Embed Size (px)
Citation preview
The Spine Journal 9 (2009) e17–e19
Spontaneous spinal cord herniation: recurrence after 10 years
Panagiotis Selviaridis, MD, PhD, Ioannis Balogiannis, MD, PhD, Nicolas Foroglou, MD, PhD*,Athanasios Hatzisotiriou, MD, PhD, Ioannis Patsalas, MD, PhD
Department of Neurosurgery, AHEPA University Hospital, 1, Stilponos Kyriakidi str, 54636 Thessaloniki, Greece
Received 9 December 2007; accepted 22 March 2008
Abstract BACKGROUND CONTEXT: Transdural spo
FDA approval sta
plicable devices/drugs
The authors do no
perceived as creating,
* Corresponding a
sity Hospital, 1, Stilpo
(30) 2310235472; fax
E-mail address: n
1529-9430/09/$ – see
doi:10.1016/j.spinee.2
ntaneous spinal cord herniation is a very rare noso-logical entity, which despite recent reports in the medical literature remains often misdiagnosed pre-operatively. Usually it affects the thoracic segment, protrudes ventrally, presents clinically asa progressive Brown-Sequard syndrome and carries a favorable surgical outcome.PURPOSE: To describe a rare case of delayed recurrence of spontaneous spinal cord herniationdespite excellent outcome for 10 years, and discussion of management and observation issues.STUDY DESIGN/SETTING: Case report/University Hospital.METHODS: We describe the management of a patient with spontaneous spinal cord herniationthat presented initially with a Brown-Sequard syndrome and has been treated successfully with sur-gery. After 10 years free of symptoms, the patient developed progressive paraparesis and urinaryincontinence because of recurrence of the herniation at the same level.RESULTS: Despite technical challenges, during the second operation the enlarged ventral duraldefect was meticulously closed and the patient’s neurological condition presents 9-month postsur-gery considerable improvement. To our best knowledge, recurrences of spontaneous spinal cordherniation are extremely rare.CONCLUSIONS: The reported case underlines the necessity to be aware of this rare but treatablespinal disease, notify the possibility of late recurrences and the need of long-term follow-up even ifinitial outcome is favorable. � 2009 Elsevier Inc. All rights reserved.
Keywords: Brown-Sequard syndrome; Spontaneous spinal cord herniation; Ventral dural defect; Delayed recurrence
Introduction
Transdural Spontaneous Spinal Cord Herniation (SSCH)is a rare and frequently misdiagnosed condition that pres-ents with various spinal cord syndromes. The treatable na-ture of the disease force us to focus attention on SSCH asa rare cause of Brown-Sequard syndrome that usually hasa favorable outcome. We report a case of SSCH treated atour institution that has fully recovered after the first opera-tion and relapsed 10 years after initial treatment.
tus: This article does not discuss or include any ap-
.
t have a financial relationship that creates, or may be
a conflict related to this article.
uthor. Department of Neurosurgery, AHEPA Univer-
nos Kyriakidi str, 54636 Thessaloniki, Greece. Tel.:
: (30) 2310994708.
[email protected] (N. Foroglou)
front matter � 2009 Elsevier Inc. All rights reserved.
008.03.013
Case report
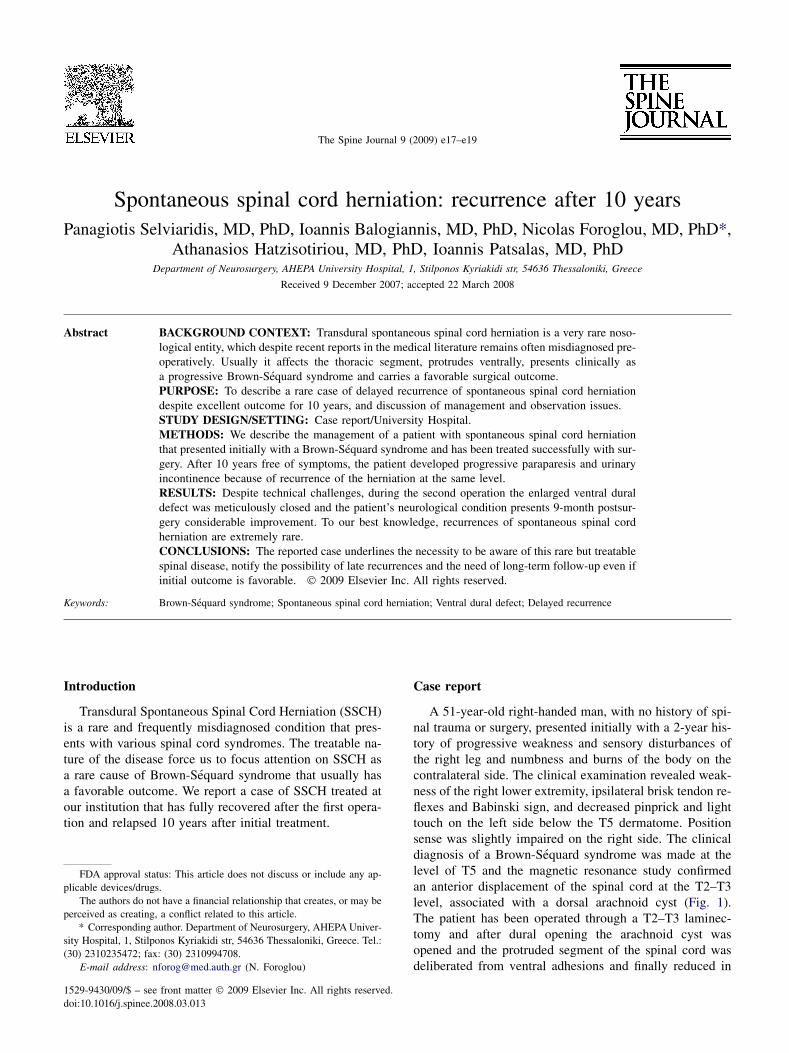
A 51-year-old right-handed man, with no history of spi-nal trauma or surgery, presented initially with a 2-year his-tory of progressive weakness and sensory disturbances ofthe right leg and numbness and burns of the body on thecontralateral side. The clinical examination revealed weak-ness of the right lower extremity, ipsilateral brisk tendon re-flexes and Babinski sign, and decreased pinprick and lighttouch on the left side below the T5 dermatome. Positionsense was slightly impaired on the right side. The clinicaldiagnosis of a Brown-Sequard syndrome was made at thelevel of T5 and the magnetic resonance study confirmedan anterior displacement of the spinal cord at the T2–T3level, associated with a dorsal arachnoid cyst (Fig. 1).The patient has been operated through a T2–T3 laminec-tomy and after dural opening the arachnoid cyst wasopened and the protruded segment of the spinal cord wasdeliberated from ventral adhesions and finally reduced in
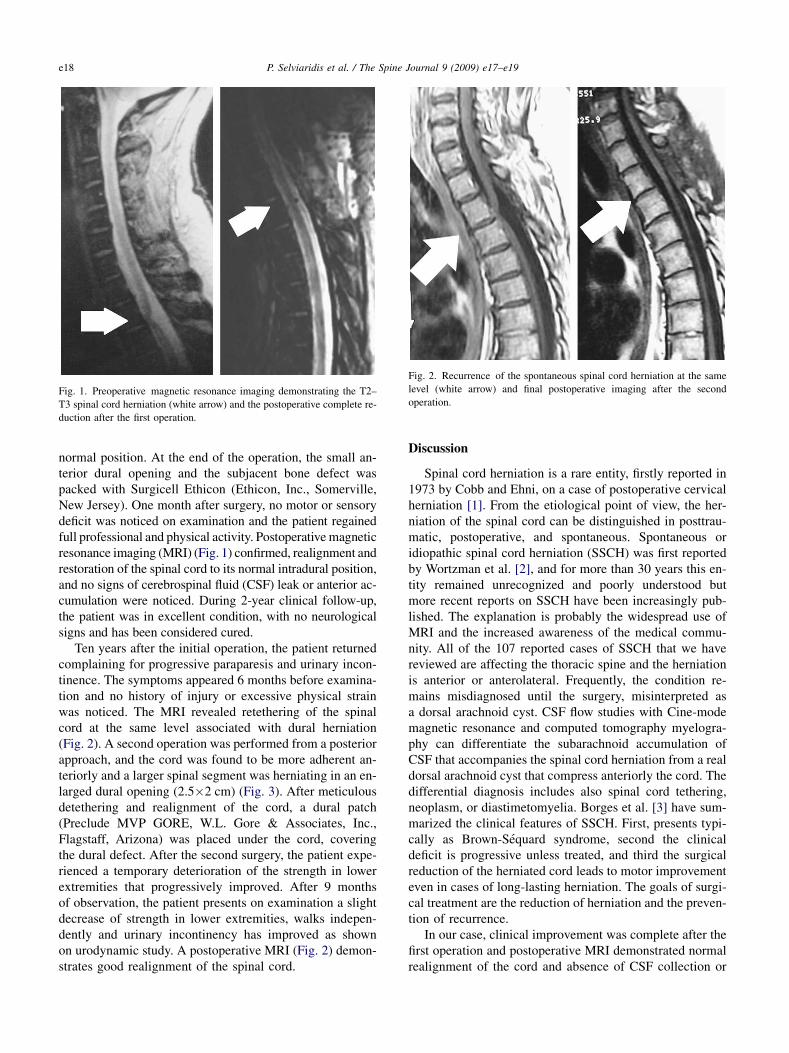
Fig. 1. Preoperative magnetic resonance imaging demonstrating the T2–
T3 spinal cord herniation (white arrow) and the postoperative complete re-
duction after the first operation.
Fig. 2. Recurrence of the spontaneous spinal cord herniation at the same
level (white arrow) and final postoperative imaging after the second
operation.
e18 P. Selviaridis et al. / The Spine Journal 9 (2009) e17–e19
normal position. At the end of the operation, the small an-terior dural opening and the subjacent bone defect waspacked with Surgicell Ethicon (Ethicon, Inc., Somerville,New Jersey). One month after surgery, no motor or sensorydeficit was noticed on examination and the patient regainedfull professional and physical activity. Postoperative magneticresonance imaging (MRI) (Fig. 1) confirmed, realignment andrestoration of the spinal cord to its normal intradural position,and no signs of cerebrospinal fluid (CSF) leak or anterior ac-cumulation were noticed. During 2-year clinical follow-up,the patient was in excellent condition, with no neurologicalsigns and has been considered cured.
Ten years after the initial operation, the patient returnedcomplaining for progressive paraparesis and urinary incon-tinence. The symptoms appeared 6 months before examina-tion and no history of injury or excessive physical strainwas noticed. The MRI revealed retethering of the spinalcord at the same level associated with dural herniation(Fig. 2). A second operation was performed from a posteriorapproach, and the cord was found to be more adherent an-teriorly and a larger spinal segment was herniating in an en-larged dural opening (2.5�2 cm) (Fig. 3). After meticulousdetethering and realignment of the cord, a dural patch(Preclude MVP GORE, W.L. Gore & Associates, Inc.,Flagstaff, Arizona) was placed under the cord, coveringthe dural defect. After the second surgery, the patient expe-rienced a temporary deterioration of the strength in lowerextremities that progressively improved. After 9 monthsof observation, the patient presents on examination a slightdecrease of strength in lower extremities, walks indepen-dently and urinary incontinency has improved as shownon urodynamic study. A postoperative MRI (Fig. 2) demon-strates good realignment of the spinal cord.
Discussion
Spinal cord herniation is a rare entity, firstly reported in1973 by Cobb and Ehni, on a case of postoperative cervicalherniation [1]. From the etiological point of view, the her-niation of the spinal cord can be distinguished in posttrau-matic, postoperative, and spontaneous. Spontaneous oridiopathic spinal cord herniation (SSCH) was first reportedby Wortzman et al. [2], and for more than 30 years this en-tity remained unrecognized and poorly understood butmore recent reports on SSCH have been increasingly pub-lished. The explanation is probably the widespread use ofMRI and the increased awareness of the medical commu-nity. All of the 107 reported cases of SSCH that we havereviewed are affecting the thoracic spine and the herniationis anterior or anterolateral. Frequently, the condition re-mains misdiagnosed until the surgery, misinterpreted asa dorsal arachnoid cyst. CSF flow studies with Cine-modemagnetic resonance and computed tomography myelogra-phy can differentiate the subarachnoid accumulation ofCSF that accompanies the spinal cord herniation from a realdorsal arachnoid cyst that compress anteriorly the cord. Thedifferential diagnosis includes also spinal cord tethering,neoplasm, or diastimetomyelia. Borges et al. [3] have sum-marized the clinical features of SSCH. First, presents typi-cally as Brown-Sequard syndrome, second the clinicaldeficit is progressive unless treated, and third the surgicalreduction of the herniated cord leads to motor improvementeven in cases of long-lasting herniation. The goals of surgi-cal treatment are the reduction of herniation and the preven-tion of recurrence.
In our case, clinical improvement was complete after thefirst operation and postoperative MRI demonstrated normalrealignment of the cord and absence of CSF collection or

Fig. 3. Intraoperative photograph during the second operation demon-
strating the spinal cord (asterisk), the enlarged ventral dural opening (large
arrow), and the dural patch (small arrow).
e19P. Selviaridis et al. / The Spine Journal 9 (2009) e17–e19
leak (Fig. 1). We decided to interrupt follow-up after 2years of excellent clinical condition. The delayed recur-rence, underlines the necessity for long-term follow-upeven if there is excellent outcome after surgery.
From reviewing 107 cases of SSCH syndrome in the lit-erature, we founded only four cases of recurrence, appear-ing 18 months to 3 years [4–7] after initial treatment. In thereported case, the delayed onset of the recurrence, 10 yearslater, was as the first time, progressive and not associatedwith any injury or unusual physical activity. In Ammaret al. [4], the dural defect was not closed and recurrenceoccurred 18 months after treatment. In the second opera-tion, detethering of the spinal cord followed by duroplastywith patch leaded in a short-term clinical improvement.Batzdorf [5] reported the case of a young woman withSSCH syndrome who has been operated successfully butrelapsed 3 years later. In that case, dural graft did not pre-vent recurrence. Nakagawa et al. [6] reported a case wherethe spinal cord was adhered and herniated in a bone defect.Although the bone defect was filled with fat tissue and thedural opening was closed with dural patch, recurrenceoccurred 3 months after the initial operation. In Waters
et al. [7], after reduction of the spinal cord the ventral sur-face was not explored and the dural defect was not repairedat the first operation.
In most reported cases, as in the present case, the mostprobable reason of recurrence is the inadequate closure ofthe dural defect. In the reported case, during the first oper-ation after detethering of the cord, the small opening of thedura and subjacent bone defect were filled only with smallpieces of Surgicell Ethicon, considering that it was suffi-cient for obliteration. Despite excellent radiological andclinical initial outcome, an explanation for the delayed re-currence can be the chronic spinal cord movement. Thecord is mobile and pulsates through cardiac and respiratorycycles in an anteroposterior direction and this movement ismaximal in areas where more severe pathology exists. Thisfacilitates the spinal cord to lie ventrally against the duraldefect and the development of adhesions with the edgesof the dural defect. If the ventral dural opening is not prop-erly closed and the spinal cord not completely isolated fromthe vertebral canal, then recurrence seems possible. Basedon our experience, we believe that adequate dural closureis favored by synthetic dural patches that simultaneouslyprevent formation of adhesions.
Conclusions
In conclusion, based on our experience and also from re-viewing other reports, patients with SSCH have a good sur-gical outcome. Dural and bone defect should be properlyobliterated and a synthetic dural patch is probably the bestmean for watertight closure and prevention of retethering.Long-time follow-up is necessary even if clinical outcomeis excellent.
References
[1] Cobb C III, Ehni G. Herniation of the spinal cord into an iatrogenic
meningocele. J Neurosurg 1973;39:533–6.
[2] Wortzman G, Tasker RR, Rewcastle NB, Richardson JC. Pearson FG
spontaneous incarcerated herniation of the spinal into a vertebral body:
a unique cause of paraplegiadcase report. J Neurosurg 1974;41:631–5.
[3] Borges LF, Zervas NT, Lehrich JR. Idiopathic cord herniation: a treat-
able cause of the Brown-Siquard syndromedcase report. Neurosur-
gery 1995;36:1028–33.
[4] Ammar K, Pritchard P, Matz P, Hadley M. Spontaneous thoracic spinal
cord herniation: three cases with long-term follow-up. Neurosurgery
2005;57:E1067.
[5] Batzdorf U. Idiopathic cord herniation: a treatable cause of the Brown-
Siquard syndromedcase report. Neurosurgery 1995;36:1031–2.
[6] Nakagawa H, Kamimura M, Uchiyama S, Takahara K, Itsubo T,
Miyasaka T. Idiopathic spinal cord herniation associated with a large
erosive bone defect: a case report and review of the literature. J Spinal
Disord Tech 2003;16:299–305.
[7] Waters MR, Stears JC, Osborn AG, Turner GE, Burton BS, Lillehei K,
et al. Transdural spinal cord herniation: imaging and clinical spectra.
AJNR Am J Neuroradiol 1998;19:1337–44.





























