Embed Size (px)
Citation preview
Volume 27 Number 5, Part 1 November 1992 Brief communications 775
If I I
Surface microscopy in the diagnosis of micropapular cutaneous metastatic melanoma
Bryan K. Pang, MBBS, and Steven Kossard, PhD Sydney, Australia
Epiluminescence microscopy, with a stereomicro- scope and immersion oi/, renders the epidermis translucent and permits the examination and local- ization of pigmented skin lesions from the level of the epidermis to the dermis. 1 The technique provides a variety of clues that aid in the differential diagnosis of pigmented skin lesions. In a recent study of more than 3000 pigmented skin lesions, morphologic cri- teria were defined 2 for various pigmented lesions, and the authors reported a significant improvement in their diagnostic accuracy. 3 More recently, an in- expensive hand-held instrument based on the same principle of skin surface microscopy has been devel- oped and is being widely used for the study of cuta- neous lesions. 4 This article illustrates that skin sur- face microscopy is helpful in the diagnosis of cuta- neous metastatic melanoma.
CASE REPORT
In 1977, a 58-year-old white man reported a dark "mole" of unknown duration on his left shoulder. Exam- ination revealed an 8 X 10 mm, darkly pigmented lesion with an irregular margin, and a 1.5 mm smaller pig- mented lesion, approximately 6 mm distant from the main lesion. Both were excised. Histopathologic exami- nation showed that the larger lesion was a malignant melanoma, Clark level III, 0.4 mm in depth to the level of subpapillary vascular plexus. The smaller lesion was reported to be a second primary melanoma arising from a focus of lentigo maligna with a maximal thickness of 0.15 mrn. One month later, a left axillary lymphadenec- tomy was performed with no histopathologic evidence of metastatic melanoma.
From November 1985 to September 1991, this patient was seen at 3- to &month intervals and on each of these follow-up visits, three to five small new darkly pigmented papules, measuring 1 to 3 mm in diameter, were noted mainly on the left anterior chest wall but also on the right anterior chest wall and right shoulder. Studies failed to reveal other evidence of metastatic disease.
Histopathologic examination of most of the deeply pigmented papules showed metastatic melanoma, but
From the Skin and Cancer Foundation.
No reprints available.
16/54/38791
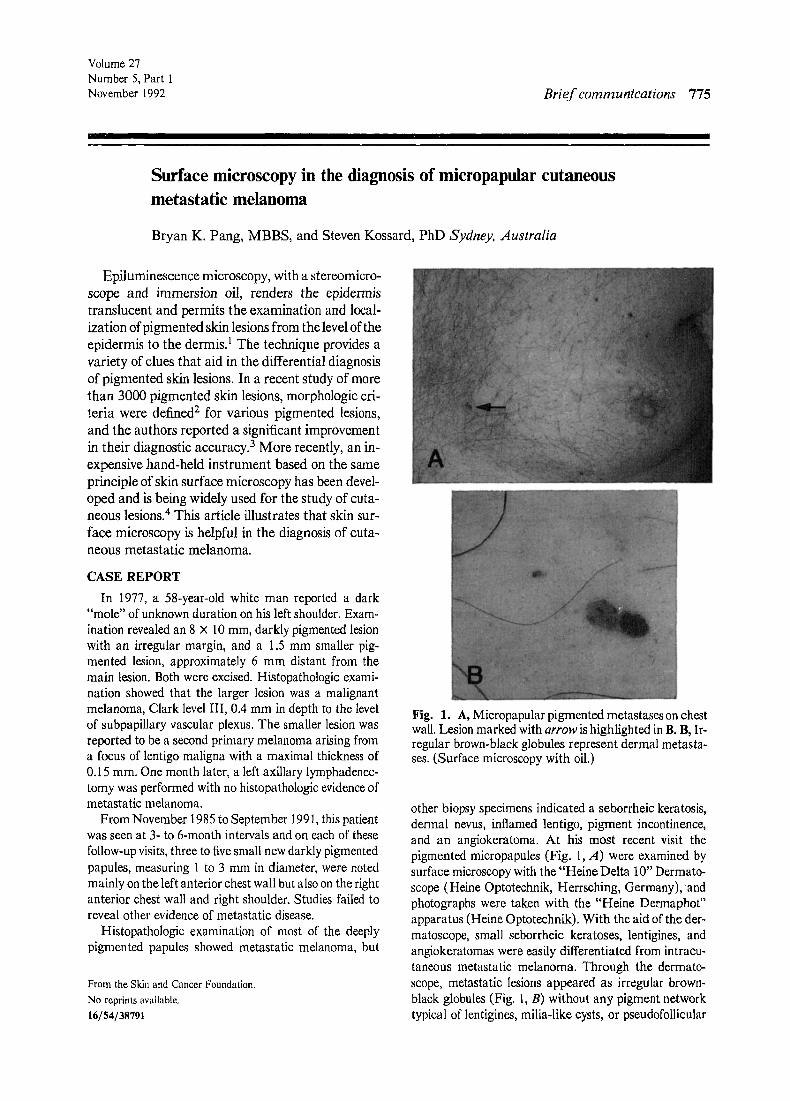
Fig. 1. A, Micropapular pigmented metastases on chest wall. Lesion marked with arrow is highlighted in B. B, Ir- regular brown-black globules represent dermal metasta- ses. (Surface microscopy with oil.)
other biopsy specimens indicated a seborrheic keratosis, dermal nevus, inflamed lentigo, pigment incontinence, and an angiokeratoma. At his most recent visit the pigmented micropapules (Fig. 1, A) were examined by surface microscopy with the "Heine Delta 10" Dermato- scope (Heine Optotechnik, Herrsching, Germany), and photographs were taken with the "Heine Dermaphot" apparatus (Heine Optotechnik). With the aid of the der- matoscope, small seborrheic keratoses, lentigines, and angiokeratomas were easily differentiated from intraeu- taneous metastatic melanoma. Through the dermato- scope, metastatic lesions appeared as irregular brown- black globules (Fig. 1, B) without any pigment network typical of lentigines, milia-like cysts, or pseudofollicular

776 Brief cornrnunications
Journal or the American Academy of
Dermatol%y
Fig. 2. Clusters of pleomorphic melanocytes in dermis represent metastases. (Hematoxylin-eosin stain; •
openings typical of seborrheic keratoses or engorged ves- sels typical o f angiokeratoma. Histologic evaluation of the pigmented lesions selected for removal after surface mi- croscopy revealed an epidermis of irregular thickness un- der which there were clusters of pigmented melanocytes with nuclear pleomorphism, forming large aggregates within the papillary dermis. These represented intracuta- neous metastatic melanoma (Fig. 2).
DISCUSSION
In a study by Curley et al. 5 of 116 pigmented le- sions, only 50% were diagnosed correctly by experi- enced dermatologists. To aid in diagnosis, Doppler sonography, 6 three-dimensional nevoscopy, 7 com- puterized digital imaging processing 8 for primary melanomas, and immunoscintigraphy with radioac- tive-labeled monoclonal antibodies 9 for metastatic disease have been developed. However, most of these are in the investigational stage, require experienced personnel, are not readily available, and are imprac- tical for general use in the diagnosis of melanomas. With defined morphologic criteria, skin surface mi- croscopy was shown to improve the diagnostic accu- racy of most pigmented lesions significantly. 2, 3 In recent reviews 2, 3, 10 the surface microscopic mor- phology of most pigmented lesions has been defined and illustrated, but the appearance of micropapular intracutaneous metastatic melanoma was not in- cluded. Cutaneous pigmented lesions, when small and intensely pigmented, may provide difficulties in
diagnosis. They may represent a lentigo, a vascular lesion such as angiokeratoma, a minute seborrheic keratosis, a pigmented basal cell carcinoma, or even foreign pigment such as a tattoo. With the aid of surface microscopy, these lesions can be differenti- ated. In our case, we found that this technique was useful and even small darkly pigmented papules measuring 1 to 3 mm in diameter of intracutaneous metastatic melanoma could be recognized.
The cutaneous secondaries showed asymmetric brown-black globules and lacked the irregular pig- ment network, radial streaming, pigmented pseudo- pods, or black dots associated with primary mela- noma. However, the surface microscopic appear- ance of these melanoma metastases is unlikely to be specific and their appearance would probably be shared by some forms of pigmented dermal nevi. Nonetheless, in the context of newly developing le- sions, particularly when they are asymmetric, the finding can be helpful.
This patient remains well despite a 6-year history of recurrent cutaneous metastases. We have elected to excise all micrometastases. Surface microscopy provides a practical and valuable diagnostic tool for their recognition.
REFERENCES
1. MacKie R. An aid to the preoperative assessment of pigmented lesions of the skin. Br J Dermatol 197 I;85:232-8.
2. Pehamberger H, Steiner A, Wolff K. In vivo epilumines- cence microscopy of pigmented skin lesions. I. Pattern analysis of pigmented skin lesions. J AM ACAD DERMATOL 1987;17:571-83.
3. Steiner A, Pehamberger H, Wolff K. In vivo epilumines- cence microscopy of pigmented skin lesions. I[. Diagnosis of small pigmented lesions and early detection of malignant melanoma. J AM ACAD DERMATOL 1987;17:584-91.
4. Stolz W, Bilek P, Landthalen M. Skin surface microscopy. Lancet 1989;2:864-5.
5. Curley R, Marsden R, Fallowfield M. Diagnostic accuracy in the cfinical evaluation of melanocytic lesions. Br J Der- matot 1988;l19(suppl 33):34-5.
6. Srivastava A, Hughes L, Woodcock J, et aL Vascularity in cutaneous melanoma detected by Doppler sonography and histology. Br J Cancer 1989;59:89-91.
7. Dhawan A. Early detection of cutaneous malignant mela- noma by three-dimensional nevoscopy. Comput Methods Progr Biomed 1985;21:59-68.
8, Murray A, Neill S, Harland C, et al. A new method for the quantification of physical change in unstable pigmented le- sions using digital image processing techniques. Br J Der- matol 1988;199(suppl 33):45.
9. Mechl Z, Bauer J. The detection of metastases. In: Cas- cinelli N, Santinami M, Veronesi U, eds. Cutaneous mel- anoma biology and management. Milano: Masson, 1990: 218-9.
10. Bahmer F, Fritsch P, Kreusch J, et al. Terminology in sur- face microscopy. J AM ACAD DERMATOL 1990;23:1159- 62.





























![Case Report A Rare Case of Metastatic Malignant Melanoma ...downloads.hindawi.com/journals/crigm/2014/312902.pdf · metastatic malignant melanoma of the GI tract [ ]. In fact, Wysocki](https://img.dokumen.tips/doc/110x75/5f9b841cf1457c0af634448c/case-report-a-rare-case-of-metastatic-malignant-melanoma-metastatic-malignant.jpg)