Embed Size (px)
Citation preview

Spinal Cord: Motor Neuron Diseases
Kourosh Rezania, MD*, Raymond P. Roos, MD
KEYWORDS
� Motor neuron diseases � Amyotrophic lateral sclerosis � Spinal cord� Familial amyotrophic lateral sclerosis
KEY POINTS
� Amyotrophic lateral sclerosis (ALS), which targets upper and lower motor neurons (MNs),is the most common motor neuron disease.
� Clinicians need to be able to differentiate ALS from motor neuron disease mimics bymeans of the clinical examination, electromyography, imaging, and appropriate laboratorystudies.
� ALS is not just a disease of MNs because non-MN cells can have pathological changes(as in the case of frontotemporal dementia) and can also influence disease.
� Approximately 10% of cases of ALS cases are familial (FALS) with mutations in severaldifferent genes, including SOD1, TDP-43, FUS, and C9ORF72.
� An expanded hexanucleotide repeat in C9ORF72 is the most common cause of FALS andsome cases thought to be sporadic ALS.
INTRODUCTION
Motor neuron disease (MND) represents a group of genetic or neurodegenerativediseases that primarily affect the motor neurons (MNs), resulting in progressive paral-ysis and death. This article starts with an overview of the anatomy of the anterior hornof the spinal cord, followed by the epidemiology, genetics, clinical aspects, pathogen-esis, and treatment of MNDs that affect the lower motor neurons (LMNs) of the spinalcord. The focus of the article is amyotrophic lateral sclerosis (ALS), which is the mostcommon type of MND.
ANATOMY OF THE VENTRAL HORN OF THE SPINAL CORD
MNs that innervate the skeletal muscles are located in the ventral horn (lamina IX) of thespinal cord.1 These neurons are more abundant in the cervical and lumbar cord expan-sions, where they localize in sharply demarcated regions. The number of MNs
Department of Neurology, University of Chicago Medical Center, 5841 South Maryland Avenue,MC 2030, Chicago, IL 60637, USA* Corresponding author.E-mail address: [email protected]
Neurol Clin 31 (2013) 219–239http://dx.doi.org/10.1016/j.ncl.2012.09.014 neurologic.theclinics.com0733-8619/13/$ – see front matter � 2013 Elsevier Inc. All rights reserved.

Rezania & Roos220
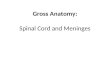
decreasessignificantly after the ageof 60.2 Theaxial and truncalmuscles are innervatedbyMNs located in themedial part of the ventral horn, whereas the upper and lower limbmuscles are innervated by MNs located more laterally.1 The most posterolaterallylocated MNs supply the distal hand and foot muscles (Fig. 1). Onuf nucleus refers toa group of MNs in themost ventral aspect of the sacral spinal cord (S2-4) that innervatemuscles of the pelvic floor, including the striatedmuscles of the sphincters, through thepudendal nerves. MNs are divided based on the type of cell they innervate: a MNs,which supply the extrafusal myofibers, are larger in size than the neighboring cells(soma size of aMNs is generally >37 mm); gMNs, which innervate the intrafusal myofib-ers involved in maintaining muscle tone,3 are larger in number but smaller in size.Other cells that reside in the ventral horns and play an important role in the function
and viability of MNs include interneurons and glial cells. Renshaw cells are inhibitoryinterneurons that receive collaterals from adjacent a MNs. They mediate “recurrentinhibition” for the activated a MN they supply and for adjacent MNs through theirhigh-frequency burst discharges.4,5 Descending pathways of the spinal cord projecton to Renshaw cells and affect their firing rate, thus adjusting the sensitivity of MNsto descending inputs. Renshaw cells also make inhibitory connections with inhibitoryIa interneurons, which act on the antagonistic MNs.6 Glial cells outnumber neurons10 to 50 times in vertebrates.7 Astrocytes are involved in the housekeeping and healthof MNs, including clearance of potentially excitotoxic glutamate from the synapticspace.8 Reactive astrocytes are generated in neurodegenerative and inflammatorystates and are thought to be involved in limiting inflammation, clearing central nervoussystem (CNS) debris, and maintaining the blood-brain barrier. Microglial cells are themain immune effector cells of the CNS. Besides being involved in immune surveillance,
Fig. 1. Cervical spinal cord cross section. On the left side of the figure the location of MNs inthe anterior horn innervating different muscle groups of the upper limb and trunk is demon-strated. TheMNs innervating the flexors are dorsal to those innervating the extensors. On theright side of the figure, demarcated areas with populations of MNs are shown: 1-posterome-dial, 2-anteromedial, 3-anterior, 4-central, 5-anterolateral, and 6-posterolateral. Also notethe somatic efferent fibers from MNs have collaterals that innervate Renshaw cells. Theefferent fibers innervate the intrafusal fibers. (From Parent A, Carpenter MB. Carpenter’shuman neuroanatomy. 9th edition. Baltimore (MD): Williams & Wilkins; 1996. p. 344,Fig. 10.19; with permission.)

Motor Neuron Diseases 221
they secrete cytokines and neurotrophins that can have neuroprotective or neurotoxiceffects. An important role for oligodendrocytes in the health of MNs has been recentlyidentified.9
OVERVIEW OF MNDS
The term MND refers to a group of neurodegenerative diseases that target the LMNsand upper motor neurons (UMNs). MND is either sporadic (ie, secondary to idiopathicdegeneration of MNs) or familial, in which case the progressive loss of MNs is causedby a pathogenic mutation. ALS is the most common subtype of MND. At times, ALS isgenetic and known as familial ALS (FALS). ALS should be considered a heterogeneousdisease from the clinical and pathologic standpoint because involvement of parts ofthe CNS besides the motor system is not infrequently encountered.Progressive muscular atrophy (PMA) is characterized by predominantly LMN
involvement. It should be noted, however, that pathologic evidence of involvementof the UMNs with corticospinal tract degeneration may be found in patients withPMA, which suggests that PMA may be a subtype of ALS without clinical evidenceof UMN involvement.10,11 Spinal muscular atrophy (SMA) and spinal and bulbarmuscular atrophy (SBMA), or Kennedy disease, are two inherited MNDs with pureLMN degeneration. Monomelic amyotrophy (Hirayama disease) is a monophasicillness affecting the LMNs innervating one or both upper extremities, usually in C7/T1 distribution. Primary lateral sclerosis (PLS), which is not discussed further in thisarticle because of its emphasis on spinal cord LMN disorders, is a subtype of MNDcharacterized by pure UMN degeneration.
EPIDEMIOLOGY OF SELECTED MNDS
Sporadic ALS has an incidence of 2 to 3 and prevalence of 2 to 8 per 100,000 (12 amongothers), with a significant increase of prevalence after age 60. It is 20% to 60% morecommon in men than women (12 among others). A recent meta-analysis suggestsa rate of FALS of approximately 5%13; however, the prevalence varies from 17% to23% in prospective studies including active investigations of relatives (reviewed in14).There are several geographic clusters of ALS. Western Pacific ALS was described in
Chamorro natives of Guam and the Mariana islands, where it had an incidence of 50 to100 times greater than the rest of the world.15 Other hotspots of Western Pacific ALSare the Kii Peninsula of Japan and a small area in western New Guinea.16 During itspeak incidence, the male/female ratio of Western Pacific ALS was 2:1, with a medianage of onset of 44.15,17 More recently, there has been a dramatic decrease in the prev-alence of Western Pacific ALS18 suggesting that there may have been exposure to anenvironmental toxin that is no longer present in a population with a genetic predispo-sition for the disease. Excessive consumption on Guam during World War II of theneurotoxin b-N-methylamino-l-alanine, which is present in seeds of the Cycas circina-lis, has been proposed as a cause19,20; however, it is unlikely that a neurotoxic amountof b-N-methylamino-l-alanine could have been ingested from eating these seeds.More recently, it has been hypothesized that a sufficiently high concentration of b-N-methylamino-l-alanine was obtained by the Chamorros’ ingestion of bats, a favoritefood, because the bats feed on the cycads and can thereby concentrate it. Bats are nolonger prevalent on Guam, a potential explanation for the decrease in the incidence ofALS.19,21 This hypothesis needs to be proven, and the possibility that geneticsexplains the disease clusters remains (discussed later).SMA is the most common autosomal-recessive neuromuscular disease and the
most common cause of floppy infant syndrome. A recent study showed a carrier

Rezania & Roos222
frequency of 1 in 54 and an incidence of 1 in 11,000 in the United States.22 The inci-dence and prevalence of SBMA have been estimated at 3.3 per 100,000 for the malepopulation.23 Most of the cases of Hirayama disease are reported in Japan, where thepeak age of onset ranges from 15 to 17 years.24
GENETICS OF SELECTED MNDS
Knowledge of the pathogenesis of ALS has significantly increased through the identi-fication of mutations that cause FALS. The most common inheritance pattern of FALSis autosomal-dominant with complete penetrance; however, an autosomal-dominantpattern with incomplete penetrance, autosomal-recessive, and X-linked pattern havealso been reported.14
Cu/Zn superoxide dismutase 1 (SOD1) was the first gene identified as a cause ofFALS and the most extensively studied to date. SOD1 mutations account for approx-imately 20% of FALS cases25 (reviewed in14). Some FALS cases were subsequentlyfound to be caused by mutations in two RNA binding proteins, TAR DNA-bindingprotein-43 (TDP-43) and fused in sarcoma (FUS). More recently, expansions ofa GGGGCC hexanucleotide repeat in a noncoding region of chromosome 9 openreading frame 72 (C9ORF72) has been identified as the most frequent cause ofFALS.26,27 The latter expansion is present in 37% to 46% of FALS and 6% to 20%of sporadic ALS of European descent.26–28 Other causes of FALS include mutationsin alsin, angiogenin, senataxin, optineurin, ubiquilin 2, VAMP-associated proteintype B, polyphosphoinositide phosphatase, and valosin-containing protein. It shouldbe noted that incomplete penetrance in many pedigrees has been associated withthe previously mentioned genes.There are more than 100 genes that have been reported to impact the risk of
sporadic ALS or its course (http://alsod.iop.kcl.ac.uk/). For example, intermediate-length polyglutamine expansions in ATXN2 gene were detected in 4.7% of ALS casesunselected for family history versus 1.4% of normal control subjects.29 Furthermore, itwas shown that ATXN-2 can modify the MN toxicity of TDP-43.29 An abnormally lownumber of copies of survival of motor neuron 1 (SMN1) gene has been associatedwith ALS.30 Epha4, which encodes a receptor in the ephrin axonal repellent system,has been shown to affect the survival in MND and SMA.31
Mutations in transient receptor potential melastatin 2 (TRPM2) have been suggestedto play a role in the pathogenesis of Western Pacific ALS.32 TRPM2 encodesa calcium-permeable cation channel that is highly expressed in the brain. Inactivationof the channel by the mutation results in decreased intracellular Ca21, which is postu-lated to result in neurodegeneration through downstream signaling pathways.32
SMA is an autosomal-recessive disease that results from deletions of the telomericSMN1 gene in about 95% to 98% of patients. The remainder of SMA cases is causedby small intragenic mutations or mutations that convert SMN1 to SMN2 by disruptingexon 7.33 The SMN2 gene differs from SMN1 by a single nucleotide, leading to alter-native splicing, so that only 10% of SMN2 transcripts code for full length functionalSMN protein. The number of copies of SMN2 per chromosome varies among normalindividuals, from no copies in 10% to 15% of the population to five in most normal indi-viduals.33,34 The number of SMN2 copies correlates with the severity of phenotype ofpatients with SMA. A total of 95% to 100% of the most severely affected patients withSMA with early onset (SMA 1 patients) have one or two copies of SMN2, whereas atleast three copies of SMN2 are present in SMA 3 patients.35
SBMA is an X-linked disease caused by an expansion of a trinucleotide CAG repeat,which encodes a polyglutamine tract in the first exon of the androgen receptor gene.36

Motor Neuron Diseases 223
CLINICAL MANIFESTATIONS OF SELECTED MNDS
ALS usually runs a relentlessly progressive course, resulting in death because of respi-ratory failure, typically 2 to 3 years after onset.37 The onset of ALS peaks between theages of 50 and 75, although the onset could be in the 20s (and rarely earlier) and in the80s. The clinical manifestations of ALS are mainly secondary to dysfunction of UMNsand LMNs (Table 1). Muscle atrophy, fasciculations, hyperreflexia, and pathologicreflexes (including a hyperactive jaw jerk) are usually present, in the absence of ptosis,ocular motor abnormalities, and sensory impairment. In some cases, UMN signs maybe lacking, even in the advanced stages of the disease.38 In other cases, UMN involve-ment may be the most prominent feature of ALS, especially early in the course of thedisease, making it difficult to differentiate from PLS.The initial symptoms usually appear in a limb, and can progress in a segmental
pattern. For example, if a lower limb is initially involved, the contralateral lower limb oripsilateral upper limb is usually the next to be affected. It is speculated that UMN andLMN loss progresses along contiguous three-dimensional anatomic planes becauseof a self-propagated seededaggregation reminiscent of apriondisease, inwhich spreadoccurs to neighboring neurons and glial cells.39,40 A bulbar onset of symptomsoccurs in20% to 30% of the patients, usually in older women.16,41 In a minority of cases ALSbegins with progressive respiratory insufficiency secondary to involvement of LMNsthat innervate the diaphragm and other respiratory muscles.42,43 All cases of ALS thatlive long enough eventually develop involvement of the bulbar and respiratory muscles,resulting indeathunlessmechanical ventilation is used.At times, especiallywith an initialbulbar onset, thecourseofALSmaybe rapid,with survival less than1year after thediag-nosis. Bladder andbowel function is usually spared even in the advanced stagesof ALS,presumablybecause thedegreeof neurodegeneration in theMNsofOnuf nucleus is lesssevere than in otherMNs.44 Similarly, extraocularmuscle involvement is usually not clin-ically apparent except in patients on long term mechanical ventilation.45
Sporadic ALS and FALS can differ in some respects. The mean age of onset of high-penetrance SOD1mutations is 46 to 47 and the weakness more frequently starts in thelower limbs.14 A4V, the most common SOD1 mutation in the United States, is associ-ated with an especially rapid course of progression.46 However, some of the othermutations such as D90A, which is recessively inherited and the most common SOD1mutation in some European countries, are usually associated with a slower courseand longer survival.14,46 The age of onset is slightly younger in patients with high-penetrant FUS mutations and older with TDP-43 mutations than with SOD1 muta-tions.14,47,48 Bulbar-onset ALS and onset in upper limbs are more often encounteredin patients with FUS and TDP-43 mutations respectively than in sporadic ALS. In addi-tion, patientswith FUSmutations tend to have a shorter survival.47,48 ALS caseswith an
Table 1Clinical features of UMN and LMN dysfunction
UMN LMN
WeaknessSlowed rapid alternating movementsSpasticity, clasp knife phenomenonHyperreflexiaPathologic reflexes, including Babinski and HoffmannPresence of reflexes in atrophic limbsPseudobulbar palsy (labile affect, spastic speech, dysarthria,
brisk jaw jerk, and gag reflex)
WeaknessMuscle atrophyFasciculationsCrampsAttenuated or absent reflexesBulbar palsy

Rezania & Roos224
expanded hexanucleotide repeat in C9ORF72 have an earlier mean age of onsetcompared with those without the repeat (56–59 vs 61–62 years old); shorter survival(20 vs 26months); andmore frequent family history of dementia and parkinsonism.28,49
Although ALS is primarily a disease ofMNs, other regions of the nervous system, suchas the frontal and temporal cortex, autonomic system, sensory tracts, and basal ganglia,can be affected. This is evident in the case of ALS-frontotemporal dementia (ALS-FTD),in which there is significant impairment in cognitive functions and behavior because ofdegeneration of nonmotor cortex along with MN involvement. The finding that thesamegenes that cause FALScan lead toALSandALS-FTDandFTD in individualswithinthe same pedigree or in different pedigrees supports the close relationship of thesedisorders. Impairment of cognition, including apathy, irritability, disinhibition, and rest-lessness can occur in up to 50% of ALS-FTD cases with one of eight patients exhibitingclear FTD.50,51 Impairedword findingconsistentwith FTD is found inone-third ofpatientswith ALS.52 Involvement of cortical and extrapyramidal systems is also seen in WesternPacific ALS leading to varied clinical syndromes: ALS, a combined parkinsonism-dementia complex, or a combination of ALS, Parkinsonism and dementia.53
SMA is categorized on the basis of the age of onset and the maximum motor func-tion achieved: the onset of disease in SMA 0 is in utero; SMA 1 (Werdnig-Hoffmanndisease) has onset from birth to 6 months; SMA 2 (Kugelberg-Welander syndrome),3, and 4 have onset at 3 to 15months, 15 months to the teenage years, and adult onset(mean age, 37 years), respectively (reviewed in54). SMA 0 and 1 present with hypo-tonia, problems with sucking and breathing, and inability to sit, with survival of lessthan 2 years when there is no mechanical ventilation. SMA 2 patients are not ableto walk, whereas types 3 and 4 lose their ability to walk later in life. Other symptomsof SMA 2, 3, and 4 include proximal greater than distal muscle weakness, tremors, andfasciculations. Respiratory muscle weakness may occur in the later stages as a resultof weakness of intercostal muscles, whereas diaphragm, facial, and bulbar musclesremain relatively spared. Reflexes are typically attenuated or absent.SBMA has an onset between 30 and 60 years in males. The initial symptoms consist
of postural tremors, fasciculations, muscle cramps, and weakness of facial and bulbarmuscles, that is frequently manifest as a nasal voice and dysphagia. The diseasecourse is slowly progressive with loss of ambulation usually 15 to 20 years after theonset.55 Weakness is usually more severe in proximal than distal limb muscles. Respi-ratory tract infection secondary to aspiration is often the terminal event; however,patients can have a normal life expectancy.55 Patients can have elevated creatinekinase (CK) and mild distal sensory loss. The extraocular and sphincter muscles arespared. Other symptoms that arise from androgen insensitivity include diabetes,glucose intolerance, gynecomastia, testicular atrophy, and erectile dysfunction.56
Female carriers are usually asymptomatic, but may have high CK, hypertension, dys-lipidemia, glucose intolerance, and bulbar muscle weakness (later in life).Monomelic amyotrophy is a pure LMNsyndrome, usually startingbetweenage 15and
25 with a progression that generally lasts less than 5 years.53 The disorder can occurunilaterally or bilaterally. At times a similar process can affect the lower limbs.53,57
Imagingstudies includingcervical spinalMRIwith flexionandextension viewsare impor-tant to rule out structural lesions. The typically normal imaging studies in cases ofmono-melic amyotrophy suggest that it may represent a benign, focal form of MND.58,59
WORK-UP AND DIFFERENTIAL DIAGNOSIS OF MND
Several diagnostic criteria have been proposed for ALS, based on the presence ofUMN signs and evidence for acute and chronic denervation in the electromyography

Motor Neuron Diseases 225
(EMG) (Table 2). EMG signs of denervation include fibrillations, positive sharp waves,fasciculations, neurogenic units, and a neurogenic pattern of recruitment. The EMGcan also be helpful in differentiating ALS from mimics. Nerve conduction studies areusually normal or show diminished amplitude of compound motor action potentials.Genetic testing can expedite the diagnosis in selected cases of familial or sporadic
MND. Commercial testing is available for most of the genetic causes of FALS. Genetictesting for FALS should be considered in patients with a family history of ALS, cogni-tive and behavioral impairment, or unexplained neurodegenerative disease, but isgenerally not recommended for typical cases of sporadic ALS, at least partly becauseof the cost versus benefit. In cases with pure LMN involvement or phenotypic featuresof SMA or SBMA, genetic testing for SMN and androgen receptor mutations should beconsidered. In these cases, it is important to differentiate ALS from the less commonMNDs (SMBA, SMA, and monomelic amyotrophy) because of the different prognosesand potential implication for family members.ALS should be differentiated from other diseases that cause weakness, fascicula-
tions, muscle atrophy, and UMN signs (Tables 3 and 4). The most common mimicsof ALS are compressive myelopathy (especially myeloradiculopathy caused by
Table 2Diagnostic criteria for ALS
Revised El Escorial Criteria83
Awaji Criteria84 (Proposed to Increase theSensitivity of Revised El Escorial Criteria forEarly Diagnosis of ALS)
To make a diagnosis of ALS, there should beclinical or electrophysiologic evidence ofprogression within a region or to otherregions as well as exclusion of ALS mimicsby EMG, appropriate imaging, andlaboratory studies
Definite ALS� UMN and LMN signs* in three regions**Probable ALS� UMN and LMN signs in two regions with
some UMN signs rostral to LMN signsProbable laboratory-supported ALS� UMN and LMN signs, or only UMN signs in
one region with evidence by EMG ofdenervation in two regions
Possible ALS� UMN and LMN signs in one region or UMN
signs in at least two regions* LMN degeneration with muscle
denervation is demonstrated by thefinding on EMG of: fibrillations; positivewaves; large, long duration polyphasicmotor units; unstable and complex motorunits; and reduced recruitment
** LMN degeneration in lumbar and cervicalregions is defined by the presence ofdenervation in two muscles innervated bytwo different nerves and nerve roots. LMNdegeneration is defined by the presence ofdenervation in only one muscle in thethoracic and cranial regions
Definite ALS� Clinical or electrophysiologic evidence of
LMN *** and UMN signs in the bulbarregion and at least two spinal regions orthe presence of LMN and UMN signs inthree spinal regions
Probable ALS� Clinical or electrophysiologic evidence by
LMN and UMN signs in at least two regionswith some UMN signs necessarily rostral to(above) the LMN signs
Possible ALS� Clinical or electrophysiologic signs of UMN
and LMN dysfunction are in only oneregion, or UMN signs alone in two or moreregions, or LMN signs rostral to UMN signs
ALS mimics should be excluded by EMG,appropriate neuroimaging, and clinicallaboratory studies
*** EMG evidence for denervation has equalvalue to clinical LMN signs; when there isclinical suspicion for ALS, fasciculations haveequivalent value to fibrillations and positivewaves in determining denervation

Table 3MND mimics with UMN signs
Disease Distinguishing Features
� Spondylosis Pain and sensory signs frequent; MRIabnormalities
� Multiple sclerosis Sensory signs frequent; MRI lesions, CSFoligoclonal bands
� Sarcoidosis Systemic involvement (eg, lung, lymph node,eye, skin)
� Vasculitis, collagen vascular disease Serology (ANCA), imaging studies
� HTLV-1 and -2 myelopathy Slowly progressive spastic paraparesis withsensory loss and sphincter symptoms. HTLV-1and -2 antibody
� Adrenomyeloneuropathy85 Spastic paraparesis, sphincter impairment,polyneuropathy with slow tempo; high levelsof VLCFA, ABCD1 genotyping
� Prion diseases, especially the amyotrophicform of Creutzfeldt-Jakob disease86–88
Nonmotor signs, especially myoclonus andrapidly evolving dementia, are usuallyprominent; abnormal EEG
� Hereditary spastic paraparesis89 Pure UMN syndrome, positive family history,exclusion of other causes of myelopathy,genetic testing (can be AD, AR, and X linked);SPG4 is the most common subtype andaccounts for 50% of AD cases; SPG 11 the mostcommon AR type; SPG 11, 17, and 31 areassociated with hand amyotrophy
� Neurolymphomatosis CSF analysis, nerve root enhancement on theMRI, lymphomatous infiltration in nervebiopsy
� Radiation-induced radiculomyelopathy History of radiation treatment, presence ofmyokymic discharges on EMG
� Lyme disease Lyme antibody, CSF pleocytosis
� Polyglucosan body disease90 Polyglucosan bodies in nerve or muscle biopsy,GBE1 genotyping, sensory loss, � neurogenicbladder, cognitive dysfunction,extrapyramidal disease
Abbreviations: AD, autosomal dominant; ANCA, antineutrophil cytoplasmic antibodies; AR, auto-somal recessive; CSF, cerebrospinal fluid; GBE, glycogen brancher enzyme; HTLV, Human T-lympho-tropic virus; VLCFA, very long chain fatty acids.
Rezania & Roos226
cervical spondylosis); motor neuropathy or neuronopathy (especially multifocal motorneuropathy or a paraneoplastic syndrome); polyradiculopathy (especially chronicinflammatory demyelinating polyradiculoneuropathy); diseases of the neuromuscularjunction (myasthenia gravis and Eaton-Lambert syndrome); and myopathies (espe-cially inclusion body myositis). Differentiation can usually be made because MNDmimics are frequently associated with pain, sensory impairment, ocular motor abnor-malities, or bladder or bowel involvement. It is essential to obtain imaging studies(preferably MRIs) of the highest level of involvement: brain for cases with bulbarinvolvement, and cervical spine for upper limb involvement. This is mainly to excludethe mimics rather than to provide confirmation of the diagnosis of ALS.Viral infections that cause lower motor neuronopathy (West Nile virus, poliovirus,
and nonpolio enteroviruses, such as enterovirus 71) are distinguished from LMN forms

Table 4MND mimics with LMN but not UMN signs
Motor Neuronopathy Neuropathy- Radiculopathy Nerve HyperexcitabilityNeuromuscular JunctionDiseases Myopathy
� Acute viral diseases� Poliomyelitis� Enterovirus 7191
� WNV� Postpolio syndrome� Hexosaminidase A
deficiency(adult-onset Tay-Sachs)92
� Paraneoplastic motorneuronopathy60,61
� Multifocal motorneuropathy
� Guillain-Barre syndrome� CIDP and its variants� POEMS� Porphyria� Lead intoxication� Amyloidosis� Polyglucosan body disease
(it can involve LMNs or presentas a myopathy)
� Benign fasciculations� Fasciculation cramp
syndrome� Isaacs syndrome� Morvan syndrome
� Myasthenia gravis(including muscle-specifickinase antibody relatedmyasthenia)
� LEMS� Botulism� Congenital myasthenia
� Sporadic inclusion bodymyositis� Familial inclusion body myositis� Chronic polymyositis� Myofibrillar myopathy� Nemaline rod disease� Polyglucosan body disease� Amyloidosis� Congenital myopathies
Abbreviations: CIDP, chronic inflammatory demyelinating polyneuropathy; LEMS, Lambert-Eatonmyasthenic syndrome;MG, myasthenia gravis; POEMS, polyneur-opathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes; WNV, West Nile virus.
MotorNeuronDise
ases
227

Rezania & Roos228
of MND because they have an acute onset. West Nile CNS infection has emerged asa not infrequent cause of LMN dysfunction in the United States. Cerebrospinal fluidstudies including serologic tests (specially spinal fluid IgM antibody against the virus),and polymerase chain reaction testing are used to diagnose the latter conditions.Postpolio syndrome, especially postpolio syndrome, is a pure LMN neuronopathycharacterized by late-onset weakness with progressive atrophy of limbs that wereaffected by prior poliomyelitis. In contrast to ALS, postpolio syndrome has no UMNsigns, is slowly progressive, and tends to have a relatively benign course. Adult-onset hexosaminidase A deficiency can present with proximal weakness, however,some cases may have spasticity, hyperreflexia, cognitive, psychiatric, cerebellar,and extrapyramidal features. Diagnosis is made by hexosaminidase A enzymaticassay. A self-limited, subacute motor neuronopathy has been reported in associationwith an underlying lymphoma.60 These paraneoplastic motor neuronopathies can beassociated with antibodies to Hu and Yo.61,62 As a result of these associations, serumprotein immunoelectrophoresis/immunofixation and a paraneoplastic antibody profileare not infrequently part of the work-up of patients with MND. Imaging studies(including positron emission tomography) to detect an underlying lymphoma or carci-noma should be considered in selected cases, including those with seropositivity toparaneoplastic autoantibodies.Other categories of MND mimics include polyradiculopathies and neuropathies.
Similar to ALS multifocal motor neuropathy usually presents with asymmetric limbonset weakness and fasciculations without sensory impairment. Multifocal motorneuropathy usually targets hand muscles. Muscle atrophy can be rather mild evenwhen severe weakness is present, and UMN signs are usually not present. Multifocalmotor neuropathy can be differentiated from ALS based on of the presence of conduc-tion blocks on nerve conduction study and, in some cases, antibodies to GM1. Otherneuropathies that may mimic ALS include chronic inflammatory demyelinating polyra-diculoneuropathy and POEMS syndrome (polyneuropathy, organomegaly, endocrin-opathy, monoclonal gammopathy, and skin changes); however, in contrast to ALS,these condition have a demyelinating range of slowing on nerve conduction studies.A nerve biopsy is often necessary to diagnose polyglucosan body disease or amyloid-osis. Repetitive nerve stimulation and measurement of acetylcholine receptor bindingantibodies, muscle-specific kinase antibodies, and P/Q calcium channel antibodieshelp differentiate a neuromuscular junction disease from MND. Measurement of CKmay help differentiate a myopathy from ALS; however, an elevation of CK three tofour times normal is frequently reported in ALS cases, with occasional elevationsmore than 1000 U/L. Higher levels of CK (up to eight times normal) can be seen inSBMA.63 CK is often normal in patients with inclusion body myositis, one of themost common ALS mimics. A muscle biopsy should be considered if the CK is mark-edly elevated or if myopathic motor units are present on needle EMG. A nerve hyper-excitability syndrome is differentiated from MND based on the lack of significantmuscle weakness, the presence of neuromyotonic and myokymic discharges on nee-dle EMG, and seropositivity to antibodies to voltage-gated potassium channel in somecases.
PATHOLOGY AND PATHOGENESIS OF MND
Autopsy tissue from ALS demonstrates: a loss of MNs; astrocytosis of the motorcortex, brainstem, and spinal cord; secondary degeneration and atrophy of the pyra-midal tracts and anterior roots; secondary neurogenic atrophy of skeletal muscles.64,65
Although the pathology predominantly affects the motor system, it often involves other

Motor Neuron Diseases 229
systems, such as frontal and temporal cortex. Evidence of degeneration of long tractsof the spinal cord besides the lateral and anterior pyramidal tracts has been reported insome cases of FALS.66 As in the case with other neurodegenerative diseases, MNs ofpatients with ALS can display intracellular aggregates that form inclusion bodies(Table 5).Table 6 summarizes the proposed pathogenicity of some of the more common
genetic causes of MND. Wild-type SOD1 is an intracellular antioxidant involved inthe clearance of toxic superoxide free radicals. More than 100 different mutations inSOD1 account for about 20% of the familial cases (http://alsod.iop.kcl.ac.uk/misc/FAQs.aspx). Several transgenic mice have been produced that express differentFALS-associated mutant SOD1s and develop ALS. Studies of these transgenic micehave shown that MND in these mice is primarily caused by a toxic gain of function ofthe mutant SOD1, rather than reduced enzymatic activity. Several pathogenic featuresseem to be at play resulting inMNdegeneration including oxidative damage; glutamateexcitotoxicity; intracellular aggregates of misfolded proteins; mitochondrial dysfunc-tion; and abnormalities in axonal transport, neurotrophic factors, and RNA processing(reviewed in67). Although the toxicity ofmutant SOD1 is not fully understood,misfoldingand aggregation is generally thought to underlie the basis for MN degeneration. Aggre-gates of mutant SOD1 could cause toxicity by sequestering SOD1-binding proteinsthat are critical for viability of the MN or by exposing a toxic domain of SOD1. Theexpression of mutant SOD1 in non-MN cells, such as astrocytes, microglia, and oligo-dendrocytes, as well as MNs have an influence on the onset and progression of the
Table 5Inclusion bodies in MND
Type of Inclusion Cellular Location Characteristics
Ubiquinated inclusions93,94 Cell bodies or dendrites ofLMNs
Also in hippocampus andcerebral cortex in ALS-FTD
Contains ubiquitin and maycontain dorfin, TDP-43,ubiquilin 2, FUS, optineurin,(contains SOD1 in SOD1mutations)
Intracytoplasmic, fibrillary(skein-like) inclusions,compact inclusions, and Lewybody–like inclusions
Highly sensitive and specific forALS
Bunina bodies95 LMNs, other neurons(eg, STN, RF)
Eosinophilic, possible lysosomalorigin
Hyaline conglomerates LMNs, rarely Betz cells NF proteins and SOD1Pale, hyaline appearance,
argyrophilicOnly seen in cases of mutant
SOD1-induced FALS
Basophilic inclusions MNs, basal ganglia, thalamus,cerebellum
� ubiquitinFrequent in some cases of
juvenile-onset ALS
Spheroids Large inclusions in proximalpart of axons of the LMNs
Phosphorylated heavy, light,and medium NFs; negative orsubtle staining for ubiquitin
Not specific for ALS
Abbreviations: NF, neurofilament; RF, reticular formation; STN, sub-thalamic nucleus.

Table 6Mutated genes that cause MNDs
Gene (Encoded Protein) Phenotype, (Target Cells) Suggested Mechanism
SOD1 (Cu/Zn superoxidedismutase)
ALS (LMN, UMN, can be LMNpredominant)
Mitochondrial toxicity ofmisfolded mutant SOD1 inMNs and astrocytes,67,96,97
abnormalities of axonaltransport,98 malfunctionof the astrocytic EAAT2transporter resulting inimpaired reuptake ofglutamate with resultantexcitotoxicity,67
endoplasmic reticulumdysfunction in respondingto misfolded proteins(endoplasmic reticulumstress),99,100 paradoxicalincrease of extracellularsuperoxide radicals,resulting in oxidativestress, through theactivation of NADPHoxidase (Nox) pathway.101
C9ORF72 (unknown)26,102,103 ALS, ALS-FTD, FTD(LMN, UMN)
Abnormal RNA produced asa result of pathogenicexpanded repeat couldcause neurotoxicitybecause of a loss infunction or because ofdisruption of transcriptionor splicing/processingof mRNAs (due tosequestration ofRNA-binding proteins).
TARDBP (TDP-43)71,104 ALS, ALS-FTD, FTD Abnormal cytoplasmicaccumulation and loss ofnormal nuclear localizationof TDP-43 in neurons andglia of UMNs and LMNs,neocortex, andhippocampus.
MN toxicity could becaused by a loss offunction of nuclear TDP-43causing abnormalities inRNA splicing andmessenger RNA processingor a gain of functioncaused by cytoplasmicaggregation, ora combination of both.
(continued on next page)
Rezania & Roos230

Table 6(continued)
Gene (Encoded Protein) Phenotype, (Target Cells) Suggested Mechanism
FUS (FUS/TLS)104 ALS (LMN, UMN), ALS-FTD Inclusions immunoreactive forFUS in neuronal and glial cells.Neurotoxicity could be theresult of a toxic gain-of-function, a loss-of-functionmechanism by depletion ofphysiologic FUS, ora combination of both.
SMN gene72 (SMN) SMA (LMN) SMN is involved in the formationof snRNP complexes, whichare important for pre-mRNAsplicing. Lack of SMN functionresults in altered snRNPstructures and abnormalsplicing of RNA with resultantMN toxicity.
SMN’s interaction with RNAbinding proteins is importantin localization and transport ofmRNA in MNs. Lack offunction of SMN results indisturbance of proteinsynthesis in MN axons andsynapses.
Androgen receptor(androgen receptor)103,105
SBMA, Kennedy disease(LMN, DRG)
Abnormal polyglutamateaggregates could cause alteredfunction through aberrantprotein interactions,transcriptional dysregulation,mitochondrial dysfunction,RNA toxicity, impaired axonaltransport, and excitotoxicity.
Abbreviation: snRNP, small nuclear ribonucleoproteins.
Motor Neuron Diseases 231
disease in mutant SOD1 mice. Of note, abnormalities of the structure and function ofwild-type SOD1 have been described in sporadic ALS suggesting that abnormalities inSOD1 may be a final common pathway in the sporadic and familial disease.68
TDP-43 is a nuclear factor that functions in regulating transcription and alternativesplicing of RNA.69,70 The importance of TDP-43 in ALS was brought home by studiesthat showed that all cases of sporadic ALS have TDP-43 cytoplasmic inclusions.71 Incontrast, ALS cases secondary to mutant SOD1 have cytoplasmic aggregates of ubiq-uitinated SOD1 in neural cells without TDP-43, suggesting that mutant SOD1-inducedFALS ALS has a different pathophysiology than sporadic ALS, and that the response ofmutant SOD1 FALS transgenic mouse to treatment may not predict the response insporadic ALS. It may be that the displacement of TDP-43 from the nucleus of neuralcells in patients with ALS triggers a loss in function with respect to its interactionswith RNA (eg, splicing) aswell as a toxic gain in function. The hexanucleotide expandedrepeat found in the noncoding region of C9ORF72 may induce FALS because of“toxicity” of RNA or because of a loss in function. The toxicity of this expanded regionof the RNA may at least partly be related to sequestration of RNA-binding proteins, as

Rezania & Roos232
seems to be the case in myotonic dystrophy. The importance of TDP-43, FUS, and theexpanded hexanucleotide repeat of C9ORF72 in FALS (and SMN in SMA) has focusedinvestigators on the role of RNA in MND pathogenesis. SMA is caused by loss of func-tion of SMN, which is present in the cytoplasm and nucleus of all cells and plays a crit-ical role in pre-mRNA splicing (see Table 6).72 SBMA is caused by an expansion ofa trinucleotide CAG repeat, which encodes a polyglutamine tract in the first exon ofthe androgen receptor gene located on chromosome Xq12–21.36 The normal CAGrepeat number is 17 to 26, whereas the disease is associated with 40 to 52 repeats.An increasing number of repeats is associated with earlier onset and more severedisease.36,73 Inclusions containing the amino-terminal of the polyglutamine-expanded androgen receptor accumulate in the nucleus of LMNs and dorsal rootganglia, resulting in neuronal death.74
TREATMENT
Riluzole is the only medication that has been shown to be effective in ALS; however, itseffect is relatively small. Administration of riluzole, 50 mg twice a day, improves 1-yearsurvival by about 15% and prolongs overall survival by 2 to 3 months (reviewed in75,76).The prolongation of survival may be more significant if riluzole is started early in thecourse of the disease. Although some patients with PMA and PLS may benefit fromriluzole, the efficacy of riluzole in these conditions has not been proven.75
The cornerstones of symptomatic treatment of ALS include walking assists,management of respiratory impairment, nutritional support, treatment of sialorrhea,and palliative care. Although FVC is the most commonly used respiratory parameter,maximal inspiratory pressure, sniff nasal pressure, supine FVC, and nocturnal oxime-try are more sensitive than FVC in detecting early respiratory impairment in ALS.77
Elevated serum bicarbonate and low serum chloride in the setting of respiratory symp-toms may predict the occurrence of respiratory failure.76 Early institution of noninva-sive positive pressure ventilation probably improves survival and slows the rate ofdecline of the FVC.78 Box 1 summarizes the indications of noninvasive positive
Box 1
Indications for starting noninvasive positive pressure ventilation in ALS75,76
Any of the following symptoms or signs of respiratory muscle weakness:
� Shortness of breath (dyspnea, tachypnea, orthopnea, use of accessory respiratory muscles atrest)
� Nocturnal arousals
� Excessive daytime drowsiness and fatigue
� Morning headache
� Paradoxic respiration
AND
Any of the following abnormalities on respiratory function tests:
� FVC <80% of predicted value
� Sniff nasal pressure <40 cm H2O
� Maximal inspiratory pressure <60 mm H2O
� Nocturnal desaturation <90% for more than 1 cumulative minute on overnight oximetry
� Morning blood gas PCO2 >45 mm Hg

Motor Neuron Diseases 233
pressure ventilation in ALS.75,76 More recently, diaphragm pacing has been used inselected patients with ALS with moderately impaired respiratory function and viablephrenic nerves and diaphragm as determined by nerve conduction study, fluoroscopy,or ultrasonography (reviewed in79). Ongoing studies are being conducted to assessthe efficacy of diaphragm pacing in improving quality of life and survival in patientswith ALS. Another measure that is thought to improve survival and quality of life inpatients with ALS is percutaneous endoscopic gastrostomy. Because the percuta-neous endoscopic gastrostomy procedure has a higher complication rate when signif-icant respiratory impairment is present, it should preferably be done when the FVC isgreater than 50%predicted.75–77 Other parameters that determine the timing of percu-taneous endoscopic gastrostomy include the presence of bulbar symptoms, weightloss of more than 10%, and the patient’s general condition.Some of the promising treatment approaches to MND include stem cell transplan-
tation and methods to lower the level of pathogenic RNAs. MN cell transplantationfaces the difficulty of making appropriate and functional connections to targetmuscles. Therefore, transplantation of precursor neural cells seems to be a more real-istic approach to prevent surviving MNs from degeneration because of theirsupportive and trophic effect (reviewed in80). Antisense oligonucleotides and RNAinterference have been proposed or are being used to knock down SOD1 or
Case study
A 46 year old developed weakness of the right hand with difficulty buttoning 6 years aftera cervical spinal fusion. She had no sensory symptoms or pain. The family history was significantfor dementia in a grandmother. An MRI of the cervical spine showed postoperative changes,but no nerve root compression or central spinal stenosis. She initially underwent carpal andcubital tunnel release 8 months later with no improvement. She then developed progressiveweakness in the left hand, weakness of the right arm, difficulty rising from a chair, and muscletwitching and occasional cramping in the extremities and trunk. On examination, the cranialnerves were normal, except for a brisk jaw jerk. Moderate weakness, muscle atrophy, andfrequent fasciculations were noted in multiple muscle groups of both arms. No significantweakness was present in the lower limbs but the muscle tone was increased. Reflexes werediffusely brisk and the Hoffmann reflex was present bilaterally. Nerve conduction studyshowed normal sensory nerve action potentials. The amplitudes of the right median and ulnarmotor nerve action potentials were reduced with mildly slowed conduction velocities, andslight prolongation of distal and F wave latencies. Needle EMG demonstrated widespreaddenervation and fasciculations in all muscles tested in the upper and lower limbs and thoracicparaspinal muscles. Serum protein immunoelectrophoresis and serologic testing for Lymedisease, collagen vascular disease, vasculitis, and paraneoplastic antibody panel antibodieswere negative.
A diagnosis of ALS was made based on the history of progressive weakness and clinicalevidence of UMN involvement and LMN signs, with fasciculations in the upper limbs andEMG demonstration of widespread denervation involving three myotomes. ALS mimics(specially cervical radiculomyelopathy) were excluded with appropriate imaging and labora-tory tests. A genetic test was not performed, but could have been considered because theage of onset was earlier than typical ALS and there was a family history of dementia.
Riluzole was started after the diagnosis of ALS was made. During the next 2 years, the patientdeveloped progressive dysphagia, dysarthria, and deteriorating respiratory muscle weakness. Apercutaneous endoscopic gastrostomy was placed, and she was started on noninvasive positivepressure ventilation. Diaphragm pacing was started about 3 years after the onset of symptoms.One year later palliative care was instituted. The patient died of complications of progressiverespiratory insufficiency 5 years after the onset of symptoms and 2 years after diaphragmpacing had been started.

Rezania & Roos234
C9ORF72 expression or alter the splicing of SMN2 (reviewed in81). Other treatmentapproaches for SMA include strategies to activate SMN2 gene expression or stabilizeSMN protein (reviewed in82).
REFERENCES
1. Parent A, Carpenter MB. Carpenter’s human neuroanatomy. 9th edition.Baltimore (MD): Williams & Wilkins; 1996.
2. Tomlinson BE, Irving D. The numbers of limb motor neurons in the human lumbo-sacral cord throughout life. J Neurol Sci 1977;34(2):213–9.
3. Strick PL, Burke RE, Kanda K, et al. Differences between alpha and gammamotoneurons labeled with horseradish peroxidase by retrograde transport.Brain Res 1976;113(3):582–8.
4. Willis WD. The case for the Renshaw cell. Brain Behav Evol 1971;4(1):5–52.5. Alvarez FJ, Fyffe RE. The continuing case for the Renshaw cell. J Physiol 2007;
584(Pt 1):31–45.6. Baldissera F, Hultborn H, Illert M. Integration in spinal neuronal systems. In:
Handbook of Physiology, vol 2. The Nervous System: Motor Control AmericanPhysiological Society. Bethesda: V.B. Brooks; 1981. p. 509–95.
7. Kandel ER, Schwartz JH, Jassell TM. Principles of neural science. 4th edition.New York: McGraw-Hill, Health Professions Division; 2000.
8. Phani S, Re DB, Przedborski S. The role of the innate immune system in ALS.Front Pharmacol 2012;3:150.
9. Lee Y, Morrison BM, Li Y, et al. Oligodendroglia metabolically support axons andcontribute to neurodegeneration. Nature 2012;487(7408):443–8.
10. Sasaki S, Iwata M. Immunocytochemical and ultrastructural study of the motorcortex in patients with lower motor neuron disease. Neurosci Lett 2000;281(1):45–8.
11. Ince PG, Evans J, Knopp M, et al. Corticospinal tract degeneration in theprogressive muscular atrophy variant of ALS. Neurology 2003;60(8):1252–8.
12. Yoshida S, Mulder DW, Kurland LT, et al. Follow-up study on amyotrophic lateralsclerosis in Rochester, Minn., 1925 through 1984. Neuroepidemiology 1986;5(2):61–70.
13. Byrne S, Walsh C, Lynch C, et al. Rate of familial amyotrophic lateral sclerosis:a systematic review and meta-analysis. J Neurol Neurosurg Psychiatry 2011;82(6):623–7.
14. Andersen PM, Al-Chalabi A. Clinical genetics of amyotrophic lateral sclerosis:what do we really know? Nat Rev Neurol 2011;7(11):603–15.
15. Kurland LT, Mulder DW. Epidemiologic investigations of amyotrophic lateralsclerosis. I. Preliminary report on geographic distribution and special referenceto the Mariana Islands, including clinical and pathologic observations.Neurology 1954;4(6):438–48.
16. Mitsumoto H, Przedborski S, Gordon PH. Amyotrophic lateral sclerosis. NewYork: Taylor & Francis; 2006.
17. Kurland LT, Mulder DW. Epidemiologic investigations of amyotrophic lateralsclerosis. I. Preliminary report on geographic distribution, with special referenceto the Mariana Islands, including clinical and pathologic observations.Neurology 1954;4(5):355–78.
18. Plato CC, Galasko D, Garruto RM, et al. ALS and PDC of Guam: forty-yearfollow-up. Neurology 2002;58(5):765–73.

Motor Neuron Diseases 235
19. Spencer PS, Nunn PB, Hugon J, et al. Motorneurone disease on Guam: possiblerole of a food neurotoxin. Lancet 1986;1(8487):965.
20. Armon C. Western Pacific ALS/PDC and flying foxes: what’s next? Neurology2003;61(3):291–2.
21. Cox PA, Sacks OW. Cycad neurotoxins, consumption of flying foxes, andALS-PDC disease in Guam. Neurology 2002;58(6):956–9.
22. Sugarman EA, Nagan N, Zhu H, et al. Pan-ethnic carrier screening and prenataldiagnosis for spinal muscular atrophy: clinical laboratory analysis of >72,400specimens. Eur J Hum Genet 2012;20(1):27–32.
23. Guidetti D, Sabadini R, Ferlini A, et al. Epidemiological survey of X-linked bulbarand spinal muscular atrophy, or Kennedy disease, in the province of ReggioEmilia, Italy. Eur J Epidemiol 2001;17(6):587–91.
24. Hosokawa T, Fujieda M, Wakiguchi H, et al. Pediatric Hirayama disease. PediatrNeurol 2010;43(2):151–3.
25. Rosen DR. Mutations in Cu/Zn superoxide dismutase gene are associated withfamilial amyotrophic lateral sclerosis. Nature 1993;364(6435):362.
26. Renton AE, Majounie E, Waite A, et al. A hexanucleotide repeat expansion inC9ORF72 is the cause of chromosome 9p21-linked ALS-FTD. Neuron 2011;72(2):257–68.
27. DeJesus-Hernandez M, Mackenzie IR, Boeve BF, et al. Expanded GGGGCChexanucleotide repeat in noncoding region of C9ORF72 causes chromosome9p-linked FTD and ALS. Neuron 2011;72(2):245–56.
28. van Rheenen W, van Blitterswijk M, Huisman MH, et al. Hexanucleotide repeatexpansions in C9ORF72 in the spectrum of motor neuron diseases. Neurology2012;79(9):878–82.
29. Elden AC, Kim HJ, Hart MP, et al. Ataxin-2 intermediate-length polyglutamineexpansions are associated with increased risk for ALS. Nature 2010;466(7310):1069–75.
30. Corcia P, Camu W, Halimi JM, et al. SMN1 gene, but not SMN2, is a risk factor forsporadic ALS. Neurology 2006;67(7):1147–50.
31. Van Hoecke A, Schoonaert L, Lemmens R, et al. EPHA4 is a disease modifier ofamyotrophic lateral sclerosis in animal models and in humans. Nat Med 2012.[Epub ahead of print].
32. Hermosura MC, Cui AM, Go RC, et al. Altered functional properties of a TRPM2variant in Guamanian ALS and PD. Proc Natl Acad Sci U S A 2008;105(46):18029–34.
33. Ogino S, Wilson RB, Gold B. New insights on the evolution of the SMN1 andSMN2 region: simulation and meta-analysis for allele and haplotype frequencycalculations. Eur J Hum Genet 2004;12(12):1015–23.
34. Markowitz JA, Singh P, Darras BT. Spinal muscular atrophy: a clinical andresearch update. Pediatr Neurol 2012;46(1):1–12.
35. Mailman MD, Heinz JW, Papp AC, et al. Molecular analysis of spinal muscularatrophy andmodification of the phenotype by SMN2. Genet Med 2002;4(1):20–6.
36. La Spada AR, Wilson EM, Lubahn DB, et al. Androgen receptor gene mutationsin X-linked spinal and bulbar muscular atrophy. Nature 1991;352(6330):77–9.
37. Rowland LP, Shneider NA. Amyotrophic lateral sclerosis. N Engl J Med 2001;344(22):1688–700.
38. Kim WK, Liu X, Sandner J, et al. Study of 962 patients indicates progressivemuscular atrophy is a form of ALS. Neurology 2009;73(20):1686–92.
39. Polymenidou M, Cleveland DW. The seeds of neurodegeneration: prion-likespreading in ALS. Cell 2011;147(3):498–508.

Rezania & Roos236
40. Ravits JM, La Spada AR. ALS motor phenotype heterogeneity, focality, andspread: deconstructing motor neuron degeneration. Neurology 2009;73(10):805–11.
41. Hardiman O, van den Berg LH, Kiernan MC. Clinical diagnosis and manage-ment of amyotrophic lateral sclerosis. Nat Rev Neurol 2011;7(11):639–49.
42. Fromm GB, Wisdom PJ, Block AJ. Amyotrophic lateral sclerosis presenting withrespiratory failure. Diaphragmatic paralysis and dependence on mechanicalventilation in two patients. Chest 1977;71(5):612–4.
43. Scelsa SN, Yakubov B, Salzman SH. Dyspnea-fasciculation syndrome: earlyrespiratory failure in ALS with minimal motor signs. Amyotroph Lateral SclerOther Motor Neuron Disord 2002;3(4):239–43.
44. Kihira T, Yoshida S, Yoshimasu F, et al. Involvement of Onuf’s nucleus in amyo-trophic lateral sclerosis. J Neurol Sci 1997;147(1):81–8.
45. Mizutani T, Aki M, Shiozawa R, et al. Development of ophthalmoplegia in amyo-trophic lateral sclerosis during long-term use of respirators. J Neurol Sci 1990;99(2–3):311–9.
46. Cudkowicz ME, McKenna-Yasek D, Sapp PE, et al. Epidemiology of mutations insuperoxide dismutase in amyotrophic lateral sclerosis. Ann Neurol 1997;41(2):210–21.
47. Millecamps S, Salachas F, Cazeneuve C, et al. SOD1, ANG, VAPB, TARDBP,and FUS mutations in familial amyotrophic lateral sclerosis: genotype-phenotype correlations. J Med Genet 2010;47(8):554–60.
48. Kirby J, Goodall EF, Smith W, et al. Broad clinical phenotypes associated withTAR-DNA binding protein (TARDBP) mutations in amyotrophic lateral sclerosis.Neurogenetics 2010;11(2):217–25.
49. Byrne S, Elamin M, Bede P, et al. Cognitive and clinical characteristics ofpatients with amyotrophic lateral sclerosis carrying a C9orf72 repeat expansion:a population-based cohort study. Lancet Neurol 2012;11(3):232–40.
50. Phukan J, Elamin M, Bede P, et al. The syndrome of cognitive impairment inamyotrophic lateral sclerosis: a population-based study. J Neurol NeurosurgPsychiatry 2012;83(1):102–8.
51. Grossman AB, Woolley-Levine S, Bradley WG, et al. Detecting neurobehavioralchanges in amyotrophic lateral sclerosis. Amyotroph Lateral Scler 2007;8(1):56–61.
52. Lomen-Hoerth C, Murphy J, Langmore S, et al. Are amyotrophic lateral sclerosispatients cognitively normal? Neurology 2003;60(7):1094–7.
53. Brown RH, Swash M, Pasinelli P. Amyotrophic lateral sclerosis. 2nd edition.Abingdon (England) and Boca Raton (FL): Informa Healthcare; Distributed inNorth America by Taylor & Francis; 2006.
54. Mercuri E, Bertini E, Iannaccone ST. Childhood spinal muscular atrophy: contro-versies and challenges. Lancet Neurol 2012;11(5):443–52.
55. Atsuta N, Watanabe H, Ito M, et al. Natural history of spinal and bulbar muscularatrophy (SBMA): a study of 223 Japanesepatients. Brain 2006;129(Pt 6):1446–55.
56. Sinnreich M, Sorenson EJ, Klein CJ. Neurologic course, endocrine dysfunctionand triplet repeat size in spinal bulbar muscular atrophy. Can J Neurol Sci 2004;31(3):378–82.
57. Hamano T, Mutoh T, Hirayama M, et al. MRI findings of benign monomelic amyo-trophy of lower limb. J Neurol Sci 1999;165(2):184–7.
58. Willeit J, Kiechl S, Kiechl-Kohlendorfer U, et al. Juvenile asymmetric segmentalspinal muscular atrophy (Hirayama’s disease): three cases without evidence of“flexion myelopathy.” Acta Neurol Scand 2001;104(5):320–2.

Motor Neuron Diseases 237
59. Ammendola A, Gallo A, Iannaccone T, et al. Hirayama disease: three casesassessed by F wave, somatosensory and motor evoked potentials andmagnetic resonance imaging not supporting flexion myelopathy. Neurol Sci2008;29(5):303–11.
60. Schold SC, Cho ES, Somasundaram M, et al. Subacute motor neuronopathy:a remote effect of lymphoma. Ann Neurol 1979;5(3):271–87.
61. Verma A, Berger JR, Snodgrass S, et al. Motor neuron disease: a paraneoplasticprocess associated with anti-hu antibody and small-cell lung carcinoma. AnnNeurol 1996;40(1):112–6.
62. Khwaja S, Sripathi N, Ahmad BK, et al. Paraneoplastic motor neuron diseasewith type 1 Purkinje cell antibodies. Muscle Nerve 1998;21(7):943–5.
63. Chahin N, Sorenson EJ. Serum creatine kinase levels in spinobulbar muscularatrophy and amyotrophic lateral sclerosis. Muscle Nerve 2009;40(1):126–9.
64. Charcot JM, Joffroy A. Deux cas d’atrophy musculaire progressive avec lesionsde la substance grise et des faisceaux antero-lateraux de la moelle epiniere.Arch Physiol Neurol Pathol 1869;2:744–60.
65. Hirano A, Arumugasamy N, Zimmerman HM. Amyotrophic lateral sclerosis. Acomparison of Guam and classical cases. Arch Neurol 1967;16(4):357–63.
66. Hirano A, Nakano I, Kurland LT, et al. Fine structural study of neurofibrillarychanges in a family with amyotrophic lateral sclerosis. J Neuropathol Exp Neurol1984;43(5):471–80.
67. Rothstein JD. Current hypotheses for the underlying biology of amyotrophiclateral sclerosis. Ann Neurol 2009;65(Suppl 1):S3–9.
68. Bosco DA, Morfini G, Karabacak NM, et al. Wild-type and mutant SOD1 sharean aberrant conformation and a common pathogenic pathway in ALS. Nat Neu-rosci 2010;13(11):1396–403.
69. Kabashi E, Valdmanis PN, Dion P, et al. TARDBP mutations in individuals withsporadic and familial amyotrophic lateral sclerosis. Nat Genet 2008;40(5):572–4.
70. Neumann M, Sampathu DM, Kwong LK, et al. Ubiquitinated TDP-43 in fronto-temporal lobar degeneration and amyotrophic lateral sclerosis. Science 2006;314(5796):130–3.
71. Mackenzie IR, Bigio EH, Ince PG, et al. Pathological TDP-43 distinguishessporadic amyotrophic lateral sclerosis from amyotrophic lateral sclerosis withSOD1 mutations. Ann Neurol 2007;61(5):427–34.
72. Burghes AH, Beattie CE. Spinal muscular atrophy: why do low levels of survivalmotor neuron protein make motor neurons sick? Nature reviews. Neuroscience2009;10(8):597–609.
73. Doyu M, Sobue G, Mukai E, et al. Severity of X-linked recessive bulbospinal neu-ronopathy correlates with size of the tandem CAG repeat in androgen receptorgene. Ann Neurol 1992;32(5):707–10.
74. Li M, Miwa S, Kobayashi Y, et al. Nuclear inclusions of the androgen receptorprotein in spinal and bulbar muscular atrophy. Ann Neurol 1998;44(2):249–54.
75. Andersen PM, Abrahams S, Borasio GD, et al. EFNS guidelines on the clinicalmanagement of amyotrophic lateral sclerosis (MALS)–revised report of anEFNS task force. Eur J Neurol 2012;19(3):360–75.
76. Miller RG, Jackson CE, Kasarskis EJ, et al. Practice parameter update: the careof the patient with amyotrophic lateral sclerosis: drug, nutritional, and respira-tory therapies (an evidence-based review): report of the quality standardssubcommittee of the American Academy of Neurology. Neurology 2009;73(15):1218–26.

Rezania & Roos238
77. Rezania K, Goldenberg FD, White S. Neuromuscular disorders and acute respi-ratory failure: diagnosis and management. Neurol Clin 2012;30(1):161–85, viii.
78. Miller RG, Jackson CE, Kasarskis EJ, et al. Practice parameter update: the careof the patient with amyotrophic lateral sclerosis: multidisciplinary care, symptommanagement, and cognitive/behavioral impairment (an evidence-basedreview): report of the Quality Standards Subcommittee of the AmericanAcademy of Neurology. Neurology 2009;73(15):1227–33.
79. Scherer K, Bedlack RS. Diaphragm pacing in amyotrophic lateral sclerosis:a literature review. Muscle Nerve 2012;46(1):1–8.
80. Gowing G, Svendsen CN. Stem cell transplantation for motor neuron disease:current approaches and future perspectives. Neurotherapeutics 2011;8(4):591–606.
81. Muntoni F, Wood MJ. Targeting RNA to treat neuromuscular disease. Nat RevDrug Discov 2011;10(8):621–37.
82. Van Meerbeke JP, Sumner CJ. Progress and promise: the current status ofspinal muscular atrophy therapeutics. Discov Med 2011;12(65):291–305.
83. Brooks BR, Miller RG, Swash M, et al. El Escorial revisited: revised criteria for thediagnosis of amyotrophic lateral sclerosis. Amyotroph Lateral Scler Other MotorNeuron Disord 2000;1(5):293–9.
84. de Carvalho M, Dengler R, Eisen A, et al. Electrodiagnostic criteria for diagnosisof ALS. Clin Neurophysiol 2008;119(3):497–503.
85. Poll-The BT, Engelen M. Peroxisomal leukoencephalopathy. Semin Neurol 2012;32(1):42–50.
86. Roos R, Gajdusek DC, Gibbs CJ Jr. The clinical characteristics of transmissibleCreutzfeldt-Jakob disease. Brain 1973;96(1):1–20.
87. Kovanen J. Clinical characteristics of familial and sporadic Creutzfeldt-Jakobdisease in Finland. Acta Neurol Scand 1993;87(6):469–74.
88. Worrall BB, Rowland LP, Chin SS, et al. Amyotrophy in prion diseases. Arch Neu-rol 2000;57(1):33–8.
89. Schule R, Schols L. Genetics of hereditary spastic paraplegias. Semin Neurol2011;31(5):484–93.
90. Moses SW, Parvari R. The variable presentations of glycogen storage diseasetype IV: a review of clinical, enzymatic and molecular studies. Curr Mol Med2002;2(2):177–88.
91. Ooi MH, Wong SC, Lewthwaite P, et al. Clinical features, diagnosis, andmanagement of enterovirus 71. Lancet Neurol 2010;9(11):1097–105.
92. Mitsumoto H, Sliman RJ, Schafer IA, et al. Motor neuron disease and adulthexosaminidase A deficiency in two families: evidence for multisystem degener-ation. Ann Neurol 1985;17(4):378–85.
93. Neumann M, Kwong LK, Sampathu DM, et al. TDP-43 proteinopathy in fronto-temporal lobar degeneration and amyotrophic lateral sclerosis: protein misfold-ing diseases without amyloidosis. Arch Neurol 2007;64(10):1388–94.
94. Deng HX, Chen W, Hong ST, et al. Mutations in UBQLN2 cause dominantX-linked juvenile and adult-onset ALS and ALS/dementia. Nature 2011;477(7363):211–5.
95. Tomonaga M, Saito M, Yoshimura M, et al. Ultrastructure of the Bunina bodies inanterior horn cells of amyotrophic lateral sclerosis. Acta Neuropathol 1978;42(2):81–6.
96. Vande Velde C, Miller TM, Cashman NR, et al. Selective association of misfoldedALS-linked mutant SOD1 with the cytoplasmic face of mitochondria. Proc NatlAcad Sci U S A 2008;105(10):4022–7.

Motor Neuron Diseases 239
97. Cassina P, Cassina A, Pehar M, et al. Mitochondrial dysfunction in SOD1G93A-bearing astrocytes promotes motor neuron degeneration: prevention bymitochondrial-targeted antioxidants. J Neurosci 2008;28(16):4115–22.
98. Borchelt DR, Wong PC, Becher MW, et al. Axonal transport of mutant superoxidedismutase 1 and focal axonal abnormalities in the proximal axons of transgenicmice. Neurobiol Dis 1998;5(1):27–35.
99. Kikuchi H, Almer G, Yamashita S, et al. Spinal cord endoplasmic reticulumstress associated with a microsomal accumulation of mutant superoxidedismutase-1 in an ALS model. Proc Natl Acad Sci U S A 2006;103(15):6025–30.
100. Nishitoh H, Kadowaki H, Nagai A, et al. ALS-linked mutant SOD1 induces ERstress- and ASK1-dependent motor neuron death by targeting Derlin-1. GenesDev 2008;22(11):1451–64.
101. Harraz MM, Marden JJ, Zhou W, et al. SOD1 mutations disrupt redox-sensitiveRac regulation of NADPH oxidase in a familial ALS model. J Clin Invest 2008;118(2):659–70.
102. Wojciechowska M, Krzyzosiak WJ. Cellular toxicity of expanded RNA repeats:focus on RNA foci. Hum Mol Genet 2011;20(19):3811–21.
103. Todd PK, Paulson HL. RNA-mediated neurodegeneration in repeat expansiondisorders. Ann Neurol 2010;67(3):291–300.
104. Mackenzie IR, Rademakers R, Neumann M. TDP-43 and FUS in amyotrophiclateral sclerosis and frontotemporal dementia. Lancet Neurol 2010;9(10):995–1007.
105. Banno H, Adachi H, Katsuno M, et al. Mutant androgen receptor accumulationin spinal and bulbar muscular atrophy scrotal skin: a pathogenic marker. AnnNeurol 2006;59(3):520–6.