Embed Size (px)
Citation preview
Scand J Infect Dis 33H. Parmar et al.872
REFERENCES
1. Golematis BC, Karkanias GG, Sakorafas GH, Panoussopou-los D. Cutaneous � stula of hydatid cyst in liver. J Chir 1991;128: 439–40.
2. Gonsalez LR, Marcos J, Illanas M, Hernandez M, Pena F,Picouto JP, et al. Radiological aspects of hepatic echinococco-sis. Radiology 1979; 130: 21–7.
3. Schiller CF. Complications of Echinococcal cyst rupture.JAMA 1966; 195: 220–2.
4. Hankins JR. Management of complicated hepatic hydatidcyst. Ann Surg 1963; 158: 1020–2.
5. Lewall DB, McCorkell SJ. Rupture of echinococcal cysts: di-agnosis, classi� cation and clinical implications. AJR Am JRoentgenol 1986; 146: 391–4.
6. Patankar T, Prasad S, Rohandia OS, Mohite JD, Perrum-pillichira JJ, Radhakrishnan R. Fistulization of hepatichydatid cyst into duodenum. Indian J Gastroenterol 1998; 17:152.
Submitted March 5, 2001; accepted March 15, 2001
DOI: 10.1080:00365540110027286
Scand J Infect Dis 33: 872–874, 2001 CASE REPORT
Spontaneous Rupture of the Spleen asPresenting Event in Infectious MononucleosisROBERT A. BADURA1, OLIVIA OLIVEIRA2, MARIA JOAÑ O PALHANO3,JOAÑ O BORREGANA2 and JOANA QUARESMA1
From the Departments of 1Infectious Diseases, 2Surgery and 3Histopathology, Uni×ersity Hospital Santa Maria, Lisbon,Portugal
We report the case of a patient who underwent a life-saving splenectomy after spontaneous rupture of the spleen. The patienthad no history of recent trauma and developed obvious clinical signs of infectious mononucleosis only 5 d after thesplenectomy. Also of note was the late seroconversion in this patient.
R. A. Badura, MD, Hospital Santa Maria, SerØico de Doencas Infecciosas, Piso 5, AØenida Prof. Egas Moniz, PT-1699Lisbon, Portugal.
INTRODUCTION
Infectious mononucleosis (IM) is an acute, frequent andmostly self-limiting disease. It is characterized by a sorethroat, fever, lymphadenopathy and splenomegaly. Inthe prodromal phase, chills, sweats, febrility, anorexiaand malaise are frequently reported. Periorbital oedema,myalgia and feelings of abdominal tenderness may alsooccur.
Although spontaneous rupture of the spleen (SRS) is awell-documented complication of IM, it remains an exceed-ingly rare clinical entity. Lai (1) estimated an incidence of0.5% among IM patients in 1977. In 1978 Rutkow (2)reviewed 107 cases of supposed SRS, applying strict diag-nostic criteria: no history of recent trauma and serologicallyor haematologically con� rmed recent IM. Using these crite-ria, only 18 cases of true SRS were found. This suggestedthat the prevalence of SRS among IM patients was proba-bly lower than was previously believed, lending credit to thereport of Lee et al. (3), who found only 2 cases over a 13-yperiod in a city of 600,000 inhabitants.
SRS as the presenting complaint of IM has only beendescribed twice previously (4, 5). Two further fatal cases ofSRS in IM mentioned in the international literature (6, 7)were probably due to asymptomatic IM and to sudden SRS
with eventual fatal hypovolaemia, respectively.Atypical lymphoid cells and virus-infected B lympho-
cytes, which are normally destroyed by cytotoxic Tlymphocytes, are histopathological features of the disease.The atypical lymphoid cells result in lymphadenopathy andenlargement of the spleen. Spleen enlargement is frequentlyasymptomatic (8). Alternatively, the patient may presentwith a vague feeling of dullness in the upper lefthypochondria.
SRS must be considered in any patient with abdominalpain radiating to the left shoulder (Kehr’s sign) andanaemia. SRS may evolve quickly and is associated with ahigh mortality rate if a prompt diagnosis is not made (9).The mechanisms of SRS in IM are unclear. Studies ofruptured spleens—obtained either at autopsy or atsurgery—show that the organ is usually 2–3 times itsnormal weight (6). The spleens are also highly friable andfrequently disintegrate macroscopically (10). These observa-tions lend weight to the hypothesis that splenic rupture maybe due to an enlarged spleen and to an acute increase inportal venous pressure, causing splenic congestion (2). Typ-ically, splenic rupture is observed during the second andthird weeks of illness, which coincides with the peak oflymphocytosis.
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.
Scand J Infect Dis 33 Rupture of the spleen in infectious mononucleosis 873
CASE REPORT
A 26-y-old female factory worker self-referred to the acute medicalservices on 16 May, 1999 because of intense abdominal pain, feverand fainting episodes. There was no history of trauma to theabdomen and no other past medical history of note. At interview,she reported mild lower back pain and myalgia 2 weeks prior toadmission. She had become febrile a week later. The fever wasaccompanied by chills, nocturnal diaphoresis, nausea and vomit-ing. The patient went to the local emergency service 12 h prior toadmission and was prescribed an antipyretic and an antibiotic.
On admission the patient was pale, febrile, non-icteric, sweatingand had a pulse of 100 beats:min. Her arterial blood pressure was
100:50 mmHg. Low-grade indolent adenopathy was found in thecervical region, but there were no complaints of odynophagia. Theabdomen was painful on compression and decompression in allquadrants. Pain radiated to her back.
Laboratory investigations revealed a haemoglobin level of 8.2mg:dl and a leucocytosis of 18,100 cells:ml. There was relativelympho-monocytosis of 56% and 10% activated lymphocytes werereported. Transaminases (aspartate aminotransferase 171 U:l andalanine aminotransferase 240 U:l) and Gamma-glutamyl transpep-tidase (GGT) (94 U:l) were elevated. A slide Monospot test wasstrongly positive. A CT scan revealed subcapsular haematoma ofthe spleen and free abdominal liquid. A tentative diagnosis of SRS
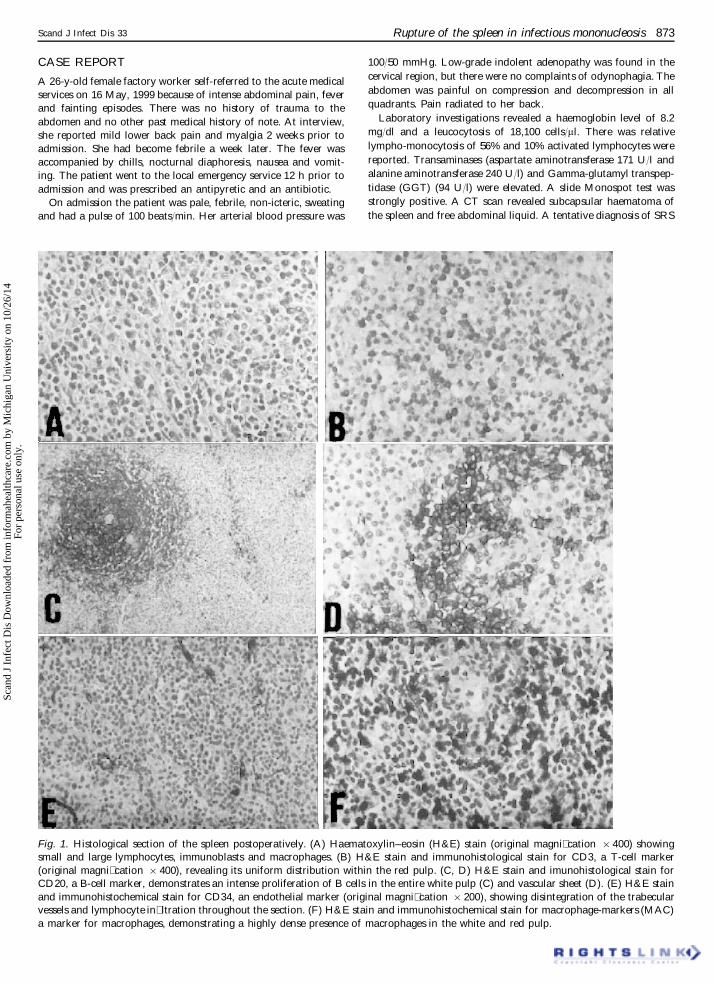
Fig. 1. Histological section of the spleen postoperatively. (A) Haematoxylin–eosin (H&E) stain (original magni� cation ½400) showingsmall and large lymphocytes, immunoblasts and macrophages. (B) H&E stain and immunohistological stain for CD3, a T-cell marker(original magni� cation ½400), revealing its uniform distribution within the red pulp. (C, D) H&E stain and imunohistological stain forCD20, a B-cell marker, demonstrates an intense proliferation of B cells in the entire white pulp (C) and vascular sheet (D). (E) H&E stainand immunohistochemical stain for CD34, an endothelial marker (original magni� cation ½200), showing disintegration of the trabecularvessels and lymphocyte in� ltration throughout the section. (F) H&E stain and immunohistochemical stain for macrophage-markers (MAC)a marker for macrophages, demonstrating a highly dense presence of macrophages in the white and red pulp.
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.
R. A. Badura et al. Scand J Infect Dis 33874
in IM was made. The patient was haemodynamically unstable andreceived a total of 3 units of packed concentrated erythrocyteswithout any signi� cant response. She was then referred for anurgent exploratory laparotomy. Free abdominal blood and a largecollection of coagulated blood in the perisplenic region were found.Two l of blood was aspirated. The spleen was about twice itsnormal weight, highly fragmented, friable and disintegrated upontouch, necessitating a splenectomy.
The patient reported odynophagia 2 d after the operation.Examination on that day revealed an hyperaemic oropharynx andoedema. Only on the 5th day postoperatively did an obviousmembranous bilateral tonsillitis compatible with IM become ap-parent. Symmetrical generalized adenopathy—most obvious in thecervical region—was also found. On the 6th day postoperatively ageneralized � ne erythematous rash without pruritus was noted. Thepatient remained febrile until the 7th day postoperatively and thenbegan to recover uneventfully. Serological evaluation on the 10thday postoperatively showed a positive Paul–Bunnell reaction witha dilution of 1 : 448.
During the follow-up period the patient’s haemoglobin levelnormalized. Seroconversion of VCA IgM and IgG was only con-� rmed 3 months later. VCA IgM became negative 6 months laterand EBNA-1 became positive only :11 months postoperatively.
Postoperative histological examination of the spleen revealed agenerally conserved architecture and several areas with obvioushaemorrhage. In addition to haematoxylin–eosin staining we alsoperformed immunohistochemical staining in order to analyse thehistological specimen more accurately (Fig. 1). The profuselymphoid proliferation of the white pulp crossed the border of thefollicle. A close-up view (Fig. 1A) reveals small and largelymphocytes, immunoblasts and macrophages throughout the en-tire spleen. This in� ltration includes the endothelium of the trabec-ular vessels, causing their disintegration as shown in Fig. 1E. Anintense proliferation of B cells, normally con� ned to the peripheryof the white pulp, involved the entire follicle (Fig. 1C) and thevascular sheet (Fig. 1D). This contrasts with the uniform distribu-tion of CD3» T cells as shown in Fig. 1B within the red pulp.Another remarkable feature is the high density of macrophages inthe white and red pulp, as seen in Fig. 1F. The histological picturewas found to be compatible with a viral infection such as IM.
DISCUSSION
We have described a rare case of SRS as the presentingfeature of IM. The clinical features and the immunologicalresponse to IM only became apparent after a splenectomywas performed. Of note was the late serological response toIM. However, this may have been due to the splenectomyitself: by removing the spleen, the viral and antigenic loadexposed to the reticulo-endothelial system was reduced.Furthermore, a signi� cant number of activated B and Tlymphocytes were removed as a result of the splenectomy.
Of interest is the histological � nding. Asgari and Begos(11) found mostly a red pulp congestedwith lymphocyticandatypical lymphoid cells. Custer and Smith (12) described acongested spleen with focal, speci� cally subcapsular, haem-orrhages, with the white pulp being essentially normal. Incontrast, we found a profuse lymphoid proliferation of thewhite pulp, mainly by B cells involving the entire follicle, andthe red pulp was dominated by a uniform distribution of T
cells and macrophages. Taking into account that the speci� cimmune response was only apparent several months later,one might attribute the histological � nding, in this case, tothe non-speci�c polyclonal B-cell proliferation so typical ofthe initial phase of IM.
Splenectomyhas been the therapy of choice for SRS in IM.Considering the immunological importance of this organand its ability to recover without any sequelae after insult,a more conservative approach has been attempted (13).However, cases of late rupture of the spleen (14) andunsuccessful conservative approaches (15) require observa-tion of the apparently haemodynamically stable patient,preferentially in a critical care setting. For the haemodynam-ically unstable patient the therapy of choice remains thesurgical approach.
REFERENCES
1. Lai PK. Infectious mononucleosis: recognition and manage-ment. Hosp Pract 1977; 12: 47–52.
2. Rutkow IM. Rupture of the spleen in infectious mononucleo-sis: a critical review. Arch Surg 1978; 113: 718–20.
3. Lee PW, Whittaker M, Hall TJ. Spontaneous rupture of thespleen in infectious mononucleosis. Postgrad Med J 1976; 52:725–6.
4. Miranti JP, Rendleman DF. Spontaneous rupture of thespleen as the presenting event in infectious mononucleosis. JAm Coll Health Assoc 1981; 30: 96–7.
5. Farley DR, Zietlow SP, Bannon MP, Farnell MB. Sponta-neous rupture of the spleen due to infectious mononucleosis.Mayo Clin Proc 1992; 67: 846–53.
6. Smith EB, Custer RP. Rupture of spleen in infectiousmononucleosis: clinicopathologic report of 7 cases. Blood1946; 1: 317–33.
7. Jones TJ, Pugsley WG, Grace RH. Fatal spontaneous ruptureof the spleen in asymptomatic infectious mononucleosis. J RColl Surg Edinb 1985; 30: 398.
8. Domerby H, Stangerup SE, Stangerup M, Hauke S. Hep-atosplenomegaly in IM assessed by US. J Laryngol Otol 1986;100: 537–9.
9. Bell JS, Mason JM. Sudden death due to spontaneous ruptureof the spleen from infectious mononucleosis. J Forensic Sci1980; 25: 20–4.
10. Robbins SL. Pathologic basis of diseases. Philadelphia, PA:Saunders, 1974: 470–2.
11. Asgari MM, Begos DG. Spontaneous splenic rupture in infec-tious mononucleosis: A review. Yale J Biol Med 1997; 70:175–82.
12. Custer RP, Smith EB. The pathology of infectious mononu-cleosis. Blood 1948; 3: 830–57.
13. Schwarz M, Zaidenstein L, Freud E, Neuman M, Ziv N,Kornreich L, et al. Spontaneous splenic rupture in infectiousmononucleosis: conservative management with gradual percu-taneous drainage of a subcapsular hematoma. Pediatr Surg Int1999; 15: 139–40.
14. Murat J, Kaisserian G, Boustani R, Grossetti D. Late sponta-neous rupture of the spleen in infectious mononucleosis. PresseMed 1987; 16: 1487.
15. Vitello J. Spontaneous rupture of the spleen in infectiousmononucleosis: a failed attempt at nonoperative therapy. JPediatr Surg 1988; 23: 1043–4.
Submitted October 16, 2000; accepted April 16, 2001
DOI: 10.1080:00365540110076741
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.