Embed Size (px)
Citation preview

Subthreshold Depression in the Elderly: Qualitative or Quantitative Distinction?
Bernhard Geiselmann and Michael Bauer
Recent studies revealed that subthreshold depression (or "subclinical" or "subsyndromal" depression) can have clinical validity because it is related to dysfunc- tion and disability and is a risk factor for major depression. However, none of these studies focused on old age. Therefore, one aim of the psychiatric part of the multidisciplinary Berlin Aging Study (BASE) was also to detect milder forms of psychopathological syndromes, especially subthreshold depression, com- pared with specified forms such as major depression
and dysthymia according to the DSM-III-R. The pres- ent evaluation shows that subthreshold depression can be characterized in 2 ways: firstly, as a quantita- tively minor variant of depression or a depression-like state with fewer symptoms or with less continuity; and secondly, as qualitatively different from major depression with fewer suicidal thoughts or feelings of guilt or worthlessness, while worries about health and weariness of living occur with a similar frequency. Copyright © 2000 by W.B. Saunders Company
S UBTHRESHOLD DEPRESSION has been de- fined as depressive syndromes which do not
qualify for formal mood disorder categories accord- ing to one of the modern operationalized diagnostic systems, especially not major depression according to the DSM classification. Several studies over the past 10 years revealed that subthreshold depressive states (or "subclinical" or "subsyndromal" depres- sion) can be associated with adverse clinical out- come, increased use of medical and mental health services, increased risk for future pronounced mood disorders, and increased social dysfunction and disability, v7 In the Zurich Study, Angst et al. 8 have demonstrated that recurrent brief depression among younger people has strong clinical validity. Conse- quently, this syndrome was introduced into the recent versions of the ICD and DSM diagnostic systems and is no longer subthreshold.
However, all of these studies did not specifically focus on old age. Several epidemiological studies found that the prevalence of major depression decreases but depressive symptoms increase in old age, 9,1° It has been reported that the DSM diagnos- tic criteria may be unsuitable for identification of old-age depression, and therefore, there may exist a significant prevalence of undetected depressive disorders. H This would be in line with the increase of suicide rates in old age. Erns0 2 suggested that
From the Department of Behavioral Therapy and Psychoso- matic Medicine, Klinik Seehof BfA, Teltow; and Department of Psychiatry, Benjamin Franklin University Hospital, Freie Uni- versitiit Berlin, Berlin, Germany.
Address reprint requests to Bernhard Geiselmann, M.D., Klinik Seehof BfA, Department of Behavioral Therapy and Psychosomatic Medicine, Lichterfelder Allee 55, D-14513 Tel- tow, Germany.
Copyright © 2000 by W.B. Saunders Company 0010-440X/00/4102-1006510.00/0
this shift from diagnoses to subthreshold syn- dromes may be due to a mitigation of severe symptoms with a selective mortality among early- onset major depressives, on one side, and a new vulnerability associated with somatic morbidity and organic brain disorders, on the other.
Is subthreshold depression in old age a variant of depression which is milder than major depression-- milder meaning that it causes less subjective suffer- ing and less disability? This would represent a quantitative distinction. On the other side, subthresh- old depression may be a qualitatively distinct variant with atypical psychopathology and different courses and correlates, but not necessarily milder.
METHODS
The Berlin Aging Study
The data presented are from the first cross-sectional wave of the Berlin Aging Study (BASE). The sample of the BASE is drawn from the city registry and comprises community-dwelling and institutionalized individuals of the western section of Berlin. The sample of 516 participants is stratified by age and sex. Forty-three men and 43 women were obtained in each of 6 5-year age groups from 70 to 100 years and older. The multidisciplinary assessment comprises 4 research units: psychia- try, internal medicine, psychology, and sociology. 13 For psychi- atric case-finding and diagnostic decision-making, the Geriatric Mental State Examination, community version A, and History and Aefiology Schedule (GMS-A/HAS) developed by Copeland et al. 14.15 was used. This is one of the most widely used structured psychiatric interviews in studies of old-age commu- nity samples. 16 It also provides case history data, observer data, and information on current life events and circumstances. All participants were examined by research psychiatrists. Diagnoses were made according to DSM-III-R and ICD-10.
Diagnostic Procedure and Threshold Definitions
In the diagnostic procedure, we introduced 3 thresholds, leading to 4 diagnostic groups: (1) no depressive symptoms, (2) depressive symptoms, (3) subthreshold depressive disorder, which is identical to the DSM-III-R "NOS depressive disorder,"
32 Comprehensive Psychiatry, Vol. 41, No. 2, Suppl. 1 (March/April), 2000: pp 32-38

SUBTHRESHOLD DEPRESSION IN THE ELDERLY 33
Threshold levels
1 9.1% I (C) Diagnostic specification: DSM-IIIR criteria
{e) Case finding: clinical judgement : ]
(A) Screening: depression score, core symptoms
• DSMJII-R diagnoses Major depr~sion N=23 Dysthymm N=I 1 Adjustment disorde" witt~ depressed mood N=5 Major depression in part~l remission N-3 Dementia w,th depression N=S
9.15 / (4) DSM'I&I'R ~Jn°ses"
1 N-a
i 13) s~r~ho~ ~pre.lve 17.8 ' k dlso,~r p,h~$ mmml (2) O,,p~=~.ve =y~ploms 839 N-~
(I) No depressive symptoms 731 N~las
Fig 1. Diagnostic procedure and prevalence of depression• Percentages are weighted for age and gender.
and (4) specified diagnoses according to DSM-III-R criteria, especially dysthymia and major depression (Fig 1).
(A) On the screening level, depressive symptoms were diagnosed if the GMS depression score was above the cutoff and included core symptoms such as depressed mood or diminished interest or suicidal ideation. Invalid answers, for example, by demented persons, were excluded on this level. (B) Since the DSM-III-R does not provide case-finding criteria, a standard- ized case-finding procedure had to be established. The case- finding level required a complex clinical judgment. First, hierarchies of syndromes had to be determined. For example, a coexistence of mild depressive symptoms and severe anxiety symptoms resulted in an anxiety disorder and no subthreshold depressive disorder. Second, uncomplicated life event reactions such as bereavement had to be excluded from the illness case level. Third, an impairment of psychosocial functioning caused by the depressive symptoms was rated using a Global Assess- ment of Functioning scale. All clinical judgments were dis- cussed in consensus conferences. (C) The diagnostic specifica- tion level was determined by the criteria for the specified
DSM-III-R categories. Specified minor depressive states such as dysthymia, adjustment disorders with depressed mood, or major depression in partial remission were DSM diagnoses, not subthreshold categories. The methodological procedure of the diagnostic decision-making process has been described else- where in detail. 17
Subjective Measures
In the BASE, different self-rating scales were used, which were administered in sessions separate from the psychiatric examination. The results of these rating scales were not used for the psychiatric diagnostic decision-making. The three scales used in this evaluation (life satisfaction, subjective health, and subjective mental health) consist of 1 question each, e.g., "How satisfied are you with life in general?". The scales are 5-point Likert scales limited by "very good" (1) and "very bad" (5).
RESULTS
DSM-III-R Criteria
The characteristics of subthreshold depressive disorder depend on the case-finding procedure, on one side, and the DSM-III-R diagnostic criteria, on the other (Fig 1). What are the consequences of the DSM-III-R criteria for the characteristics of sub- threshold depressive disorder? Major depression and dysthymia are the most important categories with the most elaborate criteria in DSM-III-R. They include 2 main components: (1) presence of symp- toms and severity of syndromes and (2) time criteria such as continuity and duration characteris- tics of symptoms (Table 1).
Table 1. Measures Used in the Present Evaluation and Their Qual i ty /Quant i ty Characteristics
Quality/Quantity Measure Major Depression Dysthymia Characteristics
Presence of symptoms and severity of syndromes (DSM-III-R)
Core symptoms
Additional symptoms
Symptom score
Symptom profile "13me criteria (DSM-III-R)
Continuity Duration
Subjective measures
Depressed mood Depressed mood Quality Anhedonia Weight or appetite Appetite Quality and quantity Sleep Sleep Psychomotor Energy Loss of energy Self-esteem Guilt or worthlessness Concentration Concentration Hopelessness Suicidality Depressed mood and anhedonia + 3 Depressed mood + 2 additional Quantity
additional symptoms or either symptoms depressed mood or anhedonia + 4 additional symptoms
Most of the day, continuously Most of the day, more days than not 2 weeks 2 years Life satisfaction, subjective health, subjective mental health
Quality
Quality and quantity Quality or quantity Quantity

34 GEISELMANN AND BAUER
Presence of Symptoms and Severity of Syndromes
The mandatory core symptoms "depressed mood" and "anhedonia" certainly signify the psy- chopathologically most important qualitative crite- rion for depression. Therefore, some atypical depres- sive syndromes which are present with somatic symptoms or anxiety or feelings of guilt but not with depressed mood or anhedonia are excluded by these criteria. Since depressed mood or anhedonia were also mandatory for the subthreshold depres- sion in the BASE study, subjects who did not endorse depressed mood and anhedonia are not represented in the subthreshold depression cat- egory.
The most reliable method to assess depressive syndromes in epidemiological studies is to use rating scales. For example, a scale score may represent a quantitative continuum and a cutoff may provide a quantitative distinction between milder and more severe syndromes. Thus, the 5 out of 9 cutoff on the major depression symptom list may warrant a certain degree of severity, and subthreshold may signify a quantitatively less se- vere category. However, even some severe depres- sive states may not be covered by the criteria. For example, a person with depressive delusions usu- ally has a severe form of depression, even if he or she presents with less than 5 of the 9 major depressive symptoms. Therefore, the symptoms presented in the list also signify a qualitative characteristic, which can be best demonstrated using a symptom profile (described later).
Duration and Continuity of Symptoms
Duration and continuity criteria should ensure that a depressive state does not lose clinical validity because of its temporariness. Major depression requires a continuous presence of symptoms for 2 weeks or longer, dysthymia in the presence of depressed mood for most of the day, more days than not, for at least 2 years. At first glance, the continuity and duration of symptoms may clearly represent a quantitative threshold. Discontinuous symptoms may be less disabling. However, fre- quently recurring symptoms may be of clinical significance, as established for recurrent brief de- pression. Therefore, certain subthreshold time pat- terns may exist which represent qualitatively dis- tinct rather than milder forms of depression. The 2-year criterion of dysthymia is a threshold for chronicity, which is also a qualitative characteris-
tic, whereas the 2-week criterion of major depres- sion seems to ensure a minimum of illness quantity.
Combination of Criteria
The combination of these types of criteria results in a complex threshold construct. If only 1 of the criteria is missed, a depressive syndrome becomes subthreshold. Consequently, the subthreshold cat- egory is certainly psychopathologically less homo- geneous than major depression or dysthymia. Why did the subthreshold cases of the BASE study fail to meet the DSM-III-R criteria?
Whereas 81% of the subthreshold subjects ful- filled the symptom criterion, only 7% met the continuity criterion for the duration period, and the duration period was more than 2 years in only 46% of the cases (Table 2). Information about the duration seemed very unreliable, and 20% were missing data. Thus, at most 6 more subjects would shift to the dysthymia category if they had more symptoms or a longer duration. Twenty-one per- cent fulfilled the 2-week depression or anhedonia criterion of major depression. Therefore, at least 18 more subjects would shift to the major depression category if they had more symptoms. This is shown once more in Fig 2. The figure also demonstrates that all of the major depression cases on the fight are close to the threshold. With 1 symptom less, 11
Table 2. DSM-III-R Dysthymia and Major Depression Criteria Applied to Subjects With Subthreshold Depressive Disorder
Subjects Meeting Criterion (n = 85)
Criteria % No.
Dysthymia Core symptom with continuity
Depressed mood most of the day most of the time 7.1 6
Symptom score >2 of 6 symptoms 81.2 69
Duration of symptoms >2 years 45.9 39 <2 years 34.1 29 Missing data 20.0 17
Major depression Core symptom with continuity
and duration Depressed mood or anhedonia
most of the day continuously for 2 weeks past month 21.2 18
Symptom score* ->3 of 9 symptoms 23.5 20 >-4 of 9 symptoms 15.3 13
*See Table 1.
S U B T H R E S H O L D D E P R E S S I O N I N T H E E L D E R L Y 3 5
of 23 subjects would shift to the subthreshold group. The combination of low symptom scores for the major depression symptoms and a failure to meet the dysthymia continuity criteria points to a quantitative rather than a qualitative distinction in our sample.
Symptom Profiles
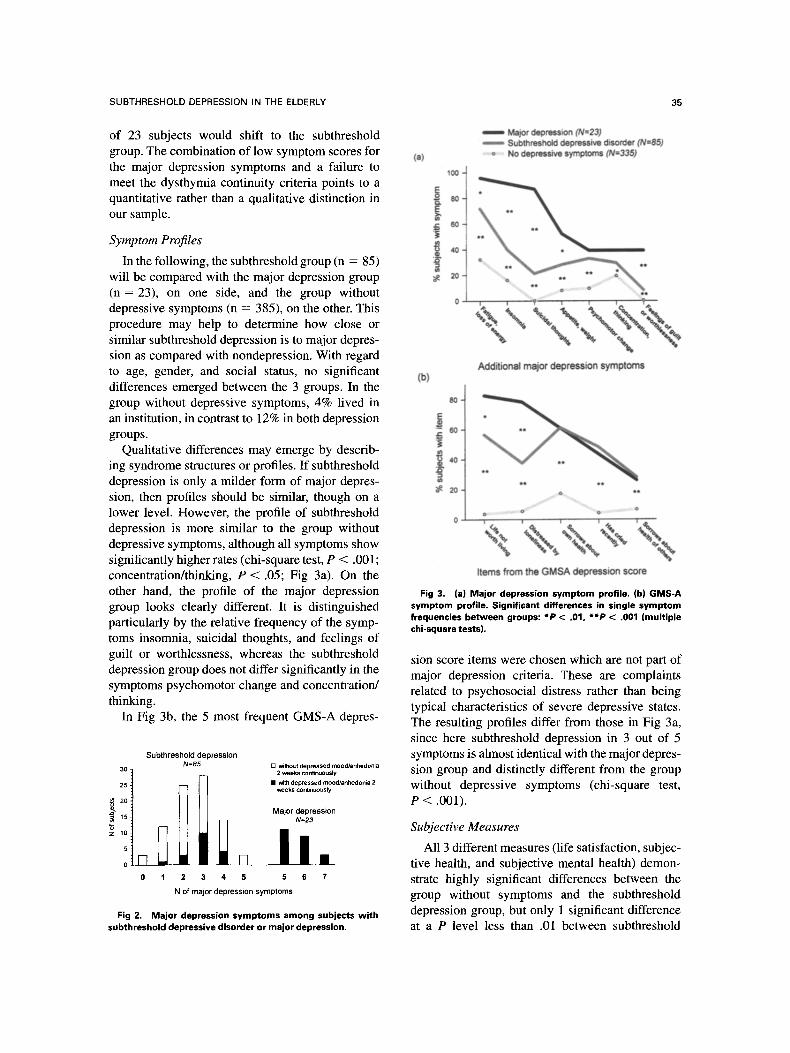
In the following, the subthreshold group (n = 85) will be compared with the major depression group (n = 23), on one side, and the group without depressive symptoms (n = 385), on the other. This procedure may help to determine how close or similar subthreshold depression is to major depres- sion as compared with nondepression. With regard to age, gender, and social status, no significant differences emerged between the 3 groups. In the group without depressive symptoms, 4% lived in an institution, in contrast to 12% in both depression groups.
Qualitative differences may emerge by describ- ing syndrome structures or profiles. If subthreshold depression is only a milder form of major depres- sion, then profiles should be similar, though on a lower level. However, the profile of subthreshold depression is more similar to the group without depressive symptoms, although all symptoms show significantly higher rates (chi-square test, P < .001; concentration/thinking, P < .05; Fig 3a). On the other hand, the profile of the major depression group looks clearly different. It is distinguished particularly by the relative frequency of the symp- toms insomnia, suicidal thoughts, and feelings of guilt or worthlessness, whereas the subthreshold depression group does not differ significantly in the symptoms psychomotor change and concentration/ thinking.
In Fig 3b, the 5 most frequent GMS-A depres-
30
25
"6 Z H)
5
0
S u b t h r e s h o l d depression N=85
0 1 2 3 4
[q
5
[ ] without depressed mood/anhedo~a 2 weeks conUnuously
• ~ depressed mood/anhedonia 2 weeks con6nuously
Major depression N=23
I t . 5 6 7
N of ma jor depress ion symptoms
Fig 2. Major depression symptoms among subjects with subthreshold depressive disorder or major depression,
I Major depression (N=23) I Subthreshold depressive disorder (N=85)
(a) o No depressive symptoms (N=335)
Additional major depression symptoms (b)
~ 40-
2 0 - * * o .
• ~ e o , e
Items from the GMSA depression score
Fig 3. (a) Major depression symptom profile. (b) GMS-A symptom profile. Significant differences in single symptom frequencies between groups: *P < .01, **P < .001 (multiple chi-square tests).
sion score items were chosen which are not part of major depression criteria. These are complaints related to psychosocial distress rather than being typical characteristics of severe depressive states. The resulting profiles differ from those in Fig 3a, since here subthreshold depression in 3 out of 5 symptoms is almost identical with the major depres- sion group and distinctly different from the group without depressive symptoms (chi-square test, P < .001).
Subjective Measures
All 3 different measures (life satisfaction, subjec- tive health, and subjective mental health) demon- strate highly significant differences between the group without symptoms and the subthreshold depression group, but only 1 significant difference at a P level less than .01 between subthreshold

36 GEISELMANN AND BAUER
depression and major depression, namely regarding subjective mental health. Together, all measures represent a pronounced amount of distress related to subthreshold depression.
DISCUSSION
The aim of the present evaluation was to answer the question of whether subthreshold depression in old age is a milder form of depression, causing less suffering and less disability (quantitative distinc- tion), or rather a distinct age-specific variant of depression comparable to DSM-III-R specified forms of depression such as major depression or dysthymia. Most of the indicators used suggest that the subthreshold depressive disorder represents a heterogeneous group of milder forms of depres- sion, at least milder than major depression, with qualitatively distinct symptom patterns.
Looking at the dysthymia and major depression criteria reveals that a majority of subthreshold depressives fail to fulfill the time and continuity criteria of both forms of depression. Only 21% reported depressed mood or anhedonia continu- ously for 2 weeks (major depression criterion), while only 7% reported depressed mood continu- ously over longer durations of depression, even if durations shorter than 2 years are not excluded. The discontinuity of symptoms may represent an age- specific pattern in both a qualitative and quantita- tive sense.
It might be argued that some of the results are age-related methodological artifacts. Information about the duration and continuity of symptoms is
extremely difficult to gather in very old persons, and is probably invalid in a considerable proportion of subjects due to impaired concentration, loss of hearing, inadequate answers, or nonresponsive- ness. Moreover, depressed mood in older persons should be inferred or observed rather than elicited by single questions, because old respondents may tend to deny depression or to somatize. 18 On the other hand, depressive feelings may be confused with dysphoria or unwellness which are not primar- ily mood-related. However, our results are at least partly consistent with other studies, l which did not specifically focus on old age. For example, Judd et al. 5 also found a relatively high prevalence of subthreshold depression in the general population ("subsyndromal symptomatic depression," 8.4%). It was characterized by a lower frequency of major depression symptoms and a failure to meet the DSM-III major depression A criterion (depressed mood with continuous depressed mood over 2 weeks). Only 30.4% endorsed this criterion, com- pared with 21.2% in our study. Broadhead et al. 1 reported that approximately 20% of their depressed symptom group ("minor depression with mood disturbance") endorsed this symptom.
Regarding the additional symptoms, the major depression criterion is met only by a minority of subthreshold depressives (24% or 14%), whereas the criterion of dysthymia is met by 81%. This may indicate that subthreshold depression is at least milder than major depression, keeping in mind that our cases of major depression are comparatively milder according to the number of DSM-III-R-
Life satisfaction Subjective health Subjective mental health
NS
Scheffd test: * p < 01
p < .001
sD .D is sb .D is sb MD
Depresslon groups: NS = no symptoms SD = subthreshold depressive disorder MD = major depression
H~
8
Fig 4. Self-rating measures with a 5-point Likert-type scale limited by "very good" (1) and "very bad" (5).

SUBTHRESHOLD DEPRESSION IN THE ELDERLY 37
symptoms (Fig 2). However, looking at the symp- tom profiles shows that subthreshold depression may also be qualitatively distinct from major depression (Fig 3a). The similarity of the profile of the subthreshold depression group versus the group without symptoms suggests that subthreshold de- pression may represent a syndrome which could be labeled dysphoria or distress rather than depres- sion. In other studies as well, older depressed individuals were observed to complain less in- tensely about single symptoms such as depressed mood, loss of appetite, and fatigue. Fogel and Fretwell, 19 as well as Newmann et al.,20 have termed such age-typical depression-like conditions "depletion syndrome." However, it may not be possible to demonstrate the clinical relevance of this condition using the DSM-III-R symptom pro- file. On the contrary, the GMS-A item profile (Fig 3b) shows that worries and subjective distress due to (real or imagined) health and psychosocial life circumstances are almost as pronounced in sub- threshold depression as in major depression.
Strbthreshold depression is clearly related to diminished life satisfaction, as well as worsened subjective health or mental health, in comparison to subjects without depressive symptoms (Fig 4). Thus, subthreshold depression can be characterized as a condition in which the symptoms and continu- ity of a classic depressive disorder such as major depression are not overt, but in which---compared with subjects without depressive symptoms--the individual experiences pronounced psychological distress.
There are some restrictions to the generalizabil- ity of the present results. First, considering that the
BASE is a community-based study with extensive assessments in multiple sessions, persons with severe forms of major depression were certainly among the nonparticipants. Therefore, comparisons of subthreshold depression with major depression would reveal more pronounced differences if se- vere major depressives also could have been in- cluded. Second, psychiatric comorbidity such as organic mental disorders and physical comorbidity, as well as social factors, were not considered. Therefore, the effects and consequences of sub- threshold depression also could be due to related conditions such as cognitive impairment, physical illness or disability, and social isolation. Third, the subthreshold depression group is probably an etio- logically and psychopathologically very heteroge- neous group. It is possible that a certain subgroup of the subthreshold depressions may be of special clinical relevance. Further evaluations should con- sider this issue.
ACKNOWLEDGMENT
This research is part of the multidisciplinary BASE. The BASE is conducted by the Research Group on Aging and Societal Development of the Berlin-Brandenburg Academy of Sciences in collaboration with the Free University of Berlin, the Humboldt University Berlin, and the Max Planck Institute for Human Development and Education, Berlin. The project has been supported financially by several organizations, including the German Federal Ministry for Research and Technology (1989-1991, 13 TA 0 1 1 + 13.TA 0l l/A) and the German Federal Ministry for Family, Senior Citizens, Women, and Youth (1992-1998; 314-1722-102/9 + 314-1722-102/9a). The BASE is directed by a steering committee consisting of P.B. Baltes (chair), K.U. Mayer (vice-chair), H. Helmchen, and E. Steinha- gen-Thiessen.
REFERENCES
1. Broadhead WE, Blazer DG, George LK, Tse CK. Depres- sion, disability days, and days lost from work in a prospective epidemiologic survey. JAMA 1990;264:2524-2528.
2. Copeland JRM, Davidson IA, Dewey ME, Gilmore C, Larkin BA, McWilliam C, et al. Alzheimer's disease, other dementias, depression and pseudodementia: prevalence, inci- dence and three-year outcome in Liverpool. Br J Psychiatry 1992; 161:230-239.
3. Coulehan JL, Schulberg HC, Block MR, Janosky JE, Arena VC. Depressive symptomatology and medical co- morbidity in a primary care clinic. Int J Psychiatry Med 1990;20:335-347.
4. Horwath E, Johnson J, Klerman GL, Weissman MM. Depressive symptoms as relative and attributable risk factors for first-onset major depression. Arch Gen Psychiatry 1992;49:817- 823.
5. Judd LJ, Rapaport MH, Paulus MP, Brown JL. Subsyndro-
mal symptomatic depression: a new mood disorder? J Clin Psychiatry 1994;55(4 Suppl): 18-28.
6. Sherbourne CD, Wells KB, Hays RD, Rogers W, Burnam MA, Judd LL. Subthreshold depression and depressive disorder: clinical characteristics of general medical and mental health specialty outpatients. Am J Psychiatry 1994; 151:1777-1784.
7. Wells KB, Bumam MA, Rogers W, Hays RD, Camp P. The course of depression in adult outpatients: results from the Medical Outcomes Study. Arch Gen Psychiatry 1992;49:788- 794.
8. Angst J, Merikangas K, Scheidegger P, Wicki W. Recur- rent brief depression: a new subtype of affective disorder. J Affect Disord 1990;19:87-98.
9. Blazer D, Williams CD. Epidemiology of dysphoria and depression in an elderly population. Am J Psychiatry 1980;137: 439-444.
10. Ernst C, Angst J. Depression in old age. Is there a real

38 GEISELMANN AND BAUER
decrease in prevalence? A review. Eur Arch Psychiatry Clin Neurosci 1995;45:272-287.
11. Blazer D. Clinical features in depression in old age: a case for minor depression. Curr Opin Psychiatry 1991;4:596- 599.
12. Ernst C. Epidemiology of depression in late life. Curt Opin Psychiatry 1997; 10:107-112.
13. Baltes PB, Mayer KU, Helmchen H, Steinhagen- Thiessen E. The Berlin Aging Study (BASE): Sample, design, and overview of measures. In: Baltes PB, Mayer KU (eds): The Berlin Aging Study: Aging From 70 to 100. New York, NY: Cambridge University Press; 1999;15-55.
14. Copeland JRM, Dewey ME, Griffiths-Jones HM. A computerized diagnostic system and case nomenclature for elderly subjects: GMS and AGECAT. Psychol Med 1986;16: 89-99.
15. McWilliam C, Copeland JRM, Dewey ME, Wood M. The
Geriatric Mental State Examination. A case-finding instrument in the community. Br J Psychiatry 1988;152:205-208.
16. Katona CLE. Depression in Old Age. Chapter 2. The Measurement of Depression in Old Age. Chichester, UK: Wiley, 1994:11-28.
17. Helmchen H, Baltes MM, Geiselmann B, Kanowski S, Linden M, Reischies FM, et al. Psychiatric illnesses in old age. In: Baltes PB, Mayer KU (eds): The Berlin Aging Study: Aging From 70 to 100. New York, NY: Cambridge University Press; 1999;167-196.
18. Snowdon J. Editorial. The prevalence of depression in old age. Psychiatry 1990;5:141 - 144.
19. Fogel BS, Fretwell M. Reclassification of depression in the medically ill elderly. J Am Geriatr Soc 1985;33:446-448.
20. Newmann JP, Engel RJ, Jensen JE. Age differences in depressive symptom experience. J Gerontol 1991 ;46:224-235.





























