Embed Size (px)
Citation preview

Medical Teacher, Vol. 16, Nos. 2/3, 1994 189
Stop the video and involve the observers: an inter-reflective method to stimulate doctors’ learning about their own consultations with patients
S. LUNDEVALL, I. NJ0LSTAD & I. AARAAS, Institute of Community Medicine, University of Tromser, N-9037 Tromser. N o w a y
SUMMARY Consultations between a simulated patient and four general practitioners were videotaped. A method to use the material for learning and discussion in small groups has been developed. To let the observers’ own consultation style come to the fore the video is stopped at selected points and the observers are asked to write down what they would have said or done in that situation. Afterwards these written answers are read aloud as a starting point for discussion. This gives the observers the possibility of sharing their own professional way of thinking and acting in a safe atmosphere.
Introduction
Video-recording of patient-doctor consultations is a valuable and potent tool both in communication skills training and to stimulate realistic discussions about clinical problems. In Norway this has been encouraged through specialist training for general practice, but regular use of video in self-assessment still remains an activity for a minority. It takes time and effort both to organize recordings of one’s own consultations and to learn from it afterwards. A more fundamental problem may be that doctors observing video consultations sometimes take a distant and critical position towards the performance of the videotaped colleague, with a correspondingly low learning benefit for all involved. Doctors’ know-it-all-manner exposed in those settings may represent what Balint (1964) called the doctor’s “apostolic function”-described as a “vague, but almost unshakeably firm idea of how a patient ought to behave when ill. Although this idea is anything but explicit and concrete, it is immensely powerful, and influences practically every detail of the doctor’s work with his patients.” According to Balint, doctors tend to view
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 11
/17/
14Fo
r pe
rson
al u
se o
nly.
190 S. Lundevall et al.
their personal way of treating and advising patients as the very best-maybe not even recognizing that alternatives exist. When using videotapes in education we think it is important to be conscious about this tendency and to make every effort to reduce its deleterious effect on learning.
We present our experience with the development and use of an educational programme, based on a consultation experiment, where prerecorded videotaped consultations serve as a substitute for own-produced ones, and where certain procedures are used to secure the identification between the observing group and the videotaped colleague.
A consultation experiment with two aims
In a consultation experiment, videotape recordings were made of the encounters between an actress taking the role of a patient and four different general practi- tioners. According to the patient role description, the actress had two reasons for encounter: tachycardia and fear of HIV infection. She had great difficulties talking about her fear of being HIV infected and she presented her suspicions only through vague cues. The doctors knew they were meeting an actress, but the patient role description was unknown to them.
The first aim was to explore how different doctors approach an identical patient problem. All doctors spent most of the time on tachycardia, the first presented symptom. None of them paid real attention to the patient’s signal of emotional distress and did not discover her fear of being HIV-positive (Aaraas et al., 1993). The doctors tended to use the medical record in a way that hindered good patient-doctor communication (Njdstad et al. , 1992).
The second aim was to initiate learning among colleagues. Inspired by the concept of the ‘Patient-centred clinical method’ (Levenstein et al., 1986) and by the consultation analysis of Pendleton et al. (1984), we wanted to focus on patient-doctor communication at a postgraduate course for general practitioners. Using video material where different doctors talk to the same patient, our intention was to create a setting where the participants in a structured way, as peers, could share and reflect on their own approaches towards patients.
Development of involving procedures
On review immediately after the recordings none of the doctors felt very content with hisher own performance. However, three of them felt that in spite of shortcomings they could agree to show their consultations to colleagues. Two of the consultations were then shown to a group of doctors and students attending a university course in medical philosophy. The group was asked to reflect in general on what they had seen and to discuss freely afterwards. The discussion that followed opened our eyes: some of the group immediately took an aloof position and ranked the two doctors’ performances. They also started to give instructions about what the videotaped doctors should have done. Our intention of showing these rather imperfect consultations was not to get personal advice from a distant audience, but to create an atmosphere of mutual reflection and learning. We realized that the observers had to be stimulated to identify with the doctor on the screen with the help from the question: “What would I have done in this situation?”
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 11
/17/
14Fo
r pe
rson
al u
se o
nly.
Stop the video and involve the observers 19 1
Having scrutinized the video and the transcripts, we decided to focus on features common to all consultations and dilemmas familiar to all doctors, such as how to start talking with the patient and how to respond to patient utterings and demands regarding emotions (here hidden as vagueness), physical symptoms, medication, and sick leave. T o enhance the process of identification, we systematically tried to make the conditions for the observers as similar as possible to the conditions for the videotaped doctors. In the original experiment the doctors had been given a few minutes to look through a summary of the patient’s record before the consultation. We therefore decided to let the observers have the same access to the record summary, the essentials of which were:
36-year-old female bank assistant. Husband working off-shore. Many consultations for tachycardia for which she had been taking a beta- blocker for 10 years. She had also presented with a number of other benign problems over a period of many years. Thoroughly investigated during a hospital stay 3 months ago with no pathologic findings.
Our method of involving the observers further was to freeze the picture in situations where the videotaped doctor was left with a dilemma of how to respond, and then give the observers a short time to write down their spontaneous answers to simple questions like ‘What would you have done or said now?’ We selected 12 illustrative situations and formulated a question to each of them. The time allowed for answering varied from 5 to 60 seconds according to the question. A simple form on which to write down the answers was prepared.
Examples of situations and questions
Question 1. A copy of the two-page record summary was handed out to each observer before the first video consultation was shown. After 2 minutes the following question was asked:
Is there anything in this medical record that strikes you particularly? (60 seconds)
Question 2. With a still picture of the doctor receiving the patient in the office at the beginning of the consultation the following instruction was given. Imagine yourself as a doctor in this consultation which is to be finished within 10 minutes. You have seen the record but you have no previous knowledge of the patient. Imagine this situation: the patient has entered your office and you have greeted her.
What is your opening remark? That is: how would you start this consultation? (30 seconds)
Question 4. At the beginning of the first consultation, when the patient has presented her palpitations and some vague additional cues, she asks very hesitat- ingly “What I was wondering about ... may be to have an examination ... which in a way covered everything ... ?”
Question 8. In the second consultation the patient and the doctor discuss exami- nations already carried out to clarify her episodes of palpitations over many years and the doctor says: “I can reassure you that the examinations which have been done are thorough.’’
What is your answer to this? (45 seconds)
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 11
/17/
14Fo
r pe
rson
al u
se o
nly.
192 S. Lundevall et al.
Do you think her heart problem has been sufficiently clarified? If not, which additional examinations would you suggest now? (45 seconds)
Would you prescribe Valium to the patient? (5 seconds)
Would you give the patient sick-leave? (5 seconds)
What do you think is the patient’s main reason for the encounter? (45 seconds)
Question 10. The patient asks for some Valium.
Question 11. The patient asks whether she should continue to work.
Question 12. After having seen the consultations with all three doctors:
Experiences with the method
The 45 minute-video was shown to 40 experienced general practitioners at a postgraduate training course, followed by 2 hours of discussions in small groups. The doctors had no problems in engaging themselves in the video. In fact, every doctor answered every question. In the small groups we instructed the participants to choose one of the questions at a time and read their answers aloud as a starting point for reflection. T o illustrate, we quote a few of the answers to question 4 above, where the patient asks for an examination that “covers everything.”
Dr A: We don’t have an examination that covers everything. Dr B: You have already been to a cardiologist who did not find anything
wrong. The risk that there is anything wrong with your body is small. Dr C: We can examine your heart to see if the reason lies there. Dr D: What are you afraid of? Dr E: Everything?
The diversity of answers lead to lively and open minded discussions where the participants shared their own questions and uncertainty with each other. Through this method the focus changed from the videotaped doctors’ performance to the group members’ own.
Reading the answers aloud in the small group of peers has proved to be an important part of the training format. Not only does it give the small group work a clear structure, but when some participants tend to declare more generally what should have been said or done in a similar situation, the repeated instruction: “Please read what you have written on the form” serves as a reminder that the participants are committed by their own answers, and in that sense have already said or done something.
We have used this arrangement with slight modifications at many seminars and courses for doctors with varying degrees of experience, ranging from 3rd year medical students to specialists in several fields of medicine. We have listened to many and tape-recorded some of the group discussions, collected answer forms, and received written and oral general evaluating comments from participants. This evaluation material has been used to shape the programme into its present form. Evaluating remarks are generally very positive, such as: “The video managed to actively involve us, not only in discussing the colleague on the video.. . . It promotes reflection and self-examination . . . It is good that there is no predetermined answer ... We lose some of our fear of making fools of ourselves.”
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 11
/17/
14Fo
r pe
rson
al u
se o
nly.
Stop the video and involve the observers 193
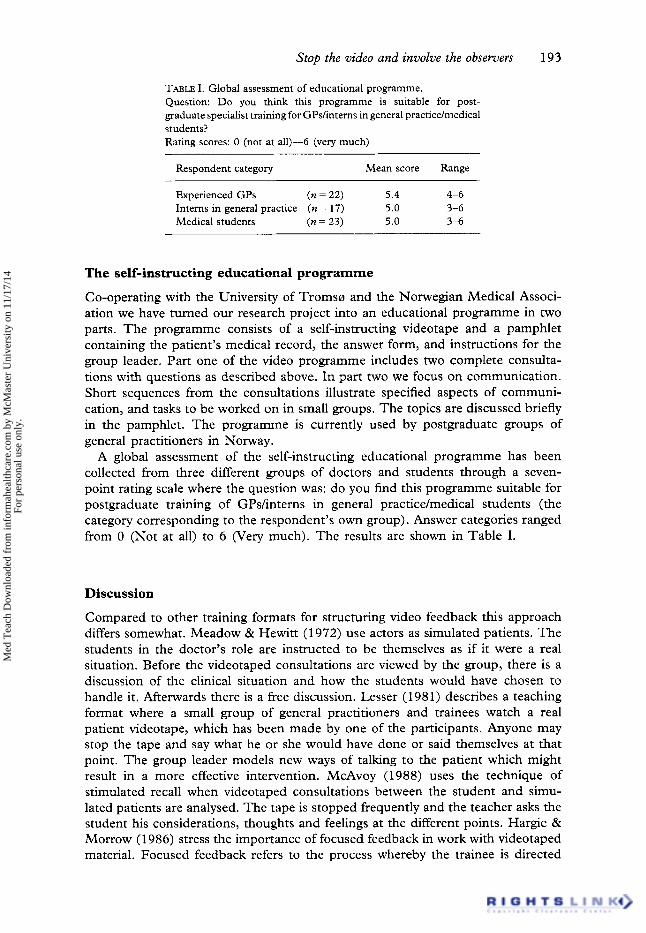
TABLE I. Global assessment of educational programme. Question: Do you think this programme is suitable for post- graduate specialist training for GPdinterns in general practicdmedical students? Rating scores: 0 (not at all)-6 (very much)
Respondent category Mean score Range
Experienced GPs (n = 22) 5.4 4-6 Interns in general practice (n = 17) 5.0 3-6 Medical students (n = 23) 5.0 3-6
The self-instructing educational programme
Co-operating with the University of Tromsa and the Norwegian Medical Associ- ation we have turned our research project into an educational programme in two parts. The programme consists of a self-instructing videotape and a pamphlet containing the patient’s medical record, the answer form, and instructions for the group leader. Part one of the video programme includes two complete consulta- tions with questions as described above. In part two we focus on communication. Short sequences from the consultations illustrate specified aspects of communi- cation, and tasks to be worked on in small groups. The topics are discussed briefly in the pamphlet. The programme is currently used by postgraduate groups of general practitioners in Norway.
A global assessment of the self-instructing educational programme has been collected from three different groups of doctors and students through a seven- point rating scale where the question was: do you find this programme suitable for postgraduate training of GPshnterns in general practice/medical students (the category corresponding to the respondent’s own group). Answer categories ranged from 0 (Not at all) to 6 (Very much). The results are shown in Table I.
Discussion
Compared to other training formats for structuring video feedback this approach differs somewhat. Meadow & Hewitt (1 972) use actors as simulated patients. The students in the doctor’s role are instructed to be themselves as if it were a real situation. Before the videotaped consultations are viewed by the group, there is a discussion of the clinical situation and how the students would have chosen to handle it. Afterwards there is a free discussion. Lesser (1981) describes a teaching format where a small group of general practitioners and trainees watch a real patient videotape, which has been made by one of the participants. Anyone may stop the tape and say what he or she would have done or said themselves at that point. The group leader models new ways of talking to the patient which might result in a more effective intervention. McAvoy (1988) uses the technique of stimulated recall when videotaped consultations between the student and simu- lated patients are analysed. The tape is stopped frequently and the teacher asks the student his considerations, thoughts and feelings at the different points. Hargie & Morrow (1 986) stress the importance of focused feedback in work with videotaped material. Focused feedback refers to the process whereby the trainee is directed
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 11
/17/
14Fo
r pe
rson
al u
se o
nly.
194 S. Lundevall et al.
towards specific aspects of the video playback, rather than trying to concentrate on the total performance.
In contrast, our inter-reflective way of using video implies two distinctive ele- ments:
(1) it secures identification between the videotaped doctor and the group mem- bers, as described; and
(2) the method insures reflection in a group where all participants get the opportunity of becoming involved at the same emotional level. The partici- pants observe the consultations simultaneously and involve themselves in the same way through the written answers. This is a simple way to attain affective learning, which in addition to the cognitive learning process is necessary to get new knowledge ‘under your skin’. Perhaps one of the most consistent features of the small group discussions is that the participants realize not only cogni- tively, but also emotionally, that there is not only one ‘truth’. The participants observe the same consultations, yet it is demonstrated for them that they interpret their observations and act in different ways.
One strength of this method is its simplicity and acceptability. The learning goals do not need to be restricted to communication skills. Clinical performance and practical judgements about diagnoses, examinations and treatments can be focused as well. Any suitable videotape of a doctor-patient consultation can be used in a similar way for structured discussions where the observers are turned into involved participants. As no video recording or other preparation from the partic- ipants is necessary, and there is no threatening assessment process, one can hopefully overcome some of the problems of self-selection bias to courses in communication skills. (St Claire, 1992)
There will often be a gap between what one thinks one should do and what one actually does. T o what extent do the participants’ spontaneously written answers in our approach represent what they actually do? Both the ‘temperature’ of the discussions and the reluctance many participants regularly show towards reading their answers aloud indicate that this approach brings about a personal commit- ment, the same as would be expected if the small group discussion were based on what the participants actually had done or said. Hearing what a group of col- leagues didsaid in the same situations creates an opportunity for the participating doctors to have their own ‘apostolic functions’ revealed. Our repeated observations of colleagues, deeply engaged in discussions that exceed all pre-set time limits, have strengthened our impression that this way to involve the observers really works.
Correspondence: Sverre Lundevall, Spingbergveien 30B, 0853 Oslo, Norway.
REFERENCES AARAAS, I., LUNDEVAIL, S., NJ0LSTAD, I. & MELBYE, H. (1993) Stuck with the patient: what would my
colleague have done? A video recorded consultation experiment with an actor simulating as the same patient for different doctors, Family Practice, 10, pp. 4 3 4 5 .
BALINT, M. (1964) The Doctor, His Patient and the Illness (London, Pitman). BYRNE, P.S. & LONG, B.E.L. (1976) Doczors Talking to Patients (London, HMSO).
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 11
/17/
14Fo
r pe
rson
al u
se o
nly.

Stop the video and involve the observers 195
HARGIE, O.D. & MORROW, N.C. (1986) Using videotape in communication skills training: a critical evaluation of the process of self-viewing, Medical Teacher, 8, pp. 359-365.
LESSER, A.L. (1981) The psychiatrist and family medicine: a different training approach, Medical Education, 15, pp. 398-406.
LEVENSTEIN, J.H., MCCRACKEN, E.C., MCWHINNEY, I.R. ET AL. (1 986) The patient-centered clinical method: 1. A model for the doctor-patient interaction in family medicine, Family Ractice, 3,
McAvou, B.R. (1988) Teaching clinical skills to medical students: the use of simulated patients and videotaping in general practice, Medical Education, 22, pp. 193-1 99.
MEADOW, R. & HEWITT, C. (1972) Teaching communication skills with the help of actresses and videotape simulation, British Journal of Medical Education, 6, pp. 317-322.
NJ~LSAD, I., AARAAS, I. & LUNDEVW, S. (1992) Look at the patient, not the notes, Lancet, 340, pp. 413414.
PENDLETON, D., SCHOEFIELD, T., TATE, P. & HAVELOCK, P. (1984) The Consultation: an approach to learning and teaching (Oxford, Oxford University Press).
ST CWRE, L. (1992) Evaluating a workshop designed to help medical students improve their skills in communicating about cancer: methodological considerations-and worries, Medical Teacher, 14,
pp. 24-30.
pp. 65-76.
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 11
/17/
14Fo
r pe
rson
al u
se o
nly.