Embed Size (px)
Citation preview

Successful Medical Management of Neutropenic Enterocolitis
WOODROW GANDY, MD,' AND BERNARD R. GREENBERG, MDt
The medical management of neutropenic enterocolitis has been associated with a 100% mortality rate according to recent reports. This report describes two cases which were successfully managed without colonic resection. In one case, 67Ga radionuclide scanning was utilized a s an aid in the diagnosis. The incidence, pathogenesis, diagnosis, and previously reported cases of medical management of neutropenic enterocolitis are reviewed, and the role of granulocyte transfusions and %a scanning are discussed.
Cancer 51 A551 -1 555. 1983.
NTEROCOLITIS is a well-recognized complication of E neutropenia in the setting of chemotherapy for malignan~ies,'-~ immunosuppressive therapy in trans- plant patient^,^ benign cyclic ne~tropenia,"- '~ and aplastic anemia.9.'4,15 The diagnosis has been recognized primarily in autopsy but there are a number of recent reports of successful surgical manage- ment.16-** There have been no reports to our knowledge of successful medical management of neutropenic enterocolitis in patients with prolonged neutropenia. In this report, two cases are described which were success- fully managed without colonic resection.
Case Reports
Case I A 53-year-old Mexican-American woman with acute non-
lymphocytic leukemia ( F A 9 Class MI) was treated with the fallowing chemotherapeutic regimen: daunomycin 50 mg/m2 intravenously on days 1 through 3; cytarabine 100 mg/m* on days I through 10 by continuous intravenous infusion; vin- cristine 1.2 mg/m2 on days 1 and 8 intravenously; prednisone 40 mg/m2 on days 1 through 10 orally. She also received tri- methoprim and sulfamethoxazole. On day 9 of chemotherapy, the patient developed a temperature of 38.3"C and therapy was started with nafcillin and tobramycin. She appeared to have cellulitis in the upper right thigh and blood cultures grew out Streptococcus sanguis 1. The cellulitis improved, but she continued to have fever, and on day I I she complained of right-lower-quadrant abdominal pain and loose stools. Ab- dominal examination was notable for slight tenderness in the
midpelvic area. By the next day, bloody diarrhea, abdominal distention, absent bowel sounds, and rebound tenderness in the right lower quadrant were noted. Ticarcillin and clinda- mycin were added to the antibiotic regimen and surgical con- sultation obtained. Her leukocyte count was 0.5 X I03/mm3 with an absolute granulocyte count of 0. Bone marrow aspi- ration revealed a very hypocellular specimen. Hematocrit was 28.8% and platelet count 32,000/mm3. Blood and urine cul- tures were negative and stool culture revealed only Candida albicans. Stool culture for Clostridium dificile was negative and plain film of abdomen (KUB) was unremarkable. C. d$ ficile toxin assay was not obtained. Proctoscopy was considered but because of the patient's critical condition it could not be done. Whole-body survey with 5 mCi of Gallium-67 ("Ga) citrate was obtained on day 13, and on both the 24- and 96- hour views there was a distinct increase in activity in the pos- terior right lower quadrant (Fig. IA). The lack of interval change and configuration made bowel activity an unlikely pos- sibility; the results were felt to be most consistent with a lo- calized inflammatory process. The cellulitis had resolved by this time, and posteroanterior and lateral views confirmed the intra-abdominal location of the inflammation demonstrated by the scan. Daily granulocyte transfusions were begun at this time and continued for a total of 13 days (day 13-26). The patient continued to manifest spiking temperatures and had evidence of low grade disseminated intravascular coagulation. The bloody diarrhea and right-lower-quadrant abdominal ten- derness gradually decreased, resolving by day 18. At this time her absolute granulocyte count was 0 with a leukocyte count of I .3 X 103/mm3. Bone marrow aspiration on day 25 revealed signs of early recovery and her clinical status continued to improve. Antibiotics were discontinued on day 3 I . She was ready for discharge, but on day 31 she had a recurrence of spiking fevers without localized abdominal findings. The source of this fever was unclear but she was begun empirically on tobramycin and clindamycin. A repeat 67Ga scan was ob- tained on dav 34 (Fig. 19) which revealed no further abnormal
From the Department of Internal Medicine, University of Califor- nia, Davis Medical Center, Sacramento, California.
* Resident, Department of Internal Medicine. t Associate Professor of Medicine, Division of Hematology and , ~Y
Oncology.
Tucson. AZ 85723.
activity in the abdomen on the 24-, 72-, and 96-hour scans.
midlung field which was not associated with an abnormality
Address for reprints: Bernard R. Greenberg, MD, Section of He- matology and Oncology, Veterans Administration Medical Center, There was, however, an area of increased activity i n the left
Accepted for publication January 18, 1982. on chest x-ray. The patient became afebrile and after seven
0008-543)</83/04 I5/155 I $ I .05 GJ American Cancer Society
1551

1552 CANCER April 15 1983 Vol. 51
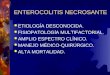
FIGS. 1A AND IB (A, left) "Ga citrate scan with arrow pointing to abnormal uptake in right lower quadrant of abdomen on day 13. (B. right) Resolution of abnormal activity in abdomen on day 37.
days the antibiotics were discontinued and she was discharged. She did well as an outpatient but relapsed in October 1981, six months after achieving a complete remission.
Case 2
A 21-year-old black man with acute nonlymphocytic leu- kemia (FAB Class M2) diagnosed one year previously and treated successfully with chemotherapy, had relapse of his leu- kemia and was admitted for reinduction. Chemotherapy was begun with daunomycin 120 mg IV daily for 3 days; cytarabine 800 mgfday by continuous intravenous infusion for 7 days; and 6-thioguanine 200 mg orally twice daily for 7 days. On day 1 of therapy, the patient's leukocyte count was 4.3 X lo3/ rnm3 with only 34/mm3 granulocytes. Platelet count was 100,000/mm3 and hematocnt 33%. The patient developed a temperature of 38.7"C and was begun on carbenicillin, naf- cillin and tobramycin on day 1 of chemotherapy. By day 4 he had defervesced, and the cytarabine was increased to I680 mg/ day by continuous intravenous infusion. On day 9 he devel- oped guaiac positive diarrhea which persisted but stool cultures revealed only I + coliforms and 2+ yeast. On day 13, the pa-
tient developed recurrent fever with a maximum temperature of 38.3"C. The nafcillin and tobramycin were discontinued and cefazolin and amikacin substituted. The carbenicillin was continued. On day 14, a repeat bone marrow revealed persis- tent leukemia. The patient continued to have guaiac positive diarrhea and fever. Because of the possibility of fungal infec- tion amphotericin-B was begun at a dose of 0.15 mg/kg/day. By day 19 the dose had been increased to 0.75 mg/kg/day. At this time he complained of midline abdominal pain just below the umbilicus. His leukocyte count was 0.8 X I03/mm3 with I granulocyte/mm3; platelet count was 10,000/mm3; and he- matocrit, 27.7%. On day 20 the abdominal pain localized to the right lower quadrant and there was marked rebound ten- derness in that area accompanied by absent bowel sounds. The maximum temperature was 39.4"C. Surgical consultation was obtained and the patient underwent an emergency laparotomy with a presumptive diagnosis of appendicitis or typhlitis. At surgery it was noted that there was marked rnesentenc lym- phadenitis but the colon, cecum, appendix, and small bowel appeared viable. The small bowel and its mesentery were some- what hemorrhagic. Colonic resection was not undertaken. Postoperatively, the patient received daily granulocyte trans-

No. 8 NEUTROPENIC ENTEROCOLITIS - Candy and Greenberg 1553
fusions beginning on day 20 and continuing through day 28. The cefazolin was discontinued on day 20 and cefoxitin was substituted for a possible anaerobic infection. The postoper- ative course was complicated by a partial small bowel obstruc- tion which responded well to suction. Amphotericin-B was discontinued on day 24. The patient continued to be febrile, but on day 26 bowel sounds returned. The leukocyte count was then 1.1 X 103/mm3 with an absolute granulocyte count of 14/mm3. Repeat bone marrow aspiration revealed persistent leukemia. By day 29 the patient had defervesced. Antibiotics were discontinued on day 30 and the diarrhea resolved by day 33. He was discharged from the hospital and died several months later of leukemia.
Discussion
Neutropenic enterocolitis is characterized by agran- ulocytic cellulitis often involving the cecum most prom- inently, and frequently manifesting the symptoms and signs of fever, guaiac positive diarrhea, absent bowel sounds, and abdominal pain (Table 1). Pseudomem- branous and ischemic colitis have also been seen in neu- tropenic patients and may present with symptoms and signs similar to those of neutropenic enterocolitis. Ef- forts to distinguish these entities from neutropenic en- terocolitis including proctoscopy or colonoscopy and stool cultures and toxin assay for C. diflcile should be undertaken. Ischemic colitis may be extremely difficult to diagnose preoperatively.
TABLE 1. Nomenclature in Enteropathies Occumng in ~~~~~~~~~i~ patients] .2.5.7-9.I5.1 7.18.2 1-26
1. Necrotizing enterocolitis (necrotizing enteropathy) A. Pseudomembranous colitis B. Neutropenic enterocolitis, ileo-cecal syndrome, agranulocytic
colitis (typhlitis sometimes used to indicate more specifically inflammation localized to the cecum)
C. Acute ischemic colitis 11. Appendicitis
Other lesions such as leukemic infiltrates and hemorrhagic lesions have been described but are not usually manifested as clinical syn- dromes.' Also, mixed or combined processes may occur.
In both of our cases, the clinical setting, signs, and symptoms were most compatible with a diagnosis of neutropenic enterocolitis. In the patient in Case I , right lower quadrant pathologic findings were confirmed by 67Ga radionuclide scanning. The viable gross appearance of the bowel on laparotomy in the patient in Case 2 makes cecal necrosis unlikely, but the finding of pro- nounced lymphadenopathy suggests that a less severe form of enterocolitis was present. Mesenteric lymph- adenopathy has been noted at laparotomy in more fla- grant cases of neutropenic entero~olitis,'~ but also occurs in otherwise healthy individuals, mimicking appendi- iti is.*',^^ In the setting of pronounced neutropenia with otherwise typical signs of enterocolitis, it is most likely a manifestation of bowel inflammation, possibly dem- onstrating the existence of a spectrum of seventy in neu-
TABLE 2. Reported Failures in Medical Therapy of Neutropenic Enterocolitis Since 1970*
Author and year Specific case or
No. of cases Type of report Condition at diagnosis
Wagner et al.' 1970 Autopsy series
Kingry et aL6 1972 Case reports
Steinberg et al.' 1973 Autopsy series
Sherman ef aL5 1973
Exelby' 1975
Retrospective study of autopsies & surgical pathology
Retrospective study of case records of children with leukemia developing an acute abdomen
Moir & Bale' 1976
Bignold & Harvey]' 1979
Dosik el al.' 1979
Rikin'" 1980
Autopsy series
Case report of C. septicum invasion
Autopsy series
Case report of C. sepricum invasion
in cyclic neutropenia
19 Advanced
typhlitis
1 2
I 2 4
8
5
23
I
5
1 2
Not diagnosed clinically; abdominal pain frequently diffuse.
Bowel perforation at diagnosis, surgery refused. Febrile with tender RLQ mass, died 24 hrs after
Moribund, died after 18 hrs. Chemotherapy continued after onset of symptoms. Not diagnosed antemortum.
All except one moribund on admission and/or not diagnosed antemortum.
Only 2 of 5 diagnosed antemortum.
diagnosis.
Rarely diagnosed antemortum.
Moribund on admission-died 27 hours after admission.
Moribund, died 18 hrs after admission. Died four hours after admission.
* Does not include cases managed surgically. RLQ: right lower quadrant.

1554 CANCER April 15 1983 Vol. 5 1
tropenic enterocolitis. The small amount of serosal hem- orrhage was probably due to inflammation in the area of cecal lymphatic drainage or was secondary to intra- operative bowel handling in this thrombocytopenic pa- tient.
In order to ascertain the factors contributing to the lack of previous successful medical therapy, a review of the incidence, pathogenesis, methods of diagnosis, and previous medical management of neutropenic entero- colitis was undertaken (Table 2).
Incidencv und Puthogcncvis
Although many of the early reports describing neu- tropenic enterocolitis were in children, it is apparent that this disease also occurs in ad~Its.~.~,’Prolla and Kirsner’ in 1964 reported an incidence of gastrointestinal lesions of almost 100% in an autopsy series of 148 leukemic patients, but noted that there was a wide spectrum of severity and type. Moir and Bale’ reviewed 50 necropsies of leukemic children between 1968 and 1975, and found that necrosis of the colon was the primary cause of death in 38%, cecal involvement being the cause of death in 12%. Other investigators have found similar re~u1ts.l.~ It appears that many of these cases are not clearly man- ifested clinically; Exelby et 121.’ found acute abdomen diagnosed antemorturn in only 3.8% of 286 children with acute leukemia.
The pathogenesis of neutropenic enterocolitis is un- certain, but it appears to be due to invasion of the mu- cosa by bacteria, with resulting agranulocytic ~e l lu l i t i s . ’~~.~ It most commonly occurs at the nadir of leukocyte counts following chemotherapy. Shock, intramural hemorrhage, and rapid necrosis of leukemic infiltrates in an area rich in lymphoid tissue have also been pos- t ~ l a t e d . ~ Candida, Psezidomonus arriiginosa, Clostridia, E. coli, and Klebsiella and other gram negative bacteria have been isolated from stool and colonic mucosa post- mortum.2.9. 10.12.13 A ppendicitis has been noted to occur in neutropenic patients, but less frequently than neu- tropenic enterocolitis. I
Diagnosis
As indicated in Table 2, neutropenic enterocolitis has been infrequently diagnosed clinically. In most reported cases, the diagnosis was made at autopsy. This is partly due to the lack of predictable abdominal findings, with many of the patients experiencing only diffuse abdom- inal pain. The localization of pain to the right lower quadrant with rebound tenderness on physical exami- nation is highly suggestive of appendicitis or necrotizing cecal enterocolitis (typhlitis).
The radiographic findings of a relative lack of bowel gas in the right lower quadrant with slight distention of
surrounding small bowel have been reported as an early sign of typhlitis, but roentgenographic findings were un- reliable until the patient is nearly terminal.’ Typhlitis has also presented as toxic ~ e c i t i s . ~ ~ The barium enema has been advocated as a more reliable diagnostic mo- dalit~,’’,~~ but there has been at least one report of death after cecal perforation secondary to a barium enema.7 Milder et in 1973 reported the use of 67Ga citrate in localizing abscesses and osteomyelitis in neutropenic leukemic patients with successful visualization of sites of infection with white blood counts as low as 200/mm3. There have been no reports to our knowledge of radio- nuclide imaging in the diagnosis of necrotizing entero- colitis. The distinct localized uptake of gallium in the right lower quadrant of the patient in Case I , present in both the 24-hour and 96-hour views when the leu- kocyte count was only 600 with 5% granulocytes, is highly suggestive of neutropenic enterocolitis. The res- olution of this finding in the subsequent 67Ga scan, after the patient’s symptoms had resolved, supports this di- agnosis. Although this patient manifested specific signs and symptoms of right lower quadrant pathology, it is possible that gallium scanning might be useful in de- tecting neutropenic enterocolitis in cases where the signs and symptoms are less well localized. Further studies will be needed before the value of the gallium scan in diagnosing neutropenic enterocolitis is established. The use of Indium-labeled granulocytes should also be con- sidered.”
Medicul Management As is apparent in Table 2, many cases designated as
failures of medical therapy in the past were patients who were moribund on admission, or the diagnosis of neu- tropenic enterocolitis was not suspected antemorturn. Antispasmodic agents have been commonly u ~ e d , ~ . ’ ~ but recent evidence indicates that such drugs are undesirable in pseudomembranous ~o l i t i s .~ ’ N o patients with neu- tropenic enterocolitis, and only two with pseudomem- branous colitis,” have been treated with granulocyte transfusions.
Review of the literature indicates that there may be unrecognized examples of neutropenic enterocolitis oc- curring in milder form in which the patients survived with medical the rap^.^^.^^ None of these patients how- ever had prolonged neutropenia. It is likely that with the advent of more potent chemotherapeutic agents, more prolonged neutropenia has led to an increased severity and frequency of this complication. It is imperative that pseudomembranous colitis be excluded by C. diJficile stool cultures and toxin assay in addition to proctoscopy and colonoscopy if the patient can cooperate. If this diagnosis is highly suspected or confirmed, then van- comycin should be added to the treatment program.

No. 8 NEUTROPENIC ENTEROCOLITIS Candy and Greenberg I555
Although there have been well-controlled studies sup- porting the use of granulocyte transfusions in patients with documented infection, neutropenia, and failure to respond to antibiotic^,^^.^^ a recent study indicates that prophylactic granulocyte transfusions are not usefuL3’ Higby, however, has suggested that certain subsets of the neutropenic population may benefit from granulocyte transfusions in the absence of positive blood culture^.'^
At the time our patients recovered from their acute abdominal events, they were still markedly granulocy- topenic with hypocellular leukemic bone marrows. We attribute the success of our medical management to the combination of vigorous antibiotic treatment and gran- ulocyte support. It is possible that with the newer, broad- spectrum antibiotics and the wide availability of gran- ulocyte support, additional patients with neutropenic enterocolitis may be successfully managed without sur- gery, since the latter is very hazardous in such compro- mised patients. Certainly we feel that if such patients deteriorate in the face of medical management, then rapid surgical intervention is indicated in spite of the risks.
REFERENCES I. Wagner ML, Rosenberg HS, Fernbach DJ, Singleton EB. Typh-
litis: A complication of leukemia in childhood. Am J Roentgend 1970;
2. Moir DH, Bale PM. Necropsy findings in childhood leukaemia, emphasizing neutropenic enterocolitis and cerebral calcification. Pa- thology 1976; 8:247-258.
3. Exelby PR, Ghandchi A, Lansigan N, Schwartz 1. Management ofthe acute abdomen in children with leukemia. Cancer 1975: 35:826- 829.
4. Matolo NM, Garfinkle SE, Wolfman EF. Intestinal necrosis and perforation in patients receiving immunosuppressive drugs. Am J Surg 1976; 132:753-754.
5. Sherman NJ, Woolley MM. The ileocecal syndrome in acute childhood leukemia. Arch Surg 1973: 107:39-42.
6. Kingry RL, Hobson RW, Muir RW. Cecal necrosis and perfo- ration with systemic chemotherapy. Am Surg 1973; 39:129-133.
7. Steinberg D, Gold J, Brodin A. Necrotizing enterocolitis in leu- kemia. Arch Intern Med 1973; I3 1538-544.
8. Prolla JC, Kirsner JB. The gastrointestinal lesions and compli- cations of the leukemias. Ann Intern Med 1964; 6 I : 1084- 1 103.
9. Dosik GM, Luna M, Valdivieso M et a/. Necrotizing colitis in patients with cancer. Am J Med 1979; 67:646-656.
10. Rifkin GD. Neutropenic enterocolitis and Clostridium septi- cum infection in patients with agranulocytosis. Arch Intern Med 1980;
1 I . Geelhoed GW, Kane MA, Dale DC, Wells SA. Colon ulceration and perforation in cyclic neutropenia. J Pediutr Surg 1973; 8:379- 382.
12. Felitti VJ. Primary invasion by Clostridium sphenoides in a patient with periodic neutropenia. CaliJ‘Med 1970: I 13:76-78.
13. Bignold LP, Harvey HPB. Necrotising enterocolitis associated with invasion by Clostridium septicum complicating cyclic neutro- paenia. Aust N Z J Med 1979; 9:426-429.
109~34 1-350.
140:834-835.
14. Fernandez JMR, Gil GP. Enterocolitis neutropenica en agran- ulocitosis benigna. Sangre (Barc) 1980 25: 1 I 13- I 1 14.
15. Chapuis PG, Babaiants P, Delacretaz F. Enterocolites necro- santes: A propos d‘un cas associe a une agranulocytose. Chirurgie
16. Lehman JA, Armitage JO. Surgical intervention in complica- tions of acute leukemia. Postgrad Med 1980: 68:89-95.
17. Lea JW, Masys DR, Shackford SR. Typhlitis: A treatable com- plication of acute leukemia therapy. Cancer Clin Trials 1980: 3:355- 362.
18. Kies MS, Luedke DW, Boyd JF, McGee MJ. Neutropenic en- terocolitis: Two case reports of long-term survival following surgery. Cancer 1979; 43:730-734.
19. Ellison DC, Dragon RE, Linvingston WT, Toffolon EP, Smith CA. Surgical success with the medical failure of pseudomembranous colitis treatment. Conn Med 1980; 44: 10-13.
20. Seligman BR, Rosner F, Ritz ND. Major surgery in patients with acute leukemia. Am J Surg 1972; 124:629-633.
21. Ver Steeg K, LaSalle A, Ratner I. Appendicitis in acute leu- kemia. Arch Surg 1979; I14:632-633.
22. Varki AP, Armitage JO, Feagler JR. Typhlitis in acute leuke- mia: Successful treatment by early surgical intervention. Cancer 1979:
23. Archibald RB, Nelson JA. Necrotizing enterocolitis in acute leukemia: Radiographic findings. Gastrointest Radid 1978: 3:63-65.
24. Cronin TG, Calandra JD. Del Fava RL. Typhlitis presenting as toxic cecitis. Radiology 198 I: I38:29-30.
25. Del Fava RL, Cronin TG. Typhlitis complicating leukemia in an adult: Barium enema findings. Am J Roentgenol 1977: 129:347- 348.
26. Milligan DW, Kelly JK. Pseudomembranous colitis in a leu- kaemia unit: A report of five fatal cases. J Clin Pathul 1979; 32: 1237- 1243.
27. Alvear DT, Kain TM. Suppurative mesenteric lymphadenitis, a forgotten clinical entity: Report of two cases. J Pediarr Surg 1975: 10:969-970.
28. Blattner RJ. Comments on current literature: Acute mesenteric lymphadenitis. J Pediutr 1969: 74:479-48 I .
29. Milder MS, Click JH, Henderson ES. Johnston GS. 67Ga scin- tigraphy in acute leukemia. Cancer 1973: 32:803-808.
30. Dutcher JP, Schiffer CA, Johnston GS. Rapid migration of “‘indium-labelled granulocytes to sites of infection. N Engl J Med
31. Novak E, Lee JG, Seckman CE et a/. Unfavorable effect of atropine-diphenoxylate (Lomotile) therapy in lincomycin-caused diar- rhea. JAMA 1976; 235: 145 I .
32. Ackerman R, Mehta P. Acute leukemia mimicking acute a p pendicitis. J Flu MedAssoc 1981: 68:108-109.
33. Einhorn M. Temporary remission in acute leukemia after an attack of “acute appendicitis.” JAMA 196 I ; 175: 158- 160.
34. Charest LR, Holt CL. Acute myelogenous leukemia simulating acute appendicitis. J Maine Med Assoc 1954: 45:95-97.
35. Alavi JB, Root RK. Djerassi I ei a/. A randomized clinical trial of granulocyte transfusions for infection in acute leukemia. N Engl J
36. Herzig RH, Herzig GP, Craw RG, Bull MI, Ray KK. Successful granulocyte transfusion therapy for gram-negative septicemia. N Engl J Med 1977: 296:701-705.
37. Strauss RG. Connett JE, Gale RP er a/. A controlled trial of prophylactic granulocyte transfusions during initial induction che- motherapy for acute myelogenous leukemia. N Engl J Med 1981;
38. Higby DJ. Granulocyte transfusions: Where now? N Engl J
1974; 1W5 17-52 I .
43~695-697.
1981: 304~586-589.
Med 1977: 296~706-7 I I .
305~597-603.
Med (Editorial) 198 I: 305:636-637.