Embed Size (px)
Citation preview

Succession Planning: Using Simulation to Develop Nurse Leaders for the Future
October 201424 Nurse Leader
BACKGROUNDOne of the biggest shortages in healthcare middle manage-ment is that of the registered nurse (RN),1 whose average agein the United States is 47.2 With increasing chief nursingofficer (CNO) turnover, recruitment into these leadershippositions is critical to meeting the leadership and manage-ment needs of the future. Succession planning is imperative,and many organizations have embedded it into their strategicplans. Those individuals who manifest leadership skills whilemanaging patients or staff, who are not yet in formal leader-ship roles, are identified as aspiring or emerging nurse leaders.Many managers were promoted into leadership positionsbecause they were competent staff nurses and clinicians.
Oftentimes, nurses are placed in management positions with-out proper training, and they lack the necessary skills to per-form effectively in a management role, which is one reasonturnover occurs.3
Education programs such as Nurse Manager Fellowshipand Emerging Nurse Leader Institute through the AmericanOrganization of Nurse Executives (AONE), and theFoundation for Leadership Excellence through theAssociation of California Nurse Leaders (ACNL) are exam-ples of educational opportunities for aspiring leaders. Theseprograms have comprehensive modules around such neces-sary topics as human resources, finance, communication, andquality, and are conducted over a 3- to 5-day period.
KT Waxman, DNP, MBA, RN, CNL, CENP, CHSE, and Christine Delucas, DNP, MPH, RN, NEA-BC
Another method of educating emerging and current lead-ers is through simulation. Simulation has been utilized inhealthcare for the past 20 years (high-fidelity, standardizedpatients, task trainers) for students and staff. Although manyorganizations own high-fidelity simulators and have simula-tion centers, their curricula typically do not include leader-ship development.
Simulating situations in a realistic-looking environmentcan be effective in building leadership skills. Creating anenvironment that allows staff to practice their newlyacquired skills in a safe environment without judgment willnot only prepare them for the real-life experiences but alsoto identify early on whether the move to a leadership posi-tion is warranted.
LITERATURE REVIEWAs healthcare continues to evolve, it is imperative that leadersdevelop skills that will enhance their abilities to face thecompetitive environment today and in the future. Drawingon interpersonal skills, innovation, values, and experience arecritical to addressing the challenges of today’s healthcarearena.4–6 The ability to work deftly across disciplines to pro-vide the highest quality of safe, effective care requires nurseleaders to have well-honed soft skills (e.g., communication,relationship building, professionalism). Embodied in theAONE’s competencies are hard skills (e.g., finance, marketing,strategic planning) and also soft skills, plus innovation, tech-nology, and the need to address succession planning.7
In a review of the literature, (C. Delucas, unpublished data)found that although the military and aviation industries haveled many others to recognize that nontechnical leadership skillscontribute to safety and in training on human factors, health-care and nursing have lagged behind. Furthermore, it is wellknown that a significant number of nurses are of the babyboomer generation. This large population of nurses on the
brink of retirement renders succession planning critical to thecontinued success of healthcare organizations. However, morethan two-thirds of chief nurse executives (CNEs) indicatedthat they have no plans for leadership development in succes-sion planning.8
There is an abundance of discussion in the literatureregarding leadership and its impact on employees and thesuccess of an organization. An increase in dialogue regard-ing communication and team building has ensued over thelast decade. Robles9 identified the top 10 soft skills thatbusiness executives in a variety of industries stated werecritical to successful leadership. Communication andintegrity far exceeded the others in importance, followedby courtesy, responsibility, social skills, positive attitude,professionalism, flexibility, teamwork, and work ethic.Research does not negate the importance of hard skills butcorroborates that soft skills are equally as important andshould be considered complementary (C. Delucas, unpub-lished data).
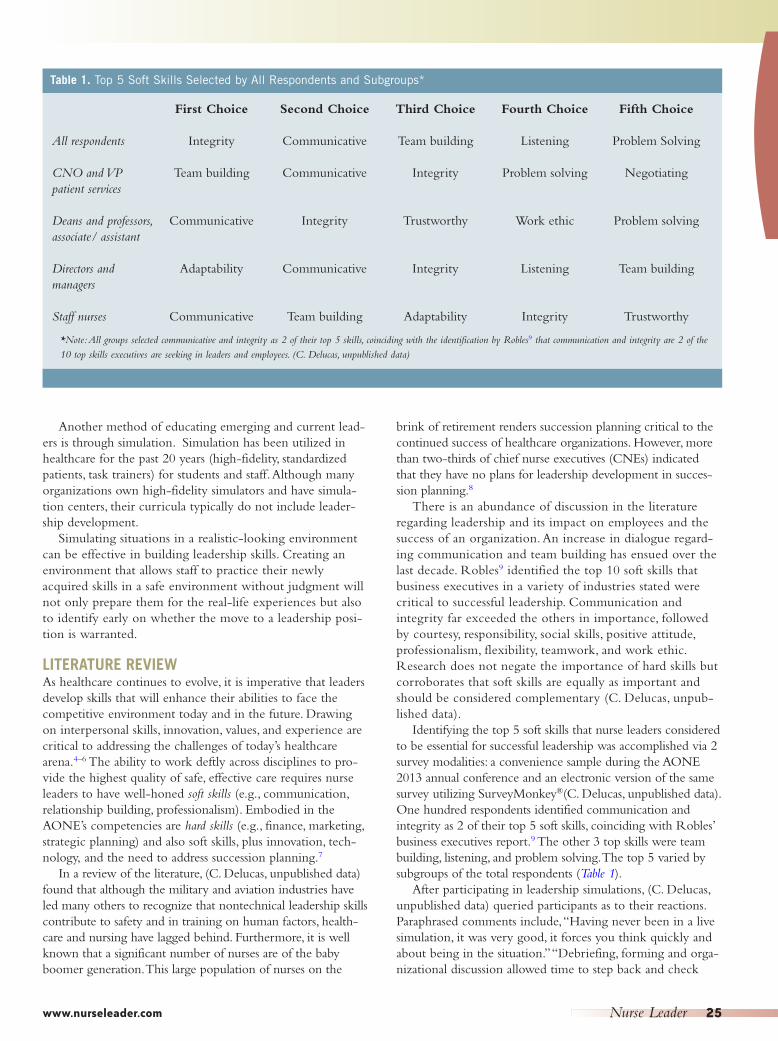
Identifying the top 5 soft skills that nurse leaders consideredto be essential for successful leadership was accomplished via 2survey modalities: a convenience sample during the AONE2013 annual conference and an electronic version of the samesurvey utilizing SurveyMonkey®(C. Delucas, unpublished data).One hundred respondents identified communication andintegrity as 2 of their top 5 soft skills, coinciding with Robles’business executives report.9 The other 3 top skills were teambuilding, listening, and problem solving. The top 5 varied bysubgroups of the total respondents (Table 1).
After participating in leadership simulations, (C. Delucas,unpublished data) queried participants as to their reactions.Paraphrased comments include, “Having never been in a livesimulation, it was very good, it forces you think quickly andabout being in the situation.” “Debriefing, forming and orga-nizational discussion allowed time to step back and check
www.nurseleader.com Nurse Leader 25
Table 1. Top 5 Soft Skills Selected by All Respondents and Subgroups*
First Choice Second Choice Third Choice Fourth Choice Fifth Choice
All respondents Integrity Communicative Team building Listening Problem Solving
CNO and VP Team building Communicative Integrity Problem solving Negotiatingpatient services
Deans and professors, Communicative Integrity Trustworthy Work ethic Problem solvingassociate/ assistant
Directors and Adaptability Communicative Integrity Listening Team buildingmanagers
Staff nurses Communicative Team building Adaptability Integrity Trustworthy
*Note: All groups selected communicative and integrity as 2 of their top 5 skills, coinciding with the identification by Robles9 that communication and integrity are 2 of the10 top skills executives are seeking in leaders and employees. (C. Delucas, unpublished data)

perceptions.” “You’re in the moment, learning for the futureand debriefing provided immediate feedback.”
Simulation, an experiential learning process led by theaviation and military industries, has been embraced for decadesto educate workers in technical and nontechnical skills.Healthcare and nursing have readily followed suit in the tech-nical skills. Though the Institute of Medicine (IOM) recog-nized simulation as a modality for communication, little hasbeen accomplished in nontechnical or soft skill development.10
A review of the California Simulation Alliance (CSA) libraryof scenarios revealed an absence of scenarios focused on lead-ership (C. Delucas, unpublished data). The IOM 2010 reportcalled for nursing to lead, through innovation and collabora-tion, the changes in healthcare.4 Simulation may be seen as aninnovative modality to address leadership assessment and devel-opment of soft skills, as well as a method for candidate selec-tion and succession planning.
Addressing the gap in soft-skill leadership developmentscenarios was accomplished with an evidence-based tem-
plate. The scenarios were validated and tested by CSAfaculty, who are experienced nurse leaders with core com-petencies in the subject matter as well as in simulation.Content for the scenarios was developed based on actualexperiences of colleagues and the authors, both formerCNOs and currently nurse executives. The scenarios pro-vide experiential learning situations for middle managers.Debriefing questions were designed to be open-ended andto elicit insight from participants as to their actions anddialogue during simulation (for an example leadershipscenario from the CSA library, Appendix).
Patrician et al.11 offered that with the looming turnover innursing leadership, educating charge nurses in leadership skillsis paramount to addressing succession planning. Additionally,they identified that minimal, if any, education and training iscurrently provided for nurses embarking on leadership roles,especially as frontline charge nurses. The authors’ recommen-dations included that leadership courses should includeobservation and simulation, not only for charge nurse posi-tions, but also for other leadership roles.
Coaching, mentoring, residencies, and formal courses areexamples of more conventional methods of leadership devel-opment. All are valuable; however, adding simulation providesan enhancement to the educational processes. Coaching maybe defined as educating, schooling, tutoring, preparing, orinstructing. Mentoring is often defined as counseling, sup-porting, advising, and tutoring. Simulation incorporates most,if not all, of those characteristics and is an adjunct to manyformal courses in all levels of nursing education.
Simulation provides a realistic experience for aspiring andcurrent leaders in a safe environment whereby different stylesmay be assessed and developed. Situational awareness is evi-dent and the student has the opportunity to delve into theissues with accomplished facilitators. Debriefing after a simu-lation is akin to coaching, because open-ended questions arefundamental, and listening on the part of the facilitatorassures that the participant develops an understanding of howto address the same circumstance in a variety of situations.The literature shows that most learning occurs in thedebriefing session immediately following the scenario.12
WHY USE SIMULATION FOR LEADERSHIPDEVELOPMENT FOR ASPIRING/EMERGINGLEADERS?The CSA has been writing and creating simulation scenariossince 2006, when the California Institute for Nursing andHealth Care (CINHC) created the Bay Area SimulationCollaborative (BASC).13 The BASC was funded through agenerous grant from the Gordon and Betty Moore Foundationto create a faculty development plan and 50 simulation scenar-ios. Scenarios were written for areas such as critical care, pedi-atrics, medical/surgical, and obstetrics. Initially, scenarios weredeveloped to be used with high-fidelity simulators or standard-ized patients in a simulated clinical environment. Movingtoward multiple types of scenarios, such as standardized patientsand virtual reality, a new category of scenarios was developedthat focuses on leadership development. These scenarios are
October 201426 Nurse Leader
1. Assessing the communication skills in management
2. Candidates
3. Coaching staff nurses
4. Combatting lateral violence in the healthcare
5. Communication
6. Crucial conversations: lateral violence in the workplace
7. Empathy
8. Good leader, bad manager
9. Having a difficult conversation with a direct report
10. HIPAA violation
11. Improving patient outcomes through system changeand leading with the heart
12. Integrity
13. Listening
14. NP to MD communication: leadership and the scopeof practice
15. Nurse leader communication challenges
16. Observing culturally insensitive nursing care to a gen-der minority
17. Post-op pain control
18. Teamwork and collaboration
19. Teamwork in a primary care setting: improvingcommunication
HIPAA, Health Insurance Portability and Accountability Act; NP, nurse practitioner.
Box 1. List of Sample Scenarios
www.nurseleader.com Nurse Leader 27
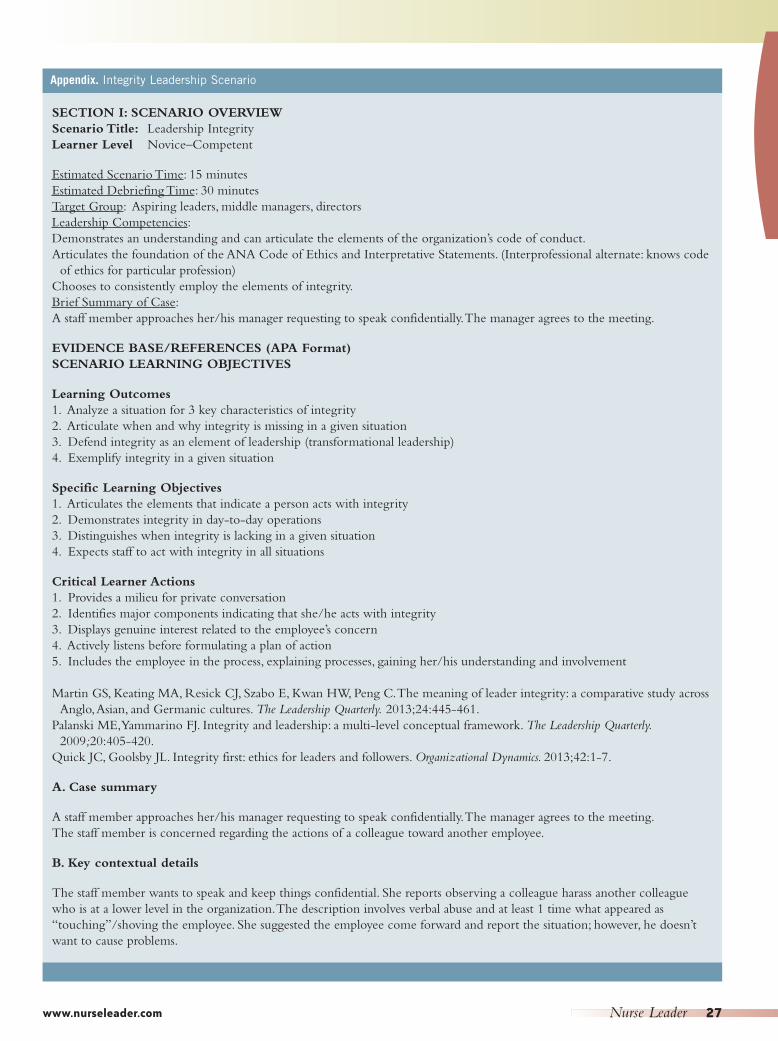
Appendix. Integrity Leadership Scenario
SECTION I: SCENARIO OVERVIEWScenario Title: Leadership IntegrityLearner Level Novice–Competent
Estimated Scenario Time: 15 minutesEstimated Debriefing Time: 30 minutesTarget Group: Aspiring leaders, middle managers, directorsLeadership Competencies:Demonstrates an understanding and can articulate the elements of the organization’s code of conduct.Articulates the foundation of the ANA Code of Ethics and Interpretative Statements. (Interprofessional alternate: knows code
of ethics for particular profession)Chooses to consistently employ the elements of integrity.Brief Summary of Case: A staff member approaches her/his manager requesting to speak confidentially. The manager agrees to the meeting.
EVIDENCE BASE/REFERENCES (APA Format)SCENARIO LEARNING OBJECTIVES
Learning Outcomes 1. Analyze a situation for 3 key characteristics of integrity2. Articulate when and why integrity is missing in a given situation3. Defend integrity as an element of leadership (transformational leadership) 4. Exemplify integrity in a given situation
Specific Learning Objectives1. Articulates the elements that indicate a person acts with integrity2. Demonstrates integrity in day-to-day operations3. Distinguishes when integrity is lacking in a given situation 4. Expects staff to act with integrity in all situations
Critical Learner Actions 1. Provides a milieu for private conversation2. Identifies major components indicating that she/he acts with integrity3. Displays genuine interest related to the employee’s concern4. Actively listens before formulating a plan of action5. Includes the employee in the process, explaining processes, gaining her/his understanding and involvement
Martin GS, Keating MA, Resick CJ, Szabo E, Kwan HW, Peng C. The meaning of leader integrity: a comparative study across Anglo, Asian, and Germanic cultures. The Leadership Quarterly. 2013;24:445-461.
Palanski ME, Yammarino FJ. Integrity and leadership: a multi-level conceptual framework. The Leadership Quarterly.2009;20:405-420.
Quick JC, Goolsby JL. Integrity first: ethics for leaders and followers. Organizational Dynamics. 2013;42:1-7.
A. Case summary
A staff member approaches her/his manager requesting to speak confidentially. The manager agrees to the meeting.The staff member is concerned regarding the actions of a colleague toward another employee.
B. Key contextual details
The staff member wants to speak and keep things confidential. She reports observing a colleague harass another colleaguewho is at a lower level in the organization. The description involves verbal abuse and at least 1 time what appeared as“touching”/shoving the employee. She suggested the employee come forward and report the situation; however, he doesn’twant to cause problems.
October 201428 Nurse Leader
designed for the nurse executive or nurse educator to be uti-lized in their own organizations as an adjunct to their currenteducation program for leadership development and can also beused for existing staff.
Using the approved, evidence-based, validated scenario tem-plate already used by the CSA, the template was modified toincorporate leadership competencies derived from the AONEand other leadership literature. Benner’s model14 is used toclassify the learner’s level of understanding of the scenarios.
At the University of San Francisco, 15 additional scenarioswere written, validated, and tested by doctoral students. Anexecutive leadership doctor of nursing practice student con-tributed 5 scenarios as part of her final project. Leadershipdevelopment areas for these scenarios included: HealthInsurance Portability and Accountability Act (HIPAA) viola-tions, nurse/physician communication, counseling difficultemployees on absenteeism, integrity, empathy, team building,and more (Box 1). The scenarios in Box 2 are designed foremerging, new, or current managers to assess and gain leader-ship skills in dealing with difficult employees, communica-tion, teambuilding, etc.
CONCLUSIONSimulation, a proven and effective methodology for educatingstaff and students, may be used for leadership skills assessmentand development. Providing an opportunity in a safe, non-judgmental environment assists nurse leaders at all levels toacquire the skills that they need to move in to the leadershippositions currently vacant or newly created. The aviationindustry has been successful in mandating that all of its pilotsexperience simulation before flying a plane. Should health-care not do the same for emerging leaders? NL
References1. Eddy LL, Doutrich D, Higgs ZR, Spuck, J, Olson M, Weinberg S. Relevant
nursing leadership: an evidence-based programmatic response. InternationalJ Nurs Educ Scholarsh. 2009; 6:Article 22.
2. Nursing Faculty Shortage Fact Sheet. 2010-2011 Salaries of Instructionaland Administrative Nursing Faculty in Baccalaureate and Graduate Programsin Nursing. American Association of Colleges in Nursing website.http://www.aacn.nche.edu. Accessed December 11, 2012.
3. Stichler JF. Succession planning: why grooming their replacements is criticalfor nurse leaders. Nurs Womens Health. 2008;12:525-528.
4. Institute of Medicine. The Future of Nursing: Leading Change, AdvancingHealth. Washington, DC: National Academies Press; 2010.
5. Dow AW, Salas E, Mazmanian PE. Improving quality in systems of care:solving complicated challenges with simulation-based continuing profession-al development. J Contin Educ Health Prof. 2012;32:230-235.
6. Kalargyro V, Pescosolido AT, Kalargiros EA. Leadership skills in managementeducation. Acad Educ Leadersh J. 2012;16(4):39-63.
7. The AONE Nurse Executive Competencies. American Organizations of NurseExecutives website. http://www.aone.org/resources/leadership%20tools/PDFs/AONE_NEC.pdf. Accessed April 13, 2013.
8. Havens DS, Thompson PA, Jones PB. Chief nursing office turnover: chiefnursing officers and healthcare recruiters tell their stories. J Nurs Adm.2008;38:515-525.
9. Robles MM. Executive perceptions of the top 10 soft skills needed in today’sworkplace. Bus Prof Commun Q. 2012;75:453-465.
10. Institute of Medicine. To Err Is Human: Building for a Safer Health System.Washington, DC: National Academies Press; 1999.
11. Patrician PA, Oliver D, Miltner RS, Dawson M, Ladner KA. Nurturing chargenurses for future leadership roles. J Nurs Adm. 2012;42:461-466.
12. Dieckmann P, Reddersen S, Zeiger J, Rall M. Video-assisted debriefing insimulation-based training of crisis resource management. In: Kyle R, MurrayWB. Clinical Simulation. San Diego, CA: Academic Press; 2008.
13. Waxman KT, Nichols A, O’Leary-Kelley C, Miller M. The evolution of astatewide alliance: the Bay Area Simulation Collaborative. Simul Healthc.2011;6:345-351.
14. Benner P. From Novice to Expert: Excellence and Power in Clinical NursingPractice. Menlo Park, CA: Addison-Wesley; 1984.
KT Waxman, DNP, MBA, RN, CNL, CENP, CHSE, is assis-tant professor and chair DNP Department at the University of SanFrancisco and Director, California Simulation Alliance in SanFrancisco, California. She can be reached at [email protected] Delucas, DNP, MPH, RN, NEA-BC, an assistant pro-fessor at College of Nursing, University of New Mexico inAlbuquerque, New Mexico.
Note: Dr. Waxman discloses that she received speaker fees for presen-tations related to simulation and is an independent contractor for theCINHC.
1541-4612/2014Copyright 2014 by Elsevier Inc.All rights reserved.http://dx.doi.org/10.1016/j.mnl. 2014.07.009





























