CHU de Kremlin-Bicêtre, Kremlin-Bicêtre, Francec Service de physiologie respiratoire, CHU de Grenoble, Grenoble, Franced Service SSR, centre de gériatrie Henri-Choussat, CHU de Bordeaux, Bordeaux, Francee Service de gériatrie, CMLS Lormont, CHU de Bordeaux, Bordeaux, Francef Service de pneumologie, hôpital Bichat, CHU, Paris, Franceg Service de pneumologie, centre cardiopneumologique, CHU de Rennes, Rennes, Franceh Service de médecine gériatrique, CHU de Saint-Étienne, Saint-Étienne, Francei Centre de gérontologie, CHU de Grenoble, Grenoble, Francej Service de maladies infectieuses, centre hospitalier d’Annecy, Annecy, France
Available online 22 October 2011
� Scientific committee: Louis-Jean Couderc, Bruno Crestani, Philippe Devillier, Francoise Forette, Alain Franco, Hervé Guenard,hilippe Godard, Maurice Hayot, Claude Jeandel, Élizabeth Orvoen-Frija, Francois Piette, Geneviève Pinganaud, Christophe Pison,rancois Puisieux, Benoît de Wazières.�� This article is the English translation of the following manuscript, which was originally published in French inevue des Maladies Respiratoires. Please cite this article as: ‘‘Puisieux F, D’andrea C, Baconnier P, Bui-Dinh D, Castaings-Pelet S,restani B, Desrues B, Ferron C, Franco A, Gaillat J, Guenard H, Housset B, Jeandel C, Jebrak G, Leymarie-Selles A, Orvoen-Frija E,iette F, Pinganaud G, Salle JY, Strubel D, Vernejoux JM, De Wazières B, Weil-Engerer S. Troubles de la déglutition du sujet âgé etneumopathies en 14 questions/réponses. Rev Mal Respir 2009;26:587—605’’.∗ Corresponding author.
E-mail address: [email protected] (F. Puisieux).
761-8425/$ — see front matter © 2011 Published by Elsevier Masson SAS on behalf of SPLF.oi:10.1016/j.rmr.2011.09.007

Swallowing disorders, pneumonia and respiratory tract infectious disease in the elderly e77
k EFR, hôpital du Haut-Lévêque, CHU de Bordeaux, Bordeaux, Francel Service de pneumologie-pathologies environnementales, CHI de Créteil, Créteil, Francem Centre de gérontologie clinique, CHU de Montpellier, Montpellier, Francen Service d’ORL, CHU de Grenoble, Grenoble, Franceo Service de physiologie, CHU de La Pitié-Salpêtrière, Paris, Francep Service de gérontologie, hôpital Charles-Foix, CHU, Ivry-sur-Seine, Franceq Département de médecine physique et réadaptation, CHU de Limoges, Limoges, Francer Service de gérontologie et prévention du vieillissement, CHU de Nîmes, Nîmes, Frances Service des maladies respiratoires, hôpital du Haut-Lévêque, CHU de Bordeaux, Bordeaux,Francet Service de médecine gériatrique, CHU de Nîmes, Nîmes, Franceu Unité de gériatrie aiguë, hôpital Rothschild, Paris, France
KEYWORDSSwallowing disorders;Elderly;Pneumonia;Dysphagia;Cough;Aspiration;Lower respiratorytract infectiousdisease
Summary Swallowing disorders (or dysphagia) are common in the elderly and their preva-lence is often underestimated. They may result in serious complications including dehydration,malnutrition, airway obstruction, aspiration pneumonia (infectious process) or pneumonitis(chemical injury caused by the inhalation of sterile gastric contents). Moreover the repercus-sions of dysphagia are not only physical but also emotional and social, leading to depression,altered quality of life, and social isolation. While some changes in swallowing may be a naturalresult of aging, dysphagia in the elderly is mainly due to central nervous system diseases such asstroke, parkinsonism, dementia, medications, local oral and oesophageal factors. To be effec-tive, management requires a multidisciplinary team approach and a careful assessment of thepatient’s oropharyngeal anatomy and physiology, medical and nutritional status, cognition, lan-guage and behaviour. Clinical evaluation can be completed by a videofluoroscopic study whichenables observation of bolus movement and movements of the oral cavity, pharynx and larynxthroughout the swallow. The treatment depends on the underlying cause, extent of dysphagiaand prognosis. Various categories of treatment are available, including compensatory strate-gies (postural changes and dietary modification), direct or indirect therapy techniques (swallowmanoeuvres, medication and surgical procedures).© 2011 Published by Elsevier Masson SAS on behalf of SPLF.
tpiwoto
Qw
Ta‘sadh
C
Introduction
Eating and drinking come second in Virginia Henderson’sclassification of fundamental human needs. Eating involvesgathering people, sharing, anticipating, seeing, smelling,salivating, tasting, and more. It also involves swallowingmore than 300 times per hour during a meal. Eating is anecessity for all, a pleasure for many, a sin for some; it isalso a danger for others.
The term ‘‘swallowing disorders’’ includes various typesof disorders varying in severity; some without clinical con-sequences, and others that can cause aspiration, lowerrespiratory tract infections, and malnutrition. The maindiseases that cause swallowing disorders show a markedincrease in incidence and prevalence with age.
Method
This collaborative study was produced by a multidisciplinaryworking group formed as a joint initiative of the Sociétéfrancaise de gériatrie et gérontologie (French Society ofGeriatrics and Geronology) and the Société francaise de
pneumologie (French Society of Pneumology). This groupmet on 9 and 10 December 2006. Logistical support wasprovided by GSK laboratories, and scientific secretariat byConcept Santé.Mb(
After a literature review, the group concentrated onhe writing of this document to inform geriatricians, chesthysicians, primary care physicians, and other professionalsnvolved. For this reason, a question and answer structureas chosen. This study was destined to be published in thefficial reviews of both societies. It has a two-part structure:he first on swallowing disorders in the elderly, and the sec-nd on acute, subacute and chronic complications.
uestion 1: How does swallowing changeith age?
he various structures and functions of the oropharyngealrea do not escape the aging process. The concept of‘presbyphagia’’ in the elderly can be defined as a generallowing of the process of swallowing, affecting both the oralnd pharyngeal phases. In the absence of co-morbid con-itions, these changes take place slowly and are not veryandicapping, even at a very advanced age [1,2].
hanges in the oral phase
asticatory function is generally preserved in the elderly,ut there are dental and neuromuscular changes [3,4]Table 1).

e78 F. Puisieux et al.
Table 1 Presbyphagia: alterations in the oral phase.
Diminished strength of the masticatory andtongue muscles
Difficulties in preparing the bolus (oralpreparation time)
Diminished anteroposterior tonguemovement
Diminished strength of bolus propulsiontowards the pharynx
Functional deterioration of the dentalapparatus
Failure of soft palate elevation to close theposterior oral cavity; leakage of food in thepharynxDiminished saliva secretion
fft
C
Ant
gWnih
C
Tom(tHc[
tihtaera
bp
ri
Qs
Abof[l
qiaps6sd
mt
The voluntary nature of the oral phase should not beorgotten. This enables conscious patients to compensateor these difficulties by choosing foods with the appropriateexture and increasing chewing time.
hanges in the pharyngeal phase
ging of the pharyngeal muscles disrupts both the mecha-isms of bolus propulsion and upper airway protection, againhrough various closely linked mechanisms [5,6] (Table 2).
In practice, because of its reflex nature, the pharyn-eal phase of swallowing remains the most preoccupying.hen swallowing disorders occur at this level, patients can-
ot establish compensatory mechanisms on their own. Thenfectious complications that may arise make them appre-ensive about eating and can result in malnutrition.
hanges in the oesophageal phase
he most frequently encountered abnormalities of theesophageal phase in the elderly are: interruption of pri-ary peristalsis, bolus retention in the proximal oesophagus
possibly related to lack of upper oesophageal sphinc-er compliance), and more frequent tertiary contractions.owever, they are asymptomatic or do not show anyorrelation with the symptoms presented by patients7—9].
In all, even though the elderly swallow more slowlyhan young adults, the safety of oropharyngeal swallow-ng is not compromised simply because of age. Studiesave demonstrated that there is no significant increase inhe risk of aspiration in the elderly compared with youngdults, in the absence of associated disorders. However, thelderly are more likely to develop dysphagia during neu-ological or upper aerodigestive tract diseases than young
dults.Studies have shown that the cough reflex is not affectedy age. Katsumata et al. measured in 110 healthy peo-le aged 20 to 78 years the threshold of inhaled citric acid
ibpl
Table 2 Presbyphagia/Changes in the pharyngeal phase.
Delayed triggering of the pharyngealswallowing reflex
Failure of laryngeal elevation
Diminished strength of pharyngeal contractionFailure of upper oesophageal sphincter opening
equired to trigger a cough reflex and did not find a decreasen threshold with age [10].
• Thus, all these data suggest that age itself does notsignificantly increase the risk of aspiration. However,the incidence and prevalence of the main diseasesresponsible for deterioration in swallowing greatlyincrease with age.
uestion 2: What is the prevalence ofwallowing disorders?
study published in 1990 in the British Medical Journal [11],ased on questionnaires completed by 136 subjects agedver 87 on symptoms suggestive of swallowing disorders,ound that 16% reported dysphagia. Similarly, Kawashima12], using a questionnaire administered to 1313 subjectsiving at home and aged over 65, found dysphagia in 13.8%.
In 2002, Lin published the results of a study associating auestionnaire, a neurological examination, and a swallow-ng test. Of the 1221 subjects included in the study, with anverage age of 77 ± 10 years, 32% of those on a normal dietresented swallowing disorders [13]. Ekberg evaluated 56ubjects with a mean age of 83; the imaging studies showed3% had problems in the oral phase of swallowing, 25% pre-ented pharyngeal dysfunction, and 36% oesophageal motorysfunction [14].
Compared with young subjects, the 53 patients with aean age of 76 studied by Nilsson showed poorer results for
he Repetitive Oral Suction Swallow test [15]. Finally, it is
nteresting to note that, even in patients who are elderlyut have retained at least 20 teeth, oral transit time andharyngeal transit time assessed with a barium swallow wereonger compared with young subjects [16].Increased length of pharyngeal swallowingtimeFood stasis in the epiglottic vallecula and/orpyriform sinusesFood dropping into the larynx/aspiration

tiou
v7oti
M
Mocrwd
O
Do[
L
Chaa
tptoraot[
Qd
Aptccdgcaa
tcva
Swallowing disorders, pneumonia and respiratory tract infec
The prevalence of dysphagia is estimated at between 8and 15% in patients living at home, and 30 to 40% in patientsliving in institutions.
One consequence is an increased risk of malnutrition asshown in the study by Suominen [17].
Question 3: What are the main disordersresponsible for swallowing disorders in theelderly?
Cerebrovascular disease and degenerative neurological dis-eases are the main causes of dysphagia in the elderly.
Neurological disorders
Regardless of age or localization, the incidence of dyspha-gia ‘‘after a stroke’’ is high but variable depending on thestudy and the investigations chosen. Incidence is low whenbased on history taking or a basic physical examination (37to 45%), higher using a clinical examination or tests con-ducted by experienced practitioners (51 to 55%), and higherstill using instrumental techniques (64 to 68%) [18,19]. Overtwo thirds of patients hospitalized after a stroke are over65, making this disorder a major cause of swallowing dis-orders in the elderly [20]. Even though dysphagia improvesin the majority of patients after a stroke, 10 to 30% showpersistence of swallowing difficulties. The systematic searchfor swallowing disorders in acute stroke has a socioeco-nomic impact. The detection of swallowing disorders andtheir management can reduce the incidence of pneumonia(from 6.7% to 0% in a population of 123 patients 2 yearsafter the introduction of a systematic search for aspiration inacute stroke) [21]. Respiratory complications were respon-sible for an average extension of stay in acute care unitsof 7.8 days [22] and an increase in the average burden ofcare.
‘‘In Parkinson disease’’, swallowing disorders fluctuate,but can already be present in the early stages of the disease[23,24]. All the phases of swallowing are involved [23,24].Feeding difficulties in patients with Parkinson disease arealso caused by chewing difficulties, head posture in flexion,motor disorders of the upper limbs, and possible associatedcognitive disorders [23,24].
Swallowing disorders are practically constant occur-rences ‘‘in the progression of dementias’’, be theydegenerative or vascular, but are underestimated and oftenignored [25,26]. All the phases of swallowing are affected,but anomalies of the oral phase are predominant. Strictlyspeaking, swallowing disorders cause problems less oftenthan eating disorders (absence of swallow or forgettingto swallow, difficulties with fluid intake, archaic suck-ing reflexes, etc.). The consequences of food provided bythird parties are also an issue (inadequate volume, accu-mulation of food in the mouth, eating too fast, etc.)[27—29]. Sedative treatments can worsen the difficul-
ties.‘‘Charcot-Marie-Tooth disease’’, lacunar stroke, and pro-gressive supranuclear palsy are other neurological causesmore rarely encountered.
d
c
s disease in the elderly e79
‘‘In geriatric institutions, studies have demonstrated aery high frequency of swallowing disorders affecting 50 to5% of the residents’’. This reflects the very high prevalencef cerebrovascular and neurodegenerative diseases and con-ributes to the very high incidence of lower respiratory tractnfections in this population [30,31].
uscular disorders
any muscle diseases are likely to result in swallowing dis-rders due to involvement of the pharyngolaryngeal andervical oesophageal striated muscles. Their prevalenceemains difficult to assess, and is often underestimatedhen the objective signs are compared with the functionalisorders described by patients [32,33].
ther disorders
iabetes [34,35], malnutrition [20], and dehydration are endf life situations often accompanied by swallowing disorders36].
ocal causes
ertain local causes can give rise to swallowing disorders:ead and neck cancer, Zenker diverticulum, oesophagealchalasia, cervical osteophytes, and oropharyngeal candidi-sis [20].
In addition to surgical or radiotherapy treatment, par-icular attention must be paid to dysphagia caused by theresence of endoluminal devices in the upper aerodigestiveract. A nasogastric tube prevents direct inhalation of foodr fluids, but not inhalation of saliva that presents a higherisk of colonization by pathogenic bacteria, because of thebsence of oral feeding. It also contributes to incompetencef the upper and lower oesophageal sphincters, and thushe occurrence of reflux and aspiration of gastric contents20].
uestion 4: Can drugs cause swallowingisorders?
ll drugs likely to induce dryness of the mouth or impairedroduction of saliva can cause dysphagia [20,37,38]. This isrue of all anticholinergic treatments: antihistamines, tri-yclic antidepressants, neuroleptics, anti-emetics, agentsontaining atropine, antidiarrheal drugs, antiparkinsonianrugs, and also diuretics. Many inhaled drugs (ENT decon-estants, vasoconstrictors, anticholinergics, asthma drugs,orticosteroids, mucolytics or mucous thinning agents) canlso cause mouth dryness, cough or oropharyngeal candidi-sis.
Moreover, many drugs that alter or depress the cen-ral nervous system and the level of alertness canause dysphagia in the elderly: benzodiazepines, anticon-ulsants, antipsychotics, opiates, antihistamines, certainnti-emetics, and lithium [37,38].
Neuroleptics can cause dysphagia through extrapyrami-al side effects or orofacial dyskinesia.
Finally, some drugs prescribed for the elderly canause dysphagia oesophageal in origin, either by decreasing

e
pgca(sa
Qsc
S••
•
et
mdnv
sd
adr
c
Qo
Cc
app
P
TiniioaoFtt
C
I
ctop
a•
•
C
80
ressure at the lower esophageal sphincter, resulting inastro-oesophageal reflux (theophylline, nitrates, calciumhannel blockers, benzodiazepines), or by direct dam-ge to oesophageal mucosa, resulting in oesophagitisnon-steroidal anti-inflammatory drugs, prednisone, bispho-phonates, and some minerals such as potassium chloridend iron sulfate) [37,38].
uestion 5: Under what circumstanceshould a swallowing disorder beonsidered?
wallowing disorder should be considered in case of:‘‘acute aspiration’’ that is clinically obvious;‘‘symptoms immediately suggestive of a swallowing dis-order’’:◦ discomfort/difficulties swallowing,◦ food leakage from the mouth,◦ nasal reflux,◦ food blockage,◦ voice changes (gurgly/wet);‘‘symptoms often misinterpreted’’:◦ drooling, food residue in the mouth,◦ reduction in food intake going as far as complete
refusal, especially in a group setting,◦ food kept in the mouth for long periods and extended
duration of meals,◦ throat clearing/hawking,◦ weight loss with repercussions on general health,◦ recurrent pneumonia,◦ unexplained febrile episodes.
When a carer notes difficulties with food intake in anlderly person, this information must be communicated tohe prescribing physician.
Nursing aides are often the staff the most present duringealtimes, and should be able to identify and report: imme-iate or delayed cough (BUT, the absence of cough does notecessarily mean the absence of aspiration!), gurgly or wetoice, and prolonged apnea.
One or more of these symptoms are the first presentingigns that should raise the question of possible swallowingisorders.
Associated symptoms identified by carers that shouldlso suggest swallowing disorders are: recurrent fever spikesistant from meals, hyperthermia of unknown cause, respi-atory tract infections, etc.
These warning signs should initiate an assessment proto-ol in search of a swallowing disorder.
uestion 6: What does clinical assessmentf swallowing disorders involve?
linical assessment of swallowing disorders can be artifi-ially divided into two major stages.
The first stage is thorough history taking with the patientnd/or carers; the second stage is examination of the threehases of swallowing: preparatory phase, oral phase andharyngeal phase.
Tbw
F. Puisieux et al.
atient interview
his is an essential element in the diagnosis of swallow-ng disorders. It is carried out in close collaboration withatural helpers, home carers and/or the nursing team. Itdentifies the difficulties encountered with food or fluidntake, specifies the frequency and circumstances of onsetf the disorders, reveals spontaneous compensatory mech-nisms, assesses comprehension, memory, judgement, andral communication skills, and the alertness of the patient.inally, it enables patients and carers to express their expec-ations and priorities in terms of diet in order to propose areatment plan appropriate for their environment.
linical examination
t explores the different phases of swallowing.Examination of the preparatory phase assesses defi-
iencies, neurosensory abilities and disabilities in gripping,ransporting food to the mouth, putting food in the mouth,lfactory, visual and auditory sensitivity, and trunk and headosture.
Afterwards, evaluation of swallowing times providesnalysis of the oral and pharyngeal phases.The examination is first performed without food intake.
In the facial, oral and lingual areas, it evaluates tactile,gustative, thermal and proprioceptive sensitivity in theentire region, as well as motor amplitudes, strength andcoordination. This is followed by analysis of performanceof the various actions. The pharyngeal region is less acces-sible. As the pharyngeal swallowing reflex involves motorand sensory tracts it is examined using sound emission,and observation of the soft palate and posterior wall atrest, and during muscle contractions (tactile stimulation).The presence of abnormal reflexes such as the suck-ing, palm-chin, and biting reflexes, indicate neurologicaldisorders that can have direct repercussions on the effec-tiveness of swallowing. Particular attention should be paidto the assessment of saliva production and oro-dentalcondition. Analysis of the number and quality of sponta-neous and then volitional swallows of saliva is related tothe preceding elements for a first functional assessmentof swallowing.The examination is continued using trials with liquids andsolids.
It enables definition of the texture, maximum volume ofbolus per swallow, taste, temperature, and posture moreconducive to effective swallowing when that is possible.
Tests are also performed using flavoured (syrup),sparkling, or iced water to facilitate triggering of theswallowing reflex with more intense afferent sensoryinput. On this occasion, basic taste, thermal and proprio-ceptive sensitivities undergo functional testing with foodsthat are sweet, savoury, acid, hot, cold, etc.
linical tests without food reintroduction tests
hese use clinical scales predictive of the risk of aspiration,ased solely on the physical examination. The signs usedere retained because of their correlation with the presence

tious disease in the elderly e81
Table 3 Clinical scale predictive of risk of aspiration.
Clinical variables Rating Score
Absence of archaic reflexes 12Presence of velar reflex 8Volitional swallow possible 7Absence of dysphonia 6Presence of gag reflex 6Laryngeal blocking possible 3TOTAL (predictive clinical score)
Clinicalpredictive score
Diagnosis Management
Total < 14 Aspiration + CompletephysicalexaminationAppropriatetreatmentstrategy
14 < total < 28 Aspiration ? Videofluoroscopy toconfirm diagnosis
Total > 28 Aspiration − Simple surveillance
Suspected aspiration or population at risk — Diagnosis ofimpaired swallowing using a clinical score predictive of
ppiaduul(
dema(t
Qi
Fcra
o[
Swallowing disorders, pneumonia and respiratory tract infec
of aspiration on the videofluoroscopic examination, the cur-rent reference technique in detection of aspiration [39].
Guinvarc’h et al. have proposed a clinical scale predic-tive of aspiration [40]. It explores six clinical signs: velar andgag reflexes, archaic reflexes, laryngeal blocking, volitionalswallow, and voice (dysphonia). Thus, application of the pre-dictive score for aspiration provides a practical approachbased on the decision tree proposed (Table 3).
This scale was applied to a validation population of 105patients. Among these patients, the scale was informativein 69.5% of cases (73/105). Sensitivity was low at 58.3%;specificity was 80.7%.
Food reintroduction tests
Various food reintroduction tests have been proposed. Theirinterpretation can be qualitative: the principle behind the‘‘3-oz water swallow test’’ [41], the most often performed.This test requires the drinking without interruption of 90 mLof water. The test is suggestive of aspiration if patientscough in the minute following drinking or if their voicebecomes gurgling, wet or hoarse. Study of its correspon-dence with videofluoroscopy attributed a sensitivity of 76%to the ‘‘3-oz test’’. This rose to 94% if only the aspirationof over 10% of the volume of fluid ingested on videofluo-roscopy was counted, and 94% for aspiration of solids onvideofluoroscopy. Apparently only four of the 44 patientstested by DePippo presented aspiration with abolition ofthe cough reflex, which for the author justified the use offood reintroduction tests alone [41]. Specificity was 59%.Gottlieb [42] validated the use of a reduced volume of50 mL.
The ‘‘water test’’, adapted by Mr Guatterie in Bordeaux,consists in the successive drinking of four spoons (2 mL) ofstill water, with an increase in the volume each time (4 mL,8 mL, 50 mL), if there is no aspiration, up to drinking of aglass of water. It can be performed by a previously trainednurse [43—46].
The ‘‘Timed test of swallowing capacity’’ [47] is a quan-titative test to explore swallowing. It involves measuring thetime of ingestion of 150 mL of cold water (from contact withthe lips to the last laryngeal elevation). If total intake is notpossible, onset of a cough or a change in voice is taken intoaccount. Temperature, flavour, and repetition of the test donot affect the rate of ingestion. The pathological thresholdfor speed is 10 mL/s (this result is valid only for subjectsaged under 70 years). However, these results have not beenconfronted with videofluoroscopic studies of aspiration.
Mixed tests
The association of suspicious signs and/or symptoms andfood reintroduction tests is an interesting strategy usedin the ‘‘Burke Dysphagia Screening Test’’ [48]. This testis positive, indicating aspiration, if one or more of thefollowing criteria are verified: (1) bilateral stroke, (2) brain-stem stroke, (3) acute pneumonia, (4) positive ‘‘3-oz Water
Swallow Test’’, (5) eating less than half of a meal (forthree consecutive meals), (6) prolonged food intake (greaterthan 30 minutes), (7) non-oral feeding. This test identifies92% of patients with complications secondary to aspiration:V
Tr
aspiration.
neumonia, aspiration syndrome or death (11 of the 12atients with complications of the 139 patients with stroken DePippo’s article [48]). Daniels [49] proposed a similarpproach and explored six clinical indicators: dysphonia,ysarthria, velar and gag reflex abnormalities, weak vol-ntary cough or cough impossible after food intake (testssing 5, 10 and 20 mL) and voice modifications after a swal-owing test. Sensitivity was 92.3%, and specificity 66.7%Table 3).
Swallowing tests are a simple method of systematicetection among populations at risk of aspiration thatnable rapid implementation of appropriate therapeuticeasures (postural and dietary modifications). Mixed tests
re the most interesting, associating sufficient sensitivity58.3 to 94%) and specificity (59 to 80.7%) for a diagnosticest.
uestion 7: What can furthernvestigations contribute?
urther investigations are particularly indicated when thelinical assessment is not contributive. They will confirm orule out the disorder, specify the mechanism and validatedaptations for alleviation.
The following explorations can be considered: videoflu-roscopy, endoscopy, and pharyngoesophageal manometry50—52].
ideofluoroscopy
his is mainly interesting for the dynamic examination ineal time of the act of swallowing: ‘‘live’’ observation of the

e
da
•
•
•
tf
ETdbpevl
PW•••
tolwnp
t•
•••
•
tps
TT•
•
RTa1fc
t
E
Pstc
rcro
ad
P
Isd
arat
vod
nr
Qm
A
‘p
82
ifferent phases of swallowing: oral (volitional), pharyngealnd oesophageal (reflexes).
This investigation can explore the three aspects:mobility of the structures involved, approach to the phys-iology of the patient during food intake;mouth muscle tone (chewing), velopharyngeal sphinc-ter, pharyngeal peristalsis enabling opening of the upperesophageal sphincter, etc.;hypopharyngeal sensitivity activating the cough reflex,beneficial in the case of aspiration.
Analysis of the results, in addition to clinical observa-ions, help in the choice of the most appropriate treatmentor the patient.
xamination conditionshe examination is rapid and non-invasive; the patientoes not need to be fasting. Two prerequisites muste met: patient alertness, and standing or sitting beingossible. Suction equipment should be on hand. Thexamination is performed in the fluoroscopy lab, withideo recording, transferred to DVD, for detailed reviewater.
rotocole advise ingestion of:three mouthfuls of Micropaque HD® alone;three mouthfuls of diluted product;three mouthfuls of an opacified solid.
The textures ingested are, of course, adjusted accordingo previous clinical observations. The choice of the numberf mouthfuls to identify a difficulty with initiating swal-owing (frontal disorder) or, conversely, increasing difficultyith aspiration at the last mouthful (early ALS). The exami-ation is interrupted in the case of massive aspiration of theroduct (over 50%).
The examination is first performed in lateral projection,o make the following observations:
documentation of aspiration, observation and localizationof stasis (valleculae, pyriform sinuses);mobility and muscle tone of the tongue and tongue base;epiglottic tilt;laryngeal elevation (N = 1.5 vertebrae), with anterior tilt,and simultaneous advancement of the hyoid bone (N = 50%of jaw length);opening of the upper oesophageal sphincter.
The examination is then performed in anterior projec-ion, for identification of pharyngolaryngeal asymmetry,articularly during emptying of the valleculae and pyriforminuses (unilateral laryngeal paralysis).
The DVD recording enables detailed analysis later.
he examinationhe examination can:
confirm whether or not further examinations are required(for example, no need for manometry or endoscopy if adisorder of the voluntary phase is involved);enable treatment choices:c
ap
F. Puisieux et al.
◦ rehabilitation if the disorder involves the voluntaryphase,
◦ adjustment of food textures,◦ possible surgical procedures: gastrostomy if the dis-
order involves the reflex phases, myotomy, botulinumtoxin (limit of the upper oesophageal sphincter).
estrictions and contraindicationshe restrictions concern the patient’s condition: alertness,nd also ability to remain standing or sitting for around5 minutes. Moreover, the patient must understand andollow the instructions given, and not present any majorognitive or psychiatric disorders.
The contraindications are lower respiratory tract infec-ion and previous certainty of massive aspiration.
ndoscopic examination of swallowing
erformed by an ENT specialist, using a flexible endo-cope and a light source, it provides direct vision ofhe velopharyngeal sphincter, hypopharynx and glottallosure.
This invasive examination requires the cooperation of aelaxed patient; it can be considered when videofluoroscopyannot be performed, due to inability of the patient toemain standing or sitting, or when there is a major riskf aspiration.
This examination does not assess the oral voluntary phasend only provides a partial view because of loss of lightinguring epiglottic tilt and glottic closure.
haryngo-oesophageal manometry
t records changes in pressure in the pharynx during pas-age of the bolus, with a nasal tube, and sensors placed atifferent levels of the pharynx.
It measures the effectiveness of pharyngeal peristalsisnd upper oesophageal sphincter tone in the phases ofelaxation (opening of the upper oesophageal sphincter)nd contraction (closure of the upper oesophageal sphinc-er).
This examination is also invasive, and is justified whenideofluoroscopy shows impaired opening of the upperesophageal sphincter (possible cricopharyngeal relaxationisorder).
It does not identify pharyngeal abnormalities and doesot provide precise indications concerning the origin of aspi-ation.
uestion 8: What are the mainechanisms of aspiration [43]?
spiration before swallowing
‘Due to absence of the swallowing reflex’’. In this case, noosture changes to facilitate swallowing or texture changes
an activate this reflex.Possible causes: surgery involving the epiglottisnd extending widely to the base of the tongue,ost-radiotherapy sensory lesions to the base of the

tiou
Ts
Tp•
•
•
ppw
R
Rwo
rsa
ttd
a
im
R
Titib
asoe
P
Swallowing disorders, pneumonia and respiratory tract infec
tongue, reconstructive laryngectomy, muscle damageas in some myopathies and in systemic scleroderma,bilateral impairment of the IX-X-XI nerve pairs,etc.
‘‘Due to delayed triggering of the swallowing reflex’’.In this case, aspiration very often involves water; simplethickening can make the disorders disappear by slowing pro-gression of the bolus in the pharynx.
Possible causes: damage to corticobulbar pathways thatno longer control activation of the swallowing reflex, phys-iological aging, etc.
Aspiration during swallowing
The protective structures of the larynx are deficient. Turn-ing the head toward the lesion enables swallowing on theopposite side to the rotation and can eliminate aspira-tion.
Possible causes: subtotal laryngectomy, vagus nerveparalysis.
Aspiration after swallowing
This kind of aspiration occurs when there is overflow duringpharyngeal stasis in the airways due to incompetent pharyn-geal propulsion and/or relaxation of the upper oesophagealsphincter.
Possible causes: pharyngeal paralysis or paresis, in somesubtotal laryngectomies, physiological aging, etc.
NB: This distinction is somewhat artificial as aspiration inboth phases can have the same cause.
Extralaryngeal aspiration
Possible causes: tracheostomy cannula due to tracheo-oesophageal fistula.
Question 9: How are swallowing disordersmanaged?
Management must have as its priority: maintaining the plea-sure in eating and drinking, while guaranteeing a vitalnecessity [53—57].
Teamwork
This is necessarily a coordinated effort involving allactors in the health system: health care profession-als including physicians, nurses, nursing aides, dietitians,rehabilitation staff (physiotherapists, speech therapists,occupational therapists, psychomotricians) with the objec-tive of adaptation or rehabilitation. The speech therapisttransforms rehabilitation into an environmental situation(everyday life), but the French decrees authorize par-ticipation of the various members of the paramedicalteam.
It is also essential to involve family members, who canprovide significant assistance, particularly concerning thepsychological and emotional investment of the elderly per-son in meals.
Fcf
s disease in the elderly e83
he installation of a patient who haswallowing disorders
he nursing staff plays a vital role from the time of mealreparation. The risk of aspiration can be reduced by:positioning the patient, sitting well upright, or half-sittingif necessary but with the head properly held up, possi-bly in anterior flexion to protect the upper airways andfacilitate opening of the upper oesophageal sphincter;arranging of the patient’s environment, with eliminationof any distractions or disruptions that could result in aspi-ration;using appropriate equipment, depending on the possiblemotor difficulties of the patient. The assessment by theoccupational therapist will enable introduction of appro-priate technical aids (cutlery with large handles, plateswith rims, glasses with a cut out section for the nose,non-skid table mats, etc.) and rehabilitation of fine move-ments.
Observation of how the objects required for eating arelaced is necessary to facilitate meal taking. Sometimes justlacing a fork too far away on the table can tire the patientho will eat less and less.
eintroduction of food intake
eintroduction of food intake is accomplishing again, andith success, the functions of chewing and swallowing, with-ut aspiration.
The decision to resume food intake or adapt food textureequires a medical prescription based on the results of thewallowing assessment, and in consultation with the nursingnd rehabilitation teams.
There are four successive stages: stage 1, ‘‘smooth’’ tex-ure; step 2, ‘‘semi-liquid’’ texture; step 3, ‘‘soft/minced’’exture; step 4, ‘‘normal’’ texture. The four steps areetailed in Tables 4—7.
The transition from one stage to another is decidedccording to well-codified criteria.
At each stage, a nasopharyngeal suction system in work-ng order must be installed in the patient’s room, in caseassive aspiration occurs.
ehabilitation
he role of the physiotherapist or speech therapist presentn the structure is that of patient rehabilitation, informa-ion and education, with their own tools; they also act asntermediaries between the patient and the nursing team,y providing practical information in a real-life situation.
The therapist must teach the nursing staff the functionalspects of swallowing; the nurses and nursing aides are thetaff the most often present on a daily basis; quality care isnly possible with the complementary skills of these differ-nt carers.
alliative strategies
aced with a progressive disease, in particular neurologi-al, for which no specific therapy is available, adaptation ofood textures is done regularly depending on the worsening

e84 F. Puisieux et al.
Table 4 ‘‘Smooth’’ texture stage.
STAGE 1: ‘‘Smooth’’ texture
Jelly (water + gelatine)High-protein creamsFromage blancStewed fruit
This smooth texture with pieces or residue helps the food to slide easily to the stomachDisobstruction is easier with the suction deviceRemaining attentive to the reactions of the patient is essential. Note
Patient behaviour (sweats, cyanosis, pleasure/displeasure, tension/relaxation, etc.)Observance of the protocolWhether swallowing was easy or notCoughing during or after oral feedingRespiration function in the hours following the meal
Be careful of silent aspiration; coughing during a meal indicates aspiration; but, conversely, absence of coughingdoes not necessarily mean the bolus was swallowed correctly. Any doubts concerning silent aspiration requirepulmonary auscultationThe test may also trigger anxiety attacks because of memories of a previous episode of aspirationThe explanations and technical advice should be repeated and rephrased as often as necessary. If anxietyremains unmanageable with a risk of failure of food reintroduction, psychological support could be proposed
The following questions should be asked concerning the patientDid this test seem to be pleasant for the patient?Was the food bolus swallowed easily?Did the patient participate in the rehabilitation process?Was the patient stimulated by the reintroduction of food?Was the patient relaxed?
If progression of the bolus is satisfactory, and does not trigger the cough reflex, a feeling of discomfort orchoking, other tests may be performed, still with smooth textures, until the technique of swallowing is perfectlymastered
The next step will depend on the results of this learning process and the complete absence of aspiration
oTetbidovra
Qcd
A
T•
•
f the condition, following a multidisciplinary approach.his situation is frequent in institutions. The question ofnteral or parenteral feeding may arise at a given time ifhe risk of aspiration and repeated infectious complicationsecomes major. Percutaneous endoscopic gastrostomy (PEG)s currently recommended in Charcot disease, as soon asysphagia is frequent, considering the progressive naturef this disease and the improvement in quality of life pro-ided by PEG. In severe dementia, however, PEG is notecommended. However, each situation requires individualnalysis in its context.
uestion 10: What are the acute andhronic complications of swallowingisorders?
cute manifestations
here are three major clinical pictures:‘‘an obvious picture of tracheobronchial aspiration of aforeign body’’, usually food. The symptoms are typical.They depend however on the volume of aspiration, going
from classical penetration syndrome, well described bythe patient or a witness, associated with attacks of suffo-cation, cough, dyspnoea, and desaturation, to a rarer andrapidly fatal picture of asphyxia, paradoxically underdiag-nosed in acute situations. An autopsy study conducted inVienna between 1984 and 2001 on 200 cases of asphyxiaby aspiration of foreign bodies showed that althoughthe episode occurred in 68% of cases in the presenceof a witness, before death, the correct diagnosis hadonly been suggested in 5% of cases in patients over 65(105/200). This study identified risk factors for massivefood aspiration, namely an underlying neurological dis-ease (Parkinson disease, Alzheimer disease, and stroke),taking sedatives (all the elderly patients who died in themorning had been given a sedative treatment the eveningbefore), a semi-solid diet (mashed vegetables, mincedmeat, fruit jam), and poor dental status (35% of thoseover 65 were edentulous) [58];‘‘a picture of gastric content aspiration producing clas-sic Mendelson syndrome’’ (aspiration pneumonitis). This is
defined as chemical pneumonitis, secondary to the aspira-tion of regurgitated sterile acid gastric fluid that, at leastinitially, is not infectious. However, it has been shownthat gastric fluid can be colonized by SStaphylococcus
Swallowing disorders, pneumonia and respiratory tract infectious disease in the elderly e85
Table 5 ‘‘Semi-liquid’’ texture stage.
STAGE 2: ‘‘Semi-liquid’’ texture
A semi-liquid texture enables the introduction of more granular textures. It also enables assessment of meal durationand patient fatiguability as the composition is the same as a normal meal
Minced meatPuréed/mashed vegetablesDesserts (stewed fruit, yoghurt, fromage blanc, etc.)
These meals are only taken at lunchtime as they are part of the rehabilitation process. The speech therapistresponsible for reintroduction of oral nourishment must do so in the presence of the nursing staff. This is anindispensable part of their training. The speech therapist notes his/her interventions on the specific report card in themedical record, indicating it is a rehabilitation session. At all the stages of this rehabilitation process, the nursing andrehabilitation teams write up their interventions on a common report cardThe dietitian contributes by determining the preferences of the patient, and the possibilities for daily meals. Thedietitian can also limit the choices of foods depending on the indications provided by the speech therapist orphysiotherapist: referred to as a personalized dietThe physician informs the team of the absence of any intercurrent medical conditions
Liquids are reintroduced gradually observing the following successive stagesCoca Cola® type sodas strong in taste and that trigger considerable sensory impulsesCool sparkling waterCool flavoured still waterCool unflavoured still waterUnflavoured still water at room temperature
If the reintroduction of oral liquids is impossible, hydration will be through an enteral feeding tube, or with jelly(water + gelatine) that has the advantage of being smooth, melting in the mouth, and having pleasant flavours.Approximately 15 pots of jelly are required to provide satisfactory hydration (a pot of jelly corresponds to a 100 mLglass)
Progress to the next stage is decided on the same criteria as for the ‘‘smooth’’ texture stageNo discomfort after oral nourishmentNo coughNo bronchial obstruction during and after eatingA pleasurable experienceObservance of the protocolAbsence of anxiety
If the patient has the motor capacity to feed him/herself, this will be one of the aims of rehabilitation. The pleasureof being able to bring food to the mouth oneself is part of patient autonomy. A feeling of frustration can emerge whenthis is not possible because of an associated physical handicapAwaiting full recovery of autonomy at meals, the assistance provided by the nursing team should pay attention to the
ppor
•
patient’s pace of progress, and be both stimulating and su
aureus or enterobacteria as pH is increased by antacidtreatments and with enteral feeding [59]. The occurrenceof chemical pneumonitis usually implies the presence ofconsciousness disorders (epilepsy, stroke). Acidity playsa key role. Experimental studies in animals have shownthat pH must be below 2.5 and volume greater than0.3 mL/kg for lung lesions to develop (chemical burn ofthe bronchial tree and inflammatory reaction of lungparenchyma). Diagnosis is not a problem when aspira-tion takes place in the presence of a witness. The picturecan very quickly become dramatic and associates polyp-noea, cough, cyanosis, pulmonary oedema, hypotensionand hypoxaemia with rapid progression to respiratory dis-tress syndrome (ARDS); Mendelson syndrome representsapproximately 10% of the causes of ARDS [60]. According
to Mylotte [61,62], chemical pneumonitis is more commonthan aspiration pneumonia, which should have an impacton treatment management, particularly by limiting theuse of antibiotics, as with a non-infectious process thetive, to supply sufficient food intake
symptoms can rapidly improve with symptomatic treat-ment;‘‘a picture of lower respiratory tract infection, oftenrecurrent’’, involving one or more events suggestiveof lower respiratory tract infection, including cough,pleural type pain, fever over 38.5 ◦C, purulent spu-tum, respiratory rate equal to or over 25 per minute,signs of localization on the physical examination (crack-les or bronchial rales) and radiological appearanceconsistent with the picture. Even though these acutesymptoms may seem unremarkable, this is the most fre-quent clinical presentation and the most difficult tounderstand, firstly because the symptoms of lower res-piratory tract infection can be atypical in the elderly,sometimes raising difficult problems with differential
diagnoses such as pulmonary embolism. These diag-nostic difficulties are increased by interrelationshipswith the patient’s constitution, whether a question ofchronic obstructive pulmonary disease or heart failure.
e86 F. Puisieux et al.
Table 6 ‘‘Soft/minced’’ texture stage.
STAGE 3: ‘‘Soft/minced’’ texture
Starter: ‘‘protein supplements’’ such as sardines, eggs, sausage, cheese pancakes, tomatoes, etc.Minced meatWhole vegetables and/or starchy foodsDairy products and/or cheeseCooked and/or stewed fruit
This type of diet requires great care. It contains foods that are often a risk for a patient still fragile concerningswallowingThe foods presenting risks are
Raw vegetablesRaw fruitRice, semolina, etc.
Raw vegetables such as grated carrots and corn, or raw fruit, must be chewed. In a patient lacking effectivemastication, due to paralysis for example, or when the food is not satisfactorily mixed with saliva (this is necessary forpropulsion of the food bolus), these foods are likely to ‘‘stick’’ and remain ‘‘blocked’’ in the pharyngolaryngealjunction. When the airways open, the bolus penetrates into the trachea and causes aspirationPulses and cereals, such as rice, semolina, peas, lentils, and small kidney beans, are often poorly mixed with saliva.They remain on the walls of the mouth and escape at an inopportune moment into the trachea. Care should also betaken with French beans as they can be stringy. They get stuck between the tonsillar pillars, and trigger nausea thatcan cause aspirationThe dietitian can have the kitchen prepare supplements such as lasagna, soufflés, and shepherd’s pie. Thesesupplements have the advantage of being high in protein, and have a ‘‘soft pieces’’ texture like pasta that get thepatient used to chewing again without being too tiring
Progress to the next stage follows the same criteria as for stages 1 and 2The following two parameters must also be considered
Meal timesThe ability to chew hard food, or poor dentition that can result in the exclusion of a food presenting a risk
S
Tapdacpoorc•
•
•
Qm(g(
Totrwia
Secondly, because once these differential diagnoseshave been ruled out, there is no certainty that theclinical picture can be attributed to a swallowingdisorder. Finally, because once a swallowing disorderhas been recognized, it may not be responsible forinfections.
ubacute or chronic manifestations
hese are more difficult to understand because clinical signsssociating dyspnoea and cough with expectoration can beresent in frequent and unremarkable chronic respiratoryisorders such as chronic obstructive pulmonary disease andsthma; possible underlying heart failure can add to theonfusion. The clinical picture can also be that of recurrentneumonia, recurrent unexplained fever, non-specific uni-r bilateral radiographic abnormalities, and so on. Chronicccult aspiration can thus cause specific disorders, quitearely described but often underestimated considering theontext of onset. For example:
paraffinomas secondary to repeated aspiration of liquidparaffin in chronic constipation with possible concomitantMycobacterium fortuitum infection;obliterating bronchiolitis with organizing pneumonia
(BOOP) [63], particularly if there are varying radiographicabnormalities;diffuse aspiration bronchiolitis, a relatively rare entitydescribed by Matsuse [64], occurring in elderly patientsitp
with an unremarkable clinical picture of dyspnoeawith cough, and bilateral micronodular infiltrates. Thisdisorder is characterized by the presence of foreign par-ticles and bronchiolar inflammatory infiltrates. It occurs inbedridden patients with a history of neurological disordersor dementia presenting swallowing disorders, whetheridentified or not.
uestion 11: Can a clinical distinction beade between chemical pneumonitis
inflammation related to aspiration ofastric fluid) and aspiration pneumoniainfection)? Is this distinction useful?
he importance of distinguishing the two entities is the-retically twofold: on the one hand, the prognosis is nothe same, it is better in chemical pneumonitis that oftenegresses with symptomatic treatment; on the other hand,ith aspiration of gastric fluid not causing infection, at least
nitially, there is no need to treat chemical pneumonitis withntibiotics immediately.
However, the distinction is not easy to establish becausen both cases there are signs suggestive of lower respiratoryract infection. Mylotte et al. studied this issue [61]. Theyropose some preliminary definitions:

Swallowing disorders, pneumonia and respiratory tract infectious disease in the elderly e87
Table 7 ‘‘Normal’’ texture stage.
STAGE 4: Texture: ‘‘normal’’
All types of startersMeatVegetablesCheese/dairy productsFruitBread
More time must be taken when progressing with meat texture as this is the most dangerous food. A piece of steak isnot only difficult to chew but also to pass into the esophagusThere are alternatives for meats more difficult to chew, such as
OmeletteFishMinced steak
Some patients will never progress to this texture, or only late in the process, but this should not interfere in any waywith the decision to remove an enteral feeding tube as energy requirements can be covered by the ‘‘soft/minced’’ dietThis last stage includes ‘‘resocialization’’, and concentration on the meal, with the objective of autonomy. If allowedby the structure of the institution, the patient should be taken to the dining room to observe whether distractionscause aspiration. Some patients may, in addition to mechanical difficulties, present learning disabilities, and attentionor concentration difficulties during meals. These can result in far greater risks than those associated with mechanicalproblems. These disorders must thus be considered and an appropriate solution found for each patient and eachstructure
Reassessment of possibilities for the patient to integrate the protocolTraining of nursing staff in higher function disordersSetting up a surveillance system for observation of meals
Criteria for effective swallowing are at this stageEase of swallowingAbsence of coughAbsence of pneumoniaMore or less normal duration of meal time (approximately 1/2 hour)Absence of anxietyPleasure
And also criteria such asNutritional status in conformity with the dietary goals set (energy needs covered by the reintroduction of oral
nourishment)In the end: ingesta (all the food and liquid intake by an individual in one day) sufficient to reduce and then stop
•
pl
gastrostomy feeding
• ‘‘definite’’ aspiration is defined as an episode of suffoca-tion in the context of vomiting or during feeding in thepresence of a witness;
• ‘‘Probable aspiration’’ (without a witness) is defined asthe appearance of at least one of the following within24 hours after an episode (with a witness) of vomit-ing, cough during feeding, displacement of a gastrictube, or the presence of vomit on clothes or the pillow:new infiltrate on the chest radiograph, tachypnoea (over18/min), fever or change in behavior without an obviouscause;
• ‘‘suspected aspiration’’ is defined as the absence of cri-teria of certainty of aspiration and by the sudden onsetof symptoms of lower airway disease, i.e. polypnoea,hypoxaemia and fever, in a previously stable patientwith at least one of the following criteria: presence of
a nasogastric tube, swallowing disorders or lower lobeinfiltrate;• ‘‘pneumonia’’ is defined as the absence of a clinical pic-ture of aspiration (definite or suspected), a radiological
w(‘
appearance compatible with one or more of the mani-festations suggestive of lower airways infection: cough,pleural pain type, fever over 38 ◦C, purulent expectora-tion, respiratory rate above or equal to 25/min, localizingsigns on the physical examination (crackles or bronchialrales);‘‘Aspiration pneumonia’’ is defined as symptoms of lowerrespiratory tract infection associated with an episode ofconfirmed or suspected aspiration and radiological signsof lower lobe infiltrates (unilateral or bilateral). This cor-responds to what we have called chemical pneumonitissecondary to aspiration of gastric fluid.
In the study by Mylotte et al., 330 institutionalizedatients admitted with suspected pneumonia were ana-yzed retrospectively. One hundred and ninety five patients
ere classified in three categories: chemical pneumonitis86 cases), aspiration pneumonia (43 cases), and episode of‘simple’’ aspiration (66 cases).
The main conclusions of the study were the following:

e88 F. Puisieux et al.
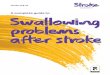
positive
NO
Symptoms of lower respiratory tract "infection"
Aspiration of gastric fluid (confirmed or suspected)
Chest radiograph
Chest radiograph
YES NO
"Chemical" pneumonitis
Episode of aspiration
Pneumonia Bronchitis
Duration of symptoms > 24 h
No antibiotics Symptomatic
treatment
Antibiotic treatment Symptomatic treatment
negative
YES
positive negative
No antibiotics Symptomatic
treatment
Figure 1. Treatment strategy in acute complications of swallowing disorders (based on Mylotte [62]).
•
•
•
•
agpoomshtarT
w[
Qa
Edt6ichomtA2rtpiKplla
according to the study definitions, chemical pneumonitiswas twice as frequent as aspiration pneumonia in insti-tutionalized elderly patients admitted to hospital with adiagnosis of pneumonia;there was no difference in terms of age, co-morbidity orlaboratory parameters between the three groups exceptfor swallowing disorders and the presence of a nasogastrictube being more frequent in the chemical pneumonitisgroup;there was no difference in the proportion of antibioticprescription (73%). Prescriptions were for 5.3 ± 2.4 daysfor pneumonia, 4.8 ± 2.7 days for chemical pneumonitis,and 3.8 ± 2.4 days for episodes of aspiration. Signifi-cantly more patients presenting chemical pneumonitisor an episode of aspiration were administered antibi-otics for less than 24 hours (11 and 23% against 0% forpneumonia);there was no difference in mortality or hospital staybetween the groups.
Following this study, based on the knowledge ofspiration of gastric fluid and appearance on the chest radio-raphs, characterizing four clinical situations (‘‘chemical’’neumonitis, pneumonia (due to aspiration), simple episodef aspiration, and bronchitis), an algorithm was devel-ped (Fig. 1) whose main objective is to guide treatmentanagement. It recommends that aspiration pneumonia
hould not be treated with antibiotics if the symptomsave lasted less than 24 hours. Patients whose symp-
oms exceed 24 hours have a risk of bacterial infectionnd should be treated. Symptomatic patients withoutadiographic images do not require antibiotic therapy.his algorithm was used prospectively in another studycdtw
hich confirmed the relevance of these recommendations62].
uestion 12: What is the epidemiology ofspiration pneumonia?
pidemiological studies have shown that, firstly, the inci-ence of pneumonia increases with age, with a risk siximes greater among those over 75 than among those under0 [65,66] and, secondly, that the incidence is greatern institutional than in community environments. Surveysonducted very regularly in the United States since 1980ave also shown an increase with time of the incidencef lower respiratory infections that are responsible forore than 45% of days of hospitalization, and an iden-
ical proportion of deaths from infectious diseases [67].n editorial in The Lancet Infectious Diseases in January006 stressed the urgency of finding ways to reduce theisk of infection in this age group. Several recent publica-ions argue that we must differentiate community-acquiredneumonias from pneumonias occuring in patients livingn institutions or receiving home care. In the article byollef in Chest in 2005 [68], patients in institutions whoresented pneumonia were older, had been hospitalizedonger, and showed different bacterial epidemiology withess pneumococci and more staphylococci and Pseudomonaseruginosa.
Concerning aspiration pneumonia, because there are no
onsensual diagnostic criteria, interpretation of literatureata is difficult. In most studies, the diagnosis is based onhe presence of lower respiratory tract infection in a patientith a risk of aspiration or occurring after aspiration [69].
tiou
a2
M
DliitCfls[doic
oosafltdcS
1Tsaflmfuep
P
Wt•
•
Swallowing disorders, pneumonia and respiratory tract infec
For aspiration pneumonia to develop there must havebeen aspiration into the larynx and lower respiratory tract oforopharyngeal contents previously colonized by pathogens.
Even though the etiology of aspiration pneumonia is mul-tifactorial [70] and the relationship between dysphagia andpneumonia is not direct [71], there is a strong associationbetween swallowing disorders and the development of aspi-ration pneumonia [72].
Loeb et al. studied the risk factors for onset of pneu-monia in residents of long-term care facilities in the UnitedStates [70]. In this study, multivariate analysis revealed thatdifficulty in swallowing food and medications were the mostimportant risk factors. Similarly, a French study has identi-fied as risk factors for nosocomial pneumonia in a geriatrichospital: malnutrition, heart failure, prescription of antibi-otics in the previous month, dependence for feeding and thepresence of a gastrostomy [73].
Several publications have also highlighted the importantrole of poor oral hygiene and reduced salivary flow [74,75]that facilitate colonization of the oropharynx. Many drugssuch as diuretics, antihistamines, anticholinergics, and neu-roleptics decrease saliva flow and thus could increase therisk for aspiration pneumonia. Moreover, randomized stud-ies have shown that good quality oral care decreased thenumber of cases of pneumonia in institutionalized popula-tions.
In a systematic review, the authors identified 17 ran-domized trials of interventions to prevent aspirationpneumonia in the elderly [76]. They concluded, how-ever, that there was insufficient proof of effectivenessof the different strategies proposed: patient positioning,dietary changes, oral hygiene, gastrostomy education forcaregivers, or drugs. New interventional studies on pre-vention are required. However, other reports suggest thatangiotensin converting enzyme inhibitors may have a pre-ventive effect because they increase levels of substanceP, a neurotransmitter that plays a key role in cough[77,78].
Question 13: What antibiotic treatmentfor aspiration pneumonia?
The French guidelines for the management of pneumoniain 2001 differentiate aspiration pneumonia and recom-mend their first-line treatment with amoxicillin associatedwith clavulanic acid (AAC) [79]. The 2003 IDSA rec-ommendations also mentioned this particular case andadvised AAC or clindamycin to cover anaerobic bacteria[80].
The 2006 SPILF (French Language Infectious DiseasesSociety) no longer differentiated aspiration pneumonia.However, they consider as special cases institution-acquiredpneumonias; we have seen that many of these are probablyaspiration pneumonia. They propose several choices: AAC,ceftriaxone or antipneumococcal fluoroquinolones (APFQ)[81].
In reality very few clinical studies are available to sup-port these proposals which are based on knowledge, albeitvery imperfect, of the germs allegedly responsible [72].In their 2003 review of aspiration pneumonia, Johnson
s disease in the elderly e89
nd Hirsch cited 18 studies including one dating from000 [82].
icrobiology of aspiration pneumonia
espite extensive investigations, a documented bacterio-ogical cause was only found in less than one in two casesn community-acquired pneumonia. This is particularly truen the elderly who are often unable to produce a spu-um specimen sufficient for microbiological examination.linical studies provide conflicting data on the microbialora responsible for pneumonia in the elderly. In sometudies, no significant difference was observed with age83]. However, in the majority of studies a higher inci-ence of Gram-negative enterobacteria and S. aureus wasbserved. Nevertheless, in community-acquired pneumonian the elderly, pneumococci remain the agents the mostommonly involved.
In fact, it is impossible to describe the microbiologyf respiratory infections in patients with swallowing dis-rders because no studies to date have focused on thispecific issue. The origin of the pathogens responsible forspiration pneumonia is the oropharynx. Oropharyngealora is dependent on many factors: previous antibioticreatment, hospitalization [84], institutional living, depen-ency, and sequelae of stroke contributing to oropharyngealolonization with enterobacteria and methicillin-resistant. aureus (MRSA) [85].
The great importance given to anaerobic bacteria in970—1980 [86] has reduced in more recent studies [87—89].his is possibly because transtracheal puncture, an aggres-ive procedure impaired by false positives [90], has beenbandoned. Furthermore, in edentulous patients, anaerobicora would be reduced. The anaerobic bacteria involved areainly Prevotella, Peptostreptococcus, Porphyromonas and
usobacteria [91]. Studies are definitely required to betternderstand the microbiology of aspiration pneumonia in gen-ral, and particularly pneumonia in institutionalized elderlyatients.
robabilistic antibiotic therapy
hen choosing probabilistic antibiotic therapy, the antibac-erial spectrum should cover:
for aspiration pneumonia in community settings or inwell elderly patients living in institutions: Streptococcuspneumoniae, Haemophilus influenza, enterobacteria andanaerobic bacteria, particularly when oral hygiene is poor.The choice may be between AAC, injectable third genera-tion cephalosporins ± imidazoles and APFQ, or ertapenem(a single daily injection). Among the fluroroquinolones,moxifloxacin is the most effective against anaerobic bac-teria [92];for aspiration pneumonia in institutional settings, thequestion is whether or not to take into account Pseu-domonas and/or MRSA. For El Solh, these two bacteriaare responsible for treatment failures and admissions toICU [93]. To take Pseudomonas into account, tazocillin
(piperacillin + tazobactam) or imipenem should be cho-sen; the addition of vancomycin is logical when there is agenuine suspicion of MRSA. Taking a sample for bacteriol-ogy, possibly endoscopic, is justified in this case, to enable
e F. Puisieux et al.
faTpom
Qpp
A
IItodemap
auogqi(ia
ATitm
I
Eotisio
Disclosure of interest
The authors declare that they have no conflicts of interestconcerning this article.
KEY POINTS
• The safety of oropharyngeal swallowing is notcompromised simply because of age, in the absenceof associated disorders.
• The cough reflex is not affected by age.• The prevalence of dysphagia is estimated at between
8 and 15% in patients living at home, and 30 to 40% inpatients living in institutions, with an increased riskof malnutrition.
• Swallowing disorders concern 50 to 75% of residentsin geriatric institutions.
• Swallowing disorders have neurological, muscle,general (diabetes, dehydration, etc.), local anddrug-associated causes.
• Information concerning any difficulties with foodintake in an elderly person must be communicatedto the prescribing physician.
• Investigation of swallowing disorders must includethorough history taking with the patient and/orcarers, as well as examination of the three phasesof swallowing: preparatory phase, oral phase andpharyngeal phase.
• Swallowing tests are a simple systematic means ofdetection in populations at risk.
• Further examinations are: videofluoroscopy,endoscopic examination and pharyngoesophagealmanometry.
• Management of swallowing disorders must have asits priority maintaining the pleasure in eating anddrinking, while guaranteeing a vital necessity.
• ‘‘Silent’’ aspiration must be detected (theimportance of pulmonary auscultation); coughingduring a meal indicates aspiration, but the absenceof cough is not synonymous with satisfactory transitof the food bolus.
• Reintroduction of food is done in four successivestages: ‘‘smooth’’ texture, ‘‘semi-liquid’’ texture,‘‘soft/minced’’ texture, ‘‘normal’’ texture.
• Acute complications of swallowing disorders aretracheobronchial aspiration, Mendelson syndrome,and a clinical picture of lower respiratory tractinfection.
• Subacute and chronic complications simulaterespiratory disorders.
• The incidence of pneumonia increases with age andis higher in institutional settings.
• Aspiration pneumonia is initially treated with
90
direct examination and guide the decision, and mainlyto readjust the prescription after 48—72 hours of initialprobabilistic treatment. The decision to take a sampledepends on the treatment plan and obviously other morepractical factors: facilities for performing the examina-tion, and ethical issues.
Concerning the prescription, the oral route is possiblerom the outset in non-severe forms. Parenteral treatmentsre more aggressive and have a higher risk of side effects.hey require discussion on the basis of severity of the clinicalicture, and the expectations and willingness of the patientsr their family/carers [94]. The switch to oral treatmentust be as rapid as possible.
uestion 14: Apart from aspirationneumonia, when should antibiotics berescribed?
cute aspiration of gastric contents
n the acute phase less than 48 hoursn the case of ‘‘normal’’ aspiration of gastric contents,here is no indication for curative or prophylactic antibi-tic therapy. This recommendation is shared by threeifferent authors [59,61,62,82,95]. These authors acknowl-dge, however, that this attitude is not respected byany practitioners, especially if there are co-morbidities,precarious state that corresponds well to elderly
atients.Antibiotic therapy can certainly be prescribed when the
cid barrier of the stomach is not functional (e.g.: antacids,pper gastrointestinal occlusion, gastrectomy). The antibi-tics the most often prescribed are: AAC, injectable thirdeneration cephalosporins, and antipneumococcal fluoro-uinolones (APFQ). The risk of Pseudomonas or MRSAnfection theoretically exists and depends on many factorsprior antibiotic treatment, state of dependence, life in annstitution with nosocomial type flora). This risk is taken intoccount on a case-by-case basis.
fter 48 hourshe persistence or the appearance of signs of pulmonary
nfection is an indication for antibiotic therapy similar tohat for aspiration pneumonia. A wait of 24 hours is perhapsore reasonable in elderly and frail patients [62].
nhalation of a foreign body
mergency endoscopic aspiration is required. For sec-ndary ventilatory disorders, the indication for antibioticherapy depends on the time to diagnosis and the possibil-
ties of reventilation after endoscopy. Anaerobic bacteriahould systematically be taken into account when decid-ng on treatment (prolonged anaerobiosis distal to thebstruction).amoxicillin associated with clavulanic acid, but allantibiotic regimens remain empirical.

tiou
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
Swallowing disorders, pneumonia and respiratory tract infec
References
[1] Guatterie M, Lozano V, Walter V, et al. Contrôle neurologiquede la déglutition. Réhabilitation de la voix et de la dégluti-tion après chirurgie partielle ou totale du larynx. Paris: Arnetteéditeur; 1992, p. 73—7.
[2] Lacau St Guily J, Chaussade S. Troubles de la déglutition del’adulte. Les maladies motrices du pharynx et de l’œsophage.Monographies du CCA Wagram; 1994. p. 1—5.
[3] Veyrune JL, Lassauzay C, Peyron MA, et al. Effets du vieil-lissement sur les structures et les fonctions orales. Rev Geriatr2004;29:51—60.
[4] Robbins J, Levine R, Wood J, et al. Age effects on lingual pres-sure generation as a risk factor for dysphagia. J Gerontol A BiolSci Med Sci 1995;50:M257—62.
[5] Shaker R, Lang IM. Effect of aging on the deglutiveoral, pharyngeal and oesophageal motor function. Dysphagia1994;9:221—8.
[6] Dejaeger E, Pelemans W, Ponette MD, et al. Mechanismsinvolved in postdeglution retention in the elderly. Dysphagia1997;12:63—7.
[7] Grishaw EK, Ott DJ, Frederick MG, et al. Functional abnormal-ities of the esophagus: a prospective analysis of radiographicfindings relative to age and symptoms. AJR Am J Roentgenol1996;167:719—23.
[8] Robbins J, Hamilton JW, Lof GL, et al. Oropharyngeal swal-lowing in normal adults of different ages. Gastroenterology1992;103:823—9.
[9] Tracy JF, Logemann JA, Kahrilas PJ, et al. Preliminary obser-vations on the effects of age on oropharyngeal deglutition.Dysphagia 1989;4:90—4.
[10] Katsumata U, Sekizawa K, Ebihara T, et al. Aging effects oncough reflex. Chest 1995;107:290—1.
[11] Bloem BR, Laagay AM, Van Beeck W, et al. Prevalence of sub-jective dysphagia in community residents aged over 87. Br MedJ 1990;300:721—2.
[12] Kawashima K, Motohashi Y, Fujishima I. Prevalence of dyspha-gia among community-dwelling elderly individuals as estimatedusing a questionnaire for dysphagia screening. Dysphagia2004;19:266—71.
[13] Lin LC, Wu SH, Chen HS, et al. Prevalence of impaired swallow-ing in institutionalized older people in Taiwan. J Am Geriatr Soc2002;50:1118—23.
[14] Ekberg O, Feinberg MJ. Altered swallowing function in elderlypatients without dysphagia: radiologic findings in 56 cases. AJRAm J Roentgenol 1991;156:1181—4.
[15] Nilsson H, Ekberg O, Olsson R, et al. Quantitative aspects ofswallowing in an elderly nondysphagic population. Dysphagia1996;11:180—4.
[16] Yoshikawa M, Yoshida M, Nagasaki T, et al. Aspects of swallow-ing in healthy dentate elderly persons older than 80 years. JGerontol A Biol Sci Med Sci 2005;60:506—9.
[17] Suominem M, Muurinen S, Routasalo P, et al. Malnutrition andassociated factors among aged residents in all nursing homesin Helsinki. Eur J Clin Nutr 2005;59:578—83.
[18] Smithard DG, O’Neill PA, England RE, et al. The naturalhistory of dysphagia following a stroke. Dysphagia 1997;12:188—93.
[19] Mann G, Hankey GJ, Cameron D. Swallowing function afterstroke: prognosis and prognostic factors at 6 months. Stroke1999;30:744—8.
[20] Finiels H, Strubel D, Jacquot JM. Les troubles de la dég-lutition du sujet âgé. Aspects épidémiologiques. Presse Med2001;30:1623—34.
[21] Finestone HM, Greene-Finestone LS, Wilson ES, et al. Malnu-trition in stroke patients on the rehabilitation service and at
[
s disease in the elderly e91
follow-up: prevalence and predictors. Arch Phys Med Rehabil1995;76:310—6.
22] Odderson R, Keaton JC, McKenna BS. Swallow management inpatients on an acute stroke pathway quality is cost effective.Arch Phys Med Rehabil 1995;76:1130—3.
23] Leopold NA, Kagel MC. Prepharyngeal dysphagia in Parkinson’sdisease. Dysphagia 1996;11:4—22.
24] Leopold NA, Kagel MC. Pharyngo-esophageal dysphagia inParkinson’s disease. Dysphagia 1997;12:11—8.
25] Priefer BA, Robbins J. Eating changes in mild-stage Alzheimer’sdisease: a pilot study. Dysphagia 1997;12:212—21.
26] Portet-Tarodo F, Touchon J. Démences et troubles de ladéglutition : épidémiologie, morbidité, modalités de priseen charge. In: Les troubles de la déglutition — Prob-lèmes en Médecine de Rééducation. Paris: Masson; 1999.p. 87—92.
27] Guatterie M, Beaucourt S, Lozano V. Les dysphagies des per-sonnes âgées. Diet Med 2000:45—6.
28] Horner J, Alberts M, Dawson D, et al. Swallowing in Alzheimer’sdisease. Alzheimer Dis Assoc Disord 1994;8:177—89.
29] Chouinard J. Dysphagia in Alzheimer disease: a review. J NutrHealth Aging 2000;4:214—7.
30] Trupe EH, Siebens H, Siebens AA. Prevalence of feeding andswallow disorders in a nursing home. Arch Phys Med Rehabil1984;65:651—2.
31] Marik PE, Kaplan D. Aspiration pneumonia and dysphagia in theelderly. Chest 2003;124:328—36.
32] Buchholz DW. Neurogenic dysphagia: what is the cause whenthe cause is not obvious? Dysphagia 1994;9:245—55.
33] Schindler JS, Kelly J. Swallowing disorders in the elderly. Laryn-goscope 2002:589—601.
34] Annese V, Bassotti G, Caruso N, et al. Gastrointestinalmotor dysfunction, symptoms and neuropathy in noninsulin-dependant (type 2) diabetes mellitus. J Clin Gastroenterol1999;29:171—7.
35] Kikawa F, Kubo F, Matsuda K, et al. Relationship betweenoesophageal dysfunction and neuropathy in diabetic patients.Am J Gastroenterol 2001;97:2026—32.
36] Denys P, Périé S, Kiefer L, et al. Les troubles de la déglutitionchez les patients cérébrolésés. In: Les troubles de la dégluti-tion. Paris: Masson; 1999. p. 63—7.
37] Stoschus B, Allescher HD. Drug-induced dysphagia. Dysphagia1993;8:154—9.
38] Loeshe WJ, Bromberg J, Langmore SE, et al. Xerostomia, xero-genic medications and food avoidances in selected geriatricsgroups. J Am Geriatr Soc 1995;43:401—7.
39] Smith PEM, Wiles CM. Cough responsiveness in neuro-genic dysphagia. J Neurol Neurosurg Psychiatry 1998;64:385—8.
40] Guinvarc’h S, Preux PM, Salle JY, et al. Proposition d’uneéchelle prédictive du risque de fausses-routes. Rev LaryngolOtol Rhinol (Bord) 1998;119:227—32.
41] DePippo KL, Holas MA, Reding MJ. Validation of the 3-Ozwater swallow test for aspiration following stroke. Arch Neurol1992;49:1259—61.
42] Gottlieb D, Kipnis M, Sister E, et al. Validation of the 50 mldrinking test for evaluation of post-stroke dysphagia. DisabilRehabil 1996;18:529—32.
43] Guatterie M, Lozano V. Classification des fausses routes. Col-loque déglutition et dysphagie. Bordeaux; 1993.
44] Durand F, Guatterie M, Lozano V. Adaptation des texturesalimentaires chez les patients présentant des troubles dela déglutition. Colloque déglutition et dysphagie. Bordeaux;1993.
45] Guatterie M, Lozano V. Déglutition et dysphagie en neurologie.Lett Med Reeduc 1997;43:3—9.

e
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
92
46] Lozano V, Guatterie M. Troubles de la déglutition chez lespersonnes âgées et adaptations palliatives. Information Diet1997;1:12—4.
47] Nathadwarawala KM, Nicklin J, Wiles CM. A timed test of swal-lowing capacity for neurological patients. J Neurol NeurosurgPsychiatry 1992;55:822—5.
48] DePippo KL, Holas MA, Reding MJ. The Burke dysphagia screen-ing test: validation of its use in patients with stroke. Arch PhysMed Rehabil 1994;75:1284—6.
49] Daniels SK, Lindsay AB, Mahoney MC, et al. Clinical pre-dictors of dysphagia and aspiration risk: outcome measuresin acute stroke patients. Arch Phys Med Rehabil 2000;81:1030—3.
50] Leder SB. Serial fiberoptic endoscopic swallowing evaluationsin the management of patients with dysphagia. Arch Phys MedRehabil 1998;79:1264—9.
51] Wooi M, Scott A, Perry A. Teaching speech pathology studentsthe interpretation of videofluoroscopic swallowing studies.Dysphagia 2001;16:32—9.
52] Langmore SE, Schatz K, Olson N. Fiberoptic endoscopic exam-ination of swallowing safety: a new procedure. Dysphagia1988;2:216—9.
53] Cot F, et al. La dysphagie oropharyngée chez l’adulte. Maloine;1996.
54] Feinberg MJ, Knebl J, Tully J. Prandial aspiration and pneumo-nia in an elderly population followed over 3 years. Dysphagia1996;11:104—9.
55] Guatterie M, Lozano V. Problématique des troubles de la dég-lutition. Rev Laryngol Otol Rhinol 1990;2:401—6.
56] Logemann JA. Evaluation and treatment of swallowing disor-ders. San Diego: College Hillpress; 1983.
57] Barat M, Miremont F, Guatterie M, Lozano V. Troubles de ladéglutition dans les affections neurologiques dégénératives. In:Les troubles de la déglutition — Problèmes en médecine derééducation. Masson; 1999. 37:69—75.
58] Berzlanovich AM, Fazeny-Dörner B, Waldhoer T, et al. Foreignbody asphyxia. A preventable cause of death in the elderly. AmJ Prev Med 2005;28:65—9.
59] Segal R, Pogoreliuk I, Dan M, et al. Gastric microbiota in elderlypatients fed via nasogastric tubes for prolonged periods. J HospInfect 2006;63:79—83.
60] Marik PE. Aspiration pneumonitis and aspiration pneumonia. NEngl J Med 2001;344:665—71.
61] Mylotte JM, Goodnough S, Naughton BJ. Pneumonia versus aspi-ration pneumonitis in nursing home residents: diagnosis andmanagement. J Am Geriatr Soc 2003;51:17—23.
62] Mylotte JM, Goodnough SR, Gould M. Pneumonia versusaspiration pneumonitis in nursing home residents: prospec-tive application of a clinical algorithm. J Am Geriatr Soc2005;53:755—61.
63] Mukhopadhyay S, Katzenstein AL. Pulmonary disease due toaspiration of food and other particulate matter: a clinico-pathologic study of 59 cases diagnosed on biopsy or resectionspecimens. Am J Surg Pathol 2007;31:752—9.
64] Matsuse T, Oka T, Kida K, et al. Importance of diffuse aspirationbronchiolitis caused by chronic occult aspiration in the elderly.Chest 1996;110:1289—93.
65] Jokinen C, Heiskanen L, Juvonen H, et al. Incidenceof community-acquired pneumonia in the population offour municipalities in eastern Finland. Am J Epidemiol1993;137:977—88.
66] Kaplan V, Angus DC, Griffin MF, et al. Hospitalized community-acquired pneumonia in the elderly: age- and sex-relatedpatterns of care and outcome in the United States. Am J Resp
Crit Care Med 2002;165:766—72.67] Curns AT, Holman RC, Sejvar JJ, et al. Infectious disease hospi-talizations among older adults in the United States from 1990through 2002. Arch Intern Med 2005;165:2514—20.
[
[
F. Puisieux et al.
68] Kollef MH, Shorr A, Tabak YP, et al. Epidemiology and out-comes of health-care-associated pneumonia: results froma large US database of culture-positive pneumonia. Chest2005;128:3854—62.
69] Oh E, Weintraub N, Dhanani S. Can we prevent aspirationpneumonia in the nursing home? J Am Med Dir Assoc 2005;6:S76—80.
70] Loeb M, McGeer A, McArthur M, et al. Risk factors forpneumonia and other lower respiratory tract infections inelderly residents of long-term care facilities. Arch Intern Med1999;159:2058—64.
71] Langmore SE, Terpenning MS, Schork A, et al. Predictors ofaspiration pneumonia: how important is dysphagia? Dysphagia1998;13:69—81.
72] Mylotte JM, Tayara A, Goodnough S. Epidemiology of blood-stream infection in nursing home residents: evaluationin a large cohort from multiple homes. Clin Infect Dis2002;35:1484—90.
73] Rothan-Tondeur M, Meaume S, Girard L, et al. Risk fac-tors for nosocomial pneumonia in a geriatric hospital: acontrol-case one-center study. J Am Geriatr Soc 2003;51:997—1001.
74] Palmer LB, Albulak K, Fields S, et al. Oral clearance andpathogenic oropharyngeal colonization in the elderly. Am JRespir Crit Care Med 2001;164:464—8.
75] Abe S, Ishihara K, Adachi M, et al. Oral hygiene evaluation foreffective oral care in preventing pneumonia in dentate elderly.Arch Gerontol Geriatr 2006;43:53—64.
76] Loeb MB, Becker M, Eady A, et al. Interventions to preventaspiration pneumonia in older adults: a systematic review. JAm Geriatr Soc 2003;51:1018—22.
77] Arai T, Yasuda Y, Toshima S, et al. ACE inhibitors and pneumoniain elderly people. Lancet 1998;12:1937—8.
78] Arai T, Yasuda Y, Takaya T, et al. Angiotensin-convertingenzyme inhibitors, angiotensin-II receptor antagonists, andpneumonia in elderly hypertensive patients with stroke. Chest2001;119:660—1.
79] Chidiac C. Révision de la IVe conférence de consen-sus en thérapeutique anti-infectieuse de la Société depathologie infectieuse de langue francaise. Med Mal Infect2001;30:268—301.
80] Mandell LA, Bartlett JG, Dowell, et al. Update of prac-tice guidelines for the management of community-acquiredpneumonia in immunocompetent adults. Clin Infect Dis2003;37:1405—33.
81] SPILF. 15e conférence de consensus en thérapeutique anti-infectieuse. Prise en charge des infections des voiesrespiratoires basses de l’adulte immunocompétent. Med MalInfect 2006;5:235—44.
82] Johnson JL, Hirsch C. Aspiration pneumonia. Recognizingand managing a potentially growing disorder. Postgrad Med2003;113:99—112.
83] Ruiz M, Ewig S, Marcos MA, et al. Etiology of community-acquired pneumonia: impact of age, comorbidity, and severity.Am J Respir Crit Care Med 1999;160:397—405.
84] Preston AJ, Gosney MA, Noon S, et al. Oral flora of elderlypatients following acute medical admission. Gerontology1999;45:49—52.
85] Abe S, Ishihara K, Okuda K. Prevalence of potential respira-tory pathogens in the mouths of elderly patients and effectsof professional oral care. Arch Gerontol Geriatr 2001;32:45—55.
86] Bartlett JG, Gorbach SL. The triple threat of aspiration pneu-monia. Chest 1975;68:560—6.
87] Jansens JP, Krause KH. Pneumonia in the very old. Lancet2004;4:112—24.
88] Fernandez-Sabe N, Carratala J, Rozon B, et al. Community-acquired pneumonia in very elderly patients, causative

tiou
[
[
Swallowing disorders, pneumonia and respiratory tract infec
organisms and clinical characteristics and outcome. Medicine2003;82:159.
[89] El-Solh AA, Pietrantoni C, Bhat A, et al. Microbiology of severeaspiration pneumonia in institutionalized elderly. Am J RespirCrit Care Med 2003;167:1650—4.
[90] Gaillat J, Sédallian A. Conditions pour le diagnostic d’uneinfection respiratoire basse à anaérobies. Med Mal Infect2000;330:126S—32S.
[91] Sedallian A, Bland S. Epidémiologie et facteurs de risque. MedMal Infect 2000;30:85S—90S.
[92] Behra-Miellet J, Dubreuil L, Jumas-Bilak E. Antianaerobicactivity of moxifloxacin compared with that of ofloxacin,
[
s disease in the elderly e93
ciprofloxacin, clindamycin, metronidazole and beta-lactams.Int J Antimicrob Agents 2002;20:366—74.
93] El-Solh AA, Aquilina AT, Dhillon RS, et al. Impact of invasivestrategy on management of antimicrobial treatment failure ininstitutionalized older people with severe pneumonia. Am JRespir Crit Care Med 2002;166:1038—43.
94] Chen JH, Lamberg JL, Chen Y. Occurrence and treatment ofsuspected pneumonia in long-term care residents dying with
advanced dementia. J Am Geriatr Soc 2006;54:290—5.95] Janda M, Sheeren TW, Noldge S. Management of pul-monary aspiration. Best Pract Res Clin Anaesthesiol 2006;20:409—27.