Embed Size (px)
Citation preview

Pediatr Blood Cancer 2010;54:170–172
BRIEF REPORTSuccessful Radiation Therapy for Supratentorial Primitive Neuroectodermal
Tumor and Epidermolysis Bullosa Simplex
Sejal Bavishi, BA,1 Kenneth Wong, MD,1 Thamani Delgardo, BA, RTT,1 Araz Marachelian, MD,2
and Soumen Khatua, MD2*
INTRODUCTION
Epidermolysis bullosa (EB) is a heritable skin disorder
characterized by increased skin fragility and blister formation
after minor mechanical trauma. Three major inherited forms are
EBS, junctional epidermolysis bullosa (JEB), and dystrophic
epidermolysis bullosa (DEB) [1]. Phenotypic variants range from
mild blistering largely localized to the hands and feet, to a more
severe generalized form, leading to death in early infancy. EBS is the
most common and the mildest form of EB and has three subtypes.
They are EBS-Koebner, EBS Weber-Cockayne and EBS Dowling-
Meara. Blisters in EBS usually occur in the intraepidermal area.
EBS-Koebner commonly presents at birth to early infancy and
involves the hands, feet and extremities. EBS Weber-Cockayne
commonly occurs in children and adults and presents on the palms
and soles only after a distinct traumatic event. EBS Dowling-Meara,
a severe form of EBS, occurs at or shortly after birth with a
generalized distribution of blisters [2]. Skin lesions in EBS usually
heal without scarring and extracutaneous involvement is extremely
rare. Evaluation of malignancies in EB shows that squamous cell
carcinoma (SCC) is the most serious complication of EB in adults,
especially those with DEB. By mid-adulthood, nearly all patients
with DEB will have had at least one SCC and nearly 80% will have
died of metastatic SCC despite aggressive surgical resection [3].
Central nervous system (CNS) tumors in children with EB are
extremely rare. Only one case has been reported of an infant with
JEB diagnosed with congenital rhabdoid tumor of the CNS at
autopsy [4].
Supratentorial primitive neuroectodermal tumor (sPNET) in
children are rare and represent less than 2.5% of childhood brain
tumors, with the median age at presentation of 3 years. While the
treatment for sPNETs is not well defined, current treatment involves
a multifaceted approach that includes surgery, chemotherapy, and
post-operative radiotherapy. However, sPNETs are more resistant
to conventional treatment modalities, making them less curable than
medulloblastomas. High-dose cyclophosphamide-based chemo-
therapy with stem cell support after risk-adapted craniospinal
irradiation (CSI) results in excellent event free survival (EFS) in
patients with newly diagnosed average risk (AR) sPNET [5]. Long-
term neurocognitive toxicity and development of secondary malig-
nancies are well-known complications of CSI. The tolerability of
CSI in patients with EB and the long-term complications is unknown
and has not been reported. However there are reports of radiation
delivered locally to treat SCC in patients with underlying DEB [6].
This novel case demonstrates the presentation of a patient with EBS
and sPNET and highlights the feasibility and successful use of CSI
and focal tumor bed radiation.
CASE REPORT
A 7-year-old male presented with generalized hyperpigmenta-
tion of the skin at birth. A diagnosis of EBS was confirmed by skin
biopsy. His skin blistered after minor trauma, which was managed
symptomatically using emollients and topical antibiotics. One year
prior to presentation, he started developing nonfocal headaches.
Though initially mild, they increased over the following year and
were associated with vomiting. These episodes were treated
symptomatically as sinus infections. One week prior to admission,
he developed ataxia and diplopia, with increasing intensity of
headaches. He was evaluated in the emergency department, where a
CT scan followed by an MRI showed a mixed cystic solid lesion in
the left anterior temporal lobe. Following admission, he underwent a
craniotomy and gross total resection of the left temporal lobe mass
(Fig. 1). His spine MRI and CSF cytology were negative for any
evidence of metastasis. Pathology was consistent with sPNET.
Post-operatively his symptoms improved dramatically. Following
GCSF stimulation, he underwent successful stem cell harvest. He
was then treated with conventional CSI to a total dose of 23.4 Gy in
13 fractions. CSI was followed by a focal boost to the tumor bed
using intensity modulated radiotherapy (IMRT) to a dose of 32.4 Gy
in 18 fractions. Several important precautionary measures were
taken to protect the patient’s underlying fragile skin condition from
the effects of radiotherapy. Radiation therapy was administered in
the supine position in contrast to the conventional prone position.
Epidermolysis bullosa simplex (EBS) is a heritable skin disordercharacterized by skin fragility and blistering. While its most severevariant, dystrophic epidermolysis bullosa (DEB) is associated withsquamous cell carcinoma (SCC), the development of extracutaneousneoplasms in EBS is extremely rare. We report a novel case of
supratentorial primitive neuroectodermal tumor (sPNET) in a 7-yearmale with EBS. Experience of radiation therapy and its challenges inchildren with EBS has rarely been reported. Pediatr Blood Cancer2010;54:170–172. � 2009 Wiley-Liss, Inc.
Key words: epidermolysis bullosa simplex; radiation therapy; supratentorial PNET
� 2009 Wiley-Liss, Inc.DOI 10.1002/pbc.22281Published online 16 September 2009 in Wiley InterScience(www.interscience.wiley.com)
——————1Department of Radiation Oncology, Childrens Hospital Los Angeles,
Los Angeles, California; 2Center for Cancer and Blood Disorders,
Neural Tumors Program, Childrens Hospital Los Angeles, Los
Angeles, California
The authors declare that there is no disclosure and any conflict of
interest.
*Correspondence to: Soumen Khatua, 10232 Splendor Ridge Avenue,
Las Vegas, NV 89135. E-mail: [email protected]
Received 27 July 2009; Accepted 12 August 2009
The treatment couch as well as the customized head immobilization
cushion was lined with cotton padding. The HeadFix device was
fabricated with a nasal bridge rather than a conventional bite block.
Petroleum jelly was liberally applied to the upper lip, nose, and other
high friction points along with topical emollients to minimize the
effects of friction injury. His skin toxicity profile was restricted
to grades 1–2 (Fig. 2). This included small patches of moist
desquamation in his ear folds and a few subcentimeter bullae on his
occiput. Mild increase in his hyperpigmentation was seen during his
radiation, which is slowly resolving. He had minimal nausea and
vomiting, which were treated symptomatically and mild myelo-
suppression during his radiation therapy. He is currently doing well
and will begin four cycles of dose-intensive cyclophosphamide
based chemotherapy with stem cell rescue.
DISCUSSION
The association of EB with brain tumors and its treatment has not
been reported earlier. The only prior case report is of a male child
with JEB who was found to have a cerebellar atypical teratoid
rhabdoid (AT/RT) tumor at autopsy [4]. Due to the extreme rarity of
this case, the tolerability of CSI is unknown in these patients. There
are a few case reports of SCC in adult DEB patients, who were
treated with localized radiation, but the toxicity was not reported
Pediatr Blood Cancer DOI 10.1002/pbc
Fig. 1. Pre-operative (A) and post-operative (B) MRI scans showing a mass in the left temporal lobe with gross total resection. [Color figure can be
viewed in the online issue, which is available at www.interscience.wiley.com.]
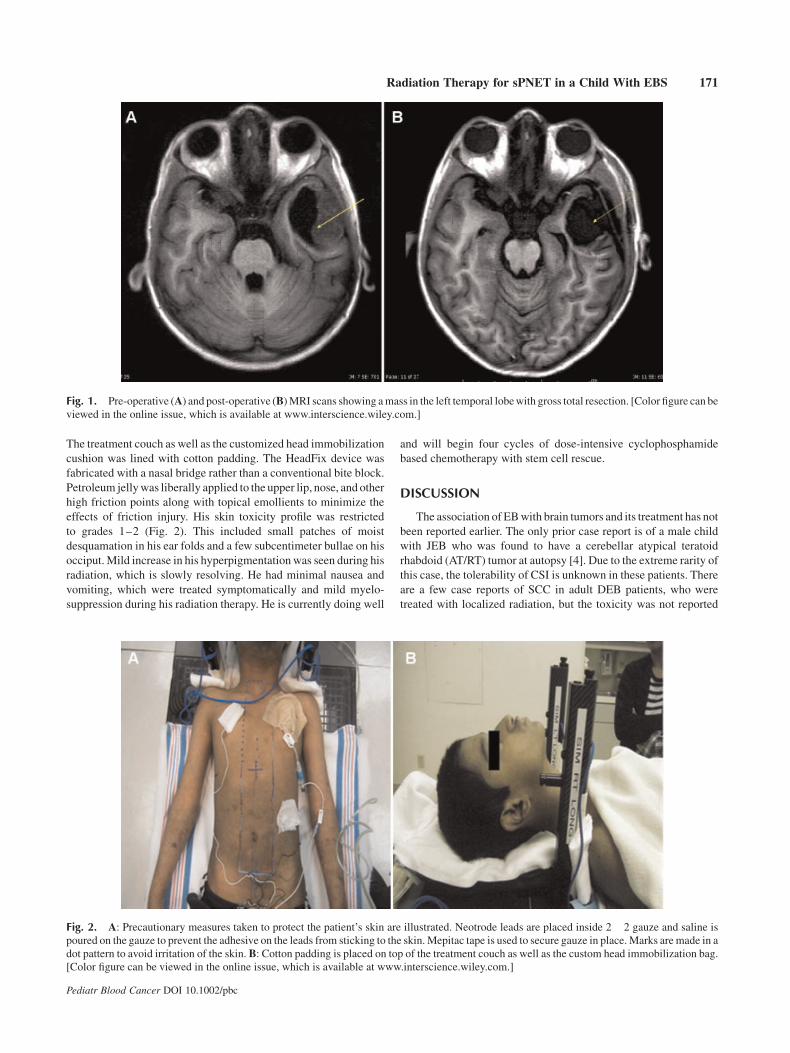
Fig. 2. A: Precautionary measures taken to protect the patient’s skin are illustrated. Neotrode leads are placed inside 2� 2 gauze and saline is
poured on the gauze to prevent the adhesive on the leads from sticking to the skin. Mepitac tape is used to secure gauze in place. Marks are made in a
dot pattern to avoid irritation of the skin. B: Cotton padding is placed on top of the treatment couch as well as the custom head immobilization bag.
[Color figure can be viewed in the online issue, which is available at www.interscience.wiley.com.]
Radiation Therapy for sPNET in a Child With EBS 171

[7,8]. The only pediatric case in the literature reported a 13-year-old
female with DEB who developed SCC, and was treated surgically
without any radiation therapy [9]. Due to the underlying delicate
condition of the patient’s skin and its propensity to blister
after minor trauma, delivering CSI with focal boost was a
therapeutic challenge from the beginning. Several known side
effects to the skin following radiation therapy include irritation,
dryness, erythema, blistering, hyperpigmentation, and desquama-
tion. It was expected that these side effects would be exacerbated in
children with EB like our patient. Using precautionary measures to
the skin as mentioned earlier and delivering radiation in the supine
position, we were able to limit the skin toxicity to grade 2. However,
it remains to be seen how children with the EB and its variants would
tolerate extended field radiation and whether long-term toxicities
would include increased incidence of SCC in these children.
Radiation therapy is an important component of the multi-
modality treatment for children with sPNET. Though similar
histologically to the medulloblastoma, the more distinct oncogenic
pathways in these tumors make them different from their
infratentorial counterparts [10]. They are very aggressive and have
been treated with intensive therapy including CSI of 36 Gy. Several
studies have supported the beneficial role of high-dose radiation
treatment of the entire neuraxis as a critical part of the multimodality
treatment for sPNET [11,12]. Though efforts have been devoted in
various studies to eliminate, delay, or reduce dose and fields of
radiation therapy, the results have met with reduced survival rates
[13–15]. Thus, 36 Gy CSI remains an integral part of the
multimodality therapeutic approach for children with these tumors.
However, a recent study using reduced dose CSI of 23.4 Gy in AR
patients followed by four cycles of high dose cyclophosphamide
based chemotherapy with stem cell rescue showed a 5-year overall
survival rate of 88� 13% survival [5]. Based on these promising
data, we treated our AR patient with a reduced dose CSI of 23.4 Gy.
This dose was hoped to reduce the long-term neurocognitive sequela
and development of secondary malignancies.
This report highlights several precautionary measures to
potentially protect the integrity of the fragile skin in pediatric
patients with EBS during radiation treatment. In addition, the case
emphasizes the importance of the genetic and pathophysiologic
associations between the development of brain tumors in children
with underlying EB. Children with EB and brain tumors require a
multimodality therapeutic approach to further define optimal
treatment strategies.
REFERENCES
1. Pai S, Marinkovich MP. Epidermolysis bullosa: New and emerging
trends. Am J Clin Dermatol 2002;3:371–380.
2. Pfender EG, Bruckner A, Conge P, et al. Basic science of
epidermolysis bullosa and diagnostic and molecular character-
ization: Proceedings of the 2nd International Symposium on
Epidermolysis Bullosa, Santiago, Chile, 2005. Int J Dermatol 2007;
46:781–794.
3. Fine JD, Johnson LB, Weiner M, et al. Epidermolysis bullosa and
the risk of life-threatening cancers. The National EB registry
experience, 1986–2006. J Am Acad Dermatol 2009;60:203–211.
4. Krous HF, Chadwick AE, Haas EA, et al. Congenital cerebellar
malignant rhabdoid tumor in an infant with junctional epidermol-
ysis bullosa. Pediatr Dev Pathol 2007;10:481–486.
5. Chintagumpala M, Hassall T, Palmer S, et al. A pilot study of risk-
adapted radiotherapy and chemotherapy in patients with supra-
tentorial PNET. Neuro Oncol 2009;11:33–40.
6. Bastin KT, Steeves RA, Richards MJ. Radiation therapy for
squamous cell carcinoma in dystrophic epidermolysis bullosa:
Case reports and literature review. Am J Clin Oncol 1997;20:
55–58.
7. Weber F, Bauer JW, Sepp N, et al. Squamous cell carcinoma in
junctional and dystrophic epidermolysis bullosa. Act Derm
Venereol 2001; 81:189–192.
8. McGrath JA, Schofield OM, Mayou BJ, et al. Epidermolysis
bullosa complicated by squamous cell carcinoma: Report of
10 cases. J Cutan Pathol 1992;19:116–123.
9. Ayman T, Yerebakan O, Ciftcioglu MA, et al. A 13-year-old girl
with recessive dystrophic epidermolysis bullosa presenting with
squamous cell carcinoma. Pediatr Dermatol 2002;19:436.
10. Inda MM, Perot C, Guillaud-Bataille M, et al. Genetic hetero-
geneity in supratentorial and infratentorial primitive neuroecto-
dermal tumours of the central nervous system. Histopathology
2005;47:631–637.
11. McBride SM, Daganzo SM, Banerjee A, et al. Radiation is an
important component of multimodality therapy for pediatric non-
pineal supratentorial primitive neuroectodermal tumors. Int J
Radiat Oncol Biol Phys 2008;72:1319–1323.
12. Timmermann B, Kortmann RD, Kuh LJ, et al. Role of radiotherapy
in supratentorial primitive neuroectodermal tumor in young
children: Results of the German HIT-SKK87 and HIT-SKK92
trials. J Clin Oncol 2006;24:1554–1560.
13. Massimino M, Gandola L, Spreafico F, et al. Supratentorial
primitive neuroectodermal tumors (S-PNET) in children: A
prospective experience with adjuvant intensive chemotherapy
and hyperfractionated accelerated radiotherapy. Int J Radiat Oncol
Biol Phys 2006;64:1031–1037.
14. Pizer BL, Weston CL, Robinson KJ, et al. Analysis of patients with
supratentorial primitive neuro-ectodermal tumours enteredinto
the SIOP/UKCCSG PNET 3 study. Eur J Cancer 2006;42:1120–
1128.
15. Johnston DL, Keene DL, Lafay-Cousin L, et al. Supratentorial
primitive neuroectodermal tumors: A Canadian pediatric brain
tumor consortium report. J Neurooncol 2008;86:101–109.
Pediatr Blood Cancer DOI 10.1002/pbc
172 Bavishi et al.





























