Embed Size (px)
Citation preview
Surgical Treatment of Migraine HeadachesBahman Guyuron, M.D., Tarvez Tucker, M.D., and Janine Davis, R.N.Cleveland, Ohio
This prospective study was conducted to investigate therole of removal of corrugator supercilii muscles, transec-tion of the zygomaticotemporal branch of the trigeminalnerve, and temple soft-tissue repositioning in the treat-ment of migraine headaches. Using the criteria set forthby the International Headache Society, the researchteam’s neurologist evaluated patients with moderate tosevere migraine headaches, to confirm the diagnosis. Sub-sequently, the patients completed a comprehensive mi-graine headaches questionnaire and the team’s plasticsurgeon injected 25 units of botulinum toxin type A (Bo-tox) into each corrugator supercilii muscle. The patientswere asked to maintain an accurate diary of their migraineheadaches and to complete a monthly questionnaire doc-umenting pertinent information related to their head-aches. Patients in whom the injection of Botox resulted incomplete elimination of the migraine headaches thenunderwent resection of the corrugator supercilii muscles.Those who experienced only significant improvement un-derwent transection of the zygomaticotemporal branch ofthe trigeminal nerve with repositioning of the temple softtissues, in addition to removal of the corrugator superciliimuscles. Once again, patients kept a detailed postopera-tive record of their headaches. Of the 29 patients includedin the study, 24 were women and five were men, with anaverage age of 44.9 years (range, 24 to 63 years). Twenty-four of 29 patients (82.8 percent, p � 0.001) reported apositive response to the injection of Botox, 16 (55.2 per-cent, p � 0.001) observed complete elimination, eight(27.6 percent, p � 0.04) experienced significant improve-ment (at least 50 percent reduction in intensity or sever-ity), and five (17.2 percent, not significant) did not noticea change in their migraine headaches. Twenty-two of the24 patients who had a favorable response to the injectionof Botox underwent surgery, and 21 (95.5 percent, p �0.001) observed a postoperative improvement. Ten pa-tients (45.5 percent, p � 0.01) reported elimination ofmigraine headaches and 11 patients (50.0 percent, p �0.004) noted a considerable improvement. For the entiresurgical group, the average intensity of the migraine head-aches reduced from 8.9 to 4.1 on an analogue scale of 1to 10, and the frequency of migraine headaches changedfrom an average of 5.2 per month to an average of 0.8 permonth. For the group who only experienced an improve-ment, the intensity fell from 9.0 to 7.5 and the frequencywas reduced from 5.6 to 1.0 per month. Only one patient(4.5 percent, not significant) did not notice any change.
The follow-up ranged from 222 to 494 days, the averagebeing 347 days. In conclusion, this study confirms thevalue of surgical treatment of migraine headaches, inas-much as 21 of 22 patients benefited significantly from thesurgery. It is also evident that injection of Botox is anextremely reliable predictor of surgical outcome. (Plast.Reconstr. Surg. 109: 2183, 2002.)
Migraine headaches affect 18 percent ofwomen and 6 percent of men in the UnitedStates.1 One-third of the patients with periodicor chronic migraine headaches are not helpedby standard therapies. In addition, even themost efficacious medications do not entirelyeliminate migraine headaches but only reducetheir severity and frequency.
We have recently reported the unexpectedelimination or improvement in migraine head-aches noted following rejuvenation of the fore-head involving removal of hyperactive corruga-tor supercilii muscles.2 The retrospective studyindicated that of 39 patients with migraineheadaches who underwent a forehead aes-thetic procedure, 15 (38.5 percent) reportedcomplete disappearance of their headachesand 16 patients (41 percent) observed signifi-cant improvement within a mean follow-up pe-riod of 46.5 months.
This prospective study was conducted to con-firm the findings of our retrospective study.The patients likely to have a successful out-come following surgery were identified usinginjection of botulinum toxin type A (Botox,Allergan, Inc., Irvine, Calif.). These patientsunderwent surgical removal of the corrugatorsupercilii muscles alone or in conjunction withtransection of the zygomaticotemporal branchof the trigeminal nerve and repositioning of
From the Departments of Plastic Surgery and Neurology, Case Western Reserve University; and the American Migraine Center. Received forpublication September 5, 2001.
Presented at the 70th Annual Meeting of the American Society of Plastic Surgeons, in Orlando, Florida, November 3 through 7, 2001.
2183
the temple soft tissues to prevent recoaptationof this nerve.
PATIENTS AND METHODS
Patients who complained of migraine head-aches were initially evaluated by the researchteam’s neurologist (T.T.) to confirm the diag-nosis of migraine headaches on the basis ofcriteria set forth by the International Head-ache Society.3 The patients completed a com-prehensive migraine headaches questionnairethat contained 56 items and recorded theirsymptoms during the month before the proce-dures. Frequency, duration, characteristics,and severity of headaches, graded on an ana-logue scale from 1 to 10 (10 being very severe),were documented. Corrugator supercilii mus-cle hypertrophy was clinically assessed in allpatients and graded from 1 to 5 (5 being sig-nificant). Patients with medical or neurologicconditions likely to induce migraine headacheswere considered ineligible for the study. Simi-larly, those who were deemed unacceptablesurgical risks and patients who were pregnantor nursing at the time of neurologic examina-tions were excluded from the study. In addi-tion, patients whose migraine headaches re-sponded to over-the-counter medications werebarred from the study. Patients who were ingood health, between 18 and 75 years old, andwho experienced two or more moderate tosevere migraine headaches each month wereconsidered eligible for the study.
Twenty-five units of Botox were injected bythe plastic surgeon (B.G.) into each corrugatorsupercilii muscle of the volunteers who ful-filled the study criteria. After injection of Bo-tox, patients were asked to refrain from usingany regular prophylactic migraine headachesmedications and to keep an accurate diary ofany headaches, including the details of symp-toms, location, severity, and frequency of theheadaches. The patients were instructed, how-ever, to use their migraine headache medica-tions if they experienced an acute attack.
Those patients who responded favorably tothe injection of Botox with complete elimina-tion of migraine headaches for at least 6 weeks,or those who observed significant (at least 50percent) reduction in intensity or severity oftheir migraine headaches, were consideredsuitable candidates for surgery. Subjects whoobserved complete elimination of their mi-graine headaches following Botox injection un-derwent a thorough resection of each corruga-
tor supercilii muscle. Those patients whonoted only improvement following Botox in-jection underwent a combination proceduresimilar to an endoscopic forehead rejuvena-tion. This consisted of complete removal ofeach corrugator supercilii muscle, transectionof the zygomaticotemporal branch of the tri-geminal nerve, and repositioning of the templesoft tissues to minimize the potential for reco-aptation of the transected nerves.
After injection or surgery, patients kept adiary of their headaches and completed a ques-tionnaire on a monthly basis. A reduction inintensity or frequency of at least 50 percent wasconsidered improvement. The results werethen statistically analyzed using binomial distri-bution Z statistics with continuity correction.The p values were calculated by comparing theobserved proportion on the basis of 29 patientsundergoing Botox injection against 1 percentimprovement and the proportion on the basisof 22 patients who underwent surgery whencompared against 5 percent improvement, re-spectively. When comparing the presurgicaland postsurgical frequency and intensity data,we used the two-tailed Wilcoxon signed ranktest.
Surgical Techniques
For the transpalpebral approach,4,5 a skinincision was made in the upper tarsal crease ofeach eyelid, approximately 1 inch in length,and deepened through the orbicularis muscleonly. In the anatomic plane between the orbic-ularis muscle and orbital septum, the dissec-tion was continued cephalad until the corruga-tor supercilii muscles were exposed. Preservingthe supraorbital and supratrochlear nerves,both corrugator supercilii muscles were re-moved as thoroughly as possible. A smallamount of fat, often protruding on the medialaspect of the upper eyelid, was harvestedthrough a small opening in the orbital septumand applied to the corrugator supercilii musclesite. This fat graft was sutured in place using 6-0polyglactin (Vicryl). The skin incision was re-paired using 6-0 plain catgut.
The combination of corrugator superciliimuscle resection, temporal release, and tran-section of the zygomaticotemporal branch ofthe trigeminal nerve was performed throughan endoscopic approach. Five half-inch inci-sions were made, one in the center and two oneither side in the temple area. The endoscopicaccess devices were inserted. A subperiosteal
2184 PLASTIC AND RECONSTRUCTIVE SURGERY, June 2002

dissection was carried to the supraorbital rim,lateral orbital rim, zygomatic arch, and malarregion. The zygomaticotemporal branch of thetrigeminal nerve was transected and coagu-lated. The periosteum and the arcus marginaliswere released over the lateral orbital regionand the supraorbital area to allow reposition-ing of the tissues. The supraorbital nerves andeach corrugator supercilii muscle were ex-posed. The glabellar area was dissected and theperiosteum was released. Next, each corruga-tor supercilii muscle was removed as com-pletely as was feasible. Fat graft, harvested fromthe temporal region, deep to the intermediateor deep temporal fascia, was applied to thecorrugator supercilii muscle site. Fixation wasachieved with 3-0 polydioxanone fascia sutureslaterally and bone tunneling through the me-dial incision in the temple area. A suctiondrain was placed in position and anchored tothe skin using 5-0 plain catgut. The incisionswere repaired using a combination of 5-0 poly-glactin (Vicryl) and 5-0 plain catgut.
RESULTS
Twenty-nine patients with a confirmed diag-nosis of moderate to severe migraine head-aches constituted the study group. There were24 women and five men, closely matching thenational gender-based distribution of the mi-graine headache patient population (Table I).The patients ranged in age from 24 to 63 years,with an average age of 44.9 years. The averagecorrugator supercilii muscle hypertrophy was4.7, ranging from 4 to 5.
Outcome following Injection of Botox
After injection of Botox, 24 of the 29 patients(82.8 percent, p � 0.001) noted an improve-ment in their migraine headaches. In 16 pa-tients (55.2 percent, p � 0.001), migraineheadaches disappeared completely (Table II),whereas eight patients (27.6 percent, p � 0.04)observed significant improvement for 6 consec-utive weeks or more. The average frequencydecreased from 6.4 to 2.1 per month and theintensity fell from 8.6 to 6.1 (Table II). Five
TABLE IEntire Patient Population
PatientAge
(years) GenderAura/
Nonaura
Before Treatment After Botox Injection After Surgery
CorrugatorSuperciliiMuscle
Hypertrophy
MigraineHeadacheFrequencyper Month
MigraineHeadacheIntensity
per Month
MigraineHeadacheFrequencyper Month
MigraineHeadacheIntensity
per MonthBotox
Outcome
MigraineHeadacheFrequencyper Month
MigraineHeadacheIntensity
per MonthDays of
Follow-UpSurgical
Outcome
1 47 F A 4 6 9 2 8 SD 1.8 7.2 313 SD2 40 F A/N 5 8 9 0 0 E 0.2 5.0 320 SD3 49 M N 5 8 9 2 6 SD 0.7 9.5 277 SD4 40 F A 5 3 10 0 0 E 0 0 382 E5 42 F N 5 4 9 0 0 E6 35 F N 5 8 9 12 7 NR7 38 F A 5 5 10 2 9 SD8 44 M A 4 4 10 0 0 E 0 0 461 E9 47 M A 4 5 8 2 7 SD 3.2 6.8 347 SD
10 53 F A 5 3 10 0 0 E 0 0 361 E11 41 F N 5 6 7 0 0 E 6.0 6.7 311 NR12 49 F A 4 6 8 0 0 E 0 0 494 E13 48 F A 5 4 8 0 0 E 0 0 326 E14 63 M N 4 6 9 15 9 NR15 58 M N 5 9 7 2 8 SD 0 0 340 E16 53 F A 4 3 9 0 0 E 0 0 312 E17 47 F N 5 4 8 1 4 SD 0.1 9 347 SD18 34 F A 5 9 0 0 E 0.7 6.4 404 SD19 53 F N 5 4 9 5 7 NR20 45 F N 5 5 8 5 4 SD 1.5 5.7 340 SD21 30 F A 5 3 8 0 0 E 0 0 222 E22 29 F A 4 5 9 0 0 E 0.8 8 362 SD23 49 F N 5 9 10 0 0 E 1.5 9.7 306 SD24 24 F A 5 5 9 0 0 E 0 0 322 E25 63 F N 4 19 7 10 7 NR26 62 F A 5 8 9 11 9 NR27 44 F A 5 3 10 0 0 E 0.3 8.5 349 SD28 38 F N 4 8 10 1 3 SD 0 0 341 E29 38 F N 5 3 10 0 0 E 0.2 7.0 389 SD
Average 44.9 F 24 A 14 4.7 5.9 8.7 2.4 3.0 E 16 0.9 4.1 347 E 10M 5 N 14 SD 8 SD 11
NR 5 NR 1
E, elimination; SD, significant decrease; NR, no response; A, aura; N, nonaura; M, male; F, female.
Vol. 109, No. 7 / SURGICAL TREATMENT OF MIGRAINE HEADACHES 2185
patients (17.2 percent, not significant) re-ported no change (Table II). Two patients (6.9percent) noted transient unilateral upper eye-lid ptosis that lasted 2 weeks for one patientand 3 weeks for the other patient.
Outcome following Surgery
Of the 24 patients who noted a favorableresponse to injection of Botox, 22 underwentsurgery. This group included 18 women andfour men ranging in age from 24 to 58 yearsold. Of the 22 patients who underwent surgery,21 (95.5 percent, p � 0.001) observed an im-provement in the migraine headaches. Tenpatients (45.5 percent, p � 0.01) noted elimi-nation of migraine headaches (Table II) and11 (50.0 percent, p � 0.004) noted a significantimprovement (Table II). The average intensityof migraine headaches for the entire surgicalgroup was reduced from 8.9 to 4.1 (p � 0.04)on an analogue scale of 1 to 10, and the fre-quency changed from 5.2 to an average of 0.8(p � 0.001) per month. When the group withimprovement only was analyzed, the intensityfell from 9.0 to 7.5 and the frequency changedfrom 5.6 to 1.0 migraine headaches per month.Only one patient failed to notice an improve-ment (Table II). The follow-up ranged from222 to 494 days, with an average of 347 days.
There was no incidence of wound infection.Three patients received an infusion of desmo-pressin (DDAVP) for moderately excessive
bleeding during surgery. All patients experi-enced some numbness in the temple area last-ing 1 to 6 months, with an average of 2.3months. All patients reported complete sen-sory recovery during the follow-up period. Allpatients noted aesthetic improvement, with thedisappearance or diminution of the foreheadline and better eyebrow position. The patientwho failed to notice enough improvementstated that the location and the pattern of hermigraine headaches were different when com-pared with her preoperative headaches. Hermedical history confirmed long-standing peri-nasal sinus disease, and an internal nose exam-ination revealed a notable deviation of the sep-tum. Similarly, three of 11 patients whoreported only improvement in migraine head-aches stated that the pattern and the locationof the migraine headaches were differentpostoperatively.
DISCUSSION
There has been no report of a surgical curefor conventional migraine headaches as a re-sult of muscle resection or transection of thezygomaticotemporal branch of the trigeminalnerve. Partial or complete section of the tri-geminal nerve has been advocated as an effec-tive treatment for cluster-type headaches.6–10
These surgical procedures, however, are com-plex, and the associated morbidity, especially
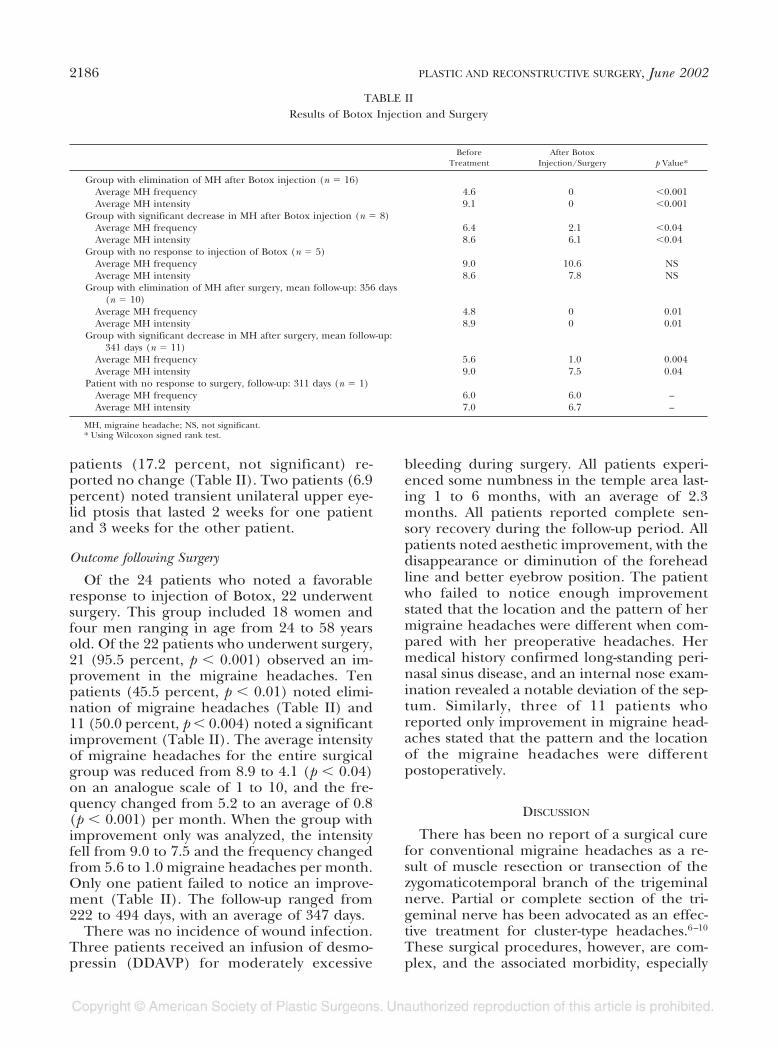
TABLE IIResults of Botox Injection and Surgery
BeforeTreatment
After BotoxInjection/Surgery p Value*
Group with elimination of MH after Botox injection (n � 16)Average MH frequency 4.6 0 �0.001Average MH intensity 9.1 0 �0.001
Group with significant decrease in MH after Botox injection (n � 8)Average MH frequency 6.4 2.1 �0.04Average MH intensity 8.6 6.1 �0.04
Group with no response to injection of Botox (n � 5)Average MH frequency 9.0 10.6 NSAverage MH intensity 8.6 7.8 NS
Group with elimination of MH after surgery, mean follow-up: 356 days(n � 10)
Average MH frequency 4.8 0 0.01Average MH intensity 8.9 0 0.01
Group with significant decrease in MH after surgery, mean follow-up:341 days (n � 11)
Average MH frequency 5.6 1.0 0.004Average MH intensity 9.0 7.5 0.04
Patient with no response to surgery, follow-up: 311 days (n � 1)Average MH frequency 6.0 6.0 –Average MH intensity 7.0 6.7 –
MH, migraine headache; NS, not significant.* Using Wilcoxon signed rank test.
2186 PLASTIC AND RECONSTRUCTIVE SURGERY, June 2002
ophthalmic anesthesia, can have graveconsequences.
Our surgical approach involves the periph-eral branches of the trigeminal nerve and mus-cles affecting these terminal branches; as a re-sult, the surgical procedures are lesscomplicated and serious morbidity is extremelyrare. The role of the trigeminal nerve in thepathogenesis of migraine headaches has beenstudied for over 30 years. It is postulated thatstimulation of this nerve results in release ofneuropeptides such as substance P, calcitoningene-related peptide, and neurokinin A.11,12
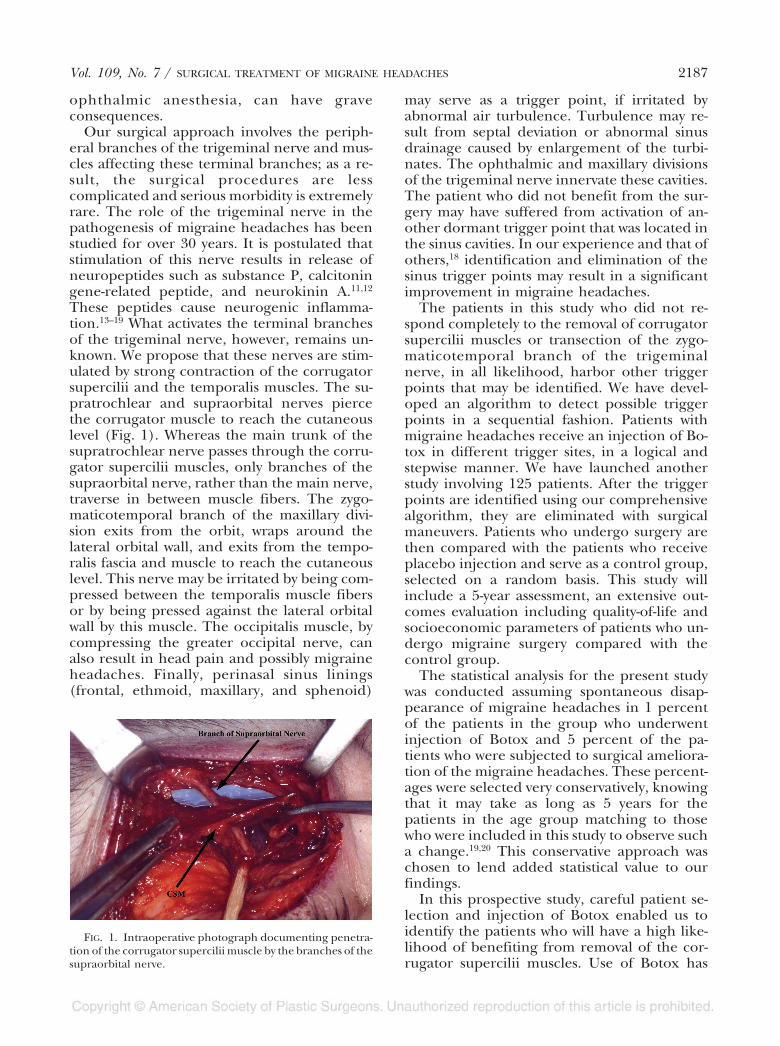
These peptides cause neurogenic inflamma-tion.13–19 What activates the terminal branchesof the trigeminal nerve, however, remains un-known. We propose that these nerves are stim-ulated by strong contraction of the corrugatorsupercilii and the temporalis muscles. The su-pratrochlear and supraorbital nerves piercethe corrugator muscle to reach the cutaneouslevel (Fig. 1). Whereas the main trunk of thesupratrochlear nerve passes through the corru-gator supercilii muscles, only branches of thesupraorbital nerve, rather than the main nerve,traverse in between muscle fibers. The zygo-maticotemporal branch of the maxillary divi-sion exits from the orbit, wraps around thelateral orbital wall, and exits from the tempo-ralis fascia and muscle to reach the cutaneouslevel. This nerve may be irritated by being com-pressed between the temporalis muscle fibersor by being pressed against the lateral orbitalwall by this muscle. The occipitalis muscle, bycompressing the greater occipital nerve, canalso result in head pain and possibly migraineheadaches. Finally, perinasal sinus linings(frontal, ethmoid, maxillary, and sphenoid)
may serve as a trigger point, if irritated byabnormal air turbulence. Turbulence may re-sult from septal deviation or abnormal sinusdrainage caused by enlargement of the turbi-nates. The ophthalmic and maxillary divisionsof the trigeminal nerve innervate these cavities.The patient who did not benefit from the sur-gery may have suffered from activation of an-other dormant trigger point that was located inthe sinus cavities. In our experience and that ofothers,18 identification and elimination of thesinus trigger points may result in a significantimprovement in migraine headaches.
The patients in this study who did not re-spond completely to the removal of corrugatorsupercilii muscles or transection of the zygo-maticotemporal branch of the trigeminalnerve, in all likelihood, harbor other triggerpoints that may be identified. We have devel-oped an algorithm to detect possible triggerpoints in a sequential fashion. Patients withmigraine headaches receive an injection of Bo-tox in different trigger sites, in a logical andstepwise manner. We have launched anotherstudy involving 125 patients. After the triggerpoints are identified using our comprehensivealgorithm, they are eliminated with surgicalmaneuvers. Patients who undergo surgery arethen compared with the patients who receiveplacebo injection and serve as a control group,selected on a random basis. This study willinclude a 5-year assessment, an extensive out-comes evaluation including quality-of-life andsocioeconomic parameters of patients who un-dergo migraine surgery compared with thecontrol group.
The statistical analysis for the present studywas conducted assuming spontaneous disap-pearance of migraine headaches in 1 percentof the patients in the group who underwentinjection of Botox and 5 percent of the pa-tients who were subjected to surgical ameliora-tion of the migraine headaches. These percent-ages were selected very conservatively, knowingthat it may take as long as 5 years for thepatients in the age group matching to thosewho were included in this study to observe sucha change.19,20 This conservative approach waschosen to lend added statistical value to ourfindings.
In this prospective study, careful patient se-lection and injection of Botox enabled us toidentify the patients who will have a high like-lihood of benefiting from removal of the cor-rugator supercilii muscles. Use of Botox has
FIG. 1. Intraoperative photograph documenting penetra-tion of the corrugator supercilii muscle by the branches of thesupraorbital nerve.
Vol. 109, No. 7 / SURGICAL TREATMENT OF MIGRAINE HEADACHES 2187
proved to be an extremely reliable prognosti-cator. Botox is currently being studied for tem-porary treatment and prevention of migraineheadaches with or without aura.21 Injection ofBotox into the frontalis, temporalis, glabellar,and occipital areas has been found to reducethe severity and frequency of migraine head-aches in small studies.22,23 Larger trials are cur-rently under way.24 Interestingly, Botox may beas effective in treating migraine headaches as itis in treating tension-type headaches.25 In ad-dition, two pilot open-labeled studies haveshown improvement in headache severityscores and reduction in headache duration inpatients with chronic and episodic tension-typeheadaches.26
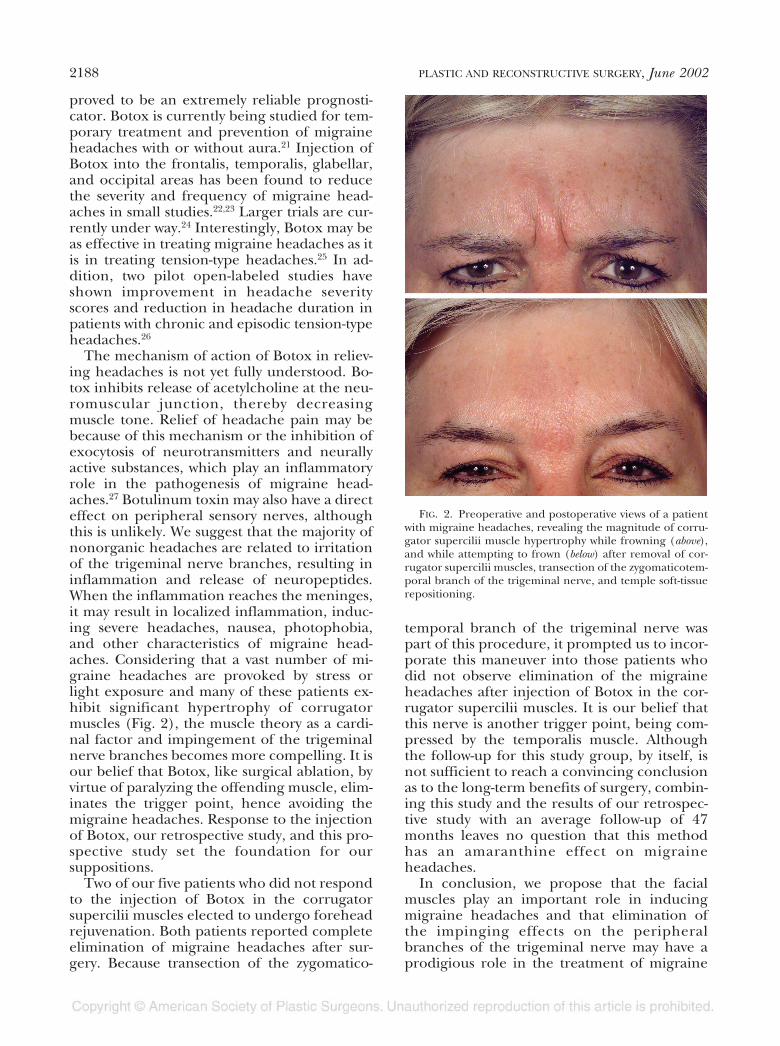
The mechanism of action of Botox in reliev-ing headaches is not yet fully understood. Bo-tox inhibits release of acetylcholine at the neu-romuscular junction, thereby decreasingmuscle tone. Relief of headache pain may bebecause of this mechanism or the inhibition ofexocytosis of neurotransmitters and neurallyactive substances, which play an inflammatoryrole in the pathogenesis of migraine head-aches.27 Botulinum toxin may also have a directeffect on peripheral sensory nerves, althoughthis is unlikely. We suggest that the majority ofnonorganic headaches are related to irritationof the trigeminal nerve branches, resulting ininflammation and release of neuropeptides.When the inflammation reaches the meninges,it may result in localized inflammation, induc-ing severe headaches, nausea, photophobia,and other characteristics of migraine head-aches. Considering that a vast number of mi-graine headaches are provoked by stress orlight exposure and many of these patients ex-hibit significant hypertrophy of corrugatormuscles (Fig. 2), the muscle theory as a cardi-nal factor and impingement of the trigeminalnerve branches becomes more compelling. It isour belief that Botox, like surgical ablation, byvirtue of paralyzing the offending muscle, elim-inates the trigger point, hence avoiding themigraine headaches. Response to the injectionof Botox, our retrospective study, and this pro-spective study set the foundation for oursuppositions.
Two of our five patients who did not respondto the injection of Botox in the corrugatorsupercilii muscles elected to undergo foreheadrejuvenation. Both patients reported completeelimination of migraine headaches after sur-gery. Because transection of the zygomatico-
temporal branch of the trigeminal nerve waspart of this procedure, it prompted us to incor-porate this maneuver into those patients whodid not observe elimination of the migraineheadaches after injection of Botox in the cor-rugator supercilii muscles. It is our belief thatthis nerve is another trigger point, being com-pressed by the temporalis muscle. Althoughthe follow-up for this study group, by itself, isnot sufficient to reach a convincing conclusionas to the long-term benefits of surgery, combin-ing this study and the results of our retrospec-tive study with an average follow-up of 47months leaves no question that this methodhas an amaranthine effect on migraineheadaches.
In conclusion, we propose that the facialmuscles play an important role in inducingmigraine headaches and that elimination ofthe impinging effects on the peripheralbranches of the trigeminal nerve may have aprodigious role in the treatment of migraine
FIG. 2. Preoperative and postoperative views of a patientwith migraine headaches, revealing the magnitude of corru-gator supercilii muscle hypertrophy while frowning (above),and while attempting to frown (below) after removal of cor-rugator supercilii muscles, transection of the zygomaticotem-poral branch of the trigeminal nerve, and temple soft-tissuerepositioning.
2188 PLASTIC AND RECONSTRUCTIVE SURGERY, June 2002

headaches. Because 21 of 22 patients re-sponded positively to surgery, we conclude thatsurgical treatment of migraine headaches issuccessful. Even in patients who did not expe-rience complete elimination of migraine head-aches, the reduction in frequency was remark-able. Considering that 21 of 22 patients (95.5percent, p � 0.001) who were selected to un-dergo surgery on the basis of favorable re-sponse to Botox injection enjoyed a positiveoutcome from the surgery, it is logical to con-clude that Botox is an extremely reliable prog-nosticator of the surgical outcome for the treat-ment of migraine headaches.
Bahman Guyuron, M.D.29017 Cedar RoadCleveland, Ohio [email protected]
ACKNOWLEDGMENTS
The authors gratefully acknowledge the invaluable assis-tance from Saied Amini, Ph.D., M.B.A., J.D., in statisticalanalysis, and Bryan Michelow, M.D., in preparation of themanuscript.
REFERENCES
1. Stewart, W. F., Shechter, A., and Rasmussen, B. K. Mi-graine prevalence: A review of population-based stud-ies. Neurology 44 (6 Suppl. 4): S17, 1994.
2. Guyuron, B., Varghai, A., Michelow, B. J., Thomas, T.,and Davis, J. Corrugator supercilii muscle resectionand migraine headaches. Plast. Reconstr. Surg. 106: 429,2000.
3. Headache Classification Committee of the InternationalHeadache Society. Classification and diagnostic cri-teria for headache disorders, cranial neuralgias andfacial pain. Cephalalgia 8 (Suppl. 7): 1, 1988.
4. Guyuron, B. Corrugator supercilii resection throughblepharoplasty incision. Plast. Reconstr. Surg. 107: 604,2001.
5. Guyuron, B. Surgical Control of Migraine Headaches.Microsoft PowerPoint Presentation, 2001.
6. Stein, J. IHS: Surgery improves chronic cluster head-ache. Docguide July 2, 2001.
7. Kunkel, R. S., and Dohn, D. F. Surgical treatment ofchronic migrainous neuralgia. Cleve. Clin. Q. 41: 189,1974.
8. Horton, B. T., MacLean, A. R., and Craig, W. M. A newsyndrome of vascular headache: Results of treatment
with histamine. Preliminary report. Mayo Clin. Proc. 14:257, 1939.
9. Maxwell, R. E. Surgical control of chronic migrainousneuralgia by trigeminal ganglio-rhizolysis. J. Neurosurg.57: 459, 1982.
10. Miller, H. Pain in the face. Br. Med. J. 2: 577, 1968.11. Goetz, C., and Pappert, E. Textbook of Clinical Neurology.
Philadelphia: Saunders, 1999.12. Moskowitz, M. A. The neurobiology of vascular head
pain. Ann. Neurol. 16: 157, 1984.13. Williamson, D. J., and Hargreaves, R. J. Neurogenic
inflammation in the context of migraine. Microsc. Res.Tech. 53: 167, 2000.
14. Grosser, K., Oelkers, R., Hummel, T., et al. Olfactoryand trigeminal event-related potentials in migraine.Cephalalgia 20: 621, 2000.
15. de Tommasso, M., Guido, M., Libro, G., et al. The threeresponses of the blink reflex in adult and juvenilemigraine. Acta Neurol. Belg. 100: 96, 2000.
16. Moskowitz, M. The trigeminovascular system: Scientificbasis of migraine. Presented at the 49th Annual Meet-ing of the American Academy of Neurology, Boston,April 12–19, 1997.
17. Goadsby, P. J. Advances in the pharmacotherapy of mi-graine: How knowledge of pathophysiology is guidingdrug development. Drugs R. D. 2: 361, 1999.
18. Levine, H. Personal communication.19. Silberstein, S. D. Menstrual migraine. J. Womens Health
Gend. Based Med. 8: 919, 1999.20. Silberstein, S. D., and Lipton, R. B. Epidemiology of
migraine. Neuroepidemiology 12: 179, 1993.21. Binder, W., Brin, M. F., Blitzer, A., Schenrock, L., and
Diamond, B. Botulinum toxin type A (BTX-A) formigraine: An open label assessment. Mov. Disord. 13(Suppl. 2): 241, 1998.
22. Wheeler, A. H. Botulinum toxin A: Adjunctive therapyfor refractory headaches associated with pericranialmuscle tension. Headache 38: 468, 1998.
23. Jankovic, J., and Brin, M. F. Botulinum toxin: Historicalperspective and potential new indications. MuscleNerve Suppl. 6: S129, 1997.
24. Ward, T. Pericranial Injections of Two Dosages of BotulinumToxin Type A in the Prophylactic Treatment of Migraine.Rancho Mirage, Calif.: Annenberg Center for HealthSciences at Eisenhower, 2000.
25. Silberstein, S., Mathew, N., Saper, J., and Jenkins, S.Botulinum toxin type A as a migraine preventive treat-ment. Headache 40: 445, 2000.
26. The Use of Botulinum Toxin Type A for Headache Management.Rancho Mirage, Calif.: Annenberg Center for HealthSciences at Eisenhower, 2000.
27. Hohne-Zell, B., Galler, A., Schepp, W., et al. Functionalimportance of synaptobrevin and SNAP-25 duringexocytosis of histamine by rat gastric enterochromaf-fin-like cells. Endocrinology 138: 5518, 1997.
Vol. 109, No. 7 / SURGICAL TREATMENT OF MIGRAINE HEADACHES 2189





























