Embed Size (px)
Citation preview

I I
CLINICAL NUTRITION CASES
SULFASALAZINE INHIBITS FOLATE ABSORPTION
Anemia has long been associated with in- flammatory bowel disease (IBD).1-4 The early reports of anemia in ulcerative colitis cited the chronic blood loss, hemorrhagic episodes, disturbed gastrointestinal (GI) motility, chronic sepsis, and anorexia as factors causing depressed erythropoiesis. About half the patients studied had hemo- globin levels below 11 g/dI. In the study by Beal and coworkers,’ 26 of 32 patients were iron-deficient, but none was vitamin B,,-deficient. Omerod2 concluded from a review of the literature, a survey of past ad- missions to a hospital in London, and an intensive study of 28 inpatients that iron deficiency was the overriding cause of ane- mia in ulcerative colitis. In 14 of these pa- tients, however, four had low or subnormal levels of plasma folate. In contrast, a report by Hoffbrand et a13 noted that the anemia in 64 cases of Crohn’s disease was principally macrocytic and was attributed to folic acid deficiency. Vitamin B,, deficiency was un- common in these patients and occurred only when they had resection of the small bowel. Andersson and colleagues4 re- ported that half of a series of 52 patients with Crohn’s disease in Goteborg, Sweden, had serum folates less than 3 ng/ml and 25 percent of a parallel series of 25 patients with ulcerative colitis had similarly low values of serum folate.
It is now recognized that all patients with IBD are at risk for folate deficiency. Despite the fact that folate is absorbed principally in the jejunum and IBD affects principally the terminal ileum, colon, and rectum, fo- late malabsorption does occur in a sizable proportion of cases with IBD. Franklin and R~senberg ,~ moreover, have shown that the malabsorption of folate is not only an- other facet of jejunal dysfunction in IBD, but that this malabsorption is worsened by
sulfasalazine, a drug frequently used in the treatment of IBD. Prednisone had no such effect.
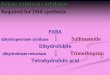
Sulfasalazine is composed of an antibi- otic sulfapyridine linked via an azo group to 5-aminosalicylate (Figure 1). This com- pound is not absorbed in the stomach or upper small intestine, passes into the distal small intestine and colon, and is split by bacteria. Sulfapyridine is absorbed and ex- creted in the urine, but the salicylate moiety remains in the colon and is excreted in the stool. The effectiveness of sulfasala- zine in ulcerative colitis is attributed on the anti-inflammatory action of the salicylate moiety rather than to the antimicrobial ef- fect of sulfapyridine, although both may contribute.
The case to be presented is one of a series of patients with ulcerative colitis in whom folate absorption, both before and after sulfasalazine administration, was studied by Franklin and R~senberg .~
Case A 53-year-old man with a 10-year history of ul-
cerative colitis with abdominal pain, fever, weight loss, and bloody diarrhea was admitted to Billings Hospital of the University of Chicago. The onset of his disease was characterized by intermittent symptoms of diarrhea (five to ten semiformed stools per day) interspersed with periods of normal or near-normal health. The disease had progressed to include episodes of fever and weight loss. There was no involvement of the ascending colon or the small bowel, and no evidence of carcinomatous change was ob- served. He was maintained on prednisone and sulfasalazine.
On physical examination the patient pre- sented as a thin, well-developed, well-nourished middle-aged man 5’10 (178 cm) tall and weigh- ing 150 Ib (69 kg). Vital signs were normal. Phys- ical examination was not remarkable except for left lower quandrant abdominal tenderness. On
320 NUTRlTlON REVIEWSIVOL 46. NO SISEPTEMBER 198%

SU L FA S A LA 2 I N E .COOH
SU L FAPY RI 01 N E 5-AMINOSALICY LIC ACI 0
FOLK ACID OH COOH
Figure 1. Chemical formulas of sulfasalazine and folic acid.
sigmoidoscopy the patient showed loss of nor- mal mucosal detail, increase in mucosal friabi- lity, and presence of thick inflammatory exudate composed of pus, mucous, and blood.
Laboratory data showed a red blood count of 2.9 x lo6 cells per I*.I (normal 4.6 to 6.2 x lo6 cells per FI), hematocrit 34 ml/dl (normal 40 to 52 mlidl), mean corpuscular volume 115 f l (nor- mal 80 to 100 fl), indicating macrocytic anemia. The serum folate level was depressed to 0.7 ng/ml (normal 4 to 15 ng/ml), total protein was 6.9 g/dl (normal 6.0 to 8.0 g/dl), and albumin 3.8 g/dl (normal 3.5 to 5.5 g/dl). The d-xylose ab- sorption test, fecal fat, plasma iron, total iron- binding capacity, the Schilling test, and plasma vitamin B,, levels were all within normal ranges.
The presence of macrocytic anemia, a mega- loblastic bone marrow, a low plasma folate, and a normal plasma B,2 level led to the diagnosis of folate deficiency. The absorption of tritiated pteroylmonoglutamic acid ([3H]FA) was then studied. [3H]FA (25 KCi per 200 pg) was admin- istered orally to this patient, who was given only water for 4 hours and then allowed to resume his normal diet. All medications were continued on their usual schedule with the exception of sulfasalazine, which was administered in the usual dose at the time the tritiated folate was in- gested. A week later the patient was restudied in the absence of the sulfonamide. Six control
subjects absorbed 66 t 12 percent of the oral dose, whereas this patient absorbed 49 percent when off the drug and only 12 percent on sulfa- salazine. Absorption of folate was depressed in nine patients with ulcerative colitis whether on or off sulfasalazine. Figure 2 shows, futhermore, that the elevation of serum folate in plasma over the fasting level in normal subjects after a 500 p,g dose of folic acid was depressed by taking 1 g of sulfasalazine 15 minutes before the [3H]FA.
Comment The existence of folic acid deficiency in
this patient with ulcerative colitis was in- tensified when he was given a sulfonamide that is very effective in combatting the in- flammation associated with this disease. Sulfasalazine depressed the absorption of folate in this patient from approximately 49 to 12 percent (normal 65 2 12 percent) of the administered dose and undoubtedly contributed to the development of his rne- galoblastic anemia. Dietary inadequacy was considered partially responsible for the folate deficiency because of the fresh fruit-free and vegetable-free diets com- monly recommended for patients with IBD.
NUTRITION REVIEWSIVOL 46, NO 9ISEPTEMBER 1988 321

I m c 20 a Y
10 r
n - 0 i 2 3
HOURS
Figure 2. The effect of sulfasalazine per os on absorp- tion of SO0 p,-g of folic acid in nine normal subjects. Each point represents the mean & SD of the increment in serum folate above pretest baseline. -0- = control values; - -0- - = effect of 1 g sulfasalazine given 15 minutes before the ["JFA.
Although most observers have reported normal jejunal biopsies in IBD, Salem et a16 and Salem and Truelove7 reported the presence of a mucosal lesion by biopsy in ulcerative colitis consisting of partial villus atrophy associated with impaired fat and xylose absorption. Jankey and Price8 found similar changes in four of ten patients with ulcerative colitis, but failed to find histo- chemical abnormalities in a battery of mu- cosal enzymes studied. Jalan et a19 found partial or total villus atrophy in eight of 27 patients. Abnormal d-xylose excretion was present in 25 percent and steatorrhea in 50 percent of their patients.
The malabsorption of folate in patients with regional enteritis was shown earlier by Cox et all0 and Hoffbrand et al.3 Klipstein" measured the urinary excretion of orally administered tritium-labeled folic acid (40 pg/kg) in four patients with regional enter- itis, noting severely depressed absorption in one patient with jejunal involvement and borderline absorption in the other three.
Franklin and Rosenberg5 found that five out of 11 patients with ulcerative colitis had anemia, serum folate values below 3.6 ng/ml, and macrocytosis. Even without sul-
fasalazine they found folate absorption de- creased below normal. In some patients who had jejunal biopsies, branching and shortening of the intestinal villi was noted. These investigators also showed a reduc- tion in uptake of [3H]FA by rat intestinal rings in the presence of 50 mg/dI of sulfa- salazine, but not in the presence of either sulfapyridine or 5-aminosalicyclic acid. Surprisingly, sulfasalazine did not interfere with the bioassay for folate by Lactoba- cillus casei.
In subsequent studies, Selhub et all2 showed that sulfasalazine is a competitive inhibitor of intestinal folate transport, al- though the mechanisms of its action re- mains uncertain. Because all f o l k acid de- rivatives, regardless of the state of oxidation and the carbon substitution, are absorbed by a common transporter, the ef- fect of sulfasalazine on dihydrofolate re- ductase, methylenetetrahydrofolate reduc- tase, and serine transhydroxymethylase, was studied. Each of these enzymes was in- hibited by sulfasalazine in the same con- centration range as that previously ob- served to inhibit intestinal folate transport, and the kinetic data were consistent with a competitive mode of inhibition. Specificity of inhibition was demonstrated by the find- ing that the reduction of the pteridine ring of pteroylheptaglutamic acid by dihydrofo- late reductase was subject of inhibition, whereas the hydrolysis of the y-glutamyl peptide side chain by chicken pancreatic conjugase was not affected. These results are interpreted to indicate that sulfasala- zine interferes with a folate binding site that is common to these enzymes and to the intestinal transport system.
Inflammation of the GI tract has a global character unsuspected for many years. The pathologic involvement of any one part may, to different degrees, affect the integ- rity of other parts. In the case of IBD, lower bowel disease affects upper bowel func- tion. The mechanism by which this occurs is unclear; it may be due to the primary dis- ease process or to other factors associated with the primary process such as malnutri- tion. In addition, as shown in this case,
322 NUTRITION REVlEWSlVOL 46, NO 9ISEPTEMBER 1988

some drugs used to combat the inflamma- tion associated with IBD may worsen nutri- tional status. Drug-nutrient interactions should be carefully considered by physi- cians whenever they order an antibiotic or ant i-i n f lam mat o ry d rug .
1.
2.
3.
4.
5.
BW Beal, AP Skyring, J McRae, and BG Fir- kin: The Anemia of Ulcerative Colitis. Gas- troenterology 45: 589-603, 1963 TP Omerod: Observations on the Incidence and Cause of Anemia in Ulcerative Colitis.
AV Hoffbrand, JS Stewart, CC Booth, and DL Mollin: Folate Deficiency in Crohn’s Disease: Incidence, Pathogenesis, and Treatment. Br Med J 2: 71 -75, 1968 H Anderson, G Dotevatl, R Gillberg, R Ja- genburg, and NG Kock: Absorption Studies in Patients with Crohn’s Disease and in Pa- tients with Ulcerative Colitis. Acta Med Scand 190: 407-410, 1971 JL Franklin and IH Rosenberg: Impaired Folic Acid Absorption in Inflammatory Bowel Disease: Effects of Salicylazosulfa- pyridine (Azulfidine). Gastroenterology 64:
Gut 8: 107-113, 1967
517-525, 1973
6.
7.
8.
9.
10.
11.
12.
JN Salem, SC Truelove, and WDC Rich- ards: Small-Intestinal and Gastric Changes in Ulcerative Colitis: A Biopsy Study. Br Med J 1 : 394-398, 1964 JN Salem and SC Truelove: Small-lntes- tinal and Gastric Abnormalities in Ulcer- ative Colitis. Br Med J 1 : 827-831, 1965
N Jankey and LA Price: Small-Intestinal Histochemical and Histological Changes in Ulcerative Colitis. Gut 10: 267-269, 1969 KN Jalan, IW Percy-Robb, and JPA McManus: Malabsorption in Ulcerative Co- litis in Malabsorption. RH Girdwood and AN Smith, Editors. Edinburgh University Press, Edinburgh, Scotland, 1969 EV Cox, MJ Meynell, WT Cooke, and R Gaddie: The Folic Acid Excretion Test in the Steatorrhea Syndrome. Gastroenterol-
FA Klipstein: The Urinary Excretion of Orally Administered Tritium-Labeled Folic Acid as a Test of Folic Acid Absorption.
J Selhub, GJ Dhar, and IH Rosenberg: Inhi- bition of Folate Enzymes by Sulfasalazine. J Clin Invest 61 : 221 -224, 1978
Ogy 35: 390-397, 1958
Blood 21 : 626-639, 1963
NUTRITION REVIEWSIVOL 46, NO SISEPTEMBER 1988 323