Embed Size (px)
Citation preview
SPINAL
CORD
INJURIES
David Garvey, PhD, MD, FACEP
International Trauma Conference 2016
SCI Spinal Cord Injuries
DISCLOSURE
I have no actual or potential
conflict of interest in relation
to this program/presentation.
SCI Spinal Cord Injuries
OUTLINE
Statistics
Anatomy
Traumatic Causes
Pathophysiology
What’s What?
Backboards and
Collars
SCI Statistics
12-20K SCIs per year
Societal cost is astronomical
Males ages 15-35 account for >50%
Male to female ratio is approx. 4:1
>10% occur in patients over age 60
<10% occur in patients under age 15
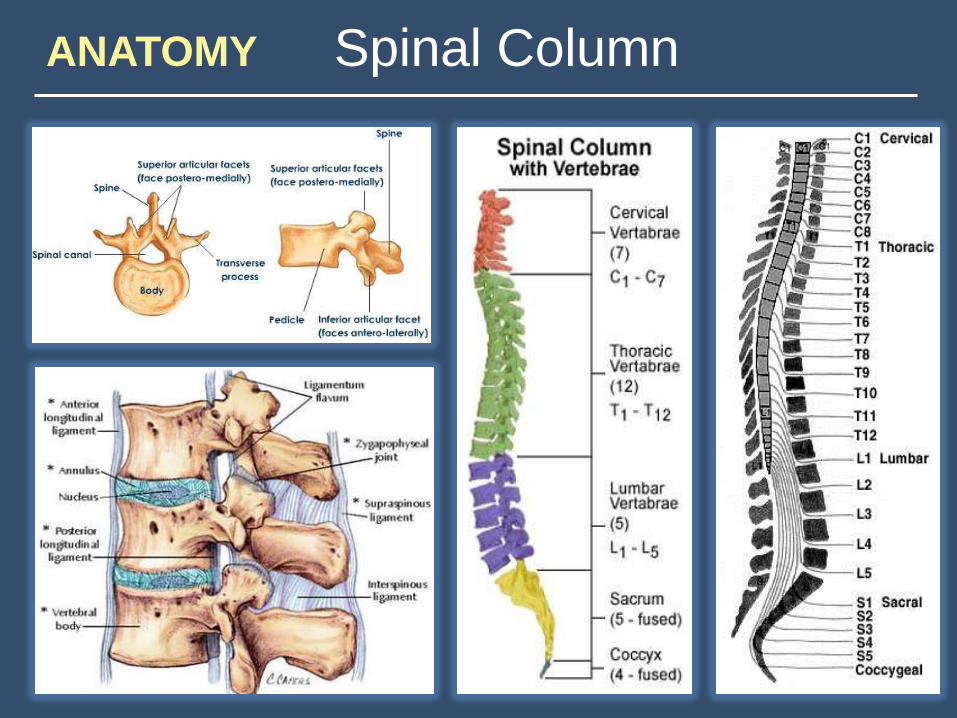
ANATOMY Spinal Column
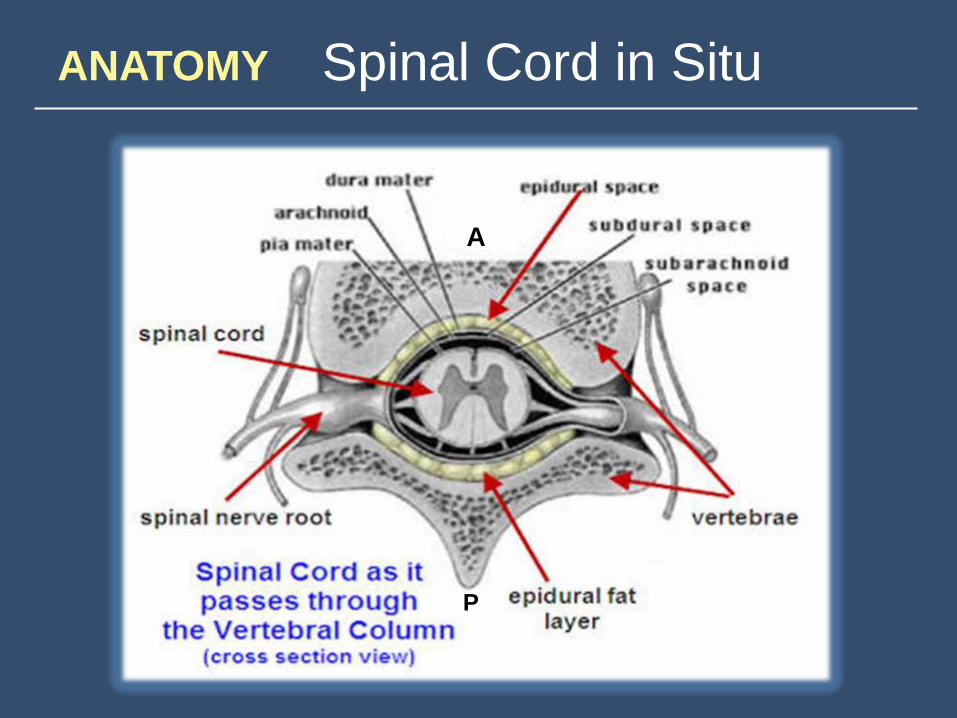
ANATOMY Spinal Cord in Situ
A
P

ANATOMY Spinal Cord
Dorsal (Posterior)
Ventral (Anterior)
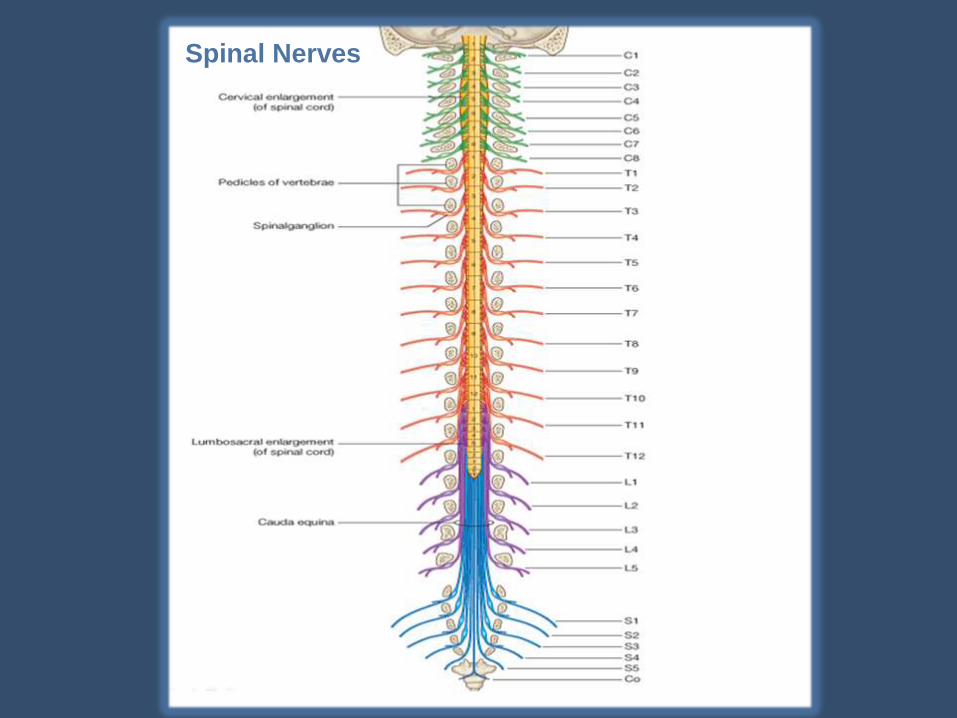
Spinal Nerves
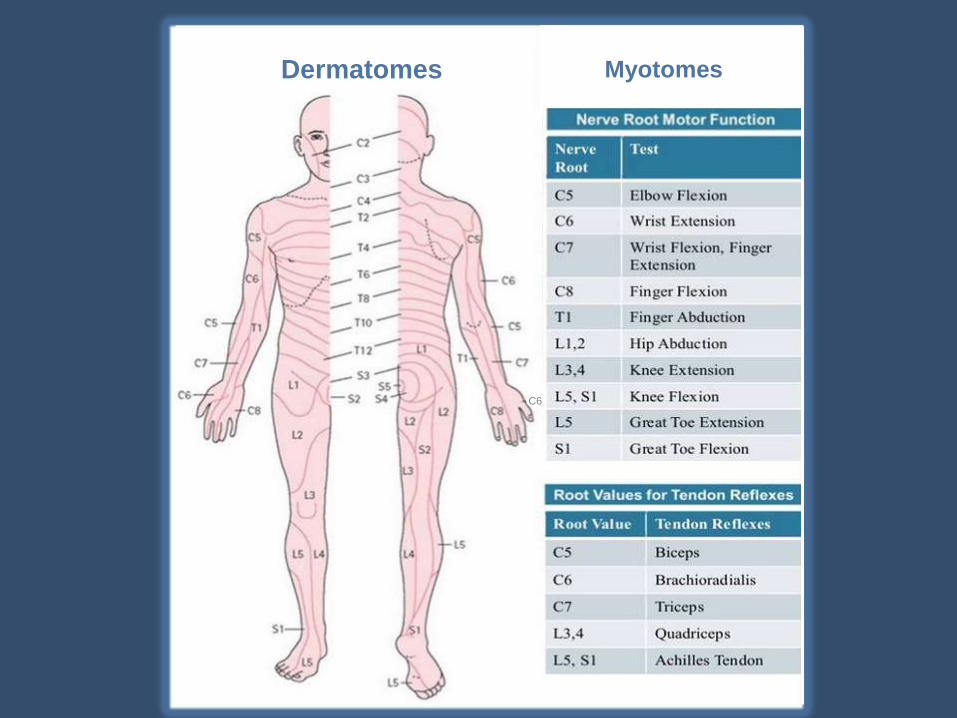
Dermatomes Myotomes
C6
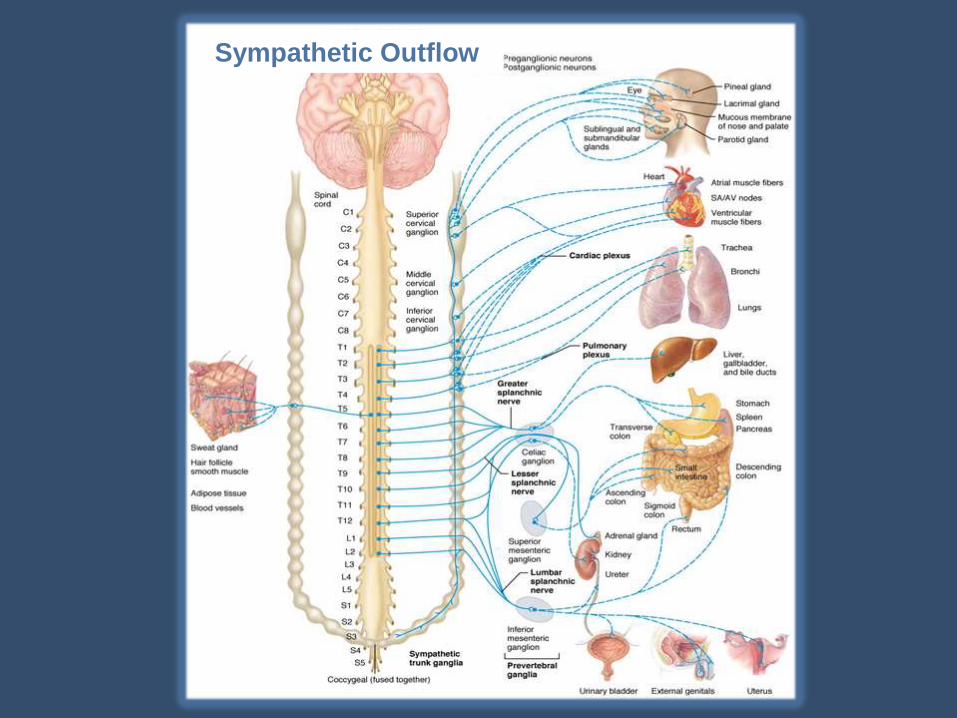
Sympathetic Outflow
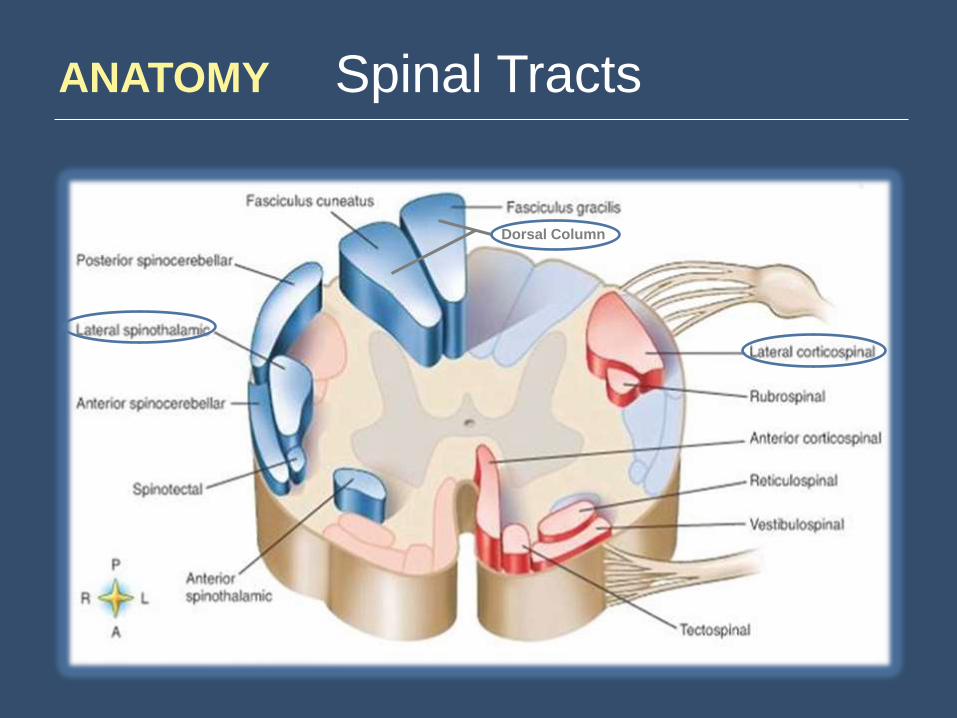
ANATOMY Spinal Tracts
Dorsal Column
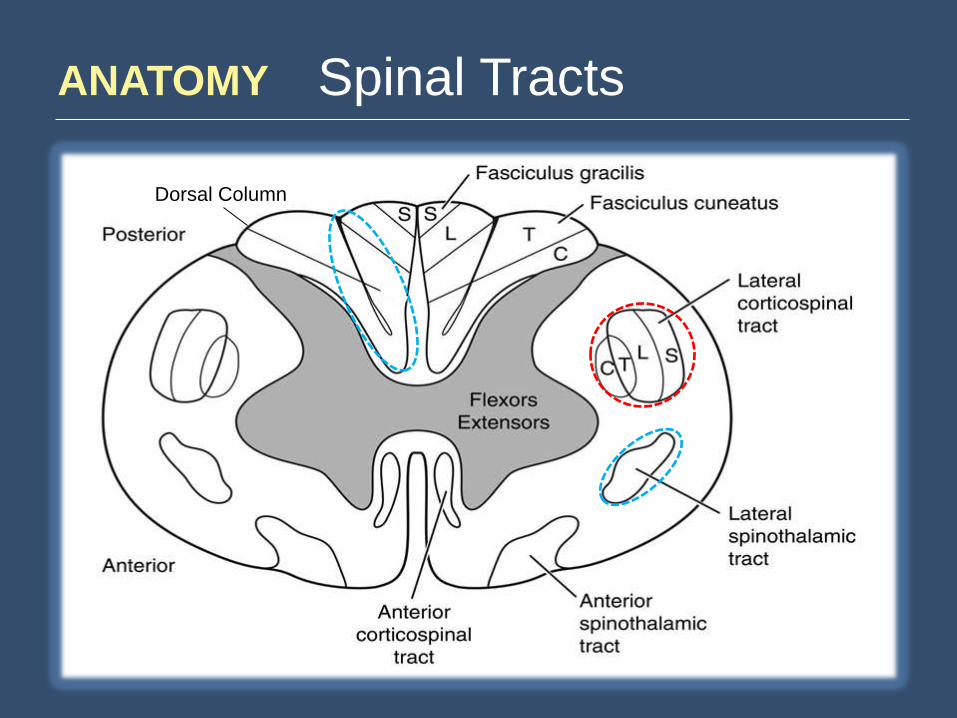
ANATOMY Spinal Tracts
Dorsal Column
SCI Traumatic Causes
MVCs – 40-50%
Falls / Work-Related – 30%
Violent Crimes – 15%
Sports-Related – 10%
• Hyperextension
• Hyperflexion
• Compression
• Rotation
• Lateral Stress
• Distraction
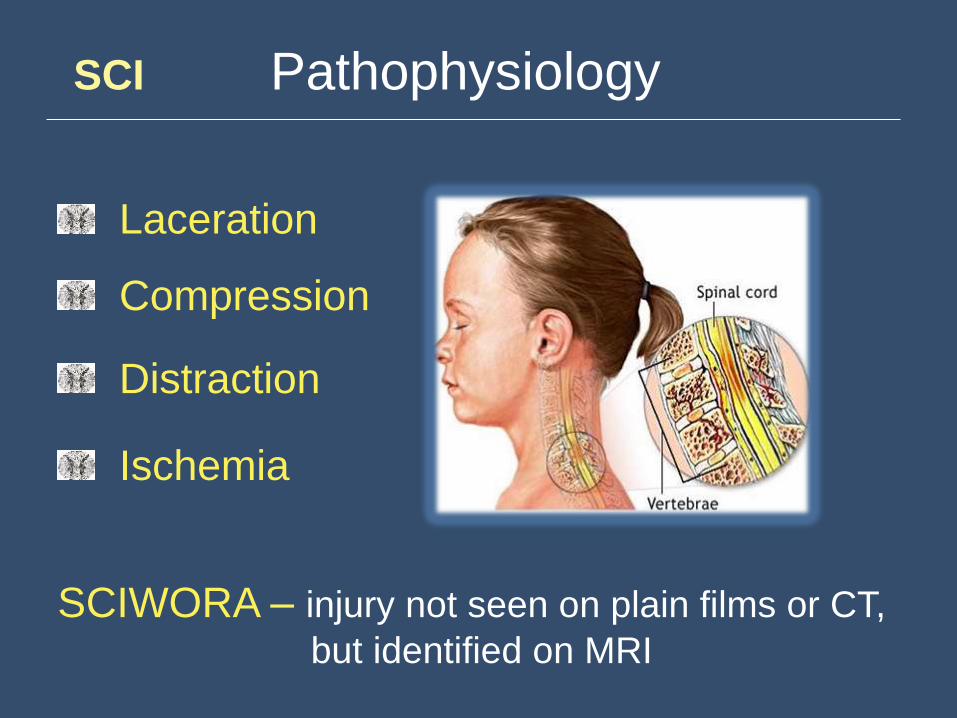
SCI Pathophysiology
Laceration
Compression
Distraction
Ischemia
SCIWORA – injury not seen on plain films or CT,
but identified on MRI
What’s What ?
Stable versus Unstable Spinal Injuries
Complete versus Incomplete Cord Injuries
Neurogenic versus Spinal Shock
Safe / “Cleared” versus Unsafe Spine
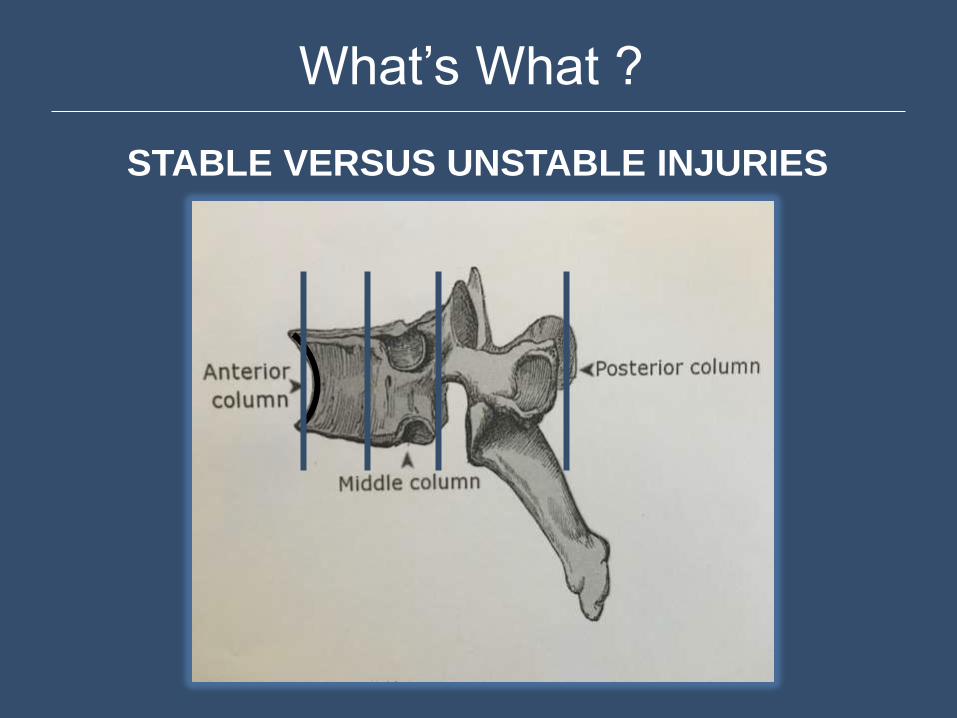
What’s What ?
STABLE VERSUS UNSTABLE INJURIES
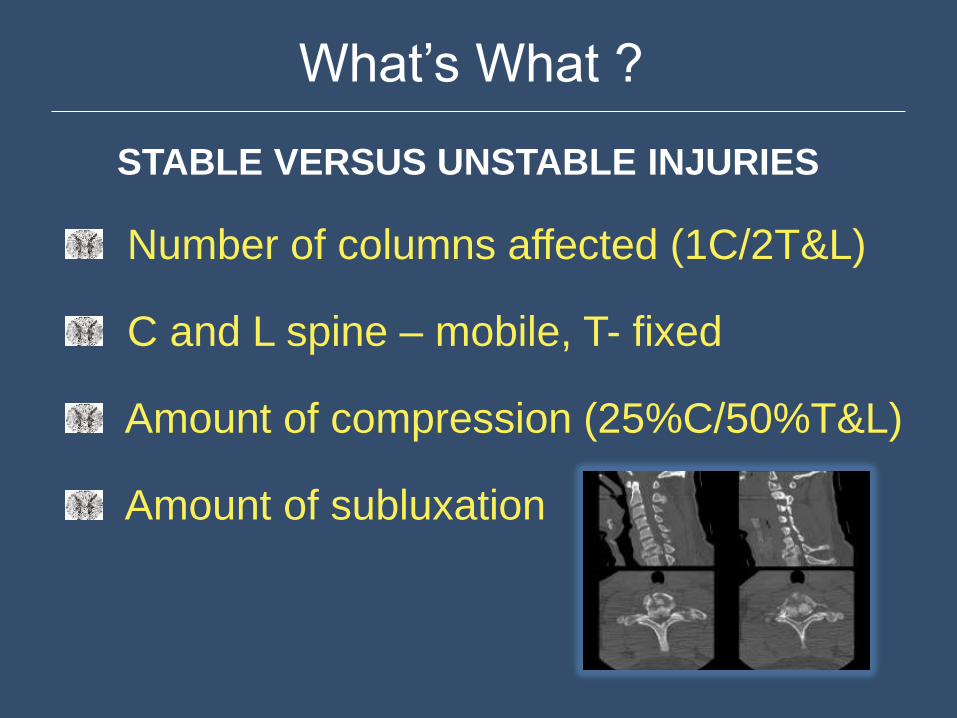
What’s What ?
STABLE VERSUS UNSTABLE INJURIES
Number of columns affected (1C/2T&L)
C and L spine – mobile, T- fixed
Amount of compression (25%C/50%T&L)
Amount of subluxation
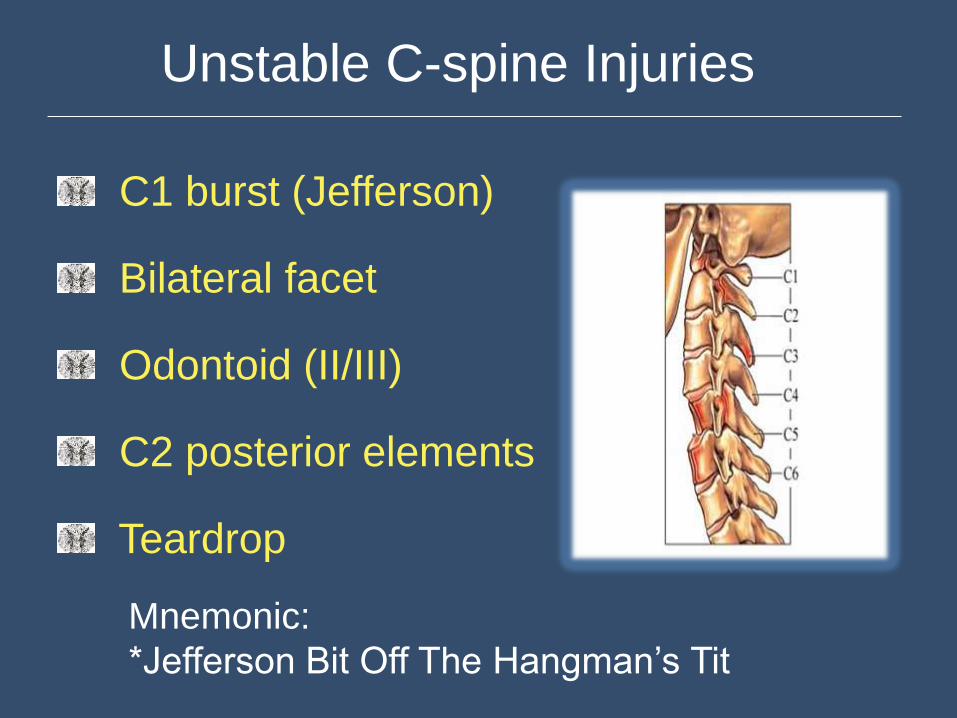
Unstable C-spine Injuries
C1 burst (Jefferson)
Bilateral facet
Odontoid (II/III)
C2 posterior elements
Teardrop
Mnemonic:
*Jefferson Bit Off The Hangman’s Tit
What’s What ?
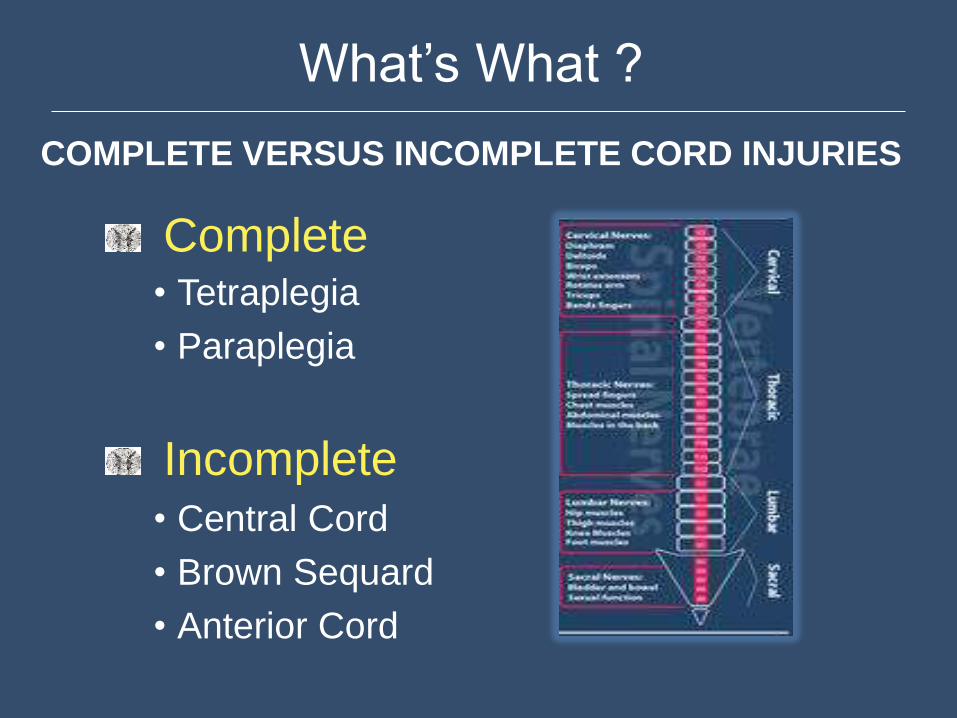
COMPLETE VERSUS INCOMPLETE CORD INJURIES
Complete • Tetraplegia
• Paraplegia
Incomplete • Central Cord
• Brown Sequard
• Anterior Cord
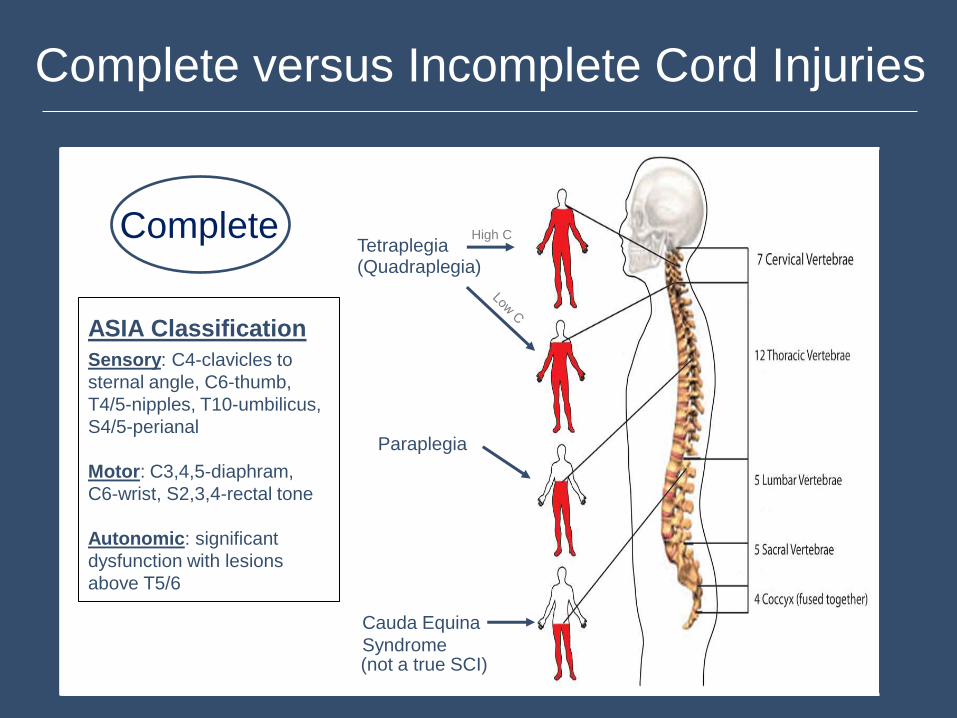
Complete versus Incomplete Cord Injuries
Tetraplegia
Tetraplegia (Quadraplegia)
Paraplegia
Cauda Equina
Syndrome
ASIA Classification
Sensory: C4-clavicles to
sternal angle, C6-thumb,
T4/5-nipples, T10-umbilicus,
S4/5-perianal
Motor: C3,4,5-diaphram,
C6-wrist, S2,3,4-rectal tone
Autonomic: significant
dysfunction with lesions
above T5/6
Complete
(not a true SCI)
High C
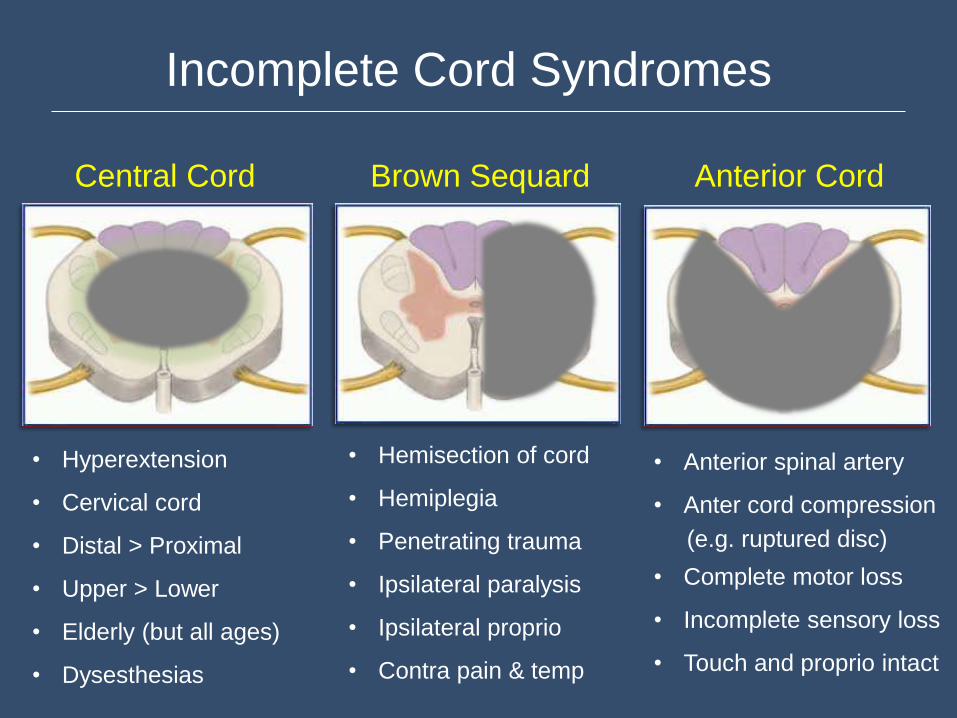
Incomplete Cord Syndromes
Central Cord Brown Sequard Anterior Cord
• Hyperextension
• Cervical cord
• Distal > Proximal
• Upper > Lower
• Elderly (but all ages)
• Dysesthesias
• Hemisection of cord
• Hemiplegia
• Penetrating trauma
• Ipsilateral paralysis
• Ipsilateral proprio
• Contra pain & temp
• Anterior spinal artery
• Anter cord compression
(e.g. ruptured disc)
• Complete motor loss
• Incomplete sensory loss
• Touch and proprio intact
What’s What ?
NEUROGENIC VERSUS SPINAL SHOCK
Neurogenic Shock • Vasodilation • Bradycardia • Hypotension
Spinal Shock
• Temporary loss of all neurological activity
below the level of the cord injury, includes
reflexes (e.g. bulbocavernosus reflex)
What’s What ?
SAFE “CLEARED” VERSUS UNSAFE C-SPINE
Initial Assessment • ABCDE
• D (Neuro) - LOC (AVPU/GCS), Motor
• Question - “Any numbness/weakness?”
* ANY NEUROLOGIC COMPLAINT must raise suspicion for SCI
(e.g. paresthesias, dysesthesias, weakness, numbness, etc.)
with or without physical findings, even if transitory
How do we assess the C-spine? • Spine Assessment Protocol
C-Spine Rules
NEXUS (Low Risk Criteria)
• No Midline Tenderness
• No Altered Mental Status or Intoxication
• No Neurological Deficits (Signs or Symptoms)
• No Distracting Injuries
CCR (High Risk)
• Age > 65
• Dangerous Mechanism*
• Paresthesias in the Extremities
CCR Dangerous Mechanism
Fall from height >3 ft or 5 stairs
Axial load to head (e.g. diving)
High speed MVC (>60 mph), rollover
or ejection
Collision involving an ATV or bicycle
Hit (rear-ended) by a bus, truck or high-
speed vehicle or pushed into oncoming
traffic
SCI Prehospital / ED Treatment
Immobilization (C-collar / Backboard)
Oxygenation / Ventilation
Fluids / Pressors
Steroids
Hypothermia
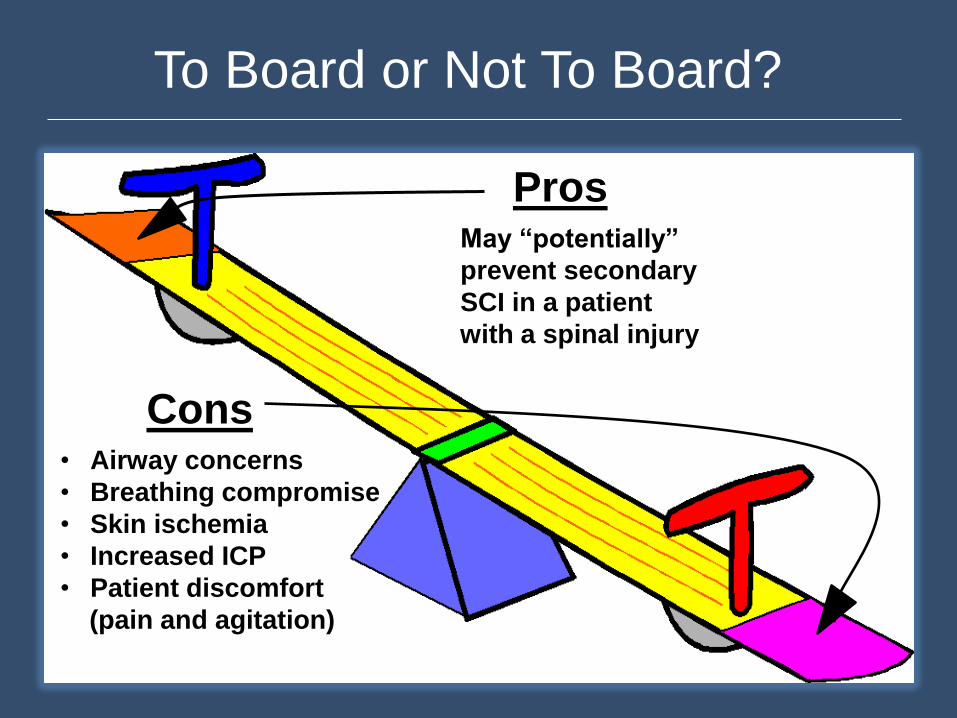
To Board or Not To Board?
Cons
Pros
• Airway concerns
• Breathing compromise
• Skin ischemia
• Increased ICP
• Patient discomfort
(pain and agitation)
May “potentially”
prevent secondary
SCI in a patient
with a spinal injury
QUESTIONS? _________________________
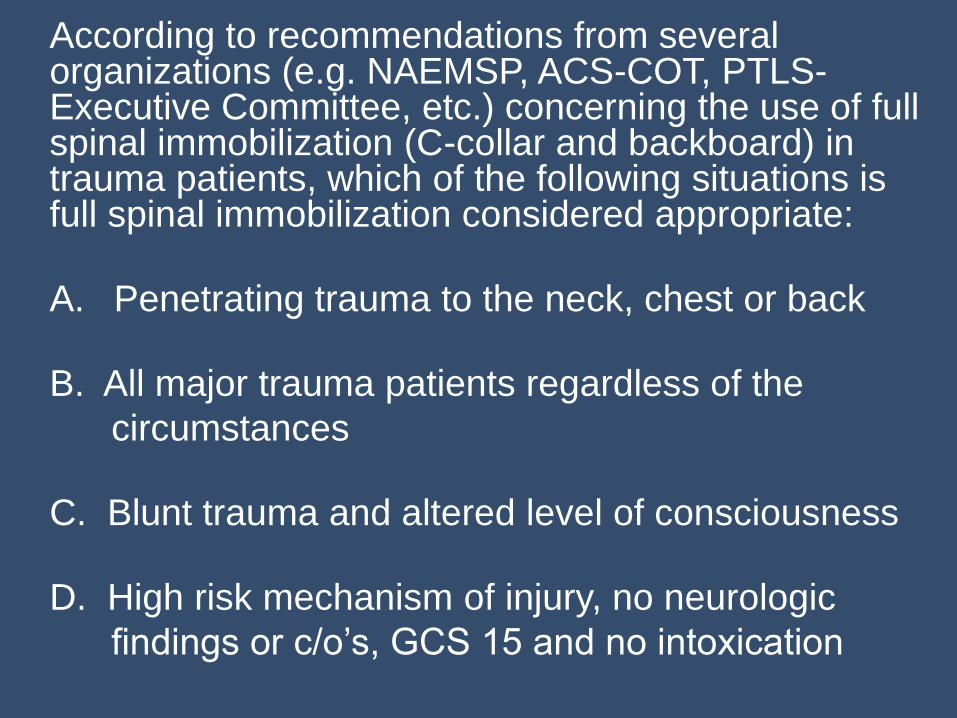
According to recommendations from several organizations (e.g. NAEMSP, ACS-COT, PTLS-Executive Committee, etc.) concerning the use of full spinal immobilization (C-collar and backboard) in trauma patients, which of the following situations is full spinal immobilization considered appropriate:
A. Penetrating trauma to the neck, chest or back
B. All major trauma patients regardless of the
circumstances
C. Blunt trauma and altered level of consciousness
D. High risk mechanism of injury, no neurologic
findings or c/o’s, GCS 15 and no intoxication