Embed Size (px)
Citation preview
Subelavian Steal in Patients withBlalock-Taussig Anastomosis
By GORDON M. FOLGER, JR., M.D., AND KIsHOR D. SHAH, M.D.
ALTHOUGH the collateral anastomoticchannels that occur secondary to ob-
struction of the first segment of the subclavianartery have received relatively little commentby anatomists, the participation by the verte-bral artery in such instances has been men-tioned.' Recently, the finding of retrogradeflow from the vertebral artery on the side ofan obstruction in the first part of the sub-clavian artery to the distal segment of thatsubelavian artery has been noted by severalinvestigators.2-10 Anatomically, obstructionmay be complete or, if partial, of sufficientseverity to lower the pressure in the sub-clavian artery to below that in the vertebralartery. The reversal of flow, demonstrableangiographically, may cause basilar arteryinsufficiency giving rise to symptoms ofheadache, visual disturbance, paresthesia,hemiparesis, dizziness, and syncope. This con-dition, first reported by Reivich and co-work-ers,2 has been termed the "subelavian stealsyndrome."" With the exception of one re-port,12 the subelavian obstruction in all thecases of the entity recorded to date has beenon the basis of atherosclerotic disease withinthe vessel.
Anastomosis of subelavian artery to pul-monary artery13 has been performed since1945 on a large number of patients sufferingfrom cardiac anomalies associated with pul-monary stenosis or atresia. On the assump-tion that patients treated in this mannermight exhibit the subelavian steal angiograms
From the Cardiac Clinic, Children's Medical andSurgical Center of the Johns Hopkins Hospital andthe Departments of Pediatrics and Medicine, TheJohns Hopkins University School of Medicine, Balti-more, Maryland.
Supported in part by Training Grant 5-T1-JE-5405-04, National Institutes of Health, U. S. Public HealthService.
Circuclation, Volume XXXl, February 1965
performed at the Johns Hopkins Hospital onsuch patients between 1961 and 1964 werereviewed with specific attention directed tothe manner of opacification of the subclavianartery distal to the anastomotic site. The fol-lowing report concerns the findings in 12 pa-tients with Blalock-Taussig anastomoses whohave shown evidence of the subelavian steal.To our knowledge this condition in patientsso treated has not previously been reported.
Materials and MethodsA total of 123 biplane angiocardiograms done
by the selective injection of contrast material intoeither the right or left ventricular cavity was re-viewed. Only frontal projections were examined.Exposure speeds varied somewhat, with the ma-jority of studies performed at four or six framesper second.
Care was taken to include only angiocardio-grams of those patients having a subclavian ar-tery to pulmonary artery anastomosis and onlyangiocardiograms that were satisfactory from alltechnical aspects. After this selection 114 angio-cardiograms were acceptable for analysis.The acceptable angiocardiograms were then
subdivided into four groups. Group 1 consistedof 12 studies that were considered to have distinctevidence of late filling of the distal subclavianartery from the vertebral artery on the side ofthe Blalock-Taussig anastomosis. Group 2 consist-ed of eight angiocardiograms that revealed latefilling of the distal subclavian artery from an anas-tomotic channel other than the vertebral artery onthe side of the Blalock-Taussig anastomosis. In-terestingly, one patient with bilateral anastomosesdemonstrated findings of group 1 on one side andgroup 2 on the other and is included in bothgroups. In group 3 were 91 angiocardiograms inwhich late filling of the distal subclavian artery onthe side of the Blalock-Taussig anastomosis wasapparent but the contributing anastomotic chan-nels could not be positively identified. Group 4was comprised of four angiocardiograms in whichthe distal subclavian artery on the side of theBlalock-Taussig anastomosis never opacified. Thiswas an unexpected occurrence and the numberof studies in this group is understandably small.
In groups 1 and 2 the charts of the patients241
by guest on July 4, 2018http://circ.ahajournals.org/
Dow
nloaded from
FOLGER, SHAH
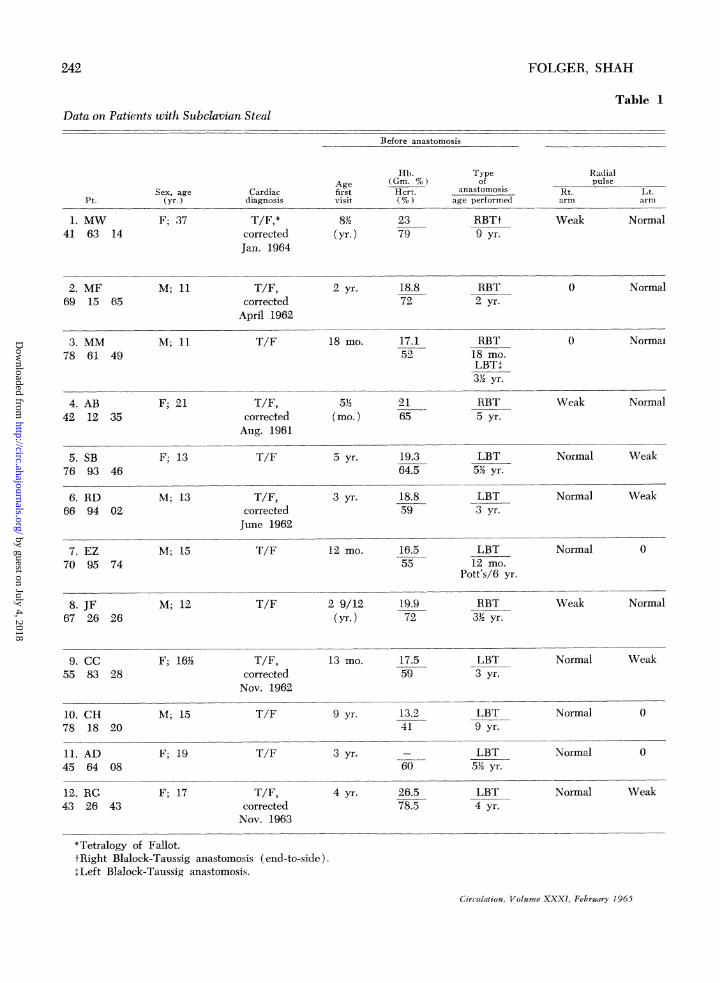
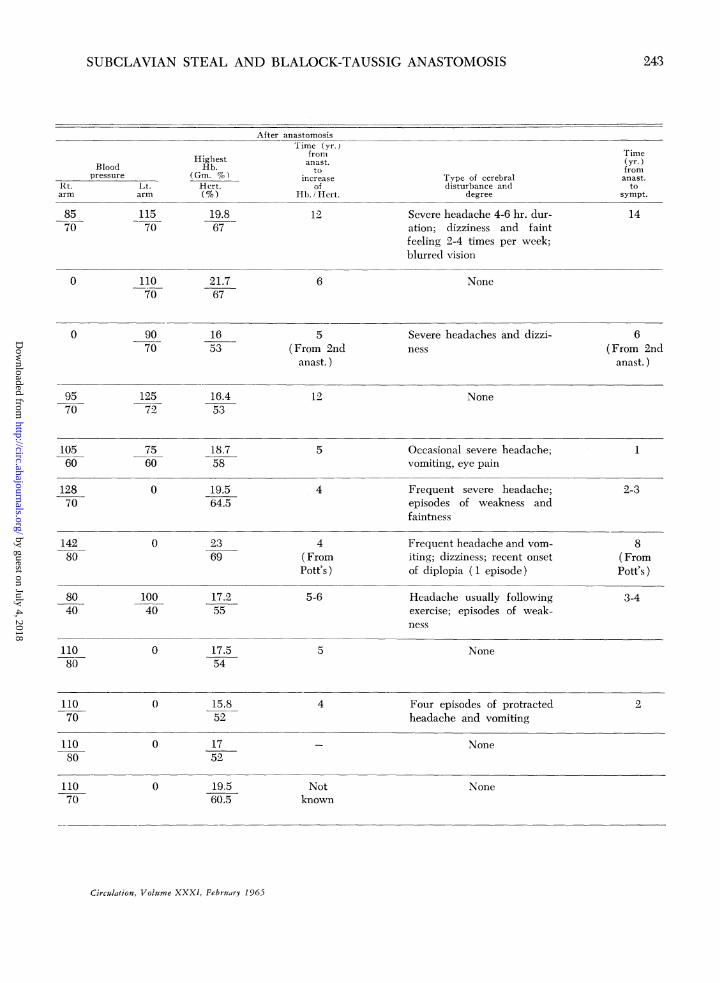
Table IData on Patients with Subclavian Steal
Before anastomosis
Radialpulse
Rt. Lt.arm arm
Weak Normal
0 Normal
3. MM78 61 49
4. AB42 12 35
5. SB76 93 46
6. RD66 94 02
M; 11
F; 21
F; 13
M; 13
7. EZ M; 1570 95 74
T/F
T/F,correctedAug. 1961
T/F
T/F,correctedJune 1962
T/F
18 mo. 17.152
5j2(mo.)
5 yr.
3 yr.
2165
19.364.5
18.859
12 mo. 16.555
RBT18 mo.LBT+332 yr.
RBT5 yr.
LBT52 yr.
LBT3 yr.
LBT12 mo.
Pott's/6 yr.
0
Weak
Norma!
Normal
Normal Weak
Normal Weak
Normal 0
2 9/12 19.9(yr.) 72
13 mo.
9 yr.
3 yr.
4 yr.
17.559
13.241
60
26.578.5
RBT332 yr.
LBT3 yr.
LBT9 yr.
LBT52 yr.
LBT4 yr.
Weak Normal
Normal Weak
Normal
Normal
0
0
Normal Weak
*Tetralogy of Fallot.tRight Blalock-Taussig anastomosis (end-to-side).++Left Blalock-Taussig anastomosis.
Circulation, Volume XXXI, February 1965
242
Pt.
1. MW41 63 14
2. MF69 15 65
Sex, age(yr.)
F; 37
M; 11
Cardiacdiagnosis
T/F,*correctedJan. 1964
T/F,correctedApril 1962
Agefirstvisit
8,'(yr.)
2 yr.
Hb.(Gm. %)Hcrt.
2379
18.872
Typeof
anastomosisage performed
RBTt9 yr.
RBT2 yr.
8. JF67 26 26
9. CC55 83 28
10. CH78 18 20
11. AD45 64 08
12. RG43 26 43
M; 12
F; 16/2'
M; 15
F; 19
F; 17
T/F
T/F,correctedNov. 1962
T/F
T/F
T/F,correctedNov. 1963
by guest on July 4, 2018http://circ.ahajournals.org/
Dow
nloaded from
SUBCLAVIAN STEAL AND BLALOCK-TAUSSIG ANASTOMOSIS
HighestHb.
(Gm. %)Lt. Hcrt.arm (%)
11570
110
19.867
21.767
After anastomosisTime (yr.)
fromanast.
toincrease
ofHb. i Hcrt.
12
6
Time(yr.)fromanast.
tosympt.
14
Type of cerebraldisturbance and
degree
Severe headache 4-6 hr. dur-ation; dizziness and faintfeeling 2-4 times per week;blurred vision
None
90 1670 53
12572
7560
16.453
18.758
0 19.564.5
0 2369
10040
0
0
0
0
17.255
17.554
15.852
1752
19.560.5
5(From 2nd
anast. )
12
5
4
4(FromPott's )
5-6
5
4
Notknown
Severe headaches and dizzi- 6ness (From 2nd
anast. )
None
Occasional severe headache;vomiting, eye pain
Frequent severe headache;episodes of weakness andfaintness
Frequent headache and vom-iting; dizziness; recent onsetof diplopia ( 1 episode)
Headache usually followingexercise; episodes of weak-ness
None
Four episodes of protractedheadache and vomiting
None
1
2-3
8(FromPott's )
3-4
2
None
Circulation, Volume XXXI, February 1965
243
Bloodpressure
Rt.arm
8570
0
0
9570
10560
12870
14280
8040
11080
11070
11080
11070
by guest on July 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

FOLGER, SHAH
were reviewed, questionnaires were sent to allsurviving patients, and when possible the patientsthemselves were examined for findings suggestingbasilar artery insufficiency. All the available ma-terial was evaluated with respect to neurologicsymptoms and their temporal relationships toanastomotic procedures, degrees of peripheraloxygen desaturation, and, when pertinent, the ef-fect of total correction of the cardiac malformation.
The patients in groups 3 and 4 were of neces-sity excluded from further analysis in view of theinability to demonstrate adequately the vascularpathways leading to the involved subclavian ar-tery.
Case Analysis
The pertinent data on all 12 patients comprisinggroup 1 are summarized in table 1. The cardiacmalformation in all is the tetralogy of Fallot. Allthe patien-ts are Caucasian. Four of these patientsare briefly described as follows.
Case 1M.W. (JHH no. 41 63 14) is a 37-year-old
housewife who has been followed in the CardiacClinic since the age of 8 years with the diagnosisof tetralogy of Fallot. Because of increasing cy-anosis in 1947, at the age of 10 years, she under-went anastomosis of the end of the right subclavi-an artery to the side of the right pulmonary arterywith satisfactory improvement, and she was ableto lead a normal life for 14 years. Throughoutthis period the physical findings were those oftetralogy of Fallot with a functioning Blalock-Taussig anastomosis. Moderate polycythemia per-sisted, which increased gradually although neverreaching alarmingly high levels. Pulses were al-ways obtainable, though weaker in the right armthan in the left; blood pressure in the right armwas 85/70 mm. Hg compared to 120/55 mm. Hgin the left arm.The patient delivered a 42-pound stillborn in-
fant in 1959, but in 1960 she gave birth to a 5-pound 4-ounce normal infant after a full-termpregnancy.
Six months later she met with a minor autoaccident following which she noted the onset ofdizzy spells and severe headaches, although therewas no evidence of central nervous system injury.The headaches occurred several times daily, oftenlasting for a number of hours, and were unrelatedto exertion or posture. Hemoglobin and hematocritvalues at this time were 18.2 Gm. per cent and62 per cent, respectively.
Right ventricular selective angiocardiographyin 1963 revealed typical findings of tetralogy ofFallot. The left vertebral and subclavian arterieswere seen to opacify normally from the arch ofthe aorta 22 seconds after the injection. Retro-
grade opacification of the right vertebral and sub-sequently the right subclavian arteries was ob-served 4% seconds later.The following year she underwent total correc-
tion of her cardiac defect with the use of cardio-pulmonary bypass. Four months postoperativelyshe is leading a normal life and has had no recur-rence of headache or dizziness.
CommentThis patient had symptoms suggestive of basilar
artery insufficiency 14 years after creation of aBlalock-Taussig anastomosis. At this time therewas no evidence of increasing hypoxemia and justprior to this she was capable of carrying a preg-nancy to full term satisfactorily. Although theautomobile accident in which she was involvedmay have contributed to this problem, she wasnot known to have suffered injuryv, and severalexaminations failed to uncover evidence of cere-bral trauma. Selective angiocardiography con-firmed retrograde filling of the right subelavianartery by way of the right vertebral artery.
Case 2M.F. (JHH no. 69 15 65) is an 11-year-old boy
wvho was first seen at the age of 9 months becauseof cyanosis and cyanotic spells. He was diag-nosed as having tetralogy of Fallot. In view ofincreasing cyanosis, anastomosis of the end of theright subclavian to the side of the right pulmonaryartery was performed at 2 years of age followedby marked improvement.He was able to lead an active, unrestricted
life over the following 4i2 years. From this time,however, he gradually developed noticeable fatig-ability and when seen 5i2 years postoperativelyhe had significant polycythemia with hemoglobinand hematocrit values of 18 Gm. per cent and 60per cent, respectively. He was only slightly cy-anotic and the continuous murmur originatingfrom the anastomosis was satisfactory.When seen 71 years postoperatively he was
markedly incapacitated. His cyanosis had deep-ened and his hemoglobin had risen to 21.3 Gm.per cent with a hematocrit value of 67 per cent.At no time were blood pressures or pulses re-corded in the right arm.A right ventricular selective angiocardiogram
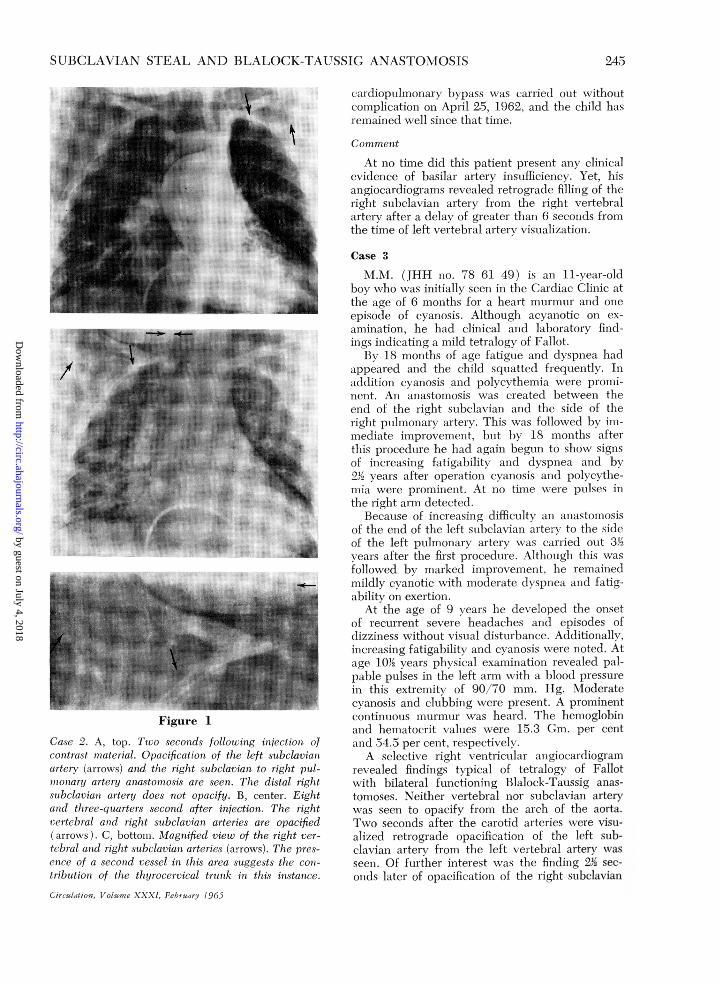
revealed findings typical of tetralogy of Fallot.The left subelavian and vertebral arteries wereseen to opacify from the arch of the aorta 2 sec-onds following injection (fig. 1A); opacificationof the right subclavian artery in a retrograde man-ner from the right vertebral artery was observed834 seconds from injection, a lag of 6% seconds fromopacification of the left vertebral artery (fig. 1Band C).
Total correction of his tetralogy of Fallot underCirculation, Volume XXXIJ February 1965
244
by guest on July 4, 2018http://circ.ahajournals.org/
Dow
nloaded from
SUBCLAVIAN STEAL AND BLALOCK-TAUSSIG ANASlTOMOSOSIS
Figure 1
Case 2. A, top. Ilwo seconds followiing inijectioni. ofcontfrast mfater ial. Opacification of thie left subclaviaInartery (arrow s) and the righ7t subclavian to right puil-
monary artery anastonuosis ar1e seen1. The distal r'ighltsubclavian artery does not opacify. B, ceniter. Eightand three-q1uarters seconid after injectioni. The rightvertebral andcl righlt suibclaviatn arteries are opacified(arrowvs). C, bottomii. AMagnified view of the right ver-
tebrial and uight snibclaviat arteries (arrows). The pres-
ence of a seconid vessel in this area suggests the coJI-tribuitiotn of the thiyr ocervical tr llsku in this instance.
Circauilion, Volume XXXI, Febrtuay 10965
c'ardiopulmonarv bypass was cai-i-ied ouit withoutcomplication oni April 25, 1962, and the child hasreminained well sinice that time.
Commet t
At no time did this patient present ainyv clinicalevidenice of basilar artery inisufficiencxv. Yet, hisangiocardiograms revealed retrograde filling of theright stubelavian artery from the right vertebralartery after a delay of greater thani 6 seconds fromthe time of left vertebl)al arteu-v visualizationi.
Case 3
M.M. (JHmH no. 78 61 49) is an 1 -year0-oldlovy xvho wvas initially seen in the Cardiac Clinic atthe age of 6 months for a heart murmuir anid oneepisode of cyan.osis. Although acvanotic oni ex-amilnation, he had clinical and laboratory finid-inigs inidicating a mild tetralogv of Fallot.
By7 18 monthbs of age fatigue and dyspniea hadappeared and the child squiatted frequently. Indldition- evtynosis and polvcvtthemia xvere pr-omi-
nienit. An anastomosis xvas created between- theen(I of the right subclaviani aind the side of theiight puilmonaryv arter y. This xvas followed by im-me(liate im-provemient, but by 18 ns-onths afterthis procedture he had againi begunii to shoxx signsof increasinig fatigability anid dyspnea andcl bv212 vears after operationi cvainosis and polycythe-mctia were promiuneuit. At io tiumie were puilses inthe right ariiii detected.
Becauise of incr-easintg difficulty an anlastoln)isisof the end of the left stibclaviain arteuxv to the sideof the left ptulmionary arter-v xvas caLiiied ouit 33M>vears after the fir-st procedture. Although this wcasfolloxed bv mar-ked im-provemiien-t, he reemainedlmildlv cyaniotic xvith moderate dyspnea aiid fatig-abilitv on exertion.
At the age of 9 vears lhe developed the onsetof recurrent sever-e headaches and episodes ofdizziness vithouit visuial disturibance. Additionally,increasinig fatigabilitv anid cvanosis xvere nioted. Atage 10'2 vears physical examiination r-evealed pal-pable pulses in the left anm xitlh a blood pressurein this extremlity of 90/70 mm. Hg. Moderatecyanosis anid clubbing vere presenit. A prominentconitinutous mulrnmuri- wvas hearcl. The hiemoglobinand liemi-atocrit valtues xwere 1 5.3 G1. per centan:d 54..5 per- cenit, respectivelv.A selective right ventrictilar angiocardiograim
-evealed finidinigs typical of tetr alogv of Fallotx ith bilateral functioning Blalock-Taussig anas-tomoses. Neither vertebral nor- subclaviani arteryxvas seeni to opacify fr-om the arch of the aorta.Tvo seconds after the carotid arteries were visui-alized retrograde opacification of the left sub-claviain arterv fromi the left vertebral arterv wasseen. Of further initerest xvas the finiding 22' sec-oinds later of opacificationi of the right stibelavian
245-
by guest on July 4, 2018http://circ.ahajournals.org/
Dow
nloaded from
FO24F(Y'O(EII, SIIAlI
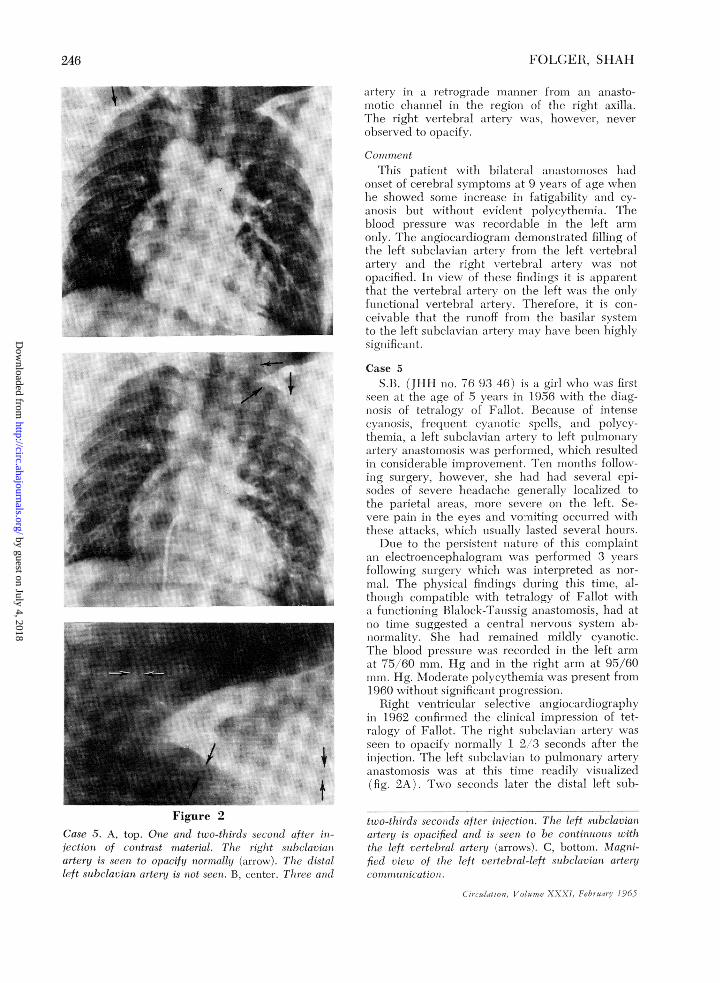
Figure 2
Case 5. A, top. Onie and ttco-tl'/tids Stsconti of/cr in-jection of contrast matecria. 7I/te rig/it .sabclavtianar-tery is seeni to opacify niormalbl (art eoxx). distailleft slnbclaviant iarteryl is not seen. B, centet- Ilitte anda
artcrv ill a retiograde 1miamer frm lla aiLtlsto-ilnotic chlannel ini the r-egionl of' the r-iglit axilla.Thlie r-iglit vertelbral arter xwas, hoxevei, neverobserv (e(1 to opiCtifv.
('out inc ittThis patient vithi bilateral atiiastoiioses had
onset of cerelblal sviptomiis alt 9 VearS (of age xx henhel showedI som01e increasein fatigability and c v-anosis )iiut xvithout evicletit polycythem-ia. The1)1l0( priessuire was lecor(lable in the left armoulIv. The angiocardiogram dlemionstiate( fillinig ofthe left sulbldavial ar-tet y ft-om the left vertebralarterx and the right x ertebral artetyx x is notopaifiel. In x iexw of these findings it is apparentthat the vertebt-Ll arterx on the left wvais the onvxfulnl-ictional vertelral arter v. Therefo e, it is cots-ceivxabile that the rniiioff from the basilair systemiito the left subclavian arteix iav haxve been highlxsigrll ifieilant.
Case 5S.13. (JHII nio. 76 93 46) is a giil xxio xxas fii-st
seen att the age of S xears in 1-956 xithl the (iag-itosis of tetralogy of Fallot. Because of intenseCx allOsis, frequenit cvaitot!c spells, and(1 pohvcx-thtemia, a left subclavian atrterv to left pilthonarai'terxy aastomosis xxit.s perifoirmed, wxhich resultediii considerable imilproveimienit. Teni miioniths folloxx-inig surgery, however, she hadl hadl Several epi-sodes of sevei-e headache generall localized tothe parietal areas, miior-e severe oni the left. Se-vecie pain in the exes aniiid vomiting occuiredl witlhthese aittacks, xvhiclh itsuiallv laste(d several hours.
Duie to the persistent natuire of this complaintan electroencephalogram ixvs pet-for-imedI 3 x earsfolloxwing snirigevx whlich xxas ititer-pr-eted as nor-inal. The phxsical fininiigs duilnillg this timie, al-though com-ipatible xxithi tetralogv of Fallot xithai ftnctioniing Blalock-Tauissig anastonmosis, liad atno timesiieggestedl a cenitral l nexVOnIS sxvstein ab-tiormanlitv. Shi1e lhadi r-eml-ainied imlildlv cvanotic.Thle blood pressii -e xas recordledI in the left arimiat 75/60 mnm. IJig aud ini the right armq- at 95/6(0into. Hg. Mlodeirate polxcxytheiiiia xxvas presenit from1960 xitholit significanit piogression.
lighit ventricular selective angiocardiogr apipin 1_962 convfirimledI the cliniical im]pr ession of tet-ialogy of Fallot. The -ight stthelavi:m arterx xxasseeni to opacifx norimall 1 2 3 secon(ls after theitjectiotn. Thlie left sibelaxvian to pulmonary arterytlmiastotn1osis xvas at this timiie reaclilv ViSuIaIlized(fig. 2A). Txxwo seconds later- the distal left sub-
ttco-thi/iids seconds aifter inijectiot. fI8e left s ibclaviactat ter y is opacified anid is secn to be continuous zcitli(lie left vcrtel)al artery (arroxvs). C, bottom. Mllagnii-fi(d vticc of tf/e /lft teitebtal-lcft *snbc/1rian artcry.omm71 1it II ic.'ut1 /) 1/,
(.i}t/g.ti oS/(j/J/C,ye XXXI. Febru7,,) t J96 5
246
by guest on July 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

SUBCLAVIAN STEAL AND BLALOCK-TAUSSIG ANASTOMOSIS
clavian artery was noted to opacify in a retrogrademanner from the left vertebral artery (fig. 2Band C).Comment
This child developed symptoms indicating acentral nervous system abnormality shortly fol-lowing a Blalock-Taussig anastomosis. Althoughher attacks have had features suggestive of mi-graine, the angiographic demonstration of reversalof blood flow from the left vertebral artery to thedistal left subclavian artery and the return of re-cordable blood pressure to the left arm favorsthe diagnosis of subclavian steal. Because of herotherwise satisfactory course to the present time,corrective surgery has not yet been performed.
DiscussionThe diagnosis of the subclavian steal rests
with the angiographic demonstration of de-layed retrograde filling of the vertebral-sub-clavian system on the side of an obstructionof the first part of the subclavian artery. Thisis due to the pressure differential between thevertebral artery and the obstructed subclavianartery, flow being in the direction of the lowerpressure. To make the diagnosis, one mustascertain that the subclavian opacification hasnot occurred from any other possible anasto-motic channel.
In none of the angiocardiograms reviewedfor the present study was a complete view ofthe neck available, as the angiocardiogramswere made for the analysis of the cardiacmalformation and not primarily for the deter-mination of the existence of a vertebral-sub-clavian communication. For this reason ourdiagnostic criteria were identification of acervical vessel in the position of the vertebralartery from which the subelavian arteryopacified and the presence of opacificationsufficiently late that direct anastomosis withan artery immediately communicating withthe aorta or carotid arteries seemed unlikely.Symptoms suggesting basilar artery insuffi-
ciency were present in seven of the 12 pa-tients comprising group 1. Most prominentamong these was severe headache, which waspresent in all these seven patients. Dizzinesswas found in three patients. Feeling of faint-ness and weakness was noted in three pa-tients. Two patients had noticed visual dis-turbances: one complained of diplopia andCirculation, Volueme XXXI, February 1965
the other of blurred vision. Although all thesecomplaints are recognized symptoms of basi-lar artery insufficiency,3' 5, 10 headache wasunusually prominent in our group. Because ofthis, hypoxia14 was considered as a cause; itis evident however from table 1 that four ofthe symptomatic patients had developed cere-bral symptoms prior to the development ofsignificant polycythemia, and, of the remain-ing three, in only one (case 7) was theregreater than a 2-year period from this initialelevation of hemoglobin and hematocrit levelsto the development of symptoms. The timeinterval between the creation of the anasto-mosis and the appearance of symptoms variedfrom 1 to 14 years. It is of interest that onlyone of the seven patients in the second group,i.e., those in which subclavian opacification oc-curred through channels other than the verte-bral artery, exhibited any of the above-de-scribed symptoms, although these patientswere comparable in age, hemoglobin andhematocrit levels, and in periods of time fromthe creation of the anastomosis.
It is apparent that a subclavian steal phe-nomenon should be considered in all patientswith Blalock-Taussig anastomosis who mani-fest symptoms of cerebral disturbance.The recent report of Massumi et al.'2 of an
asymptomatic child with angiographic evi-dence of subclavian steal is worthy of note.Although our patients form a younger groupthan those previously reported with symp-toms, it is possible that in our group the de-gree of hypoxia present, together with thesubelavian steal, contributed significantly tocerebral ischemia, which may be comparableto that caused by the cerebral vascularchanges in the older patients.Only two of the patients of the sympto-
matic group have undergone total correctionof their cardiac defects. Although the periodof observation since surgery is short, both aresymptom-free 6 months and 2 years postoper-atively. It is impossible, however, to state atpresent whether our patients who are totallycorrected will develop symptoms of basilarartery insufficiency with the degenerative vas-cular changes of advancing age.
2417
by guest on July 4, 2018http://circ.ahajournals.org/
Dow
nloaded from
FOLGER, SHAH
ConclusionTwelve patients with subelavian to pul-
monary anastomoses who have angiographicevidence of the "subclavian steal" are report-ed. In seven of these patients symptoms com-monly associated with basilar artery insuffi-ciency were present. It is our belief that thereduction of cerebral blood flow caused bythe runoff from the vertebral-basilar systemto the distal portion of the ligated subclavianartery, together with significant degrees ofhypoxemia from which these patients suf-fered is the cause of their symptoms.
AcknowledgmentThe authors are indebted to Dr. Ole Ottesen and
the Department of Radiology for performing the selec-tive angiocardiograms. The authors also wish toexpress their gratitude to Dr. Catherine A. Neill andDr. Richard D. Rowe for their assistance in the pre-paration of this manuscript.
References1. LEWIS, W. H.: Anatomy of the Human Body
by Henry Gray. Ed. 21. Philadelphia, Lea andFebiger, 1924, pp. 1417.
2. REIVICH, M., HOLLING, H. E., ROBERTs, B.,AND TOOLE, J. F.: Reversal of blood flowthrough the vertebral artery and its effecton cerebral circulation. New England J. Med.265: 878, 1961.
3. NORTH, R. R., FIELDS, WV. S., DEBAKEY, M. E.,AND CRAWFORD, E. S.: Brachial-basilar insuf-ficiency syndrome. Neurology 12: 810, 1962.
4. MANNICK, J. A., SUTER, C. C., AND HUME,D. M.: "Subclavian steal" syndrome: A fur-ther documentation. J.A.M.A. 182: 254, 1962.
5. WILLIAMS, C. L., SCOTT, S. M., AND TAKARO,T.: Subclavian steal. Circulation 28: 14, 1963.
6. PRICE, D. J.: Subclavian steal. G. P. 28: 112,1963.
7. BosNIAK, M. A.: A collateral pathway throughthe vertebral arteries associated with obstruc-tion of the innominate and proximal sub-clavian arteries. Radiology 81: 89, 1963.
8. CALLOw, A. D.: Surgical management of varyingpatterns of vertebral-artery and subclavian-artery insufficiency. New England J. Med.270: 546, 1964.
9. TOOLE, J. F.: Reversed vertebral-artery flow.Subclavian-steal syndrome. Lancet 1: 872,1964.
10. SPROUL, G.: Basilar artery insufficiency secondaryto obstruction of left subclavian artery. Circu-lation 128: 259, 1963.
11. Editorial: A new vascular syndrome-"The sub-clavian steal." New England J. Med. 265:912, 1961.
12. MAssuMI, R. A.: The congenital variety of the"subclavian steal" syndrome. Circulation 28:1149, 1963.
13. BLALOCK, A., AND TAUSsIG, H. B.: The surgicaltreatment of malformations of the heart inwhich there is pulmonary stenosis or pulmon-ary atresia. J.A.M.A. 128: 189, 1945.
14. TAUSsiG, H. B.: Congenital malformations of theheart. I. General considerations. Ed. 2, Cam-bridge, Published for the CommonwealthFund by Harvard University Press, 1960, pp204.
Principles of Medical Sciences and Animal VivisectionAnimal experiment, which we have ventured to call collateral experiment, must
always be the chief instrument for the solution of fundamental medical problems. It hasto be recognized, however, that the functional gap between man and other animals, andespecially those commonly available in laboratories, is larger even than the morpho-logical gap....
The need for such caution is, however, fundamental and general, if medicine is to getthe fullest benefit from what has been, and still is, its most fruitful resource.-The Col-lected Papers of Wilfred Trotter, F.RIS. London, Oxford Universitv Press, 1946, p. 125.
Circulation, Volume XXXI, February 1965
248
by guest on July 4, 2018http://circ.ahajournals.org/
Dow
nloaded from
GORDON M. FOLGER, JR. and KISHOR D. SHAHSubclavian Steal in Patients with Blalock-Taussig Anastomosis
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1965 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.31.2.241
1965;31:241-248Circulation.
http://circ.ahajournals.org/content/31/2/241.citationlocated on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on July 4, 2018http://circ.ahajournals.org/
Dow
nloaded from






![Kurz- und Langzeitergebnisse der arteriellen Switch ... · Auswirkungen stammt aus dem Jahr 1938 von Helen Taussig [27]. Im Jahre 1950 beschrieben Blalock und Hanlon die weltweit](https://img.dokumen.tips/doc/110x75/606109f7a1439429f115b69e/kurz-und-langzeitergebnisse-der-arteriellen-switch-auswirkungen-stammt-aus.jpg)






















