CALIFORNIA STATE JOURNAL OF MEDICINE VOL. XV, No. 3
STENOSIS OF THE DUODENUM.By P. S. CAMPICHE,
M. D., F. A. C. S., M. R. C. S. (Eng.), San Francisco.Case I. In
September, 1913, Mrs. E. L., 34
years old, was referred to me by Dr. Emil Schmoll.In childhood
and as a girl she had always been
in good health. At the age of 24 she sufferedfrom dysmenorrhea
and was operated on (ventro-fixation and appendectomy). Soon after
she be-gan to have frequent attacks of vomiting; in fact,for the
last ten years she had been vomiting everyday, more or less. In
19I2 she married and hada normal confinement in July of the
followingyear. While pregnant she felt much better, butsince the
birth of her child her stomach becameworse than usual; during the
three months priorto my seeing her she had managed to keep
herbreakfast down but regularly vomited her lunchand her supper
every day, together with a greatquantity of bile. In these attacks
the food cameup first, then a gush of bile followed. She hadno
appetite and was very constipated but did notcomplain of pain. The
abdomen was never dis-tended, but was, in fact, rather retracted;
theurine was normal. Her weight was 89 pounds.
After keeping her under observation for a weekDr. Schmoll made a
diagnosis of stenosis of theintestine, probably due to adhesions,
and advisedoperation for the relief of the continuous vomiting.
I operated on October 6, 19I3, making a medianlaparotomy
incision. Exploration of the pelvisorgans revealed nothing
abnormal, although theuterus was well attached to the anterior
abdom-inal wall as a result of the previous ventro-fixation. The
colon and sigmoid flexure appearedto be much under normal in size,
but the smallintestine presented the most striking picture. Itwas
quite empty and so much contracted that itscalibre was that of an
ordinary lead pencil insome places.
This suggested an obstruction at some higherlevel and the small
intestine was followed up; thejejunum below the musculus
suspensorius duodeni(Treitz' ligament) was somewhat wider
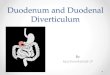
thoughstill below normal in size, while the stomach andduodenum
were found to be greatly dilated andmarkedly hypertrophied. The
caliber of the duo-denum, in fact, was three times greater than
nor-mal and its wall was thick and hypertrophied andin the third
portion, or pars inferior, especiallywas embedded in shining white
adhesions. I havetried to picture its condition in the
accompanyingsketch.
In spite of very thorough palpation no recentulcer of the
duodenum or near the pylorus couldbe detected; the gall-bladder,
apart from a fewadhesions, was normal and contained no stones.I
concluded that there had been an ulcer theresome years previously
which had healed and that,as a consequence, all these adhesions
remained.Our diagnosis, based on the result of this
longexploration, was stenosis of the duodeno-jejunalflexure due to
peritoneal adhesions with secondarydilation and hypertrophy of the
duodenum andthe stomach.
Owing to the absence of a good serosa on theduodenum a direct
anastamosis between the jeju-num and the duodenum would have been
mostunsafe. Gastro-jejunostomy done in such instancesof stenosis
below the papilla duodeni has the in-convenience that bile flows
back into the stomach,
..e. '... ;:.|
from which it escapes through the anastamosis.This could be
prevented by closure of the pylorusif the duodeno-jejunal stenosis
was incomplete, butin the case before me the stenosed part hardly
ad-mitted the tip of the finger and for fear that astill greater
contraction might develop later atthis point, I did not think it
advisable to closethe pylorus. On the other hand, gall-stone
opera-tions have shown in many cases of cholecysto-gas-trostomy
that the patient becomes accustomed tothe continuous presence of
bile in the stomachand does not suffer much discomfort or nausea.I
therefore did a typical posterior no-loop gastro-jejunostomy with a
very wide anastamosis; whenthe operation was completed I convinced
myselfthat the new stoma readily admitted three fingers.
For the first week after operation the patientwas kept on
liquids and did fairly well; on thesixth day, after eating some
toast and scrambledegg, she vomited bile in large quantities so
thatthe liquid diet was continued a little longer untilabout the
fourteenth day she was eating a regularsemi-solid diet. Her weight
was 82 pounds.,
I saw 'her lately, nearly three years after opera-tion; her
weight is now io8 pounds. She consid-ers her condition greatly
improved as evidencedby the fact that she can now eat three
squaremeals a day and does not vomit more than once
76
CALIFORNIA STATE JOURNAL OF MEDICINE
at night and only bile, which, considering herprevious state of
constant nausea, is indeed a vastchange for the better.
I have been disappointed, however, because ofher not gaining
more in weight since the opera-tion, although this may be
attributed to the con-tinuous presence of bile and pancreatic juice
inthe stomach which probably interferes to someextent with gastric
digestion; but she is satisfiedto be able to keep her food down and
to find thatshe is much stronger and much more active thanshe was
before the operation.
Case II. Mr. R. McH., 38 years old, wasreferred to me by Dr. M.
Etcheverry in Septem-ber, 19I 1.The man had been ailing for several
years and
had been treated for gastric ulcer and afterwardsfor
gall-stones; he was sent to me with a diag-nosis of gall-stones. In
spite of a fairly goodappetite he was thin and anaemic and
complainedof severe pain in the epigastrium occurring abouttwo
hours after meals, accompanied with a sen-sation of hunger; the
pain would occasionally ex-tend toward the shoulders and was
relieved byfood. Although he always felt distressed andwas often
nauseated he never vomited.When operated on in October, I9II, I
found
that the gall-bladder and the liver were slightlyadherent to the
duodenum, but normal otherwise;the serosa showed no alteration. At
the secondportion of the duodenum above the papilla duodenithere
was a hard growth, three by three centi-meters in size, somewhat
irregular and seeminglymore prominent on the anterior wall; a
narrowchannel could be felt through the tumor whichexplained the
absence of more serious symptoms,the obstruction being incomplete.
My diagnosisat the time of operation was duodenal ulcer,though
later I had to change it; I did a posteriorgastro-jejunostomy.The
patient improved very much at first; his
pains left him and in three months he gained 15pounds in weight.
However, when I again sawhim in May, I912, he had a large, hard,
irregulartumor in the liver and under the right costalmargin,
evidently a cancerous metastasis. Thisshowed conclusively that the
primary growth wasnot an ulcer but a carcinoma of the duodenum.Two
months later, in July, 1912, he died.
Stenosis of the duodenum may be congenital oracquired. A
congenital form described by Terryand Kilgore 1 was, in reality, a
malformation ofthe duodenum. As a consequence of faulty
de-,velopment at the junction of the embryonic fore-gut and midgut
the second part of the duodenumhad a very narrow canal; the general
nutrition ofthe patient had suffered very much and the
caseterminated fatally after a gastro-jejunostomy.
In the cases described by Harris 2 the troublewas also
congenital and consisted in abnormalfolds which caused constriction
of an otherwisewell-developed duodenum. Harris called thesefolds
abnormal remains of a perfectly normal em-bryologic structure. The
symptoms were mild, re-sembling those of duodenal ulcer and with
verylittle or no vomiting. In all his six cases divi-sion of the
abnormal bands was sufficient to effecta cure.A third form of
congenital constriction results
from the so-called pancreas annulare, where thehead of the
pancreas completely encircles theduodenum and compresses it.The
duodenal stenosis in the acquired form may
be due to several different causes, all of whichare fully
enumerated in Anders' 3 paper, who hascollected reports of 262
cases, and gives a sum-marv of eighty of them. In his opinion the
fac-tors most frequently responsible for stenosis areas follows,
and though these conditions are some-what rare, each of us has
probably seen them all,at least once:
1. Carcinoma of the head of the pancreas andchronic
pancreatitis, which are known to havebeen the cause of stenosis of
the pars descendensof the duodenum, although they more
ordinarilyproduce symptoms of papillary stenosis, such aschronic
and progressive jaundice, with acholicstools and marked enlargement
of the liver andgall-bladder. Such cases are common and all ofus
have seen them, no doubt.
2. Carcinoma of the duodenum, frequently men-tioned by older
authors, although it is now con-sidered a great rarity. The second
case reportedabove is a typical example of this condition, aswas
proved in the operation and by the subse-quent course of the
disease, although the clinicalsymptoms were not truly typical,
being obscuredby the fact that vomiting was absent owing tothe
incompleteness of the obstruction.
3. Duodenal ulcer is a condition which oftencauses narrowing of
the duodenum, as is attestedby Moynihan,4 who had 43 such cases in
his ownexperience; it is usually a cicatricial stenosis, butin some
instances, as was also reported by theMayos,5 an hour-glass-
duodenum was found. Moy-nihan further observed that stenosis may
occurafter the suturing of a perforation of the duo-denum.
4. Peritoneal adhesions, sometimes of unknownorigin, may cause
stenosis, which is well illus-trated by the first case-above
reported. The ulcer,originally the cause of the trouble, has
probablyhealed spontaneously or cannot be found, but ithas left
behind a trail of dense adhesions tocompress the duodenum and pave
the way forfuture complications.
5. Compression of the duodenum by gall-stonesor by an inflamed
gall-bladder is not such a veryrare condition, and here the
adhesions may also
MARCH, 19I7 77
78 CALIFORNIA STATE JOURNAL OF MEDICINE VOL. XV, No. 3
be so dense that sometimes a gastro-jejunostomybecomes
necessary.
In November, 1912, I recall, Drs. D. Voor-sanger and Charles G.
Levison's reported to thissociety a case of duodenal stenosis due
to com-pression by a long adherent gall-bladder, andwhich was cured
by cholecystectomy.
6. Compression by the root of the mesenteryis given by Anders as
a cause of stenosis and ithas been the subject of so many reports
publishedin recent years that I do not need to insist uponit
here.The symptoms of duodenal stenosis have been
clearly stated already by Wilms,7 Kausch,8 andothers. If the
construction lies above the papilla(suprapapillary stenosis), as it
was in my case otcancer of the second portion of the duodenum,the
clinical signs will be the same as those ofpyloric stenosis, such
as vomiting of food withlittle or no bile, provided that the
obstructionis complete.
If the compression is in the region of thepapilla, especially if
we have a papillary stenosis,the deep chronic jaundice with acholic
stools andthe enlargement of the liver, all give a verydefinite
picture.
In cases of infrapapillary stenosis like the firstcase reported
above, we will have two constantsymptoms, which are:
1st. Abundant and oft-repeated vomiting of foodand bile, which,
however, never becomes fecal incharacter; and,
2nd. Absence of distention, and often retractionof the abdomen,
even, which is attended with con-stipation, while the patient is
often emaciated andin a state of complete exhaustion.
In pumping out the stomach in such cases, orwhen the patient
vomits, colorless mucus or food1emnants are seen first, followed by
a gush of bileat the end of the procedure.Treatment varies both
according to the cause
of the condition and as to the site of the stenosis.In cases
where bands, congenital or otherwise,exist, and are the cause of
the constriction, divisionwill be necessary, and this will often be
sufficientas is shown in the cases reported by Harris.
In stenosis due to diseases of the gall-bladdercholecystectomy
is indicated as the best meansof removing the compression and
preventing, or atleast minimizing, the formation of new
adhesions.
If, in conditions of papillary stenosis, the duo-denum itself
has remained fairly patent, as oftenoccurs in some cases of
carcinoma of the head otthe pancreas or in chronic pancreatitis,
cholecysto-gastrostomy may give the patient great relief.When the
narrowing of the lumen is due to any
disease of the wall of the duodenum proper, suchas cancer,
ulceration, cicatrices, or to dense anddiffuse adhesions,
gastro-j1ejunostomy is indicated;but while this operation has given
complete satis-faction in suprapapillary stenosis, which
closelyresembles pyloric stenosis, it is by no means idealin cases
of infrapapillary stenosis, for the bile ancpancreatic juice will
constantly flow backward fromthe duodenum into the stomach and
certainly inter-fere to some extent with gastric digestion, so
thatthe patient is unable to gain very much in weightor even attain
first class health, as may be judgedfrom the first case here
reported. Yet this pro-cedure may be the only available one that
will besafe in such a condition.
Discussion.Dr. C. G. Levison: This paper is of interest
on account of the infrequency of stenosis of theduodenum in the
infrapapillary region. As Dr.Campiche has stated, Anders has
collected severalhundred cases and if I recall them correctly,
mos;of them have been suprapapillary conditions.There have been
comparatively few infrapapillarystenoses reported, and when one
considers the
frequency of pathological processes in the upperquadrant, it is
extraordinary that so few cases ofthis kind have come to our
notice.In the condition reported by Voorsanger and
myself that Dr. Campiche was kind enough tomention, the patient
vomited large quantities ofbile incessantly. There was no bile
entering theintestinal tract, so that the diagnosis was
compara-tively easy to make. At the operation an enlon-gated,
indurated gall-bladder was found lying acrossthe descending part of
the duodenum, producingcomplete obstruction. It is interesting when
oneconsiders the adhesions, ulcerations, old gall-bladderconditions
and carcinomata that are so frequentlypresent in this region, that
this type of obstruc-tion occurs so seldom.
Literature.1. Terry, W., and Kilgore, A.: Congenital Stenosis
of
the Duodenum in an Adult. The Journal A. M. A.,June 3, 1916, p.
1774.
2. Harris, M. L.: Constriction of the Duodenum dueto Abnormal
Folds of the Anterior Mesogastrium.The Journal A. M. A., April 18,
1914, p. 1211.
3. Anders, J.: Report of a New Case of Stenosis ofthe Duodenum.
Am. Jour. Med. Sc., 1912, p. 360.
4. Moynihan, B. G. A.: Duodenal Ulcer, 1910. W. B.Saunders Co.,
Phila.
5. Eusterman, G. B.: Hour-glass Stomach and Duode-num. Collected
Papers of the Mayo Clinic, 1914,p. 20.
6. Voorsanger, D., and Levison, C. G.: Stenosis of theDuodenum
due to Compression of the Gall-bladder.
Calif. State Med. Journ., Nov., 1912.7. Wilms, M.: Stenosis des
Unteren Duodenuins, Bruns'
Beitrage, 1897, p. 511.8. Kausch, W.: Handbuch der Praktischen
Chirurgie,
1913, vol. 3, p. 297.
ABSTRACT OF MINUTES OF THE EIGHTY-NINTH MEETING OF THE COUNCIL
OFTHE MEDICAL SOCIETY OF THE STATEOF CALIFORNIA, UNION LEAGUE
CLUB,SAN FRANCISCO.
February 3, 1917.The meeting was called to order by the
chair-
man, C. G. Kenyon, at 12:15 p. m.Present: Chairman C. G. Kenyon,
Drs. Jayet,
Ryfkogel, Bine, Ewer, Edwards, Hoisholt, Parkin-son and later
Hamlin. Dr. H. M. Sherman andMr. Hartley F. Peart, attorney for the
Society,were also present.Parkinson acting as secretary, the
minutes of
the eighty-eighth meeting were read and approved.Auditing
Committee.
Ryfkogel for the Auditing Committee reportedthat in accordance
with instructions of the Coun-cil, he had employed the firm of
McLaren, Goode& Co., certified accountants, to install a
systemof bookkeeping. This had been started and abookkeeper
employed.He then submitted a detailed statement of the
financial condition of the Society. The followingabstract shows
the position of the Society at theend of the years 1915 and 1916,
respectively:
COMPARATIVE BALANCE SHEET.Dec. 31, 1915 Dec. 31, 1916
Assets:Cash .$ 995.29 $1179.46Accounts receivable 960.86
945.09Paper on hand... 512.80 1943.80Furniture and fixtures..
897.60 1300.50
$3366.55 $5368.85Liabilities:Loan Union Trust Co..
1500.00Medical Defense........ 2483.55 721.25Sundry accounts
payable 1189.94 641.11Medical Indemnity Fund 4979.00
$5173.49 $6341.36Deficiency: End of 1915, $1806.94; 1916,
$972.51
Bine also for the Auditing Committee said thatat present no
definite statement of expense was