Embed Size (px)
DESCRIPTION
Surgical Oncology. Definition of Neoplasia. a disorder of cell growth in which there is a permanent and inherited change in cells resulting in a pathological proliferation of tissue. The Etiology of Cancer. Viruses(papilloma, Epstein-Barr, Hepatitis B, retroviruses,HIV) Radiation exposure - PowerPoint PPT Presentation
Citation preview
Definition of Neoplasia
• a disorder of cell growth in which there is a permanent and inherited change in cells resulting in a pathological proliferation of tissue.
The Etiology of Cancer
• Viruses(papilloma, Epstein-Barr,
• Hepatitis B, retroviruses,HIV)
• Radiation exposure
• Environmental industrial carcinogens
• Tobacco and alcohol consumption
• Genetic susceptibility syndromes
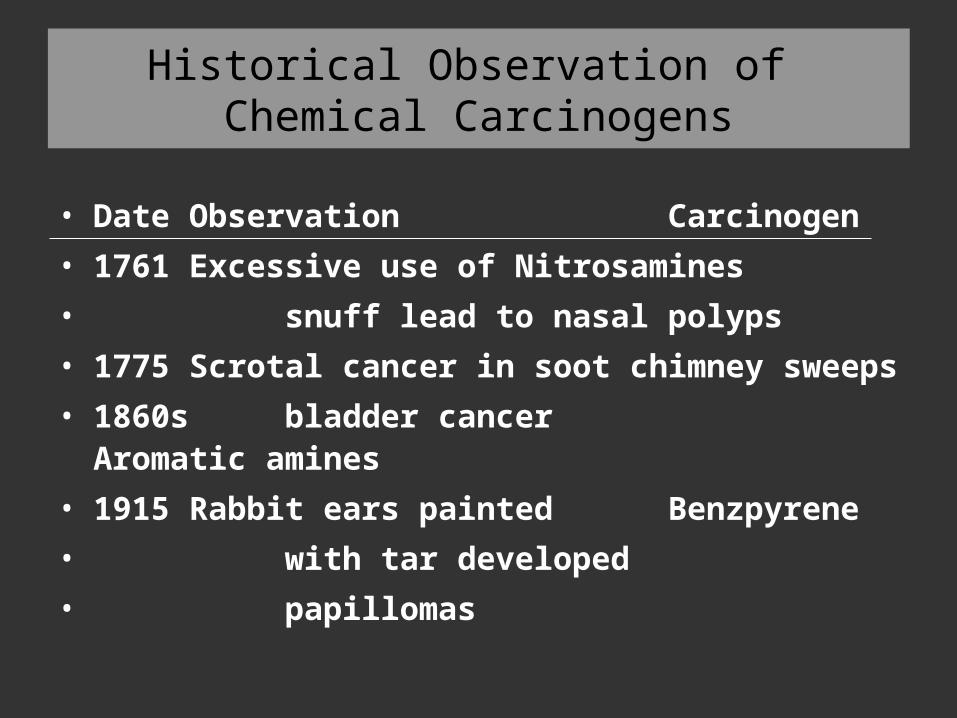
Historical Observation of Chemical Carcinogens
• Date Observation Carcinogen• 1761 Excessive use of Nitrosamines• snuff lead to nasal polyps• 1775 Scrotal cancer in soot chimney sweeps• 1860s bladder cancer Aromatic amines• 1915 Rabbit ears painted Benzpyrene• with tar developed • papillomas
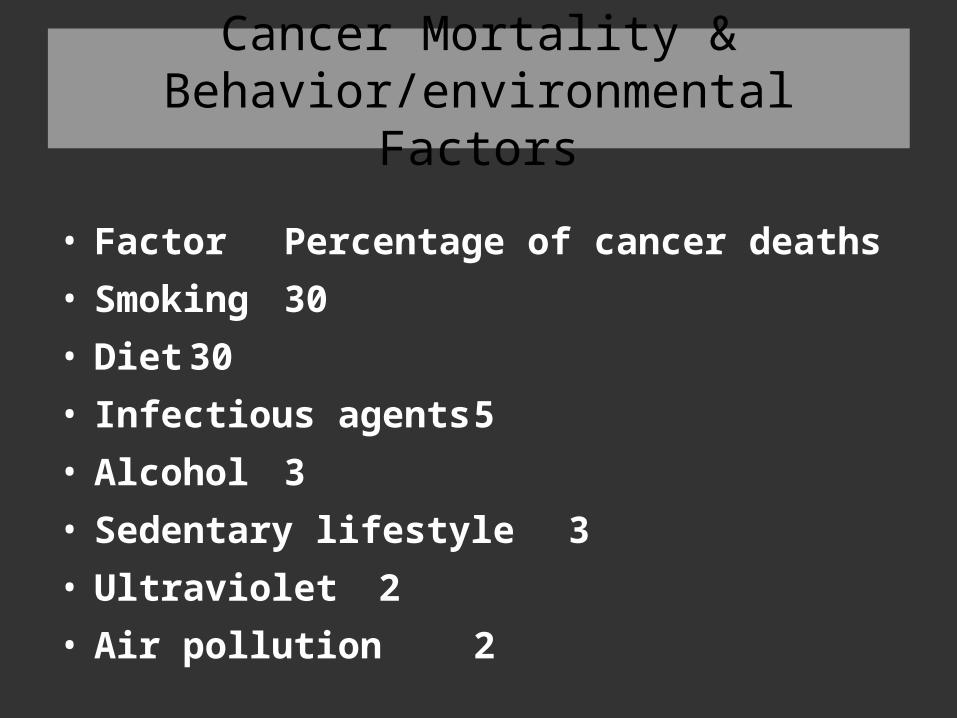
Cancer Mortality & Behavior/environmental Factors
• Factor Percentage of cancer deaths• Smoking 30• Diet 30• Infectious agents 5• Alcohol 3• Sedentary lifestyle 3• Ultraviolet 2• Air pollution 2
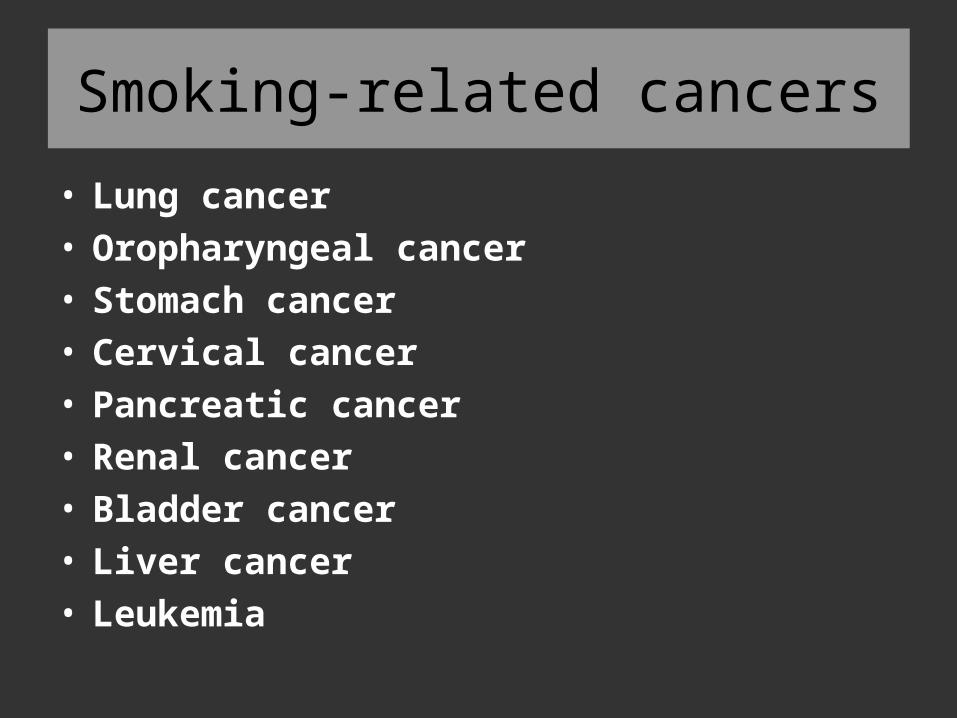
Smoking-related cancers
• Lung cancer• Oropharyngeal cancer• Stomach cancer • Cervical cancer• Pancreatic cancer• Renal cancer• Bladder cancer• Liver cancer • Leukemia
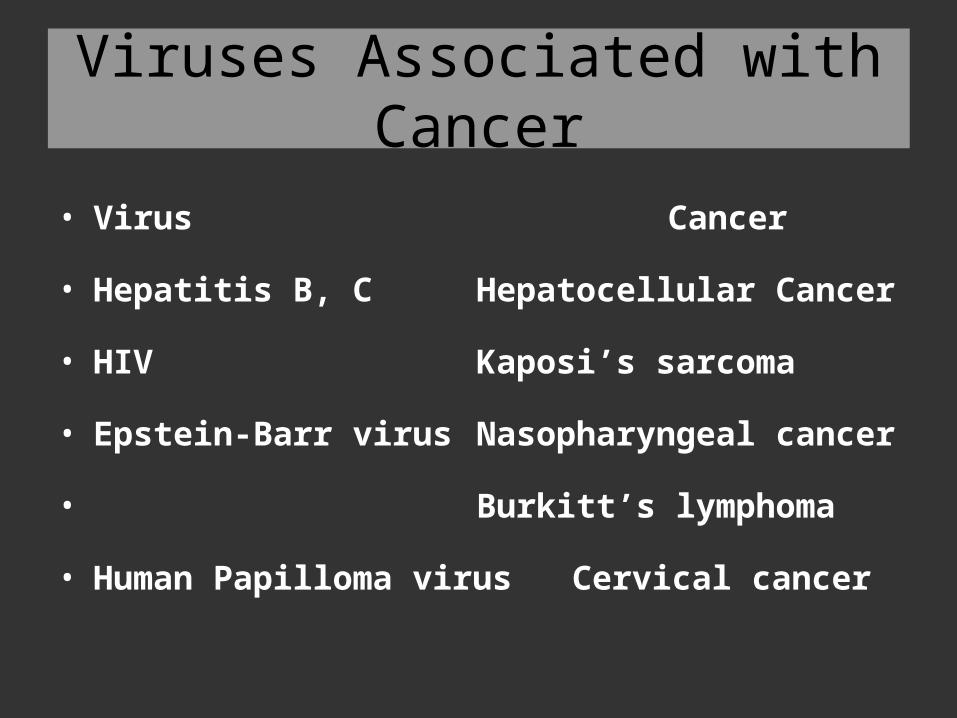
Viruses Associated with Cancer
• Virus Cancer
• Hepatitis B, C Hepatocellular Cancer
• HIV Kaposi’s sarcoma
• Epstein-Barr virus Nasopharyngeal cancer
• Burkitt’s lymphoma
• Human Papilloma virus Cervical cancer
Internal causes
• Hereditary susceptibility
• Endocrine factors
• Immune factors
Prevention• First step• etiology• Second step• early detection and treatment• Third step• improve quality of life
Major Genes in Development of Cancer
• Oncogenes
• Tumor suppressor genes
• DNA repair genes
Oncogenes
• Growth factorsEGF, TGF-α
• Growth factor receptorsEGFR, PTK
• Intracellular transducerscAMP
• Transcription factorsc-myc
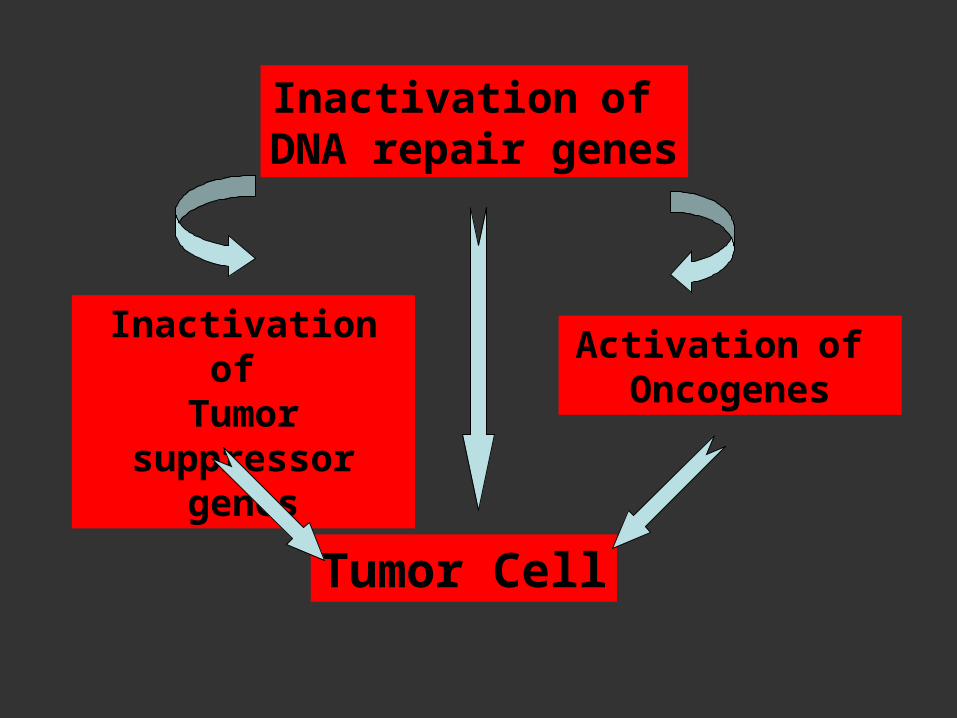
Inactivation of DNA repair genes
Inactivation of Tumor
suppressor genes
Activation of Oncogenes
Tumor Cell
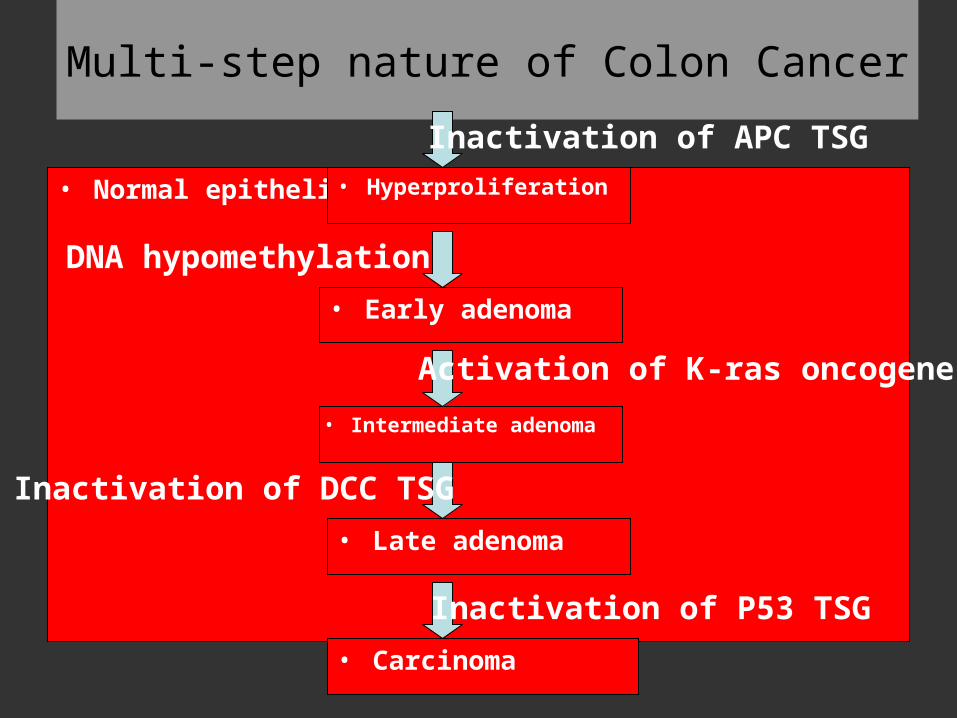
Multi-step nature of Colon Cancer
• Normal epithelium • Hyperproliferation
• Early adenoma
• Carcinoma
• Late adenoma
• Intermediate adenoma
Inactivation of APC TSG
DNA hypomethylation
Activation of K-ras oncogene
Inactivation of DCC TSG
Inactivation of P53 TSG
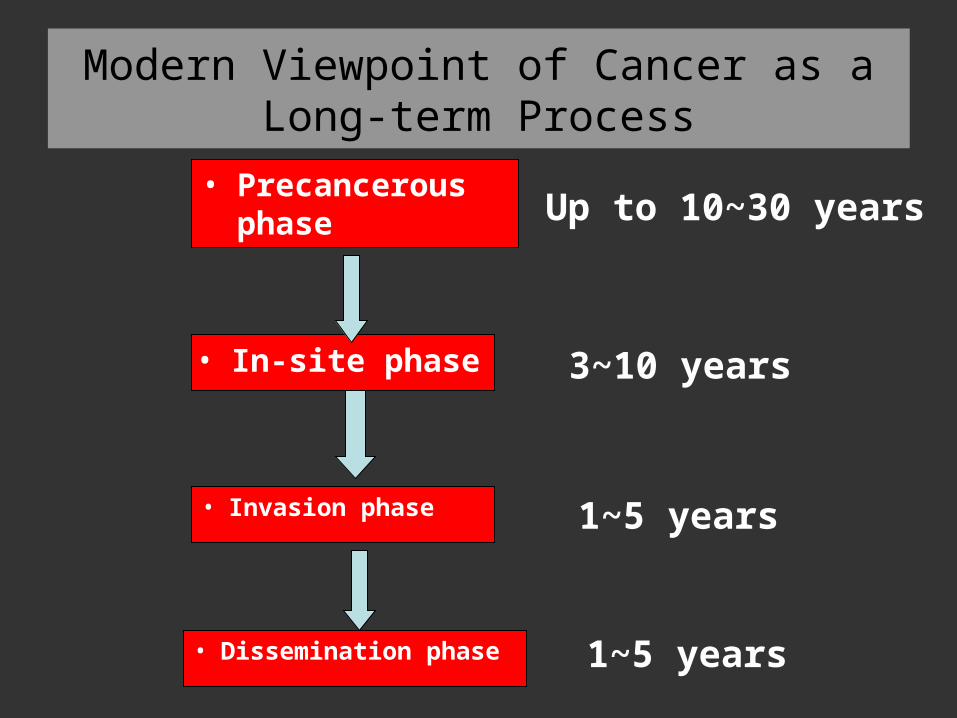
Modern Viewpoint of Cancer as a Long-term Process
• Precancerous phase
• Dissemination phase
• Invasion phase
• In-site phase
Up to 10~30 years
3~10 years
1~5 years
1~5 years
The classification and nomination of tumors
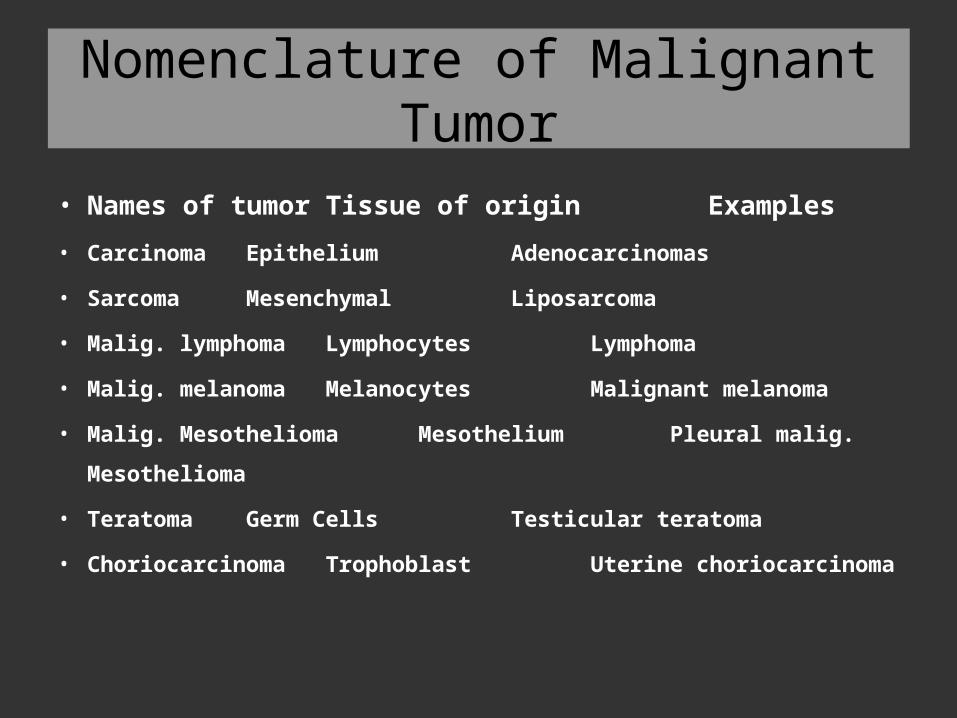
Nomenclature of Malignant Tumor
• Names of tumor Tissue of origin Examples• Carcinoma Epithelium Adenocarcinomas
• Sarcoma Mesenchymal Liposarcoma
• Malig. lymphoma Lymphocytes Lymphoma
• Malig. melanoma Melanocytes Malignant melanoma
• Malig. Mesothelioma Mesothelium Pleural malig.
Mesothelioma
• Teratoma Germ Cells Testicular teratoma
• Choriocarcinoma Trophoblast Uterine choriocarcinoma
Benign Tumors
• a limited growth potential
• the neoplastic cells closely resemble those
of the parent tissue ( well diff.)
• growing slowly by expansion
• a well-encapsulated lesion
• do not usually produce serious effect
Malignant Tumors
• proliferate rapidly• more poorly differentiated cells• progressive growth and invasion of the
surrounding tissues• metastases by lymphatic & blood vessels• if not treated early, eventually cause death
The Degree of Differentiation
• Well differentiated
• Moderately differentiated
• Poorly differentiated
The Objectives of Cancer Staging & Histological Classification
• to aid the clinician in planning of treatment
• to give some indication of prognosis
• to evaluate the efficiency of treatment
• to facilitate exchange of information
• to assist in continuing clinical studies of
cancer
Histopathological Staging & Classification
• Adenocarcinomas• Squamous carcinomas• Small cell carcinomas • Large cell carcinomas• Sarcomas Lymphomas• Leukemias Gliomas• Seminomas Teratomas
The Hallmark of Malignancy
• Local Destructive Invasion• Distant Metastasis
• ------ the cardinal behavior to distinguish benign & malignant tumor
Pathological Features of Malignancy
• ● an infiltrative uncapsulated margin
• ● invasion of baseline membrane or
surrounding structure
• ● evidence of invasion of blood vessels or
lymphatics or metastases
• ● tumor necrosis
Pathological Features of Malignancy
• ● architecture abnormalities
• e.g. increased gland/stroma ratio
• ● cytological abnormalities
• e.g. increased nuclear/cytoplasm ratio
• ● numerous mitotic figures & abnormal
mitoses
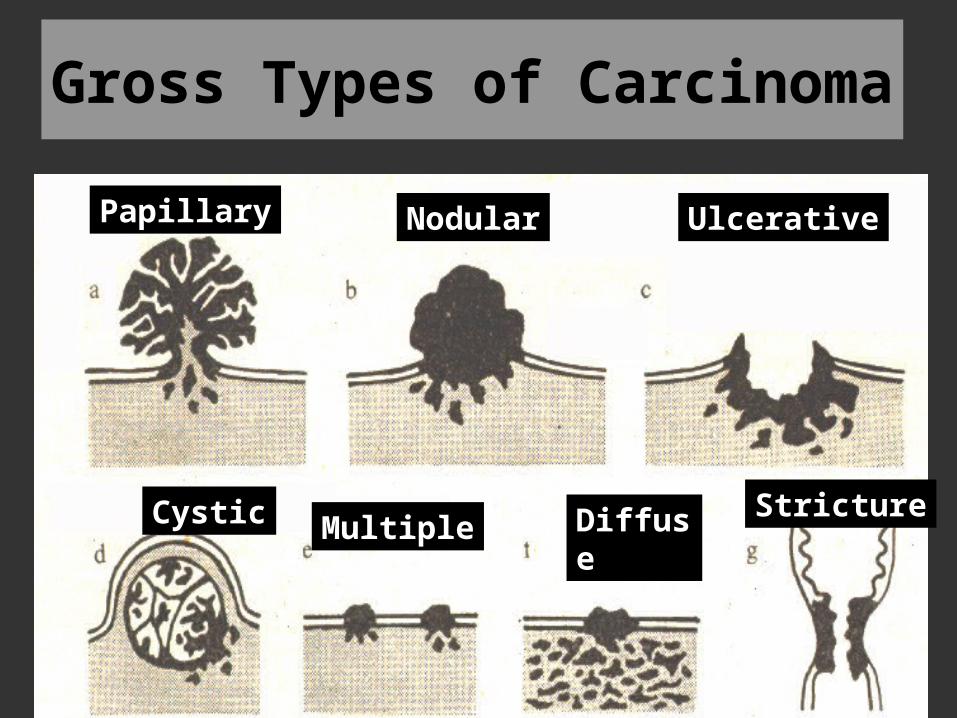
Papillary Nodular Ulcerative
Cystic Multiple Diffuse Stricture
Gross Types of Carcinoma
• Two Terms• Metaplasia
---- the replacement of one fully differentiated tissue by another
• Carcinoma in situ
the histological abnormalities are sufficiently severe to suggest carcinoma , but in the absence of basement membrane invasion
Effects of Malignancy
• Tumor arising within a hollow viscus
• obstruction
• Tumor arising from surface of organ
• ulceration and bleeding
Spread of Malignant Tumors
• Direct invasion--- Rectal cancer
• Lymphatic system to local lymph nodes
• -- Breast carcinoma, Gastric cancer
• Bloodstream to distant organs
• -- Liver, lung & brain
• Across body cavities
• -- Ovarian carcinoma
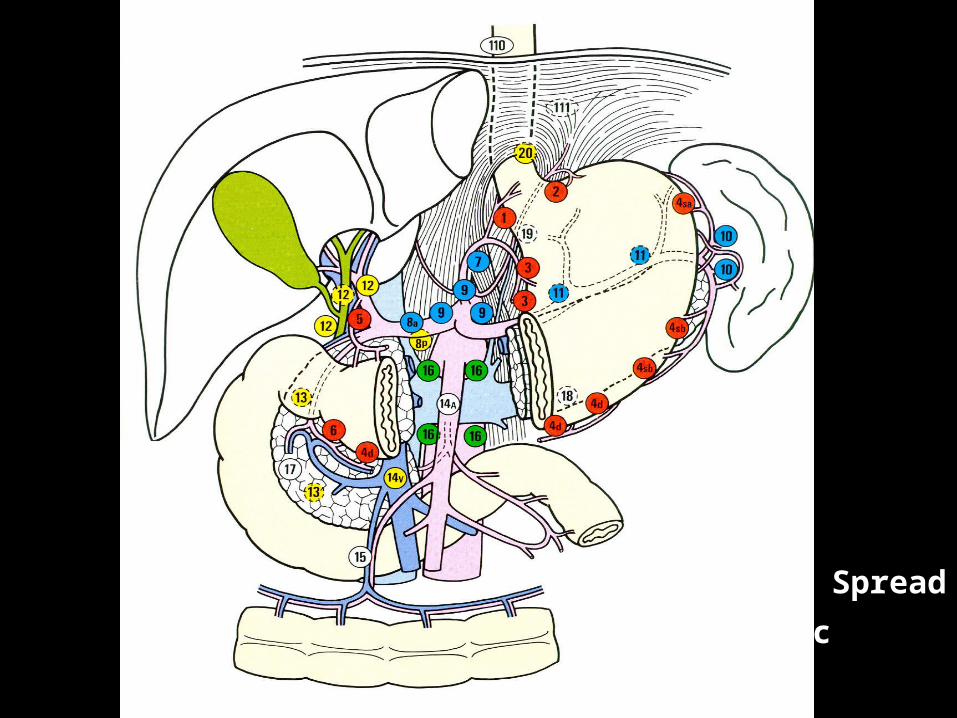
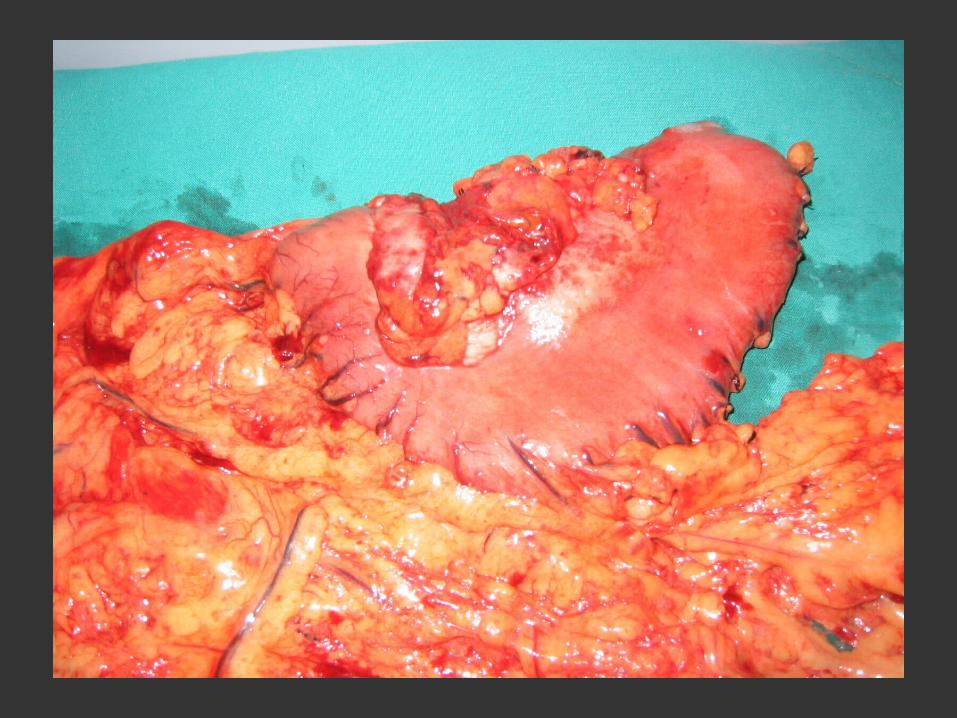
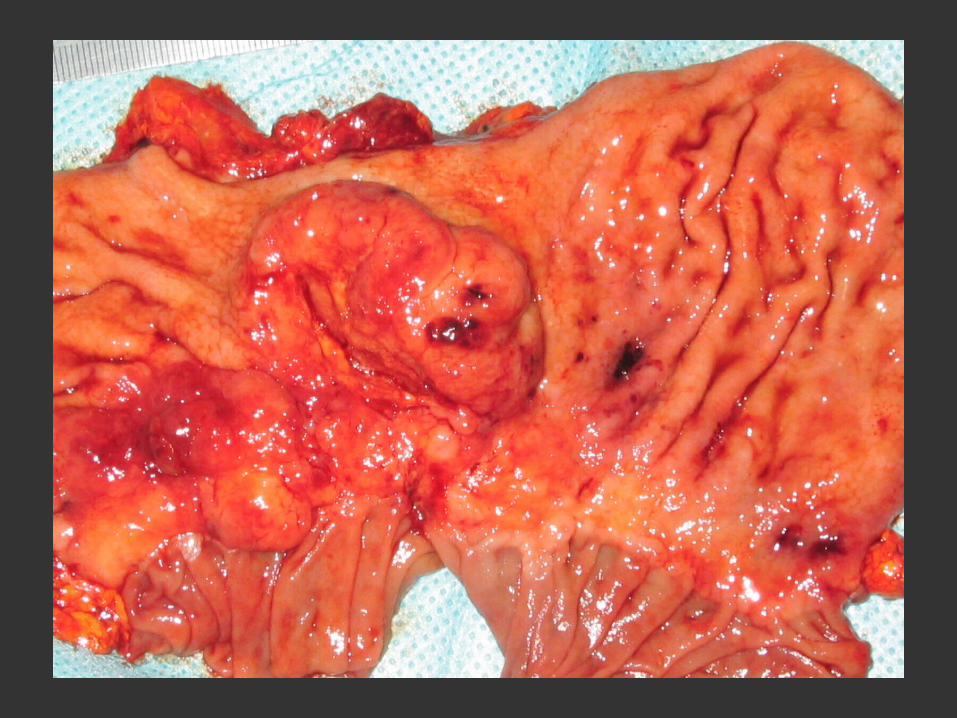
Lymphatic Spread of Gastric Cancer
Diagnosis• History
• Physical Examination
• Laboratory Tests
• Specific Procedures
Symptoms or Signs of Cancer
• Alteration in eating habit• Loss of appetite• Problems in swallowing• Change in bowel habit• The presence of a lump at any site
Symptoms or Signs of Cancer
• The appearance of bleeding• Unexplained recurrent pain• Recurrent fevers• Unexplained weight loss• Repeated infections which do not clear
with treatment

Breast Cancer
Para-neoplastic Syndrome
• Small cell carcinomas secret ACTH• Cushing’s syndrome
Renal carcinomas secret erythropoitin• polycythaemia• Mucin-secreting adenomas increasing the
coagulability • thromboembolism
The Diagnostic Procedures of Cancer
• History
• Family History Individual Habits
• Social History Occupation
• Marital & Sex History Past History
The Diagnostic Procedures of Cancer
• Physical Examination
• Systemic
• Local
• Tumor
• Metastatic foci
The Diagnostic Procedures of Cancer
• Special Procedures• ● Diagnostic Radiology• Chest X-rays• Barium enema radiography• Gastro-intestinal series radiography• Arteriography• Computerized tomography(CT)• Radioisotope scanning techniques• Mammography• Positron emission tomography(PET)
The Diagnostic Procedures of Cancer
• Special Procedures• Ultrasonic examination• Endoscopy• Cytology• Biopsy bone-marrow biopsy• needle biopsy• endoscopic biopsy• Magnetic resonance imagine(MRI)
The Diagnostic Procedures of Cancer
• Lab Test• ● Routine test: blood, urine, stool• ● Serum test: enzyme, hormone• glycoprotein, tumor markers • ● Immunology test: AFP, CEA, • tumor-related antigens• ● Flow-cytometry(FCM): DNA ploidy• DNA index• ● Gene Test: Oncogenes, DNA repair gens• Tumor suppressor genes
Tools For Early Clinical Detection
• ● Complete physical examination
• ● Regular mammography and breast self exam
• ● Haemoccult for occult blood in feces
• ● Urine analysis and blood count
• ● A complete clinical history
• ● An in-depth family medical history
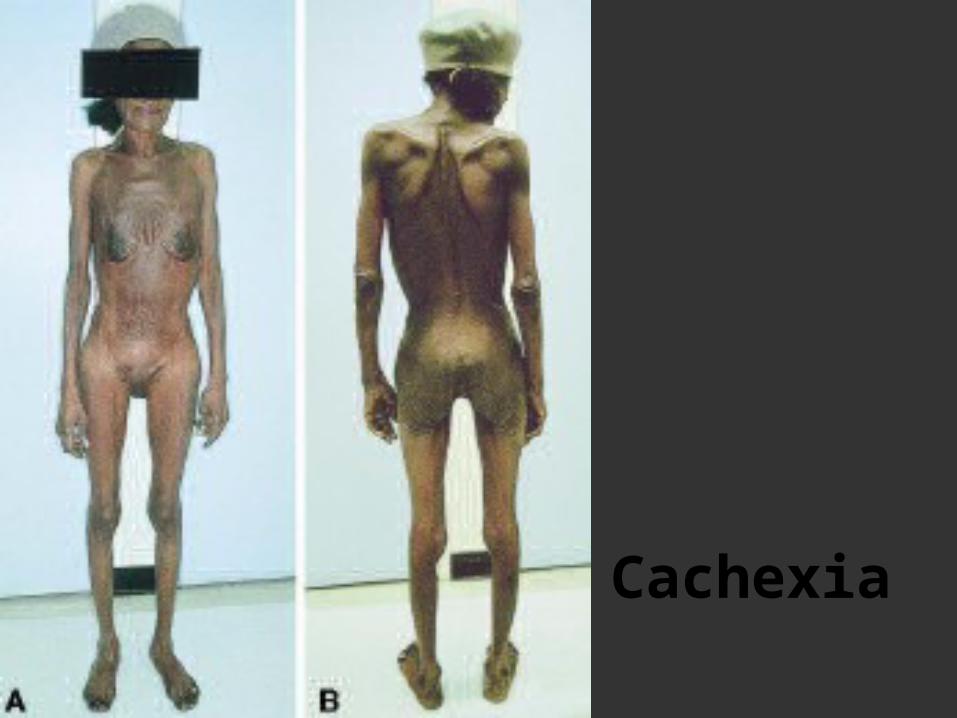
Cachexia
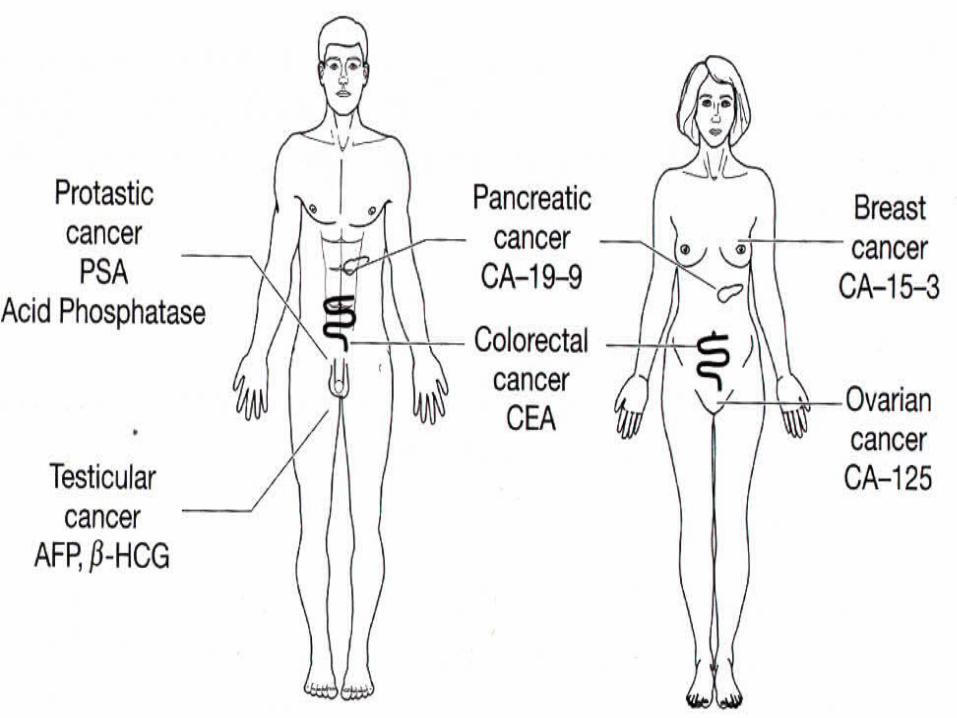
Tumor Markers
• Tumor marker Examples
• Tumor antigens AFP, CEA
• Enzymes PSA
• Hormones β-HCG
• Oncogenes Ras, c-myc,P53
• Tumor associated antigens
• CA 19-9,CA-242
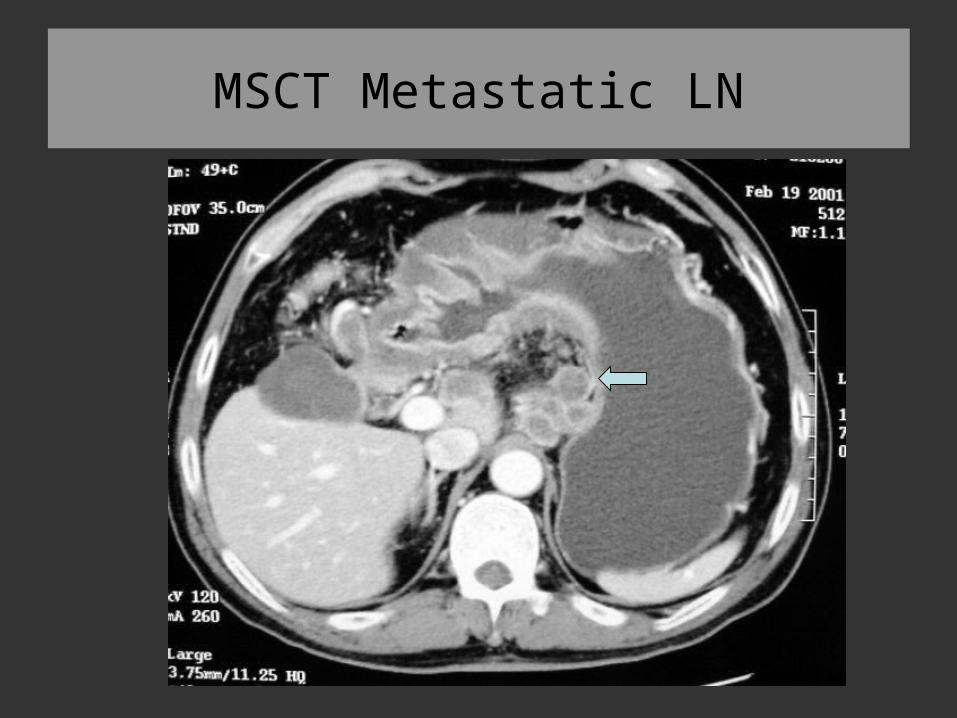
MSCT Metastatic LN

Endoscopic Ultrasonography
TNM staging
• T--- primary tumor
• N--- regional lymph node
• M--- metastases
The Principles of Cancer Surgery
Loeb’s Rules of Therapeutics
• ● If what you are doing is doing good, keep doing it.
• ● If what you are doing is not doing good, stop doing it.
• ● If you do not know what to do, doing nothing.• ● Never make the treatment worse than the
disease.
Oncology Multidisciplinary Team
• ● Surgical oncologists• ● Radiation oncologists • ● Medical oncologists• ● Palliative care specialists• ● Psychologists• ● Social workers• ● Nurses• ● Chaplains
Landmark advances in Surgical Oncology
• Year Event Surgeon• 1809 Elective oophorectomy P. Pott• 1846 Ether as anesthesia J. C.Warren• 1867 Carbolic acid as antisepsis Joseph. Lister• 1873 Laryngectomy A. T. Billroth• 1878 Resection of rectal tumor R.von Volkman• 1881 Gastrectomy A. T. Billroth• 1890 Radical mastectomy W.S. Halstead• 1908 Abdominoperineal resection W. E. Miles• 1909 Thyroid Surgery T. M. Kocher• 1935 Pancreaticoduodenectomy A.O.Whipple
Surgical Oncology
• ● Preventive surgery• ● Diagnostic surgery• Resection biopsy• Sample biopsy• Laparotomy•
Surgical Oncology•● Radical operation• Lumpectomy• Extended resection• Radical or Extended • radical operation
Surgical Oncology
•● Palliative Surgery• Palliative resection• Bypass or Ostomy• Endocrine glands resection• Cytoreductive surgery
Surgical Oncology• ● Surgery for recurrence • or metastasis• ● Reconstruction and recovery• ● Surgical oncology technique• non-cutting • en-bloc• non-touching
The Principles of Cancer Surgery
• ● Staging• ● Clinical staging• ● Imaging--preoperative• ● Fine needle aspiration--preoperative• ● Intra-operative imaging• ● Intra-operative pathology• ● Resection specimen
Key Points of Cancer Surgery
• ● Combined treatment modalities
• ● Preoperative chemotherapy--breast
• ● Postoperative chemotherapy--breast, colon
• ● Preoperative radiotherapy--rectum
• ● Postoperative radiotherapy
• --lung, breast, rectum
Cancer Treatment are Based Upon
• ● the biological behavior of the cancer• ● the mortality and morbidity of therapeutic
procedures• ● the efficacy of the therapeutic procedure• ● the performance status of the patient
Cancer Treatment are Based Upon
• ● with localized cancers are curable
• ● presenting with positive Lymph Nodes tend to bad outcome
• ● with distant metastases are rarely curable
• ● the most commonly parameters to measure survival and benefit of treatment
• --5-yr survival rates
Chemotherapy
• Indication:•● Tumors with priority • to chemotherapy•● Tumors controlled for long time•● Adjuvant chemotherapy
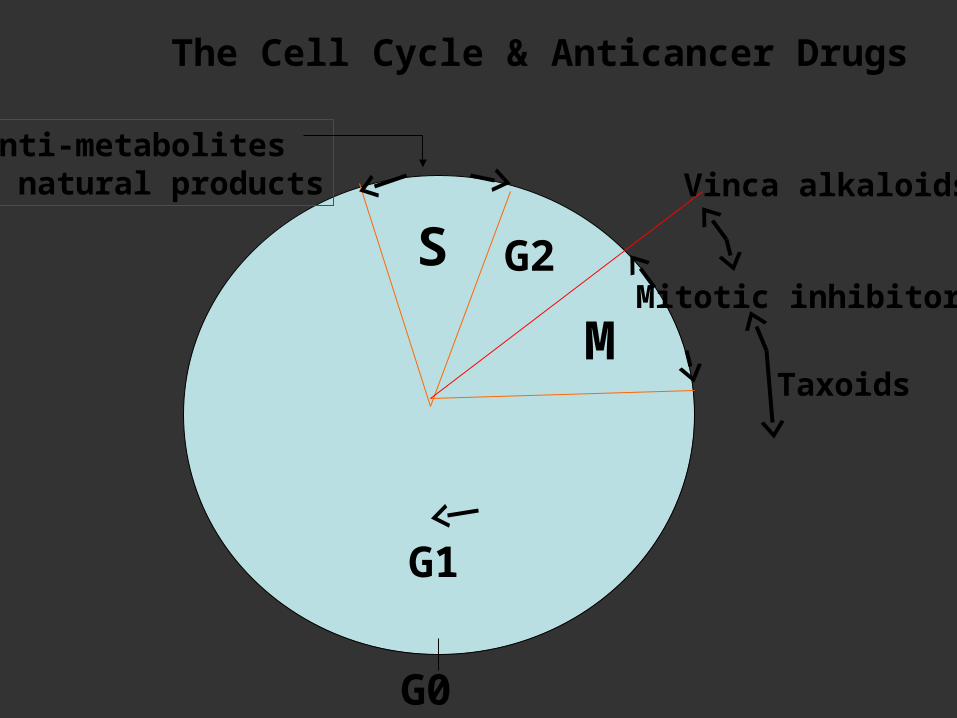
S G2
M
G1
G0
The Cell Cycle & Anticancer Drugs
Anti-metabolites& natural products
Mitotic inhibitors
Vinca alkaloids
Taxoids
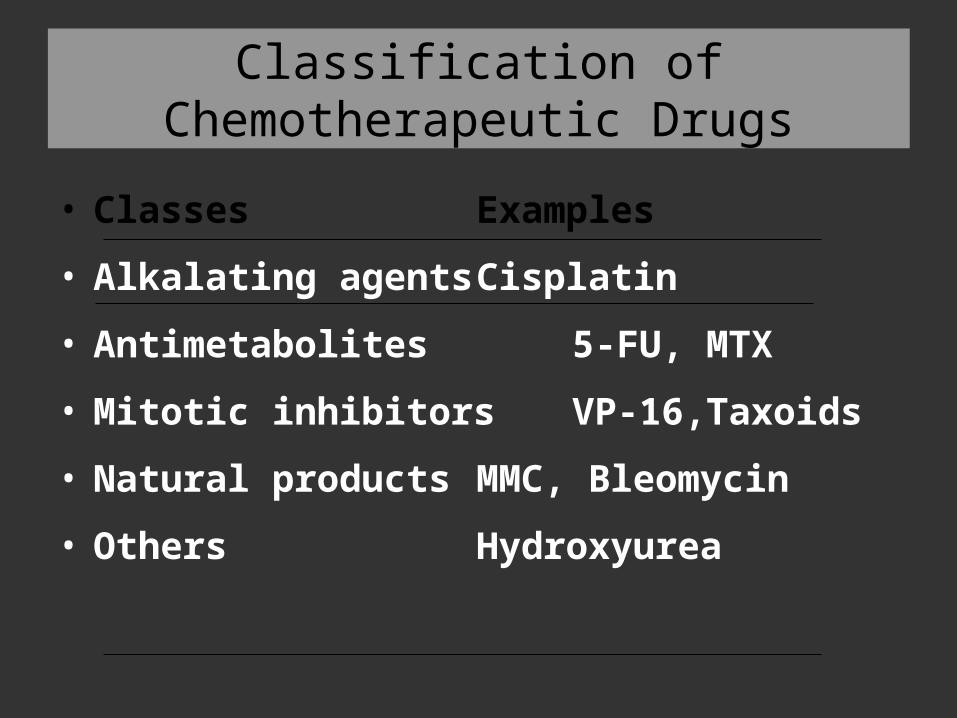
Classification of Chemotherapeutic Drugs
• Classes Examples• Alkalating agents Cisplatin• Antimetabolites 5-FU, MTX• Mitotic inhibitors VP-16,Taxoids• Natural products MMC, Bleomycin• Others Hydroxyurea
• Adjuvant therapy• Administration of systemic therapy after
optimal loco-regional therapy (surgery/ radiotherapy)
• Neo-adjuvant therapy• Chemotherapy/Radiotherapy is administered
prior to loco-regional therapy to reduce the tumor cell burden
Resistance to Chemotherapy
• ● Decreased drug-activating enzymes
• ● Increased drug-inactivating enzymes
• ● Increased DNA repair
• ● Mutations in drug targets
• ● Excretion of drug out of the cells
Chemotherapy-induced Toxicities
• ● Bone marrow suppression• ● Immunosuppression• ● Nausea and vomiting• ● Alopecia• ● Renal , pulmonary toxicity• ● Cardiotoxicity• ● Neurotoxicity• ● Gonadal damage and sterility
New Approaches of Chemotherapy
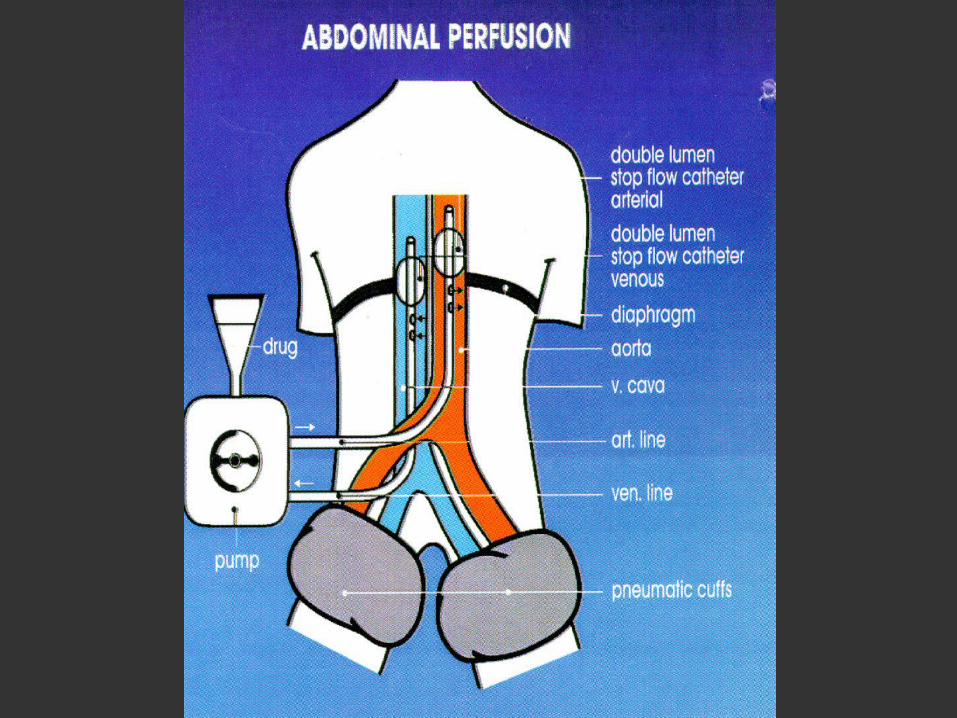
• ● New drug• --- Taxol, Topo 11Inhibitors…• ● Biomodulation• --- Leucovorin/5-FU• ● Peri-operative chemotherapy• ---Neoadjuvant chemotherapy• ● Loco-regional chemotherapy• --- IPHC , Stop-flow Technique
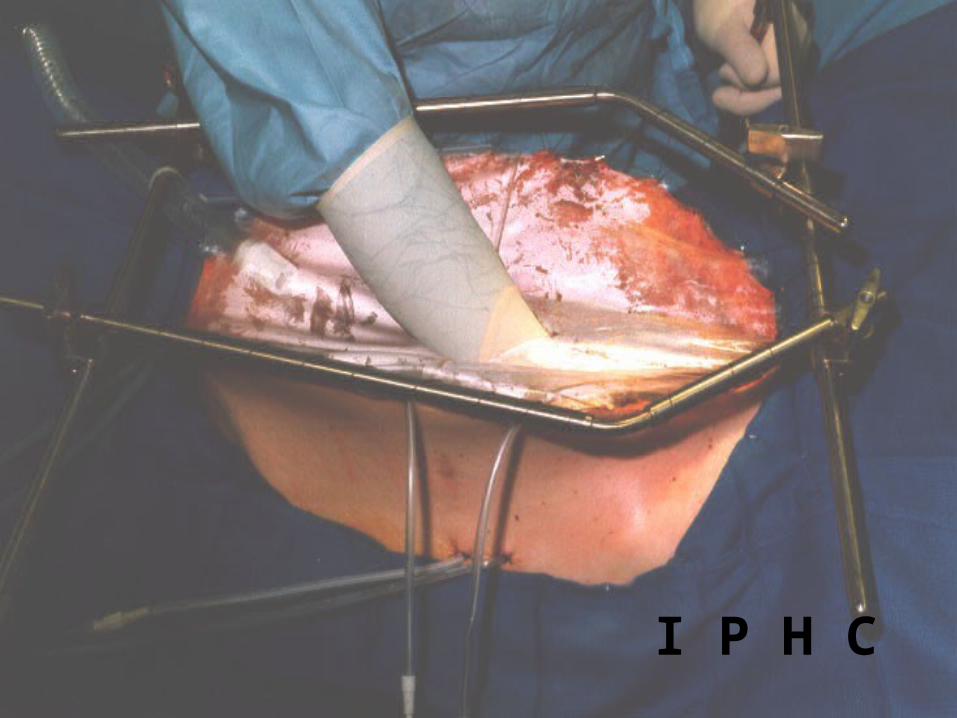
I P H C
New Approaches to Cancer
• ● Immunology• ● Biological response modifiers• ● Interferons and interleukins• ● Adoptive immunotherapy• ● Monoclonal antibodies• ● Tumor vaccines• ● Gene therapy
The Principles of Radiotherapy

Historical Perspective of Radiotherapy
• ● Roentgen described x-rays in 1895
• ● The Curies discovered radium in 1898
• ● The first patient receive radiotherapy in
1896
• ● Clinical radiation therapy as a medical
discipline in 1922
A Linear Accelerator
Radiotherapy Planning Process
• ● Pre-planning• TNM staging• Radical vs palliative intent• ● Treatment planning• description of treatment• patient immobilization• definition of tumor volumes• technique and beam modification• calculation of dose distribution
Radiotherapy Planning Process
• ● Treatment delivery
• dose prescription
• implementation of treatment
• verification
• monitoring treatment
• ● Outcome
Skin & Soft Tissue Tumors
Cell Types in the Skin
• Epidermis• Squamous• Basal• Melanocytes• Langerhans---Immunological, no tumors• Dermis• Connective tissue--blood vessels,
lymphatics, nerve supply• Appendages--hair follicles & glands
Etiology of Skin Tumors
• ● Ultraviolet (UV) light
• ● Genetics
• ● Atrophic skin lesions
• ● Chemical carcinogens
• ● Radiation exposure
• ● Immunosuppression
Common Malignancies of Skin
• ● Basal cell carcinoma
• ● Squamous cell carcinoma
• ● Paget’s disease
• ● Skin Metastasis
Common Superficial Tumor or lump
• ● Pigment nevus• ● Melanoma• ● Lipoma• ● Fibroxanthoma• ● Dermatofibrosarcoma protuberance• ● Desmoid fibromatosis
Common Superficial Tumor or lump
• ● Schwannoma• ● Neurofibroma• ● Hemangioma capillanisum• ● Hemangioma cavernosum• ● Hemangioma racemosum
Common Superficial Tumor or lump
• ● Dermoid cyst• ● Sebaceous cyst• ● Epidermoid cyst• ● Synovial cyst


Squamous cell carcinoma