Embed Size (px)
DESCRIPTION
In conjunction with the 2016 Seattle Study Club Symposium.
Citation preview

1
3PREVENTING HEART ATTACKS, STROKES AND DIABETESKNOWLEDGE IS POWER— WHAT WOMEN NEED TO KNOW ABOUT CARDIOVASCULAR HEALTHDr. Amy L. Doneen
23AN INCREDIBLE FIX FOR LOWER BACK PAINMr. Brian Bradley (Ergonomic Instruction)
35A HOPELESS TOOTH IS NOT A USELESS TOOTHDr. Marco A. Brindis
47INFLAMMATORY PERI-IMPLANT DISEASEDr. Paul Fletcher
55SOFT TISSUE MANAGEMENT OF AESTHETIC FAILUREProf. Giovanni Zucchelli
2016 Seattle Study Club ® SymposiumSPEAKER ARTICLES &
RECOMMENDED READING

2

3
PREVENTING HEART ATTACKS, STROKES AND DIABETES
KNOWLEDGE IS POWER— WHAT WOMEN NEED TO KNOW
ABOUT CARDIOVASCULAR HEALTH
Dr. Amy L. Doneen

4
Journal of Cardiovascular NursingVol. 00, No. 0, pp 00Y00 x Copyright B 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins
8-Year Outcomes of a Program for EarlyPrevention of Cardiovascular EventsA Growth-Curve Analysis
Du Feng, PhD; M. Christina Esperat, PhD, RN, FAAN; Amy L. Doneen, RN, BSN, MSN, ARNP;Bradley Bale, MD; Huaxin Song, PhD; Alexia E. Green, PhD, RN, FAAN
Background: Early identification of cardiovascular diseases allows us to prevent the progression of these diseases.
The Bale/Doneen Method, a prevention and treatment program for heart attacks and ischemic strokes, has been
adopted nationally in primary care and specialty clinics. Objectives: The main purpose of this study was to
evaluate the effect of the Bale/Doneen Method on lipoproteins and carotid intima-media thickness (IMT) for
cardiovascular disease prevention and reduction. A secondary purpose was to illustrate the use of latent
growth-curve analysis in studying trajectories of clinical outcomes and biomarkers in individual patients over time.
Method: This retrospective analysis is based on 576 patients at a nurse-managed ambulatory clinic who received
the heart attack prevention and treatment program from 2000 to 2008. All patients were white; 61% were
men; mean age was 55.5 years. Outcome measures include hemoglobin A1c, fasting blood sugar, plaque
burden score (PBS), high-density lipoprotein, low-density lipoprotein (LDL), mean carotid artery IMT, and
lipoprotein-associated phospholipase A2 test results. Latent growth-curve analysis was used in modeling changes
in these outcome measures. Results: On average, mean IMT score decreased by 0.01 per year (P G .001), PBS
decreased by 0.17 per year (P G .001), LDL decreased by 5.19 per year (P G .001), and lipoprotein-associated
phospholipase A2 decreased by 3.6 per year (P G .05). Hemoglobin A1c increased by 0.04 per year (P G .001).
Significant sex and age differences in the initial level and/or rate of change of mean IMT, PBS, fasting blood sugar,
high-density lipoprotein, and LDL scores were found. Discussion: The current findings suggest that the Bale/Doneen
Method is effective in generating a positive effect on the atherosclerotic disease process by achieving regression
of disease in the carotid arteries.
KEY WORDS: cardiovascular disease, early prevention, treatment program
Cardiovascular diseases (CVDs) are the leadingcause of mortality in developed countries. Ath-
erogenesis and, subsequently, atherosclerosis are car-diovascular (CV) processes that lead to most of thesemortalities.1 Two leading factors that are thought tofacilitate progression are oxidative stress and inflam-mation2; both are important in the pathogenesis ofatherosclerotic changes.3Y5 Prevention of progressionof these processes is at the center of the managementof CVD. A hallmark in prevention is identification ofbiomarkers (eg, hemoglobin A1c [HgbA1C], low-densitylipoprotein [LDL], plaque burden score [PBS], andintima-media thickness [IMT]) early in disease6 so thatcomprehensive and intensive management may be in-stituted to ameliorate the progression of the process.
Metabolic syndrome is a prominent factor leadingto the alarming increase in the incidence of chronicdisease in the US population. This factor is among themost predominant precursors of the onset of CVD andtherefore merits focus in the prevention efforts to con-trol and prevent these chronic conditions. Another prom-inent factor, obesity, is thought to involve inflammatory
1
Du Feng, PhDProfessor, School of Nursing, University of Nevada, Las Vegas.
M. Christina Esperat, PhD, RN, FAANProfessor,School of Nursing, Texas Tech University Health ScienceCenter, Lubbock.
Amy L. Doneen, RN, BSN, MSN, ARNPAdjunct Professor, Texas Tech Health Science Center, School ofNursing, and Cofounder and Medical Director, the Heart Attack& Stroke Prevention Center, Spokane, Washington.
Bradley Bale, MDAdjunct Professor, Texas Tech Health Science Center, School ofNursing, and Medical Director, the Heart Health Program for GraceClinic, Lubbock, Texas.
Huaxin Song, PhDLead Analyst, School of Nursing, Texas Tech University Health ScienceCenter, Lubbock.
Alexia E. Green, PhD, RN, FAANProfessor,School of Nursing, Texas Tech University Health ScienceCenter, Lubbock.
This work was supported by School of Nursing, Texas Tech UniversityHealth Science Center.
The authors have no conflicts of interest to disclose.
CorrespondenceDu Feng, PhD, School of Nursing, University of Nevada, Las Vegas4505 S Maryland Parkway, Box 453018 Las Vegas, NV 89154-3018([email protected]).
DOI: 10.1097/JCN.0000000000000141
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

5
processes and oxidative stress.7 In a study of the as-sociation between inflammatory markers and insulinresistance (IR) carried out in an elderly population, pos-sible determinants of the homeostasis model assessmentindex, including four inflammatory markers (leukocytecount, erythrocyte sedimentation rate, high-sensitivityC-reactive protein, and C3 complement the 5 elementsof the metabolic syndrome, total cholesterol, physicalactivity, as well as 4 indicators of adiposity (body massindex, waist circumference, percentage body fat, andhepatic steatosis) were studied.8 Of the 4 inflammatorymarkers simultaneously assessed in the subjects, onlyserum complement C3was significantly associated withIR.8 It is imperative that more investigations be con-ducted to support the use of biomarkers of oxidativestress and inflammatory processes in the refinement ofthe classification of disease progress and to personalizethe treatment approaches to the individual.
Various definitions of metabolic syndrome exist inthe literature. In the current study, we used the USNational Cholesterol Education Program (NCEP) def-inition, which requires at least 3 of 5 of the followingcriteria: (1) central obesity, waist circumference equalto or greater than 102 cm or 40 in for men and equal toor greater than 88 cm or 35 in for women; (2) dyslip-idemia, triglyceride (TG) level 1.7 mmol/L (150mg/dL)or greater; (3) dyslipidemia, high-density lipoprotein-cholesterol (HDL-C) level less than 40 mg/dL for menand less than 50 mg/dL for women; (4) blood pressure(BP) 130/85 mm Hg or greater (or treated for hyperten-sion); and (5) fasting plasma glucose level 6.1 mmol/L(110 mg/dL) or greater.9
Early Identification and Prevention ofCardiovascular Disease
Another hallmark in the prevention of CVD is the earlyidentification of the presence and progress of athero-genesis and arteriosclerosis among high-risk individuals.An important step in the diagnosis andmanagement ofindividuals with risk factors for CVD is the classifica-tion of people into risk categories. Currently, in office-based practice, use of algorithms of conventional riskfactors is standard practice. In the adult populationwithin the United States, it is estimated that fully two-thirds are classified as intermediate risk based on thesealgorithms.10 These individuals have to be managedaggressively to prevent the progression of the athero-genic process. The issue of adequately managing theseindividuals is fraught with challenges. Cardiovasculardisease remains the number 1 cause of mortality in theUnited States. Cerebral vascular disease remains thenumber 1 cause of disability. Many individuals expe-rience a CV event without any previous knowledge ofbeing high risk. It is very important that early diseaseprocesses be identified if these challenges are to be over-
come and that the approach to prevention of progressof the disease be appropriately individualized.
State of the science technology in the diagnosis ofCVD has progressed to the point that test modalitiesfor assessment of arterial function and structure inasymptomatic subjects are possible. Vascular ultraso-nography and tonometry are some of the most prom-ising among these modalities.6 Measurement of IMTwith B-mode ultrasonography scans in the carotid ar-teries can now determine the presence of atheroscleroticprocess in the vascular structure.11,12 This diagnostictool has the clear advantage of being a noninvasiveprocedure that could be conducted repeatedly or fre-quently. The establishment of quality control in theperformance of the test and the standardization of theprocedures for measurementmay enable the integrationof this diagnostic procedure into clinical practice, inaddition to existing CV risk stratification algorithms.10
The Prevention Program: TheBale/Doneen Method
The Bale/DoneenMethod was developed by Dr BradleyBale and Amy Doneen, ARNP, for the prevention andtreatment of heart attacks and ischemic strokes in allprimary and secondary prevention patients. This methodis now being integrated nationally into primary careclinics and specialty clinics around the country. Com-ponents of this prevention/treatment program aregrounded in a disease treatment paradigm and includeaggressive management of CV risk factors and clini-cal outcomes (eg, heart attack, stroke, and diabetesmellitus) through evaluation, medication, and lifestylemanagement. All of the medications used are Foodand Drug Administration approved. All of the lifestyleadvice is guided by nutrigenomics, prescribed by thehealthcare provider, which incorporates informationon individual genetics and specific needs for certainnutrients.13,14
Lifestyle is emphasized as the number 1way to reduceCV risk. Patients were educated on the importance ofarterial inflammation as the reason arterial disease de-velops and as the trigger plaque for heart attacks andstrokes. They were taught the numerous modifiable is-sues that can generate arterial disease and how tomanagethose issues to mitigate riskVnumerous lifestyle modifi-cations that can have a positive influence on arterialinflammation. These included instructions on physicalactivity, proper diet, adequate sleep, anxietymanagement,weight control, nicotine cessation, and oral health. Thus,patients were coached about the importance of mitigat-ing inflammation via proper lifestyle. The importance ofexercise to enhance insulin sensitivity and avoid migrat-ing on to type 2 diabetes was discussed with most ofthe patients. Daily exercise was encouraged with a mix-ture of aerobic and resistive training. Dietary advicewas
2 Journal of Cardiovascular Nursing x Month 2014
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

6
given with the guidance of the apolipoprotein E (apoE)genotype.15 In general, apoE 2’s were advised to limitcarbohydrates and apoE 4’s were told to limit fat in-take. All patients were educated about the benefit ofdiets rich in fruits, vegetables, nuts, seeds, and fish. Pa-tients were advised to limit their intake of red meat.Alcohol guidance was very individualized. ApoE 4 in-dividuals were told to avoid alcohol. Women who wereapoE 2 or 3 were warned of the increased cancer riskof alcohol consumption. Alcohol was not presented asan essential element to reduce CV risk. Patients wereinstructed to take advantage of free phone consultationwith Berkeley HeartLab dieticians.
The Bale/Doneen Method is a method of deliveringevidence- and outcome-based medical care using a sys-tem anchored in the disease of atherosclerosis ratherthan the standard practice of delivering preventativecare based solely on risk factors. All decisions for as-sessment and treatment are based on the presence ofatherosclerosis and the subsequent impact on the ath-erosclerotic process in this model of primary and sec-ondary CVD prevention/treatment. Table 1 shows the6 basic elements to the method, which hinge on pa-tient education.
It should be noted that the Bale/Doneen Methodallows for a very personalized approach to maintainhealth and wellness. The healthcare providers are ableto tailor their management for individual patients basedon their most unique characteristics.
Purpose of the Current Study
The main purpose of current study was to evaluate theeffect of a prevention/treatment program on lipopro-teins, carotid IMT (cIMT), and lipoprotein-associatedphospholipase A2 (Lp-PLA2) for CVD reduction in
patients recruited from a nurse-managed ambulatoryclinic in Northwestern United States that specializesin heart attack prevention and intervention. Componentsof this early prevention program include aggressive man-agement of CV risk factors and clinical outcomes (eg,heart attack, stroke, and diabetes mellitus) through eval-uation, medication, and lifestyle management. All of themedications used are Food and Drug Administrationapproved. All of the lifestyle advice is common andcould be prescribed by any healthcare provider.
A secondary purpose was to illustrate the use oflatent growth-curve analysis (GCA), as well as its ad-vantages, in studying trajectories of clinical outcomesand biomarkers in individual patients over time. Thismultilevel statistical method can appropriately evaluateintraindividual change by modeling individual trajecto-ries of outcomes, capture interindividual variability inchange over time, and examine factors that explain theinterindividual differences in growth trajectories. Al-though not used often in nursing research, multilevelgrowth-curve modeling techniques have become com-monly used approaches to the study of change over timein epidemiology and social behavioral fields. The ad-vantages of GCA over the traditional repeated-measuresanalysis of variance in analyzing longitudinal datahave been well documented.16Y19 This article is, to theauthors’ knowledge, 1 of the few to examine the useof GCA in studying changes in CV patients over a clin-ical trajectory. As more and more nursing researchersuse longitudinal designs to study the clinical outcomesof CVD treatment and prevention, the availability oflongitudinal data will create a shift toward the use ofnewer statistical models, such as the GCA, to the studyof change over time. This statistical method can be ofparticular interest to nursing from a clinical point ofview, as well as a way to test theoretical models.
TABLE 1 Components of the Bale/Doneen Method
Components Description
1. Education Each patient is educated about the disease state of atherosclerosis and understands how myocardial infarctionsand ischemic strokes occur.
2. Disease Each patient is evaluated for the presence of atherosclerosis, using noninvasive office-based techniques, to findasymptomatic vascular disease, and is monitored annually with an intima-media thickness (IMT) test to follow theindividual trajectory of atherosclerotic disease. In addition, all patients are monitored annually with a carotidIMT test to follow the atherosclerotic disease over time in the individual patient.
3. Inflammation Biomarkers are used to routinely determine the inflammatory state of the vascular system. Endothelial markers includehs-C-reactive protein, microalbumen/creatinine urine ratio, and fibrinogen. Lipoprotein-associated phospholipaseA2 is evaluated for intima activity. Patients were instructed to have these assessed at least biannually.
4. Root causes The root cause or causes of the atherosclerotic process are determined and managed for each patient. Rootcauses of atherosclerosis can include insulin resistance, lipo(a), familial hyperlipidemia, potentiallymyeloperoxidase, and vitamin D deficiency.51 Appropriate follow-up testing for effective management of aroot cause was done on average quarterly to semiannually.
5. Optimal goals Goals of therapy are set based on peer-reviewed, reliable research and guidelines, with optimal targets in anattempt to minimize risk and often going beyond the values set for the standard of care. Attainment of goalswas evaluated, on average, every 3Y6 months.
6. Genetics Genetic information is obtained on patients to aid in the assessment of their cardiovascular risk and to help guidetherapy. These tests were never repeated. Their clinical utility never expires, unlike other biomarkers. This makesthem arguably the least expensive tests performed.
Program for Early Prevention of Cardiovascular Events 3
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

7
Methods
Study Design, Sample, and Setting
This retrospective analysis is based on a deidentified dataset containing medical, laboratory, and demographicinformation on 576 patients who were followed over8 years in the Heart Attack Prevention Clinic inNorthwestern United States, with at least 2 carotidimaging scans between January 2000 and June 2008.Clinic patients were referred to the clinic by their pri-mary care physicians or self-referred because of CV riskfactors such as hyperlipidemia, hypertension, diabetes,smoking, and family history or known CVD.
The clinical setting for this study specializes inmakinga comprehensive assessment of patients’ CVD risk todetermine their current arterial health status and, sub-sequently, to design a customized regimen of medica-tion, diet, and exercise. The clinic protocolsmay includemedications such as statins, angiotensin-convertingenzyme inhibitors, niacin, fibrates, and "-blockers, allof which have been shown to slow the progressionof IMT.20Y23
Procedure
The institutional review board of the academic institu-tion with which the authors are associated approvedthe study, and all patients provided written informedconsent before their medical records were entered intoan electronic registry. Participation in this registry wascompletely voluntary, and only arbitrary numbers wereused to identify participants to ensure confidentiality.No monetary incentive was given for taking part in theregistry. Data entered into the deidentified data setincluded a detailed medical history questionnaire filledout by participants with a focus on coronary artery dis-ease (CAD); IMT scan results such as mean IMT andPBS; other laboratory test results such as HgbA1C,fasting blood sugar (FBS), HDL, LDL, and Lp-PLA2;as well as medication history. In most cases, partici-pants underwent ultrasound examinations of the carotidartery at 1-year intervals and took other laboratory testson regular schedules. All patients received the sameindividualized Bale/Doneen Method protocol.
Measurement
At enrollment, each patient completed a medical history,medication history, physical examination, a panel ofblood tests, and anthropometric measurements. Cur-rent or past smokers were defined as those patientswho were using cigarette, pipe, cigar, or chew tobaccoor had been these in the past. The blood tests consistedstandard laboratory results, including HgbA1C, FBS,HDL, and LDL. In addition, carotid artery IMT scansand Lp-PLA2 tests were performed among our studyparticipants.
Carotid Intima-Media Thickness AssessmentCarotid artery IMT is assessed by B-mode ultrasound.Mean common IMT was defined as the mean of six10-mm measurements taken from the left and rightanterior, posterior, and lateral common carotid views.One of the primary outcomemeasures was the presenceor absence of carotid artery plaque as demonstrated byIMT. Plaque was defined as an IMT of greater than1.2 mm in the common, bifurcation, and internal ca-rotid artery. A PBSwas defined as the sum of all plaquesidentified in a single patient.
Research has validated the use of IMT as a reliableand noninvasive measure of disease-related arterial wallchanges.24,25 Intima-media thickness has been used asa surrogate marker of CVD and risk of a CV event,as well as means of identifying atherosclerosis and fol-lowing its progress.26,27 Although a small increase inIMTmay be an adaptive response to changes in BP andblood flow, there is consensus that IMT levels greaterthan 0.9 mm are indicative of atherosclerotic vasculardisease and end-organ damage.28 Atherosclerosis ofthe large- and medium-sized arteries is associated withplaque formation, inflammation, endothelial dysfunc-tion, thrombosis, and acute or chronic luminal obstruc-tion resulting in abnormal blood flow to target organs.29
Lipoprotein-Associated Phospholipase A2
Lipoprotein-associated phospholipase A2 is a fattyenzyme that is produced by inflammatory cells (mac-rophages, T-lymphocytes, and mast cells) and hydrolyzesoxidized phospholipids in LDL. This rupture-pronesubstance builds up in the artery wall from various riskfactors including elevated LDL cholesterol and can beused to determine risk levels for both heart events andstroke. The Lp-PLA2 test detects the presence of themore dangerous soft, rupture-prone plaque hiding inthe lining of arteries. Existing studies have indicatedthat Lp-PLA2 appears to be an independent marker ofCV risk30Y32 and that Lp-PLA2 is strongly correlatedwith several CV risk factors, especially lipid fractions,and with the degree of carotid artery atherosclerosis.33
Our previous studies also suggested use of Lp-PLA2
results for finding individuals whose outcome by stan-dard cardiac screeningmay be low risk butmay actuallybe at a higher risk after evaluation of the Lp-PLA2 re-sult. Thus, the Lp-PLA2 was monitored over the studyperiod as a genotypic marker for CV risk.
Insulin ResistanceEvidence is accumulating that there is an insulin-related CAD risk. For example, research has shownthat IR is responsible for most of CVDs34Y37 and thatIR is positively correlated with elevated TG, lowHDL,BP, plasminogen activator inhibitor 1, and brachial-ankle pulse wave velocity in a clinical sample.38 Thiscondition can be identified before a patient experiencing
4 Journal of Cardiovascular Nursing x Month 2014
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

8
an heart attack or stroke or becoming diabetic. In thecurrent study, IR risk was defined as TG/HDL-C ratioof 3.5 or greater, fasting glucose level of 100 mg/dL orgreater, 2-hour glucose tolerance of 140 mg/dL or greater,or metabolic syndrome, whereas metabolic syndromewas defined by NCEP criteria.34
Framingham Risk ScoreThe 10-year CVD risk was determined using theFraminghamRisk Score (FRS) as calculated in NationalCholesterol EducationProgramAdultTreatment Panel III(NCEP-ATP III). Risk factors included in determiningFRSwere age, gender, total cholesterol,HDL-C, smoking,systolic BP, and the use of antihypertensive agents. Allparticipants were categorized, based on NCEP-ATP III,into 3 groups: FRS less than 10%, FRS 10% to 20%,and FRS greater than 20% (ie, CAD or CAD-riskequivalent).
Coronary Artery DiseasePatients also reported their diagnosis of CAD, anginapectoris, previous MI, heart failure, cardiac surgery,arrhythmia, or hypertension. Coronary artery diseasewas defined as any history of acute coronary syndrome,percutaneous coronary intervention, coronary bypassgrafting, or presence of coronary artery calcification.Coronary artery disease equivalence was defined ashistory of cerebral vascular accident, presence of periph-eral arterial disease, diabetes, or FRS of 20%or higher.
Data Analysis
StrategyDescriptive statistics were obtained for all backgroundvariables using SPSS 20.0.39 Bivariate correlations(Pearson r) between continuous measures at baseline(eg,mean IMTandLp-PLA2) were calculated. Chi-squaretests were performed to evaluate the association be-tween key categorical variables (eg, presence/absence ofIR risk and atherosclerosis).
Furthermore, because observations (clinical outcomesor tests) over time are ‘‘nested’’ within a patient in thecurrent study, a statistical technique known as GCAwas used in modeling changes in the outcome measuresamong patients at the nurse-managed ambulatory clinicwho received the heart attack prevention program. Spe-cifically, the method used in the current study, the latentcurve GCA, was conducted through hierarchical linearmodeling.17,19,40,37
The modeling of change was accomplished by aseries of 2-level analyses using linear functions. Thelevel 1 analysis captures within-subject variability (ie,individual change over time), whereas level 2 analysescapture between-subject variability. At level 1, each sub-ject’s measure on the outcome variable is regressedonto the time variable (in this case, years since baseline),
resulting in a regression equation (in this case, a linearequation) that represents each individual patient’sgrowth curve. The coefficients that make up the regres-sion equation are the individual growth parameters: theintercept, which indicates the patient’s initial level ofthe outcome measure, and the linear slope, which in-dicates the patient’s rate of change of the outcomemeasure. At level 2, each growth parameter obtainedfrom level 1 is modeled by a regression equation thatcaptures the population main effect plus the variabilityresulting from each individual. The level 2 equationsfor the current study consist of 2 linear regressionequations, linking the patient’s trajectories of changeto patient-related characteristics (eg, age at enrollment,gender), which are considered as correlates of change.Similarly, level 1 and level 2 equations were used for allclinical outcome variables, to test whether male andfemale and older versus younger patients responded dif-ferently to the intervention. Missing data were handledusing the full information maximum likelihood esti-mation method, based on its advantages over the tra-ditional missing data techniques.41,42
Results
Sample Descriptive Statistics
All patients in this sample were white, and 61% (n =344)weremen.Mean (SD) age at the time of enrollmentwas 55.5 (10.2) years. Most (89%) had hyperlipidemia,58% had hypertension, 56% had metabolic syndromes(ie, thosewho had at least 3 of the following risk factors:TG 9150 mg/dL; FBS 9100 mg/dL; BP 9130/85 mmHg;waist circumference 935 or 940 in for women or men,respectively; and HDL G50 or G40 mg/dL for womenor men, respectively), 5%were diabetic, and 37%werepast or present smokers. Regarding adjusted FRS atbaseline, 66% were at moderate risk (ie, 10% 9 FRS),24% were at moderately high risk (ie, 20% 9 FRS 910%), and 10% were at high risk (ie, FRS 9 20%).Twenty-five percent of study participants showed indi-cations of CAD or CAD equivalent. Although aninitial IMT value at or above 0.9 mm is indicative ofatherosclerotic vascular disease according to EuropeanSociety of Hypertension-European Society of Cardiol-ogy guidelines,43 we used a more conservative cutoffpoint of 1.2 mm as indication of the presence of ca-rotid plaque (ie, carotid atherosclerosis was definedas an isolated intimal thickening of Q1.2 mm). Carotidplaque was identified in 64% of patients with moder-ate FRS risk, 87% of patients at moderately high FRSrisk, and 89% of patients at high FRS risk. It should benoted that 18% of our study population were asymp-tomatic primary prevention patients. Further detailsabout the demographic and medical characteristics ofthe sample can be found in Table 2.
Program for Early Prevention of Cardiovascular Events 5
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

9
Effectiveness of the Prevention
Fixed estimates predicting the 2 random effects, inter-cept (:0i) and linear slope (:1i), for each of the outcomemeasures are presented in Table 3. The intercepts showthe initial status of each measure at baseline, and theslopes indicate the rate of change. Overall, combiningmale and female patients of all ages, mean IMT scoredecreased by 0.01 per year (P G .001) on average, PBSdecreased by 0.17 per year (P G .001), LDL decreasedby 5.19 per year (P G .001), and Lp-PLA2 decreased
by 3.6 per year (P G .05). The linear slope of FBS wasnot statistically significant, indicating that the FBS levelwas stable over time. On the other hand, HgbA1Cincreased by 0.04 per year (P G .001) on average.Variances of both the intercept and the linear slopeof all the study variables are significant, indicatingheterogeneity (ie, interindividual differences) in theinitial level and change rate of these clinical outcomes(see Table 3). Figures 1A through H show the groupgrowth curve of the clinical outcomes of interest.
Based on the interindividual differences found atlevel 2 analysis, a conditional linear model was used totest sex and age at baseline as level 2 covariates. Table 4presents the unstandardized coefficients, showing theeffects of sex and age at baseline on the initial levels("01 and C01, respectively) as well as on the rate ofchange ("02 and C02, respectively). For mean IMT, thecoefficients revealed that men had significantly highermean IMT scores at baseline compared with women(B = 0.04, P G .001) and older patients had signifi-cantly higher mean IMT scores at baseline comparedwith younger patients (B = 0.01, P G .001). However,older patients showed a faster decrease in mean IMTscores, as evidenced by the negative effect of age onlinear slope (B = j0.0004, P G .01). Similarly, thesecond column of Table 4 shows that men had sig-nificantly higher PBS scores at baseline comparedwith women (B = 0.80, P G .05) and that older pa-tients had significantly higher PBS scores at baselinecompared with younger patients (B = 0.18, P G .001).However, there are no significant sex or age effects on
TABLE 2 Baseline Patient Demographic
Characteristics (N = 576)
Characteristic n (%) or Mean T SD
Age, y 55.5 T 10.2BMI, kg/m2 27.5 T 5.0Male 344 (61)White 576 (100)Current or past smoker 209 (36)Diabetes 25 (5)Hyperlipidemia 512 (89)Hypertension 325 (58)CAD/CAD equivalent 143 (25)Metabolic syndrome 321 (56)Insulin resistant 417 (73)Adjusted Framingham Risk ScoreG10% 370 (66)10%Y20% 141 (24)920% 58 (10)
Carotid plaqueVPBS score Q1.2 mm (85)
Abbreviations: BMI, body mass index; CAD, coronary artery disease;PBS, plaque burden score.
TABLE 3 Unstandardized Coefficients of the Unconditional Linear Growth-Curve Models of
Mean Intima-Media Thickness, Plaque Burden Score, Hemoglobin A1c, Fasting Blood Sugar, Fasting
Insulin Level (Insulin), High-Density Lipoprotein, Low-Density Lipoprotein, and Lipoprotein-Associated
Phospholipase A2
Outcomes IMT PBS score HgbA1C FBS Insulin HDL LDL Lp-PLA2
Fixed effectsIntercepta, :0i 0.79b 5.30b 5.37b 96.61b 8.84b 46.48b 131.14b 189.73b
Linear slopea, :1i j0.01b j0.17b 0.04b 0.26 0.06 1.40b j5.19b j3.60c
Random effectsIntercept variance 0.03 21.65 1.85 638.70 10.95 303.27 1280.69 11605.7822 1362.48b 922.77b 969.60b 682.36b 313.43c 1238.21b 1009.07b 360.24d
df 438 338 417 392 273 457 457 295Linear slope variance 0.0004 0.29 0.01 15.87 0.58 3.73 15.62 219.2522 1008.97b 666.003b 658.91b 599.43b 372.02b 807.56b 762.34b 359.12d
df 438 338 417 392 273 457 457 295Level 1 error variancea 0.002 1.42 0.08 96.61 24.77 69.48 522.73 1116.74
Reliability of OLS regression coefficient estimateInitial status 0.59 0.53 0.61 0.30 0.06 0.43 0.34 0.25Linear change rate 0.48 0.40 0.41 0.32 0.11 0.31 0.22 0.25
Abbreviations: FBS, fasting blood sugar; HDL, high-density lipoprotein; HgbA1C, hemoglobin A1c; IMT, intima-media thickness; LDL, low-densitylipoprotein; OLS, ordinary least-squares; Lp-PLA2, lipoprotein-associated phospholipase A2; PBS, plaque burden score.
aThe level 1 equation is Yit = :0i + :1i � Timeit + eit, where Yit represents the repeatedly measured outcome variable for individual i at time t; time ismeasured in weeks.
bP G .001.cP G .05.dP G .01.
6 Journal of Cardiovascular Nursing x Month 2014
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

10
FIGURE 1. A,Group growth curve of IMTmean. B, Group growth curve of the PBS score. C, Group growth curve of HgbA1C.D, Group growth curve of fasting blood sugar. E, Group growth curve of fasting insulin level. F, Group growth curve of HDL.G, Group growth curve of LDL. H, Group growth curve of Lp-PLA2. IMT, indicates intima-media thickness; PBS, plaqueburden score; HgbA1C, hemoglobin A1c; HDL, high-density lipoprotein; LDL, low-density lipoprotein; Lp-PLA2,lipoprotein-associated phospholipase A2.
Program for Early Prevention of Cardiovascular Events 7
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

11
the rate of change in PBS. Other significant effectsfound at level 2 are as follows: Men had significantlyhigher FBS scores, higher HDL scores, and lower LDLscores at baseline compared with women (B = 5.47,P G .05) and older patients had significantly higherHDL scores at baseline compared with younger pa-tients (B = 0.29, P G .05).
Discussion
The current findings seem to suggest that the Bale/Doneen Method is effective in generating a positiveeffect on the atherosclerotic disease process, namely,achieving regression of disease in the carotid arteries.This was demonstrated by a significant decrease inmean common carotid artery IMT (CCA-IMT) andPBS. It seems logical to speculate that this may result ina decrease in CV events. The medical managementresulted in a positive effect on at least 3 important CVrisk factors: LDL, HDL, and Lp-PLA2. Several previ-ous studies also demonstrated regression along with apositive effect on both LDL and HDL.44Y46 Extended-release niacin was used in a large percentage of thepatients treated with the Bale/Doneen Method, whichprobably accounts for the positive effect on both LDLand HDL. The slight increase in HgbA1c may be ex-plained by the use of niacin and statins. Despite thisincrease, there was a positive effect on atherosclerosis.This fits some of the recently published data that ques-tion the benefit of aggressive HgbA1C targets to reduceCV events.47,48 It is interesting that the FBS did notincrease significantly. Niacin is known to have a syn-ergistic effect with statins on reducing the levels ofLp-PLA2.
49 A recent study generated a strong signalthat Lp-PLA2 may be causal of atherosclerosis. If thatis the case, it seems logical to speculate that the positivetherapeutic effect on Lp-PLA2 may have also contrib-uted to regression of disease. There were numerous othervariables measured, but not analyzed, in these data that
may have also contributed to the regression results, suchas BP. Perhaps, 1 of the most salient issues regardless ofknowing for sure all of the reasons for the results is thatthese data indicate that there is a method available tomanage CV risk that is clinically applicable and thatcan generate regression of atherosclerosis.
This data set should be analyzed further in an at-tempt to ferret out all significant variables that may beassociated with the positive results. It seems that theGCA is a valuable technique to accomplish this. Theseresults should generate hypotheses for future random-ized placebo controlled trials.
There are numerous weaknesses with the data. Therewas no placebo group. The patients were all white andmotivated to enter a prevention clinic. Most of the pa-tients were men. Perhaps, 1 of the greatest strengths isthe fact that these data were generated in an ambulatoryclinical setting and represent the first data publishedusing long-term serial cIMT to monitor atherosclerosisin a nonacademic setting. This article, to the authors’knowledge, is the first report to examine the utility ofmultilevel GCA in studying trajectories of clinical out-comes related to CVD.
Limitations and Suggestions forFuture Research
The current study is based on a single group of patientswho were enrolled at 1 clinic in Northwestern UnitedStates. Future studies should include a comparison groupand use the randomized control treatment design toevaluate the effectiveness of the prevention method. Infact, large, prospective, randomized controlled studiesare needed to evaluate the impact of novel approachesto preventing and averting CVD. The significance ofspecific risk factors, including those not amenable topharmacological treatmentVdiet, exercise, many sleep,and psychological issuesVshould be sorted out in largerstudies. Another limitation lies in the lack of diversity of
TABLE 4 Fixed Effects (Unstandardized Coefficients) of Level 2a Covariates, Sex and Age at Baseline,
in Predicting Differences in the Initial Level and Change Rate in Mean Intima-Media Thickness, Plaque
Burden Score, Hemoglobin A1c, Fasting Blood Sugar, Fasting Insulin Level (Insulin), High-Density
Lipoprotein, Low-Density Lipoprotein, and Lipoprotein-Associated Phospholipase A2
Source Mean IMT PBS HgbA1C FBS Insulin HDL LDL Lp-PLA2
Intercepta
Sex, "01 0.04b 0.80c 0.05 5.47c 0.89 j5.68b j5.87c 9.30Baseline age, C01 0.01b 0.18b 0.01 j0.01 0.03 0.29c j0.28 j0.36
Linear slopea
Sex, "02 j0.002 0.02 j0.004 j0.47 j0.07 j0.16 0.43 j1.38Baseline age, C02 j0.0004d j0.003 0.001 0.02 j0.01 j0.01 j0.01 0.10
Abbreviations: FBS, fasting blood sugar; HDL, high-density lipoprotein; HgbA1C, hemoglobin A1c; IMT, intima-media thickness; LDL, low-densitylipoprotein; Lp-PLA2, lipoprotein-associated phospholipase A2; PBS, plaque burden score.
aLevel 2 equations are as follows: :0i = "00 + "01(sex)it + "02(age at baseline)it + ei and :1i = C00 + C01(sex)it + C02(age at baseline)it + ei. Sex is dummycoded (male = 1 and female = j1); age at baseline is not centered.
bP G .001.cP G .05.dP G .01.
8 Journal of Cardiovascular Nursing x Month 2014
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

12
the current study sample. Nearly 100% of the samplesare white. Data collection across more diverse patientpopulations is needed. Although cIMT testing in theclinical setting is not commonly performed, the avail-ability of cIMT testing is increasing. Criteria for ap-propriate use of CIMT were published in the journalAtherosclerosis in October 2010.50 Cardiovascular andarteriosclerotic vascular diseases are multifactorial. Theeffective prevention methods should attempt to gainoptimal control of and influence as many of those fac-tors as possible. Future evaluation studies should alsotake into account patient motivation and adherence.Indeed, if the goal is to focus only on those risk fac-tors, the patient will generally be faced with ever higherdoses of statins and other pharmacotherapy, whichmay have lower up-front costs but higher risk of adversereactions from such agents. In addition, if that agentneeds to be withdrawn, the patient may quickly be-come uncontrolled and face added risk of CVevents. Amultifactorial disease treatment paradigm such as theBale/Doneen Method may prove to be safer and moreeconomical in the long run.
Summary
The Bale/Doneen Method for the prevention of heartattacks and strokes is a clinically based approach focusedon the actual disease of atherosclerosis. The current stan-dard of care supports managing the disease from a riskfactor approach, which has proven to support recidivisticevents and a lack of ability to determine asymptom-atic vascular disease before the patient experiencing aclinically significant ischemic event. We have proven
that our global disease treatment paradigm can be ac-complished in the ambulatory setting and can demon-strate a direct impact on the atherosclerotic process.This GCA of cIMT test results demonstrates the ef-fectiveness of a model focused on patient education,disease identification and monitoring, routine assess-ment of vascular inflammation, identifying and treatingthe root causes of atherosclerosis, setting optimal goalsfor management of risk factors, and using genetics toindividualize care to the unique individual needs ofthe patient. These data support that a disease treatmentparadigm,when applied in an ambulatory setting, causesa direct impact on the disease of atherosclerosis. Noneof the patients in this study had a CV event during the8 years of follow-up despite the fact that many hadatherosclerotic lesions and many were secondary pre-vention patients.
The purpose of this study was to evaluate CVDprevention/treatment methods based on data collectedfrom a real clinical practice, a nurse-managed clinic, byexamining changes in IMT and phenotypic and geno-typic markers associated with CVD. Using these markerscan improve the accuracy of CVD risk prediction andalso help in selecting potentially effective treatment.Because the methods of assessing and treating patientsused by the Bale/Doneen Methods are available to anypractitioner, it is believed that analysis of this data willbe beneficial in the understanding of better CV pre-vention programs.
The multilevel growth-curve modeling techniqueappears to be well suited to complex modeling of mul-tiple signs or symptoms and related outcomes. Themethod may enhance the ability of researchers to an-alyze results of the complex data that emerge whensymptom clusters are being studied. The data includethe process of change in clinical signs and symptomsand the relationship of such processes to other individ-ual and clinical characteristics of patients, as well as tounderlying mechanistic models.
REFERENCES
1. Arbab-Zadeh A, Nakano M, Virmani R, Fuster V. Acutecoronary events. Circulation. 2012;125(9):1147Y1156.
2. Collaboration IRGCERF, Sarwar N, Butterworth AS, et al.Interleukin-6 receptor pathways in coronary heart disease:a collaborative meta-analysis of 82 studies. Lancet. 2012;379(9822):1205Y1213.
3. Devaraj S, Tang R, Adams-Huet B, et al. Effect of high-dose alpha-tocopherol supplementation on biomarkers ofoxidative stress and inflammation and carotid atheroscle-rosis in patients with coronary artery disease. Am J ClinNutr. 2007;86(5):1392Y1398.
4. Blin J, Ahmad Z, Rampal LR, Mohtarrudin N, Tajudin AK,Adnan RS. Preliminary assessment of differential expressionof candidate genes associated with atherosclerosis. GenesGenet Syst. 2013;88(3):199Y209.
5. Krychtiuk KA, Kastl SP, Speidl WS, Wojta J. Inflammationand coagulation in atherosclerosis.Hamostaseologie. 2013;33(4):269Y282.
What’s New and Important
h The Bale/Doneen Method rests on a platform ofassessing and monitoring arterial disease. It is anchoredin inflammation being causal of atherosclerosis. Themethod comprehensively evaluates known sources forarterial inflammation and promotes optimal managementof all identified contributors to the arterial ‘‘fire.’’ Themethods of assessing and treating patients used by theBale/Doneen Methods are available to any practitioner.
h Previous studies have indicated that patients who receiveprevention and treatment of CVD through the Bale/DoneenMethod show stabilization of the atheroscleroticdisease process, a significant conversion of plaquemorphology to 100% echogenic lesions by the fifth yearof follow-up, and that echogenic carotid plaque issignificantly less inflamed than nonecogenic plaque.Consistent with past studies, this article shows that theBale/Doneen Method is effective in generating a positiveeffect on the atherosclerotic disease process by achievingregression of disease in the carotid arteries.
h The use of growth-curve modeling in examiningchanges in markers such as IMT and other biomarkersassociated with CVD can improve the accuracy of CVDrisk prediction and help identify effective treatments.
Program for Early Prevention of Cardiovascular Events 9
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

13
6. Belcaro G, Nicolaides AN, Ramaswami G, et al. Carotidand femoral ultrasound morphology screening and cardio-vascular events in low risk subjects: a 10-year follow-upstudy (the CAFES-CAVE study(1)). Atherosclerosis. 2001;156(2):379Y387.
7. Musa S, Haynes E. Biomarkers of obesity and subsequentcardiovascular events. Epidemiol Rev. 2007;29:1093.
8. Muscari A, Antonelli S, Bianchi G, et al. Serum C3 is astronger inflammatory marker of insulin resistance thanC-reactive protein, leukocyte count, and erythrocyte sedi-mentation rate: comparison study in an elderly population.Diabetes Care. 2007;30(9):2362Y2368.
9. Grundy SM, Cleeman JI, Merz CN, et al. Implications ofrecent clinical trials for the National Cholesterol Educa-tion Program Adult Treatment Panel III Guidelines. J AmColl Cardiol. 2004;44(3):720Y732.
10. Kullo IJ, Malik AR. Arterial ultrasonography and tonom-etry as adjuncts to cardiovascular risk stratification. J AmColl Cardiol. 2007;49(13):1413Y1426.
11. Balestrini S, Lupidi F, Balucani C, et al. One-year progres-sion of moderate asymptomatic carotid stenosis predicts therisk of vascular events. Stroke. 2013;44(3):792Y794.
12. Figueroa AL, Subramanian SS, Cury RC, et al. Distributionof inflammation within carotid atherosclerotic plaques withhigh-risk morphological features: a comparison betweenpositron emission tomography activity, plaque morphology,and histopathology. Circulation. 2012;5(1):69Y77.
13. Superko HR, Roberts R, Agatston A, et al. Genetic testingfor early detection of individuals at risk of coronary heartdisease and monitoring response to therapy: challenges andpromises. Curr Atheroscler Reports. 2011;13(5):396Y404.
14. Komduur R, Te Molder H. The role of genes in talkingabout overweight: an analysis of discourse on genetics, over-weight and health risks in relation to nutrigenomics. PublicUnderstand Sci. 2013. DOI: 10.1177/0963662512472159.
15. Eichner JE,Dunn ST, PerveenG,ThompsonDM, Stewart KE,Stroehla BC. Apolipoprotein E polymorphism and cardio-vascular disease: a HuGE review. Am J Epidemiol. 2002;155(6):487Y495.
16. Dudley WN, McGuire DB, Peterson DE, Wong B.Application ofmultilevel growth-curve analysis in cancer treat-ment toxicities: the exemplar of oralmucositis and pain.OncolNurs Forum. 2009;36(1):E11YE19.
17. Raudenbush SW, Bryk AS. Hierarchical Linear Models:Applications and Data Analysis Methods. Thousand Oaks,CA: Sage Publications; 2002.
18. RogosaDR. Myth and methods: ‘‘myths about longitudinalresearch,’’ plus supplemental questions. In: Gottman JM, ed.TheAnalysis of Change. Hillsdale, NJ: Erlbaum; 1995:3Y65.
19. Singer JD, Willet JB. Applied Longitudinal Data Analysis:Modeling Change and Event Occurrence. Oxford: Uni-versity Press; 2003.
20. Crouse JR 3rd, Raichlen JS, Riley WA, et al. Effect ofrosuvastatin on progression of carotid intima-media thick-ness in low-risk individuals with subclinical atherosclerosis:the METEOR Trial. JAMA. 2007;297(12):1344Y1353.
21. Salonen R, Nyyssonen K, Porkkala E, et al. KuopioAtherosclerosis Prevention Study (KAPS): a population-based primary preventive trial of the effect of LDL loweringon atherosclerotic progression in carotid and femoralarteries. Circulation. 1995;92(7):1758Y1764.
22. Taylor AJ, Sullenberger LE, Lee HJ, Lee JK, Grace KA.Arterial Biology for the Investigation of the TreatmentEffects of Reducing Cholesterol (ARBITER) 2: a double-blind, placebo-controlled study of extended-release niacinon atherosclerosis progression in secondary prevention
patients treated with statins. Circulation. 2004;110(23):3512Y3517.
23. WiklundO,Hulthe J,Wikstrand J, Schmidt C,Olofsson SO,Bondjers G. Effect of controlled release/extended releasemetoprolol on carotid intima-media thickness in patientswith hypercholesterolemia: a 3-year randomized study. Stroke.2002;33(2):572Y577.
24. Bots ML, Dijk JM, Oren A, Grobbee DE. Carotid intima-media thickness, arterial stiffness and risk of cardiovasculardisease: current evidence. Journal of Hypertension. 2002;20(23):17Y25.
25. Lucas FL, DeLorenzo MA, Siewers AE, Wennberg DE.Temporal trends in the utilization of diagnostic testing andtreatments for cardiovascular disease in the United States,1993Y2001. Circulation. 2006;113:374Y379.
26. Minino AM, Heron MP, Murphy SL, Kochanek KD. Cen-ters for Disease Control and Prevention, National Centerfor Health Statistics, National Vital Statistics Reports.Deaths: final data for 2004. Natl Vital Stat Rep. 2007;55(19):1Y119.
27. Rosamond W, Flegal K, Friday G, et al. Heart disease andstroke statisticsY2007 update: a report from the AmericanHeart Association Statistics Committee and Stroke Statis-tics Subcommittee. Circulation. 2007;115(5):e69Ye171.
28. Van Bortel LM. What does intima-media thickness tell us?J Hypertens. 2005;23:37Y39.
29. Orford JL, Selwyn AP, Ganz P, Popma JJ, Rogers C. Thecomparative pathobiology of atherosclerosis and restenosis.Am J Cardiol. 2000;86:6HY11H.
30. Ballantyne CM, BlazingMA, Hunninghake DB, et al. Effecton high-density lipoprotein cholesterol of maximum dosesimvastatin and atorvastatin in patients with hypercholes-terolemia: results of the Comparative HDL Efficacy andSafety Study (CHESS). Am Heart J. 2003;146(5):862Y869.
31. Packard CJ, O’Reilly DS, Caslake MJ, et al. Lipoprotein-associated phospholipase A2 as an independent predictor ofcoronary heart disease. West of Scotland Coronary Preven-tion Study Group.N Engl J Med. 2000;343(16):1148Y1155.
32. Ishida K, Cucchiara B. Therapeutic options to reduce Lp-PLA2 levels and the potential impact on vascular risk re-duction. Curr Treat Options Cardiovasc Med. 2013;15(3):313Y321.
33. Persson M, Nilsson J, Nelson J, Hedblad B, Berglund G.The epidemiology of Lp-PLA2: distribution and correla-tion with cardiovascular risk factors in a population-basedcohort Atherosclerosis. 2007;190(2):388Y396.
34. Grundy SM, Cleeman JI, Daniels SR. Diagnosis and manage-ment of themetabolic syndrome: anAmericanHeartAssociation/National Heart, Lung, and Blood Institute scientific statement.Circulation. 2005;112:2735Y2752.
35. Haffner SM,ValdezRA,HazudaHP,Mitchell BD,Morales PA,Stern MP. Prospective analysis of the insulin-resistance syn-drome (syndrome X). Diabetes. 1992;41(6):715Y722.
36. Jeppesen J,HansenTW,Rasmussen S, IbsenH,Torp-PedersenC,Madsbad S. Insulin resistance, the metabolic syndrome, andrisk of incident cardiovascular disease: a population-basedstudy. J Am Coll Cardiol. 2007;49(21):2112Y2119.
37. McFarlane SI, Banerji M, Sowers JR. Insulin resistance andcardiovascular disease. J Clin Endocrinol Metab. 2001;86(2):713Y771.
38. Tso TK, Huang WN. Elevation of fasting insulin and itsassociation with cardiovascular disease risk in women withsystemic lupus erythematosus. Rheumatol Int. 2009;29(7):735Y742.
39. SPSS forWindows [computer program]. Version 16.0. Chicago,IL: SPSS Inc; 2007.
10 Journal of Cardiovascular Nursing x Month 2014
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

14
40. Curran PJ, Muthen BO. The application of latent curveanalysis to testing developmental theories in interventionresearch. Am J Commun Psychol. 1999;27:567Y595.
41. Newman D. Longitudinal modeling with randomly and sys-tematically missing data: a simulation of ad hoc, maximumlikelihood, and multiple imputation techniques. Org ResMethods. 2003;6:328Y362.
42. Schafer JL, Graham JW. Missing data: our view of thestate of the art. Psychol Methods. 2002;7:147Y177.
43. European Society ofHypertension-European Society of Cardi-ology guidelines for the management of arterial hypertension.J Hypertens. 2003;21:1011Y1053.
44. Brown BG, Zhao XQ, Chait A, et al. Simvastatin and niacin,antioxidant vitamins, or the combination for the prevention ofcoronary disease.N Engl J Med. 2001;345(22):1583Y1592.
45. Taylor AJ, LeeHJ, Sullenberger LE. The effect of 24 monthsof combination statin and extended-release niacin on carotidintima-media thickness: ARBITER 3. Curr Med Res Opin.2006;22(11):2243Y2250.
46. Taylor AJ, Villines TC, Stanek EJ, et al. Extended-releaseniacin or ezetimibe and carotid intima-media thickness.N Engl J Med. 2009;361(22):2113Y2122.
47. Naito R, Miyauchi K, Ogita M, et al. Impact of admissionglycemia and glycosylated hemoglobin A1c on long-termclinical outcomes of non-diabetic patients with acute cor-onary syndrome. J Cardiol. 2013;63(2):106Y111.
48. Nathan DM, McGee P, Steffes MW, Lachin JM, theDERG. Relationship of glycated albumin to blood glucoseand glycated hemoglobin (HbA1C) values and to retinop-athy, nephropathy and cardiovascular outcomes in theDCCT/EDIC Study. Diabetes. 2013;63(1):282Y290.
49. Reddy KJ, Singh M, Batsell RR, Bangit JR, Miraskar RA,Zaheer MS. Lipoprotein-associated phospholipase A2
mass is significantly reduced in dyslipidemic patientstreated with lifestyle modification and combination lipid-modifying drug therapy. Prev Cardiol. 2010;13(3):130Y134.
50. Society of Atherosclerosis Imaging and Prevention, incollaboration with the International Atherosclerosis Society.Appropriate use criteria for carotid intima media thicknesstesting. Atherosclerosis. 2011;214(1):43Y46.
51. Lavie CJ, Lee JH, Milani RV. Vitamin D and cardiovas-cular disease: will it live up to its hype? J Am Coll Cardiol.2011;58(15):1547Y1556.
Program for Early Prevention of Cardiovascular Events 11
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

15
Heart Health Open Access
Received: Nov 11, 2014Accepted: Nov 21, 2014Published: Nov 26, 2014
Amy L. Doneen, DNP, ARNP*, Alice Dupler, JD, APRN-BC, and Neva L. Crogan, PhD, ARNP, FAAN
Cardiovascular Wellness and Optimal Oral HealthIn order to appreciate the oral/systemic connection as it relates
to vascular wellness, it is important to understand health from
the perspective of the arteries and the mouth. Arterial health (or
cardiovascular wellness) is a state for which atherosclerosis is
absent [1], and, if atherosclerosis is present in the arterial
system, there is no inflammation driving further development of
disease progression [2]. Optimal oral health, as it relates to
vascular wellness, is an oral environment that lacks the
inflammation to allow oral pathogens to invade the vascular
system and create the opportunity for an unstable atherosclerotic
disease state [3]. There are many conditions that cause vascular
inflammation. Oral bacteria (periodontal disease) are one of
those conditions.
Cardiovascular Disease: A costly conditionCardiovascular Disease (CVD) remains the leading cause of
death and disability in developed countries, creating a
catastrophic financial strain on our current health care system.
The current health care paradigm is structured around treating
end-stage disease, treating the disease after it becomes evident.
The annual expenditure allocated to treat vascular disease has
skyrocketed to over 600 billion dollars, including direct and
indirect costs. It is estimated to increase to 3.1 trillion dollars
annually by the year 2030 [4]. One-third of all cardiovascular
deaths occur in individuals less than 75 years of age [5]. Fifty
percent of annual major coronary events are recidivistic and of
these, fifty percent are fatal [6].
Event Reality: What causes a cardiovascular event?These statistics can be changed by understanding the
mechanism for which heart attack and ischemic stroke occur.
We can then fully appreciate the relationship between CVD and
oral health. Atherosclerotic plaque silently develops in the
artery wall, avoiding encroachment into the lumen resulting in
an asymptomatic and potentially dangerous situation. When the
artery wall weakens due to an influx of inflammation, the
protective endothelial lining can rupture or erode, exposing the
plaque to arterial blood flow, and subsequently creating the
potential for thrombus formation. Surprisingly, the majority of
these ruptures or erosions does not result in major CV events
but rather create micro vascular thrombi that lead to micro
vascular disease such as silent heart attacks, transient ischemic
events, vascular dementia and diseases of ageing such as
chronic kidney disease and peripheral arterial disease [7].
Regardless of the end result of the thrombus, the presence of an
atheroma is sine qui non for a vascular event [7].
Inflammation: the keystone joining vascular and oral
healthUnderstanding this mechanism – the inflammatory relationship
between atherosclerotic plaque development and thrombus
formation is the key to CVD prevention. The symbiosis between
CVD and periodontal disease starts here- at the inflammatory
http://dx.doi.org/10.14437/HHOA-1-104 Review Amy L. Doneen, DNP, ARNP, Heart Health Open Access 2014, 1:1
Cardiovascular Wellness and Optimal Oral Health: A symbiotic
Relationship
Corresponding Author: Amy L. Doneen, Medical
Director, Heart Attack & Stroke Prevention Center, Adjunct
professor Texas Tech Health Sciences Center USA; E-mail:
Copyright: © 2014 HHOA. This is an open-access article distributed under the terms of the Creative Commons Attribution License, Version 3.0, which permits unrestricted
use, distribution, and reproduction in any medium, provided the original author and source are credited.
Volume 1 • Issue 1 • 104 www.aperito.org

16
http://dx.doi.org/10.14437/HHOA-1-104 Page 2 of 4
Citation: Amy L. Doneen (2014 Cardiovascular Wellness and Optimal Oral Health: A symbiotic Relationship. Heart Health Open Access 1:104
juncture. Periodontal Disease (PD) is one of many causes of this
keystone ingredient – inflammation, both promoting the
development of plaque and the unpredictable cascade of plaque
rupture and thrombus formation. The American Heart
Association’s meta-analysis determined that CVD was greatly
increased in subjects with periodontitis and subsequently
confirmed an independent association between PD and CVD
with Level A evidence [8]. Potentially even more concerning,
oral bacteria associated with endodontic disease has been tied to
actual acute coronary events [9]. Cross-sectional epidemiologic
studies demonstrate the association between periodontitis and
elevated risk for CVD. Specific periodontal pathogens have
been shown to play a vital role in the atherogenic disease
process [3]. Additionally, studies have focused on the systemic
effect of periodontal intervention on surrogate indicators of
CVD, including serum inflammatory markers, serum lipid levels
and hemostatic factors [3].
The CORODENT study evaluated the role of periodontal
pathogen burden on coronary events and PD. The controlled
study of 526 patients without a known history of coronary heart
disease (CHD) had sub gingival samples of biofilm analyzed for
periodontal bacteria. The results reflected a statistically
significant association between the periodontal pathogen burden
and the presence of CHD [10]. Additionally, the INVEST trial
[11], evaluated periodontal bacteria and hypertension in 653
subjects without a history of stroke or heart attack. Findings
were adjusted for age, race, sex, education, BMI, smoking, DM,
LDL and HDL. In subjects with the highest tertile of PD
pathogen burden, systolic blood pressure was 9mmHg higher
and diastolic BP was 5 mmHg higher than in subjects with the
lowest tertile. Lastly, and importantly, end toxins of gram-
negative bacteria, such as Porphyromonas gingivalis (Pg) is
considered causative of periodontitis. Lipo polysaccharide end
toxin (LPS), a specific toxin of this bacterium, is common to
other bacterial diseases such as E. coli and Salmonella
infections. Pg LPS has been shown to stimulate atherosclerotic
related gene expression in foam cells and to stimulate
transcription of pro-inflammatory cytokines, adhesion
molecules and growth factors [10] concluding that the end
toxins of Pg are directly involved in the development of
atherosclerotic vascular disease.
Who’s role is it anyway?Appreciating the relationship between the inflammatory
cascades associated with oral health and CVD, a dialogue
between the medical provider and the dental provider must be
nurtured. A conundrum potentially exists when we find a chasm
between the medical and dental models of care. This divide is
deeply rooted in academia and carried into practice. Many
medical providers who treat vascular disease received minimal
training to know how to properly assess for oral inflammation.
Additionally, the dental providers may struggle to push
boundaries of care beyond the oral cavity, potentially fearing
the public perception. For those practicing CVD prevention in
the medical model, we celebrate dental professional
involvement on the team, being so bold as to suggest that it is
necessary if we want to mitigate the potentially devastating
effects of CVD. Statistically, 65-70% of adults see the dentist
annually whereas up to 20% of these patients have not had a
medical appointment in the preceding year.
The public agrees. Adult dental patients were surveyed as to
their perception of receiving medical screenings while in the
dental setting and there was a 94% approval of this approach.
Specifically, 90% of the patients surveyed felt it important for
dental professionals to screen for hypertension and over 80%
felt it valuable to be screened for diabetes and CVD in the
dental setting [12]. The overwhelming (>75%) opinion was that
their view of the dental provider would improve for knowledge
and professionalism, competence and compassion [13]. In
addition to gaining public approval, periodontal therapy also
saves healthcare costs in diabetic and CVD patients. Analyzing
over 100,000 PD patients with diabetes and/or CVD, mean age
48.7 (+ 10.9 years).PD treatment required > 4 dental visits
annually, mainly scaling and root planning along with flap
surgeries as needed and routine cleanings. The primary outcome
was all medical (non-dental) costs in years 2006-2009.The
secondary outcome was yearly hospitalizations/1000 clients in
Volume 1 • Issue 1 • 104 www.aperito.org

17
http://dx.doi.org/10.14437/HHOA-1-104 Page 3 of 4
Citation: Amy L. Doneen (2014 Cardiovascular Wellness and Optimal Oral Health: A symbiotic Relationship. Heart Health Open Access 1:104
years 2005-2009. Treatment of PD resulted in a 40% decrease in
annual dollars spent on stroke and diabetes. A 10% decrease in
resource expenditure was utilized for CHD care.
Hospitalizations were decreased on average 20-30% for CHD
related issues, including diabetes, stroke and heart disease [12].
Joining hands to prevent CVDThe language spoken between the medical and dental
community in regards to CVD must be one of mutual
recognition. In the medical community, laboratory data is
utilized to reveal hidden causes of vascular inflammation. We
utilize blood and urine tests to evaluate the effectiveness of
treatment, lifestyle and pharmaceutical interventions, on the
endothelium and intima layers of the artery, providing
confidence to know that the patient is safe. Likewise, we
embrace technology to identify asymptomatic atherosclerosis
and follow the disease over time. This approach, called the
Bale/Doneen Method has been proven to be effective in
generating a positive effect on the atherosclerotic disease
process by achieving regression of disease in the carotid arteries
[14]. Ultimately we are treating a disease that we hope our
patients never feel. If they were to ‘feel’ the disease, a rupture
or an erosion would have resulted in a thrombotic event.
Optimal CV wellness and optimal oral health are tied together
by a lack of inflammatory burden. Knowing that periodontal
disease and endodontic pathogen burden are one of the critical
root causes of this inflammatory disease, we rely on our dental
colleagues to participate in CVD prevention. We feel it to be
our responsibility to learn how to assess for gingival
inflammation in the medical office and we ask our dental
colleagues to participate in laboratory testing to determine
pathogen burden objectively with PCR laboratory testing so that
the language between providers can be objective and
understood.
In addition to speaking the same laboratory language to
diagnose PD and vascular inflammation, it is a solid idea to
propose a care model that invites registered dental hygienists
into the medical office to teach and assess patients about proper
dental hygiene is a strong starting point. Atherosclerotic
vascular disease is a multi-faceted inflammatory condition that
involves many specialists to properly treat. The ideal medical
model welcomes our dental colleagues to a team of specialists
that encompass providers in the areas of family practice,
cardiology, sleep medicine, endocrinology, psychology,
nutrition, exercise science and life coaching. We view
inflammation driven by oral health on par with other
inflammatory causative factors such as insulin resistance, sleep
apnea, dyslipidemia and hypertension among others. We ask for
a partnership with our dental colleagues to join in the fight
against the devastating effects of cardiovascular disease.
Together, we can achieve optimal wellness.
References1. Belcaro G, Nicolaides AN, Ramaswami G, Cesarone MR,
De Sanctis M, et al. (2001) Carotid and femoral ultrasound
morphology screening and cardiovascular events in low
risk subjects: a 10-year follow-up study (the CAFES-
CAVE study). Atherosclerosis. 156:379-387.
2. Aldrovandi A, Cademartiri F, Arduini D, Lina D, Ugo F, et
al. (2012) Computed tomography coronary angiography in
patients with acute myocardial infarction without
significant coronary stenosis. Circulation. 126:3000-3007.
3. Xiang Ying Ouyang, Wen Mei Xiao, Yi Chu, Shuang Ying
Zhou. (2011) Influence of periodontal intervention therapy
on risk of cardiovascular disease. Periodontology 56: 227-
257.
4. Go A, Mozaffarian D, Roger V, Benjamin E, Berry J, et al.
(2014). Heart disease and stroke statistics – 2014 update: a
report from the American heart association. Circulation.
129: e28-e292.
5. Roger. V, Go A, Lloyd-Jones D, Benjamin E, Berry J, et
al. (2012) American Heart Association Statistics
Committee and Stroke Statistics Subcommittee. Heart
disease and stroke statistics: 2012 update: a report from the
American Heart Association Circulation. 125: e2-e220.
6. Briffa T, Tonkin A. (2013) Put disease prevention first.
Circulation. 128: 573-575.
Volume 1 • Issue 1 • 104 www.aperito.org

18
http://dx.doi.org/10.14437/HHOA-1-104 Page 4 of 4
Citation: Amy L. Doneen (2014 Cardiovascular Wellness and Optimal Oral Health: A symbiotic Relationship. Heart Health Open Access 1:104
7. Arbab-Zadeh A, Nakano M, Virmani R, Fuster V. (2012)
Acute coronary events. Circulation. 125:1147-1156.
8. Lockhart P, Bolger A, Papapanou P, Osinbowale O,
Trevisan M, et al. (2012) Periodontal disease and
atherosclerotic vascular disease: does the evidence support
an independent association? A scientific statement from
the American Heart Association. Circulation published
online.
9. Pessi T. (2013) Bacterial signatures in thrombus aspirates
of patients with myocardial infarction. Circulation.
127:1219-1228.
10. Lei L, Li H. (2011) Porphyromonas gingivalis
lipopolysaccharide (LPS) alters atherosclerotic-related
gene expression in oxidized low-density-lipoprotein-
induced macrophages and foam cells. J Periodontal Res.
11. Desvarieux M, Demmer RT, Rundek T, Boden-Albala J,
Sacco RL, et al. (2005) Periodontal Microbiota and
Carotid Intima-media thickness: The oral infections and
vascular disease epidemiology Study (INVEST)
Circulation.111;576.
12. Jeffcoat, M. Impact of periodontal therapy on general
health: Evidence from insurance data for five systemic
conditions. Am J Prev Med 47: 166-174.
13. Greenberg B. Glick M. Assessing systemic disease risk in
a dental setting: a public health perspective. Dent Clin
North Am, 55: 863-874.
14. Feng D, Esperat C, Doneen A, Bale B, Song H, Green A.
8-year outcomes of a program for early prevention of
cardiovascular events. A growth curve analysis.J
Cardiolvasc Nurs. 2014.
Volume 1 • Issue 1 • 104 www.aperito.org

19
Statistical Fact Sheet 2013 Update
Women & Cardiovascular Diseases
Major Causes of Death for Males and Females, 2009
A indicates cardiovascular disease plus congenital cardiovascular disease (ICD-10 I00-I99, Q20-Q28); B, cancer (C00-C97 ); C, acci-dents (V01-X59,Y85-Y86); D, chronic lower respiratory disease (J40-J47); E, diabetes mellitus (E10-E14); F, Alzheimer disease (G30). Source: NCHS.
Coronary Heart Disease (CHD) (ICD/10 codes I20-I25) (ICD/9 codes 410-414, 429.2) About 6.6 million females alive today have CHD. Of these, 2.6 million have a history of myocardial
infarction (MI, or heart attack). Each year new and recurrent MI and fatal CHD will impact an estimated 380,000 women. The 2009 overall CHD death rate was 116.1. Death rates were 84.9 for white females and 110.3
for black females. 26% of women age 45 and older who have an initial recognized MI (heart attack) die within a
year compared with 19% of men. In part because women have heart attacks at older ages than men do, they’re more likely to die from them within a few weeks.
64% of women who died suddenly of CHD had no previous symptoms. 518,000 females diagnosed with CHD were discharged from short-stay hospitals in 2010.
©2013 American Heart Association, Inc. All rights reserved. Unauthorized use prohibited.
Cardiovascular Disease (CVD) (ICD/10 codes I00-I99, Q20-Q28) More than one in three female adults has some form of cardiovascular disease (CVD). Since 1984, the number of CVD deaths for females has exceeded those for males. In 2009, CVD was the cause of death in 401,495 females. Females represented 51.0% of deaths from
CVD. The 2009 death rate from CVD was 236.1. Death rates were 190.4 for white females and 267.9 for black
females. In 2010, CVD was the first listed diagnosis of 2.8 million females discharged from short-stay hospitals. In 2010, 25.1% of bypass and 32.9% of PCI patients were female. 31.3% of heart transplant patients
in 2011 were female.

20
Women & CVD - 2013 Statistical Fact Sheet
©2013 American Heart Association, Inc. All rights reserved. Unauthorized use prohibited.
Cardiovascular Disease Mortality Trends for Males and Females United States: 1979–2009
Source: NCHS.
Angina Pectoris (ICD/10 code I20) (ICD/9 code 413) More women than men have angina in total numbers (4.1 million vs. 3.7 million). Among non-Hispanic women age 20 and older, 2.8% of non-Hispanic whites; 5.4% of non-
Hispanic blacks and 3.3% of Mexican Americans have angina. Each year about 180,000 women over age 45 are diagnosed with stable angina. Congenital Cardiovascular Defects (ICD/10 codes Q20-Q28) (ICD/9 codes 745-747) The 2009 overall death rate for congenital cardiovascular defects was 1.0. Death rates were
0.9 for white females and 1.2 for black females. 27,000 females were discharged from short-stay hospitals in 2009 with a diagnosis of congenital
cardiovascular defects.
Age-Adjusted Death Rates for Coronary Heart Disease, Stroke, and Lung and Breast Cancer for White and Black Females, 2009
Source: NCHS.
21
Stroke (ICD/10 codes I60-I69) (ICD/9 codes 430-438) An estimated 3.8 million female stroke survivors are alive today. Among women age 20 and older, the following have had a stroke: 2.9% of non-Hispanic whites;
4.7% of non-Hispanic blacks and 1.4% of Mexican Americans. Each year about 55,000 more women than men have a stroke. This is because the average life
expectancy for women is greater than for men, and the highest rates for stroke are in the oldest age groups.
In 2009, stroke caused the death of 76,769 females (59.6% of total stroke deaths). The 2009 overall death rate for stroke was 38.9. Death rates were 36.6 for white females, 50.2 for
black females, 28.0 for Hispanic females, 29.6 for Asian/Pacific Islander females, and 24.6 for American Indian/Alaska Native females.
In 2010, 530,000 females were discharged from short-stay hospitals after having a stroke. High Blood Pressure (HBP) (ICD/10 codes I10-I15) (ICD/9 codes 401-404) One in three adults in the United States has HBP. A higher percentage of men than women have HBP until age 45. From 45–64 the percentage for
men and women are similar. After that a much higher percentage of women have HBP than men. Among women age 20 and older, the following have HBP: 30.7% of non-Hispanic whites; 47.0% of
non-Hispanic blacks and 28.8% of Mexican Americans. In 2009, 34,094 females died from HBP. They represented 55.2% of deaths from HBP. The 2009 overall death rate from HBP was 18.5. Death rates were 14.4 for white females and 38.3
for black females. 272,000 females diagnosed with HBP were discharged from short-stay hospitals in 2010. Heart Failure (HF) (ICD/10 code I50.0) (ICD/9 code 428.0) About 2.4 million females alive today have HF. Each year, about 320,000 new cases are diag-
nosed in females. In 2010, the overall prevalence for people age 20 and older is 2.1%. Among women, the follow-
ing have HF: 1.7% of non-Hispanic whites; 3.0% of non-Hispanic blacks and 1.1% of Mexican Americans.
In 2009, there were 32,847 female deaths from HF (58.2% of HF deaths). The 2009 overall any- mention death rate from HF was 82.3. Death rates were 72.2 for white fe-
males and 79.7 for black females. 522,000 females diagnosed with HF were discharged from short-stay hospitals in 2010. Smoking In 2011:
Females students (grades 9-12) were less likely than male students to smoke cigarettes (16.1% vs. 19.9%), smoke cigars (8.0% vs. 17.8%), or use smokeless tobacco (2.2% vs. 12.8%).
Among adults, 21.3% of men and 16.7% of women smoke cigarettes. High Blood Cholesterol and Other Lipids Among children 4 to 11 years of age, the mean total blood cholesterol level is 161.9 mg/dL.For
boys, it is 162.3 mg/ dL; for girls, it is 161.5 mg/dL. Among adolescents 12 to 19 years of age, the mean total blood cholesterol level is 158.2 mg/dL.
For boys, it is 156.1 mg/dL; for girls, it is 160.3 mg/dL.
Women & CVD - 2013 Statistical Fact Sheet
©2013 American Heart Association, Inc. All rights reserved. Unauthorized use prohibited.

22
Women & CVD - 2013 Statistical Fact Sheet
©2013 American Heart Association, Inc. All rights reserved. Unauthorized use prohibited.
For additional information, charts and tables, see Heart Disease & Stroke Statistics - 2013 Update.
Additional charts may be downloaded directly from the online publication at: http://circ.ahajournals.org/lookup/doi/10.1161/CIR.0b013e31828124ad Or at: www.heart.org/statistics The American Heart Association requests that this document be cited as follows: Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Magid D, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, Moy CS, Mussolino ME, Nichol G, Paynter NP, Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani SS, Wong ND, Woo D, Turner MB; on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2013 update: a report from the American Heart Association. Circulation. 2013; 127:e6-e245. If you have questions about statistics or any points made in the 2013 Statistical Update, please contact the American Heart Associ-ation National Center, Office of Science & Medicine at [email protected]. Please direct all media inquiries to News Media Relations at [email protected] or 214-706-1173.
Among adults age 20 and older: 41.3% of men and 44.9% of women have total cholesterol levels of 200 mg/dL or higher. 12.7% of men and 14.7% of women have levels of 240 mg/dL or higher. 31.9% of men and 30.0% of women have an LDL cholesterol of 130 mg/dL or higher. 31.8% of men and 12.3% of women have HDL cholesterol less than 40 mg/dL.
Physical Inactivity Girls are more likely than boys to report inactivity (17.7% vs. 10.0%).
In a study of 12 812 youth 9 to 18 years of age, the physical activity level in boys and girls de-clined starting at the age of 13, with a significantly greater decline in activity among girls.
Only 17.1% of adult women met the 2008 Federal Physical Activity Guidelines in 2011. Overweight and Obesity An estimated 30.4% of girls age 2 to 19 are overweight or obese; 25.6% non-Hispanic whites,
41.3% non-Hispanic blacks, and 38.2% Mexican Americans. Of these girls, 15.0% are obese; 11.7% non-Hispanic whites, 24.3% non-Hispanic blacks, and
18.2% Mexican Americans An estimated 63.7% of women age 20 and older are overweight or obese; 60.2% non-Hispanic
whites, 79.9% non-Hispanic blacks, and 78.2% Mexican Americans. Of these women, 35.6% are obese; 32.5% non-Hispanic whites, 53.9% non-Hispanic blacks, and
44.8% Mexican Americans.
Diabetes Mellitus (ICD/10 codes E10-E14) (ICD/9 code 250) Of the estimated 19.7 million American adults with physician-diagnosed diabetes, about 10.1 mil-
lion are women; 6.2% of non-Hispanic whites, 15.4%of non-Hispanic blacks and 12.0% of Mexican Americans.
Of the estimated 8.2 million Americans with undiagnosed diabetes, about 2.9 million are women; 1.8% of non-Hispanic whites, 2.9% of non-Hispanic blacks and 4.7% of Mexican Americans.
Of the estimated 87.3 million Americans with pre-diabetes, about 33.6 million are women; 30.0% of non-Hispanic whites; 29.0% of non-Hispanic blacks and 31.9% of Mexican Americans.
In 2009, diabetes killed 33,651 females. The overall death rate from diabetes was 20.9. Death rates were 15.7 for white females and 35.9 for black females.
319,000 females diagnosed with diabetes were discharged from short-stay hospitals in 2010.

23
AN INCREDIBLE FIX FOR LOWER BACK PAIN
Mr. Brian Bradley (Ergonomic Instruction)

24
TheRealSourceofHamstringPain
“Stretchingmaytemporarilyrelievetighthamstrings,buttheoriginofthediscomfortcouldbefoundelsewhereinthebody.”
PeteEgoscue
Aclientwrotetoussayinghewashavingterriblestruggleswithhishamstrings.HesaidthathestretchedthemeverydaybutstillenduredterriblepainandaskedifIhadanyrecommendationsoradvice.Well,Ido.Thisone’sforhimandanyoneelsewhosehamstringsarecausingpainorconstantlyfeeltight.PrettymuchallofyouintheDentalfieldhavebeenrotatingandflexingforwardononesideofthepatientfordecades.NowyouarepayingforthispatternandNOWisthetimetoreverseit.Inallcasesofchronicstiffnessortightness,thestiff,tightmuscleisnottheissue.Rather,it’sthesignalthatthebalanceofthemuscleactionhasbeencompromisedandcompensatedfor,probablyforaprolongedperiodoftime,andtheproblemisactuallyelsewhere.Inthecaseofstiffhamstrings,theproblemisabouttheload-bearingjoints,theshouldersandankles,yes,butprimarilythehipsandknees.Thehamstringistightforareasonandwhensomeonetellsyoutojuststretchyourhamstrings,youarejustdoingthesamething

25
everydayandexpectingadifferentresult…Insanity!First,averybriefanatomylesson.Thehamstringisactuallycomprisedofthreemuscles:thebicepsfemoris,thesemitendinosus,andthesemimembranosus.Allthreecrossboththehipandkneejoints,butthelattertwomusclesarealsoinvolvedintherotationoftheknee.Putsimply,becauseoftheirattachments,thehamstringsarenotmeanttobetightandshortonadailybasis,limitingtheirstabilityandmovementroles.
Allmusclesinthebodyrespondtostimulus,soifthehamstringistight,it’sbecauseofthestimulus,orinformation,itisreceivingfromthehipandkneejoints.Inotherwords,ifyouhavechronicallystiffhamstrings,there’snothingwrongwithyourhamstrings.They’redoingonlywhatthehipsandkneestellthemtodo.Theproblemlieswiththehipsandknees,andtheupshotisthattheyarenotbalanced.Hereareacoupleoftestsyoucantrytoseethatthesejointsaren’tbalanced.First,grabapairofshoes,anypairthatyouwearoften—couldbeofficeshoes,runningshoes,tennisshoes,whatever.Placethemtogether,soletosole,andseeifthewearpatternsmeshtogether.Ifyou’rebalanced,theywillmesh,butmyhunchistheydon’t.
Anothertest:throwonapairofshortsandstandinfrontofamirror.Lookatyourknees.You’llmostlikelyseethatoneorevenbothofyourkneesdon’tpoint

26
straightatthemirror;they’returnedtotheside.Oryou’llnoticethatoneorbotharen’tlinedupwiththefeet,meaningyourfootandkneearen’tpointinginthesamedirection.Forinstance,yourfootmightbeanglingouttotherightwhileyourkneestillpointsstraightahead.Again,theproblemisnotthehamstring.Theproblemisthejointsbeingoutofposition,somuchsothatthebodythinksthehamstringneedstobeshortened,whichiswhythehamstringisshorteningandcausingstiffness.(Whichisalsowhyjuststretchingthehamstringisn’tgoingtobringrelief;stretchingdoesn’tengageoradjustthejoints,wheretheproblemis.)Or…theproblemcouldbesomethingelse.AllskeletalmusclesareactivatedbytheCentralNervousSystem,i.e.thenerves.Thehamstringsareinnervatedbyanervethatoriginatesinthelumbarspine,orlowerback.Withthepelvisoutofposition,there’sanimpingementonthesignalofthatnerveactivity,whichmeansthepainyoufeelinyourhamstringscouldreallybeaboutpainyou’refeelingfromyoursciaticnerve.Eitherway,youneedtorepositionandrebalancetheload-bearingjoints,notonlythehipandkneejointsbutalsotheshoulderandanklejointsbecausethebodyisoneunit,andthejointsalltalktoeachother.Theimpingednerveisjustasmuchabouttheshouldersasitisthepelvis,soweneedtoloosenupthemidandupper

27
back,andit’sjustasmuchabouttheanklesasitistheknees.Rememberthattestwiththeshoes?Soanyonehavingproblemswithhamstrings,it’sprobablynotyourhamstrings.It’syourjoints,andyoursolutionisn’tstretchingyourhamstrings.Yoursolutionisbalancingyourbodyandrealigningyourjointssothatyourbodyperformsasasingleunit.KnownastheFatherofPosturalTherapy,PeteEgoscuehashelpedrelievethousandsofpeoplefromtheirchronicpain,includingmanyoftheworld’sleadingathletes.FormoreinformationonPeteandanyofhis25clinicsworldwide,gotoegoscue.comorpriortotheSSCSymposium,youcanemailBrianBradley(SSCPresentor)[email protected].

28
UnderstandingtheSourceofBackPain
Upto85percentofAmericansexperiencebackpainatsomepointintheirlives.Here'sanexplanationofwhysomanyofusaresuffering.
PeteEgoscue
IntheUnitedStates,backpainisthe#1complaintpeoplebringtotheirDoctors.Whatisthecauseofthisbackpainthatissoprevalentinourculture?Greatquestionandtheanswerisverysimple.Let’sdiscussthespinalanatomy.Thehumanspineiscalled“thesegmentedbone,”meaning,it’sabonethatthebodyrecognizesasonebone,inthesamewayitrecognizes,say,thefemur(thigh)orhumerus(upperarm),butunlikethosebones,itissegmented.Aboneinparts,andthosepartsarecalledvertebrae.Thatsaid,whenitcomestofunction,thebodydoesnotrecognizetheindividualpartsofthespine;itstimulatesandrespondstothespineasifitisasingleunit,onelonglonebone.Letscallitareallyflexiblebone.Thatflexiblespineiswhy,regardingrangeofmotion,humanshavemorecapabilitythanallothervertebrates.Themonkey,thezebra,yourpetdog—younameit,theyallhavespineswhosevertebraedonotallowforthefullrangeof

29
motionthatourvertebraeallowfor.Thisisaquintessentialcaseofthewholebeinggreaterthanthesumofitsparts.Butthere’sonecatch:forthatfullrangeofmotion,ourspinemustbeintheshapeofan“S”curve.

30
Whenthespineisan“S”itisconsideredtobeinaneutralposition,anditsloadbearingisdistributedevenlyamongallvertebrae.Asaresult,peoplewiththe“S”spinehavenorestrictionsontheirrangeofmotion,nomatterwhatthey’redoing—standing,sitting,walking,lyingdown,surfing,playingvolleyball,gardening.Peoplewithbackpaindon’thavethatfullrangeofmotion,atleastnotwithoutsomepainofdegreesrangingfromminortodebilitating,andthat’sbecausetheirspinesarenolongerinan“S”position.They’vebeencontortedintovariousforms,somegoingfrombeingan“S”toa“C”(which,amongotherdownsides,isafarlesspopularletteronWheelofFortune).The“C”curvewearetalkingaboutisverypopularamongDentistsandtheirstaff.Theconstantforwardflexionandone-sidedrotationaroundthepatientcreatesthisdysfunctionalpatterninducedcurvature.
Theresult?Chronicandacutepain,performancelimitationsandemotionalstress.
Whenthatspineisnotan“S,”theloadthatitbearsisnolongerevenlydistributedamongallvertebrae.Somevertebraaredoingmorework,moreloadbearing,thantheywereintended,andthat’swhenthevariousformsofbackpaincomein.Buthowdidthespineloseits“S”shape?That’sallaboutthealignmentofourfourload-bearingjoints—the

31
shoulders,hips,kneesandankles,fourtoeachside,eightjointsintotal.Whenthesejointsareproperlyaligned,theysitdirectlyontopofeachother,andallverticalandhorizontalplanesarestraight,andthespineremainsand“S.”
Butwhenthoseloadbearingjointsarenotaligned,that’swhenthebestlaidplansofourhumandesigngoawryandourspinesbecome“C’s”orsomeothershapeandacquireanyrangeofproblemsthatcausetheloadbearingofthespinetobedistributedunevenly.Backpain,andeverythingitrepresents,isnothingmore

32
thanthebodytellingthehostthatheorshecannotloadthespinethewaythespinewasdesignedtoloadinthepositionofthe“S”curve.Why?Becausethebodyisnotalignedandthespinereactsbyalteringitsshapetocompensate,andinthatcompensationcomespain.(Allofthisreferstomostcommonbackpainanddoesnotincludebodiesthatjustsufferedamajortrauma.)Buthere’sthething.Thehumanbodyissoamazingthatthatpainfromcompensationisthebodydoingexactlywhatit’ssupposedtodo.Discsherniatebecausetheycanand,infact,aresupposedtowhenthespineisbeingcompromisedinawaywherethehard,boneytissueissusceptibletoinjury.ButthatherniateddiscisNOTthecauseoftheproblem.ItIStheresultoftheunderlyingproblem.TheirPosture!Themisalignmentisthebody’swayofsignalingtousthatthere’saproblem.Similarly,stenosis(thebonybuildupalongthespinecausingnerveimpingement)issimplyacallousthatthebodyformstoprotectthenerverootfromthefrictionoccurringthroughmisalignment.Again,thestenosisisn’tthecauseoftheproblem.It’stheresultandcouldexplainwhyyourlowbackandneckpainareconstantlygettinginthewayofthelifeyouwanttolive.

33
Andagreatnumberofbacksurgeriestodaydonotaddresstheproblem;theyaddressthesymptom,regrettablyleavingtheoriginalproblemintact.
Thewaytoaddresstheproblemistorebalancethebodyintoproperalignment.Onceyoudothat,thenyourmuscleswilltellyourspinetoreturntoan“S”curve,andanybackpainyoufeltwillbealleviatedbecausealltheweightthatthespineisloadingwillagainbedistributedevenlyamongallthevertebrae.Andthenyoucangetbacktodoingallthethingsyouusedtodothattherestofthemammalworld,withitslessflexiblespine,simplycannot.AtSymposium,youwillhavetheopportunitytodiscussyourposture,painandperformanceissueswithBrianBradley(SSCPresentor)andhisstaff.Ifyouhaveanyquestions,youcanemailhimatbbradley@egoscue.comKnownastheFatherofPosturalTherapy,PeteEgoscuehashelpedrelievethousandsofpeoplefromtheirchronicpain,includingmanyoftheworld’sleadingathletes.FormoreinformationonPeteandanyofhis25clinicsworldwide,gotoegoscue.com.

34

35
A HOPELESS TOOTH IS NOT A USELESS TOOTH
Dr. Marco A. Brindis

36
J Oral Maxillofac Surg67:49-59, 2009, Suppl 3
Orthodontic Tooth Extrusion to EnhanceSoft Tissue Implant Esthetics
Marco A. Brindis, DDS,* and Michael S. Block, DMD†
Purpose: The purpose of this report was to review the published data on orthodontic extrusion andmake recommendations for its use according to the evidence presented, including the technique for useby clinicians.
Materials and Methods: A MEDLINE search was performed to identify reports in referenced journalsin English. These studies were collated and reviewed for clinical and animal data on orthodonticextrusion. In addition, the experiences of our team using orthodontic extrusion was added to theevidence used to make the recommendations.
Results: From this background information, orthodontic tooth extrusion is able to move the soft tissueswhen the sulcular attachment apparatus is intact. Bone formation as the tooth is extruded is dependenton the vector of the movement of the tooth. The rate of tooth extrusion is effected by the bone–toothattachment.
Conclusions: When used as we have described, extrusion can effectively move the facial gingivalmargin to allow for esthetic restoration of implants placed in the extruded tooth position.© 2009 American Association of Oral and Maxillofacial SurgeonsJ Oral Maxillofac Surg 67:49-59, 2009, Suppl 3
The position of the facial gingival margin and thepapilla are critical for an ideal esthetic appearance ofimplant-supported crowns. After placement of thefinal crown on an implant in the anterior maxilla, thefacial gingival margin can recede apically 0.5 to 1.4mm.1-4 This recession usually occurs during the first 3to 6 months after surgery.5 If the pretreatment posi-tion of the gingiva is at the ideal location, or if it isapical to the ideal planned position, the assumedgingival recession will result in an asymmetric es-thetic result. One method to move the soft tissuestoward the incisal edge is orthodontic movement ofthe affected tooth coronally, which will move thesurrounding soft tissues with it, resulting in improved
gingival morphology and position, enhancing the finalrestoration.6-9 The MEDLINE search revealed studieson the histologic changes when a tooth is extrudedand the experience of clinicians with tooth extrusionbefore implant placement. However, no well-con-trolled clinical trials were found, other than case se-ries, to verify the techniques used for this method.
In 1940, Oppenheim10 examined the natural phe-nomenon of eruption in young patients after a toothwas modified by removing the occlusal contacts. Thetooth erupted coronally with bone, increasing theheight of the alveolar crest.10 The coronal movementof teeth has been used to reduce pocket depth andchange the architecture of both hard and soft tissuesof the periodontium.11 Ingber introduced the conceptof force eruption of a tooth to treat isolated, 1- and2-wall infraosseous defects.12 When a root is orth-odontically extruded, the gingiva and supportingstructures will move with the tooth to a positioncoronal to the gingival margin present on the adjacentteeth. This therapy can be used to enhance the finalesthetic result.13
Forced eruption using orthodontic appliances hasbeen used to manage isolated nonrestorable teethbecause of trauma, caries, or iatrogenic dentistry byapical movement of the attached gingiva and thetooth from the alveolar bone. This, in conjunctionwith fibrotomy, allows for creation of the crown mar-gin with a healthy biologic width.13-16 Orthodontictreatment for crown lengthening to increase the fer-
*Assistant Professor, Department of Prosthodontics, Louisiana
State University School of Dentistry, New Orleans, LA.
†Clinical Professor, Department of Oral and Maxillofacial Sur-
gery, Louisiana State University School of Dentistry, New Orleans,
LA; and Private Practice, Metairie, LA.
Drs Brindis and Block state no financial arrangement or affilia-
tion with a corporate organization or a manufacturer of a product
discussed in this article.
Address correspondence and reprint requests to Dr Brindis:
Department of Prosthodontics, Louisiana State University School of
Dentistry, Florida Ave, Room 5465 Box 222, New Orleans, LA
70119;e-mail: [email protected]
© 2009 American Association of Oral and Maxillofacial Surgeons
0278-2391/09/6711-0307$36.00/0
doi:10.1016/j.joms.2009.07.013
49

37
ule effect by exposing sound tooth structure is oneexample of using orthodontic tooth eruption for im-proved patient treatment.17 The period needed forthis type of procedure is 4 weeks, with a 6-weekperiod required for stabilization with passive reten-tion.
The results from animal and clinical studies havesuggested that tooth extrusion produces stretching ofthe supracrestal and principal fibers, resulting in boneformation at the apex and within the alveolarcrest.10,18 After the extrusion process has been com-pleted, the tooth-bone attachment fibers return to thepre-extrusion orientation, and the supracrestal fibersmight remain stretched for longer periods.19 The at-tachment apparatus follows the controlled eruptionof the tooth. Partial fiber resection results in less boneformation at the coronal region of the extrudedtooth.20 Ritchey and Orban21 concluded that as atooth is extruded, the relationship between the alve-olar crest and cementoenamel junction is maintained.
As a tooth is extruded, the mucogingival junctionwill maintain a constant position, with an increasedthickness of the band of keratinized gingiva.22 Whenthe mucogingival junction stays in its original posi-tion, the gingival margin will follow the eruption,creating new keratinized gingiva. Gingival hyperplasiaoccurs, effectively moving the facial gingival margincoronally. By maintaining the soft tissue sulcular at-tachment to the tooth, the gingival margin will movecoronally with the tooth. The soft tissue genesis cov-ering the labial bone defects allows for subsequentbone grafting at extraction after extrusion and anesthetic restoration.
The vector of tooth extrusion is critical to boneformation or the loss of bone on the facial aspect ofthe tooth. Labial bone resorption occurs when thetooth is tipped buccally, placing pressure on the labialbone. If excessive bone resorption occurs, the epithe-lial attachment might move less than the actual toothmovement, with the attachment migrating along theroot surface.19,21,22 Reitan23 suggested that tippingadult teeth facially might cause bone destruction withlittle compensatory bone formation, resulting in rootdehiscence. If the tooth extrusion vector is parallel tothe labial bone, less resorption of the labial bone willoccur. Crestal apposition of the bone can result, with2 to 3 mm of additional bone at the crest.19,22 Crestalbone formation can occur when a tooth is movedvertically; however, if the tooth is moved along aprotrusive vector, the facial aspect of the tooth willplace compression on the labial bone, with loss of thefacial bone.24,25
If the tooth is erupted along its axis, the bone in theinterdental region should follow the tooth movement,relocating the bone on a tooth to within 5 mm of thecontact point, for papilla support. When 1 implant is
proposed adjacent to a tooth with crestal bone apicalto the tooth’s cementoenamel junction, eruption ofthe tooth can be critical for full papilla between thetooth and implant. The bone must be relocated to 5mm from the planned interdental contact.3,6,26-31
Orthodontic Extrusion in ProposedImplant Sites
Tooth extrusion can enhance the soft and hard tissueprofiles before implant placement and restoration.32-39 Atooth is connected to orthodontic appliances and ex-truded under controlled conditions to move the attach-ment apparatus and bone. This provides the necessaryridge morphology for an ideal esthetic restoration. Thenewly formed bone resulting from the orthodontictooth extrusion is viable, as evidenced by the presenceof osteocytes within the bony lacunae.40
After a tooth has been extruded, the placement ofan implant at tooth removal can reduce recession ofthe facial gingival margin2 and shorten the time fromtooth removal to eventual restoration.2,41,42 Whenlabial bone is present, immediate placement of animplant has a high incidence of success without ad-verse effects on the total healing response.2 If, aftertooth extrusion, the labial bone is deficient, thesocket will require grafting and a delayed treatmentprotocol. In a well-controlled prospective clinic trial,gingival recession occurred 1-mm less than when theimplant was placed immediately after tooth extrac-tion using a 1-stage approach.2
If the gingival margin on the tooth to be removedis apical to the planned gingival margin, extrusionof the tooth before its removal is recommended toprovide an ideal soft tissue position. Before extrac-tion of a tooth in the esthetic zone, the facialgingival margin should be at least 2 mm coronal toits planned position after the final crown is placed.This requirement anticipates gingival margin reces-sion during the implant and restorative process. Ifthe patient’s tooth has thin labial bone or thingingiva, most likely the gingival margin will moveapically after the final restoration.1 Therefore,when using orthodontic extrusion, overcorrectionof the gingival margin coronally is one goal to beachieved.43
Orthodontic Forces Necessary forTooth Extrusion
The amount of force necessary to slowly extrude atooth will be dependent on the amount of bone on thetooth to be extruded. Brackets are placed on the tooth tobe extruded and the adjacent teeth sufficient to con-trol the extrusive movement, with no movement ofthe teeth used for anchorage. For extrusion, the
50 ORTHODONTIC TOOTH EXTRUSION AND IMPLANT ESTHETICS

38
forces necessary to move the tooth slowly can be aslow as 25 to 30 g.19 Depending on the length of theroot and the level of ankylosis, the necessary force forextrusion can be as high as 50 to 75 g.44 These valuesare within the range of forces that will produce anoptimal tissue response with bone formation aroundthe tooth.45 When extruding a tooth that has hadprevious root canal therapy and some degree of an-kylosis or dense bone around the tooth, more forcemight be necessary and should be monitored with astress and tension gauge.22
The rate of tooth extrusion has not been well de-scribed in published studies. Slow movement is rec-ommended. The tooth extrusion can be as slow as 1mm/month46; however, tooth extrusion can also beas rapid as 1 mm/week without obvious clinical dam-age to the periodontal ligament space. A period of 3to 6 weeks might be sufficient to extrude a compro-mised tooth in many patients. However, excessiveforce and an accelerated rate of movement results inthe risk of tissue damage and ankylosis.44
In our experience, when less than 5 mm of boneremains at the apical region of the tooth, the tooth canmove quite rapidly with minimal orthodontic force (Fig1). These patients should be seen often, if not daily, tomodify the orthodontic appliance to avoid excessivelyrapid tooth movement because of the minimal boneanchorage on the tooth to be extruded. Because no dataare available from well-documented clinical trials or caseseries, the rate of extrusion should follow these generalprinciples:
1. Avoid moving the tooth faster than the accom-panying movement of the gingiva. The gingivashould move with the tooth.
2. Avoid moving the tooth rapidly, which will re-sult in excessive tooth instability.
3. Move the tooth with maintenance of healthygingiva.
4. Move the tooth without excessive discomfort tothe patient.
5. Move the tooth with constant observation of theincisal edge, which will require modification toavoid traumatic occlusion as the tooth erupts.
6. Move the tooth at a rate that does not move theadjacent teeth used for anchorage.
One of the indications for forced eruption is when thecrown of the tooth is fractured or has severe decay. Inthese cases, it is critical to restore the tooth temporarilyto have a surface to which to attach the brackets. Thistemporary must be at the full contour of the tooth to berestored. This prevents the anchorage teeth from tip-ping toward the semiedentulous space and preservesthe mesiodistal distance (Fig 2).
Stabilization After Tooth Extrusion
After the tooth has been extruded, it should bestabilized to allow for bone maturation. Our sugges-tions for the period necessary for tooth stabilitybefore removal and implant placement have notbeen determined from well-controlled clinical trialsbut from our clinical experience. After active toothmovement has been completed, 6 to 12 weeks ofstabilization is usually needed to allow for toothstability and bone consolidation.44 The interval oftooth stabilization from extrusion to tooth removaland implant placement has ranged from 6 to 34weeks.6,14,20,22,46 Confirmation of bone consolida-tion in the gap created by tooth extrusion usingradiography is an objective method to determinewhen it is appropriate to begin the next step. Ingeneral, 12 weeks should be allowed before toothremoval and implant placement, unless bone hasformed earlier.
As soon as is appropriate, the orthodontic appli-ances should be removed and the teeth stabilizedusing traditional dental techniques such as a tem-porary fixed partial denture or bonding. A remov-able orthodontic retainer-type vacuum form canalso be used to stabilize the tooth, or orthodonticwires with a tooth bracketed to the orthodonticwire can be used.
Contraindications for Tooth Extrusion
The contraindications for orthodontic extrusioninclude 1) the presence of chronic, uncontrollableinflammatory lesions, including combined end-odontic-periodontic lesions and fractured roots; 2)an inability to control inflammation and acute in-fection that would adversely affect healing and theoverall response to treatment; 3) an absence ofattachment apparatus because forced eruption onlyrelocates the existing attachment, it does not createa new attachment6; 4) the presence of completebony ankylosis of tooth to be extruded because anattempt to erupt an ankylosed tooth would result inintrusion or undesirable movement of the anchor-age teeth.
Limitations for Orthodontic Extrusion
If the goals for using orthodontic extrusion of atooth before implant placement include improvedgingival margin position or improvement of the un-derlying bone levels, the limitations of extrusion in-clude the following.
In cases of severe gingival recession associated withbone loss close to the tooth’s apex, the final positionof the gingival margin after extrusion might not be
BRINDIS AND BLOCK 51

39
satisfactory to establish ideal final crown esthetics. Incases in which severe circumferential bone loss ispresent, preventing implant placement, orthodonticextrusion will not create adequate vertical bone for-mation for ideal implant positioning. The amount ofvertical bone formation is difficult to predict in some
cases. Any horizontal bone deficiency will not berestored to normal width using orthodontic extru-sion. If the alveolar process is protrusive in shape, theloss of labial bone before and after tooth extrusionmight prevent implant placement at extraction. Fi-nally, a lack of bone density after tooth extrusion may
FIGURE 1. A, Initial presentation of a patient with severe root resorption of her left central incisor and left lateral incisor. Facial gingivalmargins were apical to ideal location and not favorable for an esthetic result. B, Periapical radiograph showing severe resorption and lackof bone at apical region of the maxillary left central and lateral incisors. C, Orthodontic brackets placed on teeth, and extrusion processinitiated. Note slight bend in wire, which will gently extrude left central incisor and lateral incisor. D, Periapical radiograph taken 2 weeksafter tooth extrusion process started. Rapid tooth extrusion occurred secondary to bone tooth attachment. E, After teeth were extruded, theywere stabilized in erupted position for 3 months. Two implants were placed in sequence 6 weeks apart to preserve interdental soft tissue andbone. Healing abutments placed to support soft tissue during integration period. F, Implants were provisionalized with teeth on orthodonticwire. Note improvement of gingival facial margin.
Brindis and Block. Orthodontic Tooth Extrusion and Implant Esthetics. J Oral Maxillofac Surg 2009.
52 ORTHODONTIC TOOTH EXTRUSION AND IMPLANT ESTHETICS

40
necessitate additional hard tissue grafting to preservethe labial ridge form, because thin bone tends toresorb after implant placement.
Orthodontic Tooth Extrusion Technique
PREOPERATIVE CLINICAL EVALUATION
For the esthetic zone, a clinical esthetic analysis,including radiographs, should be performed to iden-tify the proper position of the incisive edge andproper length of the incisor (Figs 3A-C). Establishingthe incisal reference is the first step for a predictableesthetic result.47,48
With the patient’s lips in a relaxed, slightly openedposition, the amount of incisor showing at rest ismeasured and recorded. The desired amount of thecentral incisor showing at rest with the lips apart is 3to 4 mm for females and 2 to 3 mm for males.49 Thesmile line and gingival display are recorded to deter-mine how critical is the position of the gingival mar-gin at the end of treatment. Any deficiencies or excesstooth show is determined and will be used to createan esthetic setup. Once the incisal edge position hasbeen established, a diagnostic cast is mounted withthat reference. Next, with the mounted casts, theesthetic tooth proportion should be established in thediagnostic setup/wax-up (Fig 3D). The tooth propor-
tion is computed by dividing the width of the clinicalcrown by its length. As a rule, a pleasing width-to-length ratio for maxillary central incisors is 75% to80%.47 The length of the esthetic central incisor isgenerally 10.5 to 11.0 mm.47
A diagnostic wax-up is created to establish for thepatient the ideal incisor show and ideal tooth propor-tion, while establishing the ideal gingival plane. Thisinformation is then used to determine the neededposition of the facial gingival margin of the teeth to berestored. Knowing the specific vertical position of theplanned gingival margin determines the implant posi-tion. Using the patient’s current soft and hard tissueprofiles, the need for orthodontic extrusion is con-firmed. The depth of the implant on the anteriormaxilla should be 3 mm from the free gingival margin.This depth allows for development of a proper emer-gence profile for the final crown.43,50
TOOTH PREPARATION BEFOREORTHODONTIC THERAPY
Orthodontic brackets are needed to extrude a toothusing conventional orthodontic wires. The currentstatus of the tooth will dictate the necessary stepsneeded to secure an orthodontic bracket in the cor-rect position on the tooth. A new temporary restora-tion might be necessary (Figs 3E,F). Because of theneed to reduce the incisor edge during the extrusionprocess, root canal therapy might be necessary beforetooth eruption. It is important to plan for tooth lengthreduction to prevent tooth tipping secondary to inap-propriate tooth contact as the tooth erupts.
The diagnostic plan is used to determine the amountof vertical extrusion necessary to achieve the ideal re-sult. Bracket placement should consider the plannedfinal position of the tooth (Figs 3G-J). It might be nec-essary to replace brackets on the extruded tooth tocarefully control the rate of extrusion. The bracketsshould be placed along the cervical margin, planning onits movement during the extrusion.
ANCHORAGE CONSIDERATIONS
Basic orthodontic mechanical considerations mustbe followed for tooth extrusion. Sufficient anchoragemust be established to control the rate and directionof the extrusion, without adverse compensatorymovement of the teeth used as anchors. This canrequire using 3 or more teeth mesial and distal to thetooth to be extruded and might require full archbrackets.34 During the extrusion, the clinician mustexamine the positions of the anchor teeth, noting anyangulation, intrusion, or flaring. If this occurs, theanchorage used was not sufficient and should bereinforced.
FIGURE 2. A, B, By attaching orthodontic bracket to full contouredtemporary crown with appropriate interproximal contacts, adja-cent teeth maintained their orientation without tipping into extrudedtooth space. As a tooth erupted, the full contour was maintainedand might need to be revised as it is shortened owing to verticalmovement of tooth.
Brindis and Block. Orthodontic Tooth Extrusion and ImplantEsthetics. J Oral Maxillofac Surg 2009.
BRINDIS AND BLOCK 53

41
BRACKET POSITION
The brackets should be positioned on the anchor-age teeth to keep these teeth in their original positionand aligned. The tooth that requires extrusion shouldhave the bracket placed as close as possible to the
gingival margin. It is necessary to have an adequatesurface and the appropriate bonding techniques tobond the bracket. If an existing crown does not havethe right references and proportions, it should bereplaced with a provisional crown before the forced
FIGURE 3. A, Initial presentation of a patient with severe bone loss on the left central and left lateral incisors. Current crowns were long, withincisal edges against lower lip. At full smile, she showed ideal gingival margin position on her right central incisor, with gingival margin onher left central incisor apical to ideal location. B, Frontal view showing excessive incisal position of left central with facial gingival marginapical to adjacent tooth. Facial gingival margin on right central incisor was at ideal position. C, Periapical radiograph showing bone losspresent on left central incisor and explaining apical position of facial gingival margin. D, Diagnostic wax-up created to establish properincisal edge position, contour, teeth proportions, and gingival margin. E, Crowns removed and temporary build-ups created to receivediagnostic provisional restoration made from diagnostic wax-up. F, Provisional restoration delivered with incisal edge of teeth at propervertical position. Note the apical position of facial gingival margin on left central and lateral incisors. G, Brackets positioned on middle thirdof anchorage teeth and as close as possible to cervical third on teeth to be extruded. Note the slight bend in the wire that will extrude theteeth. (Figure 3 continued on next page.)
54 ORTHODONTIC TOOTH EXTRUSION AND IMPLANT ESTHETICS

42
FIGURE 3 (cont’d). H, A 1-mm incisal reduction made to allow clearance during orthodontic extrusion. I, Gingival recession corrected after2 months of extrusion. J, Defect then overcorrected, anticipating facial gingival margin movement apically after implant and crowns placed.K, Periapical radiograph after orthodontic extrusion stabilized for 3 months. L, Maxillary left central extracted and implant immediatelyplaced. After 2 months, left lateral extracted and implant delivered. Photograph shows both implants with temporary abutments in place after4 months of stabilization with provisional prosthesis. M, Frontal view of smile with new set of temporaries in place, after orthodontic extrusioncompleted. This set of temporaries stabilized erupted teeth, as well as function as immediate provisional restoration after implant placement.N, Temporary abutments modified by placing subgingival resin to simulate tooth-like sulcus anatomy and further develop interdental papilla,enhancing gingival architecture. O, Revised temporary abutments placed in mouth to develop subgingival sulcus anatomy similar to that ofnatural tooth. P, Final soft tissue architecture obtained after 2 months. (Figure 3 continued on next page.)
BRINDIS AND BLOCK 55

43
eruption. In a case that requires extrusion exceeding5 mm, the clinician should plan on replacing thebrackets during the extrusion period to aid in carefulcontrol of the extrusion rate.
Metal or ceramic brackets can be used. The disad-vantage of metal is its appearance. The disadvantageof ceramic brackets is the brittle nature of the ceramicand the cost. The brackets used for orthodontic ex-trusion are those made for the straight wire tech-nique.31 We use ceramic prescription brackets (MBTPrescription, Clarity Brackets; 3M Unitek, St Paul,MN). This bracket has a metal slot, which allowscontrol of the slide of the wire. The wire type isa round, heat-activated, superelastic nickel-titaniumwire. This type of wire retains its memory tostraighten. When connected to the bracket on thetooth to be extruded, the memory of the wire worksto extrude the tooth. To provide slow and controlledmovement, a 0.014- or 0.016-size wire should beused.16,31
To place the bracket, the tooth surface needs to beprepared. A fifth generation bonding agent should beused after applying 37% phosphoric acid for 20 sec-onds. The bonding agent is applied and allowed to dryfor 5 seconds, a second layer is applied and allowed todry for another 5 seconds, and then it is light curedfor 15 seconds. A light-cured composite is used andlight cured for 20 seconds on the bracket.
The wire is measured according to the size of thearch and resized. The ends of the wire are bent to-
ward the tooth surface to avoid mucosa trauma. Thewire is positioned into the bracket slot and securedwith rubber bands. This allows the wire to movefreely, limiting movement of the adjacent anchorageteeth.
CLINICAL CONSIDERATIONS
The use of the nickel-titanium wire will allow con-stant movement of the tooth at a rate inversely relatedto the tooth’s attachment to the bone. The variablesthat provide the clinician with insight on how thetooth will move include the amount of tooth attach-ment to bone, the root length, patient age, and peri-odontal health of the tooth being extruded.
Because each patient will respond in a uniquepattern, we suggest examining the patient the dayafter activation of the orthodontic extrusion to re-evaluate the patient’s response to the extrusivemovement. Very close follow-up is necessary toprevent an unusual rate of tooth movement andpremature contacts that might create a buccal tip-ping action. The rate of tooth eruption will varyfrom one patient to another. If fast movement isnoted, the force must be stopped and the toothallowed to stay in the extruded position for a pe-riod of healing as determined by clinical intuitionand experience. Then, after the attachment fibersare recovered, the extrusion can be continued andshould be closely monitored. This will prevent los-
FIGURE 3 (cont’d). Q, Final abutments designed in wax and CAD/CAM zirconium abutments fabricated. R, After the tissue matured, theteeth were prepared. S, Zirconium crowns (Katana, Noritake, Japan) cemented. Proper symmetry established with clinically acceptableesthetic result and acceptable presence of interimplant papilla. T, Close-up of smile. Improvement of dentilabial relation obtained.
Brindis and Block. Orthodontic Tooth Extrusion and Implant Esthetics. J Oral Maxillofac Surg 2009.
56 ORTHODONTIC TOOTH EXTRUSION AND IMPLANT ESTHETICS

44
ing the sulcular attachments that ultimately deter-mine the movement of the facial gingival margin.
As the tooth erupts and is observed during thefollow-up appointments, the clinician might need tocontinuously create space incisally and lingually topreserve a vertical eruptive force.
Immediately after forced eruption, the crestal fibersremain stretched. Stabilization will allow the forma-tion of crestal bone in most, but not all, cases (Fig3K).
Depending on the specific needs of the patient, thesoft tissue deficit should be overcorrected by 2 to 3mm from the planned final, ideal position of the facialgingival margin (Figs 3I,J). Once the tissue has over-corrected, a period of up to 12 weeks of stabilizationis recommended, depending on the amount of erup-tion obtained and the speed of the tooth extrusion.
IMPLANT PLACEMENT AFTER TOOTH EXTRUSION
Before removing the tooth for implant placement,an assessment of the bone levels must be performed.The labial bone might be missing and will need to bereconstructed before implant placement. At tooth re-moval, an intrasocket graft can be placed, with im-plant placement occurring 4 months after tooth re-moval. A pontic can be placed to support the papilladuring the healing period before implant placement.If the bone is satisfactory at tooth removal, it is ad-vantageous to place the implant at tooth removal.41
Before the surgical procedure, a guide stent is use-ful to allow the surgeon to accurately place the im-plant at the correct angulation and depth. This can bedone with cone-beam computed tomography plan-ning or model-based planning. The depth of implantplacement is determined from the planned final posi-tion of the gingival margin, which should take intoaccount the overcorrection of the facial gingival mar-gin after tooth extrusion. After administration of localanesthesia, a sulcular incision is made and the toothremoved using atraumatic techniques.
To support the soft tissues of the facial gingivalmargin, immediate provisionalization (Figs 3L,M) isrecommended to provide the optimal gingival archi-tecture.51 The provisional is fabricated in the labora-tory to reduce the “chair” time, using the diagnosticwax-up with the established incisal edge position. Atsurgery, the implant is placed and a provisional abut-ment secured to the implant with a screw. The pro-visional is then relined and cemented or screw re-tained. If placement of adjacent implants is planned,an alternative immediate implant placement and pro-visionalization method can be used.52 One tooth isremoved, and the implant is placed and provisional-ized. This method preserves the blood supply to theadjacent interdental bone. After 2 months, the adja-cent second tooth is removed and the second implant
placed and provisionalized. This alternative methodallows for preservation and development of the inter-dental papilla.
After 4 months of healing, the temporary abut-ments are modified to create anatomically correctsubgingival soft tissue architecture (Figs 3N-P). Theprovisional is relined to match the abutment modifi-cations. A final customized impression is made whenthe soft tissue form has been developed to the satis-faction of the restorative clinician and patient. Thefinal abutments are fabricated (Fig 3Q), a new set oftemporaries delivered, and an esthetic analysis per-formed again. Once the soft tissue is stable, a finalabutment level impression is made. The final crownsare then delivered (Figs 3R-T).
Discussion
The benefits of forced eruption before tooth extrac-tion of hopeless teeth are well documented. It is keyin any esthetic situation to be predictable and consis-tent. When considering the orthodontic movement ofa tooth to enhance the esthetic appearance of thefinal restoration, the initial evaluation of the patientshould include the following:
1. An esthetic analysis of the teeth in relation to thepatient’s face and lips.
2. Establishment of the incisal edge position, con-sidering the vertical position and length, thehorizontal location of the incisor edge, and theangulation of the tooth.
3. A thorough evaluation of the periodontal statusof the teeth, including the tooth to be extrudedand the anchorage teeth.
4. Proper mounting and an accepted estheticwax-up to establish the proper tooth propor-tion.
5. Establishment of the ideal gingival margin posi-tion for the proposed restoration.
6. Fabrication of an appropriate provisionalizationusing the diagnostic cast and previous wax-up.
7. Planning for an overcorrection of 2 to 3 mmfrom the programmed final gingival margin po-sition.
In the data reviewed for the present report, nowell-documented evidence was available for the spe-cifics of orthodontic extrusion. Rather, a generallyaccepted consensus of the techniques have been de-cided on the basis of personal experience. No stan-dard clinical protocol has been described for forcederuption before implant placement. However, as ageneral consensus, when an attachment apparatusexists, with apical bone apposition to the tooth andsulcular attachment fibers intact, the keratinized soft
BRINDIS AND BLOCK 57

45
tissue is improved, and crestal bone formation canoccur. If crestal bone formation is not generated, themovement of the gingival margin will allow for suc-cessful bone graft reconstruction before implantplacement.
Our experience has indicated that the period re-quired for tooth extrusion is dependent on the tooth–bone attachment of the tooth to be extruded. A toothwith dense bone surrounding it will require moretime to extrude than will a tooth with minimal re-maining bone, which can be extruded within a fewdays. Close clinical observation is critical to properlyextrude the tooth within an appropriate period.
Because the disadvantages are minimal to extrudinga tooth to enhance the soft tissue profile, cliniciansshould choose this method often. When a tooth hasits facial margin at a level that will result in compro-mised esthetics, the alternatives to orthodontic extru-sion include surgical movement of the tooth with itssurrounding bone. Orthodontic extrusion is a less-morbid procedure than osteotomy. We suggest that,on the basis of our review of the published data,which showed minimal disadvantages to the tech-nique, one should consider this type of procedure inevery case in which a tooth needs to be extracted.
Each case must be approached individually, de-pending on the needs of the patient and the status ofthe teeth. We recommend monitoring each step sev-eral times each week to carefully evaluate the toothmovement and the patient’s response. The rate oftooth movement will be patient-specific. The periodneeded for tooth stabilization will also be patientspecific. After the tooth has been erupted to theprescribed level, it should be stabilized with a provi-sional restoration or orthodontic wires until the boneresponse has matured.
Movement of the facial gingiva is critical for thefinal esthetic result. If the tooth is removed withoutextrusion and re-establishment of the position of thefacial gingival margin, the final result will be cata-strophic for the patient, with a high smile. The needfor orthodontic extrusion should be planned by therestorative member of the team. It is very importantto keep in mind the importance of planning beforeattempting to extract any tooth. That could be thedifference between achieving a perfect final result ora catastrophe. Once the tooth has been removed, theability to use nature’s capacity to grow soft tissue andbone through tooth eruption is gone.
In our clinical experience, we have found that it isnot always possible to build up bone, especially thebuccal plate, because of the thin nature of the corticaltissue. However, the soft tissue formed is absolutelycritical for the success of a preparation implant sightwith bone grafting. The keratinized gingiva aroundthe extruded tooth will have been maintained and, in
occasional cases, widened during the extrusion. Theimproved soft tissue matrix has allowed hard tissuegrafting to achieve a ridge width sufficient for implantplacement.
Orthodontic extrusion is a predictable and re-sourceful method to move the facial gingival marginto a position that can result in an esthetic restoration.We encourage the use of this method when indicatedbecause of the ease of the method and its exceptionalresults.
Acknowledgment
The authors thank Ms Kathy Martello for the artwork in Figure 2.
References1. Small PN, Tarnow DP: Gingival recession around implants: A
1-year longitudinal prospective study. Int J Oral MaxillofacImplants 15:527, 2000
2. Block MS, Mercante D, Lirette D, et al: Prospective evaluationof immediate and delayed provisional single tooth restorations.J Oral Maxillofac Surg 67:89, 2009 (suppl 3)
3. Saadoun AP, LeGall M, Touati B: Selection and ideal tridimen-sional implant position of soft tissue aesthetics. Pract Periodon-tics Aesthet Dent 11:1063, 1999
4. Kois JC: Esthetic extraction site development: The biologicvariables. Contemp Esthet Restorative Pract 2:10, 1998
5. Holst S, Blatz M, Hegenbarth E: Prosthodontic considerationsfor predictable single-implant esthetics in the anterior maxilla.J Oral Maxillofac Surg 63:89, 2005 (suppl 2)
6. Salama H, Salama M: The role of orthodontic extrusive remod-eling in the enhancement of soft and hard tissue profiles priorto implant placement: A systematic approach to the manage-ment of extraction site defects. Int J Periodontics RestorativeDent 13:312, 1993
7. Kokich VG: Esthetics: The orthodontic-periodontic restorativeconnection. Semin OrthoOrthod 2:21, 1996
8. Mantzikos T, Shamus I: Forced eruption and implant site de-velopment: Soft tissue response. Am J Orthod Dentofac Orthop112:596, 1997
9. Ingber JS: Forced eruption: Alteration of soft tissue deformities.Int J Periodontics Restorative Dent 9:416, 1989
10. Oppenheim A: Artificial elongation of teeth. Am J Orthod OralSurg 26:931, 1940
11. Brown S: The effect of orthodontic therapy on certain types ofperiodontal defects. I—Clinical findings. J Periodontol 44:742,1973
12. Ingber JS: Forced eruption: Part I. A method of treating isolatedone and two wall infrabony osseous defects—Rationale andcase report. J Periodontal 45:199, 1974
13. Ingber IS: Forced eruption. Part II. A method of treating non-restorable teeth—Periodontal and restorative considerations. JPeriodontol 47:203, 1976
14. Heithersay GS: Combined enodontic-orthodontic treatment oftransverse root fractures in the region of the alveolar crest. OralSurg Oral Med Oral Pathol 36:404, 1973
15. Chambrone L, Chambrone LA: Forced orthodontic eruption offractured teeth before implant placement: Case report. J CanDent Assoc 71:257, 2005
16. Stern N, Becker A: Forced eruption: Biological and clinicalconsiderations. J Oral Rehabil 7:395, 1980
17. Potashnick SR, Rosenberg ES: Forced eruption: Principles inperiodontics and restorative dentistry. J Prosthet Dent 48:141,1982
18. Wingard BS, Browers GM: The effects on facial bone from facialtipping of incisors in monkeys. J Periodontol 47:450, 1976
19. Reitan K: Clinical and histologic observations on tooth move-ment during and after orthodontic treatment. Am J Orthod53:721, 1967
58 ORTHODONTIC TOOTH EXTRUSION AND IMPLANT ESTHETICS

46
20. Pontoriero R, Celenza F, Ricci G, et al: Rapid extrusion withfiber resection: A combined orthodontic-periodontic treatmentmodality. Int J Periodontics Restorative Dent 5:31, 1987
21. Ritchey B, Orban B: The crests of the interdental alveolar septa.J Periodontol 24:75, 1953
22. Batenhorst KF, Browers GM, Williams JE: Tissue changes re-sulting from facial tipping and extrusion of incisors in mon-keys. J Periodontol 45:660, 1974
23. Reitan K: Some factors determining the evaluation of forces inorthodontics. Am J Orthod 43:32, 1957
24. Kokich VG: Surgical and orthodontic management of impactedmaxillary canines. Am J Orthod Dentofac Orthop 126:278,2004
25. Kokick VG: Maxillary lateral incisor implants: Planning withthe aid of orthodontics. J Oral Maxillofac Surg 62:48, 2004(suppl 2)
26. Tarnow DP, Magner AW, Fletcher P: The effect of the distancefrom the contact point to the crest of bone on presence orabsence of the interproximal dental papilla. J Periodontol 71:546, 2000
27. Salama H, Salama MA, Garber D, et al: The interproximal heightof bone: A guidepost to predictable aesthetic strategies and softtissue contours in anterior tooth replacement. Pract Periodon-tics Aesthet Dent 10:1131, 1998
28. Tarnow DP, Cho SC, Wallace SS: The effect of interimplantdistance on the height of inter-implant bone crest. J Periodon-tol 71:546, 2000
29. Ryser MR, Block MS, Mercante DE: Correlation of papilla to crestalbone levels around single tooth implants in immediate or delayedcrown protocols. J Oral Maxillofac Surg 63:1184, 2005
30. Lin CD, Chang SS, Liou CS, et al: Management of interdentalpapillae loss with forced eruption, immediate implantation androot-form pontic. J Periodontol 77:135, 2006
31. Tal M: Improving soft tissue form around implants via forcederuption. Quintessence Dent Technol 28:112, 2005
32. Mantzikos T, Shamus I: Forced eruption and implant site de-velopment: An osteophysiologic response. Am J Orthod Dento-fac Orthop 115:583, 1999
33. Mantzikos T, Shamus I: Case report: Forced eruption and im-plant site development. Angle Orthod 68:179, 1998
34. Ziskind D, Schmidt A: Forced eruption technique: Rationaleand clinical report. J Prosthet Dent 79:246, 1998
35. Erkut S, Arman A, Gulsahi A, et al: Forced eruption and implanttreatment in posterior maxilla: A clinical report. J ProsthetDent 97:70, 2007
36. Danesh-Meyer MJ, Brice DM: Implant site development usingorthodontic extrusion: A case report. N Z Dent J 96:18, 2000
37. Chambrone L, Chambrone LA: Force eruption of fracture teethbefore implant placement: Case report. J Can Dent Assoc71:257, 2005
38. Holst S, Hegenbarth EA, Schlegel KA, et al: Restoration of anonrestorable central incisor using forced orthodontic erup-tion immediate implant placement, and an all-ceramic restora-tion: A clinical report. J Prosthet Dent 98:251, 2007
39. Nozawa T, Sugiyama T, Yamaguchi S, et al: Buccal and coronalbone augmentation using forced eruption and buccal roottoque: A case report. Int J Periodontics Restorative Dent 23:568, 2003
40. Celenza F: The development of forced eruption as a modalityfor implant site enhancement. Alpha Omegan 90:40, 1997
41. Lazzara RJ: Immediate placement of implants into extractionsites. Oral Maxillofac Surg Clin North Am 3:921, 1991
42. Barzilay I, Gaser GN, Caton J, et al: Immediate implantation ofpure titanium threaded implants into extraction socket. J DentRes 67:234, 1988
43. Saadoun AP, LeGall M, Touati B: Selection and ideal tridimen-sional implant position for soft tissue aesthetics. Pract Peri-odontics Aesthet Dent 11:1063, 1999
44. Proffit WR: Contemporary Orthodontics (ed 4). St. Louis: CVMosby, 2006
45. Burstone CJ, Groves MH: Threshold and optimum force valuesfor maxillary anterior tooth movement. J Dent Res 39:695,1961
46. Buskin R, Castellon P, Hochstedler JL: Orthodontic extrusionand orthodontic extraction in preprosthetic treatment usingimplant therapy. Pract Periodontics Aesthet Dent 12:213, 2000
47. Chiche GJ, Pinault A: Esthetics of Anterior Fixed Prosthodon-tics. Chicago: Quintessence, 1994, pp 13-32
48. Cohen M (ed): Interdisciplinary Treatment Planning, Princi-ples, Design, Implementation. Chicago: Quintessence, 2008
49. Vig RG, Brundo GC: The kinetics of anterior tooth display. JProsthet Dent 39:502, 1978
50. Kois JC, Kan JY: Predictable peri-implant gingival aesthetics:Surgical and prosthodontic rationales. Pract Proced AesthetDent 13:691, 2001
51. Saadoun AP: Immediate implant placement and temporizationin extraction and healing sites. Compend Contin Educ Dent23:309, 2002
52. Kan JY, Rungcharassaeng K: Interimplant papilla preservationin the esthetic zone: A report of six consecutive cases. Int JPeriodontics Restorative Dent 23:249, 2003
BRINDIS AND BLOCK 59

47
INFLAMMATORY PERI-IMPLANT DISEASE
Dr. Paul Fletcher

48
CASE REPORT
Resolution of a Peri-Implantitis Defect Using Sterile Saline for ImplantSurface Detoxification: A Case Report With Clinical Re-Entry
Paul Fletcher*† and Christos Constantinides*
Introduction: Peri-implantitis is an inflammatory disease involving the soft and hard tissues surrounding a dental im-plant. Its prevalence is increasing, and, if left untreated, it can lead to the loss of the implant. Decontamination of the implantsurface is a primary prerequisite to successfully treat this disease. The best way to accomplish this is still a source of con-troversy. To the best of the authors’ knowledge, this is the first report of a clinical re-entry in a human showing almost com-plete osseous fill of a deep circumferential infrabony peri-implantitis lesion after mechanical debridement with a curet andchemotherapeutic detoxification with only sterile saline.
Case Presentation: A patient presenting with an infrabony peri-implantitis lesion was treated with mechanical de-bridement with a curet and chemotherapeutic detoxification of the implant surface with sterile saline, followed by osseousgrafting and guided bone regeneration in an effort to eliminate the defect. At the completion of treatment, after clinical re-entry, there was almost complete fill of the infrabony component of the osseous defect with a bone-like material that closelyapproximated the implant surface.
Conclusion: It is possible to effectively clean a dental implant surface using onlymechanical debridement with a curetand chemotherapeutic detoxification with sterile saline on a cotton pellet to an extent that will allow for fill of the infrabonycomponent of an osseous defect after the use of regenerative therapy. Clin Adv Periodontics 2015;5:235-241.
Key Words: Bone regeneration; bone transplantation; decontamination; dental implants; peri-implantitis.
BackgroundZitzmann and Berglundh1 defined peri-implantitis as aninflammation of the peri-implant tissues along with break-down of the alveolar bone.
Initially, it was believed that the peri-implantitis lesionwas similar to periodontitis,2 but histopathologic studiesshowed distinct differences. Specifically, in periodontitis,there is a “self-limiting” response to the progression of
the inflammation, evidenced by the presence of a connec-tive tissue (CT) capsule separating the inflammatory cell
infiltrate from the bone.3 This capsule is absent in peri-
implantitis, allowing the inflammatory infiltrate to become
more widespread and penetrate further apically.4
Much of the research on the treatment of peri-implantitisis relatively short term, consisting of follow-ups of£3 years.5Additionally, there are variations between studies, including
disagreement as to the threshold of bone loss used in defin-
ing the disease, differences in surface texture of the implants,
and variations in the configuration of the osseous defects.1
Adequate decontamination of an implant surface is of pri-mary importance in obtaining resolutionof a peri-implantitisdefect. Multiple decontamination protocols were presentedin the literature.6-11 Persson et al.6 in an animal study showed
* Division of Periodontics, Columbia University College of Dental Medicine,New York, NY.
† Private practice, New York, NY.
Submitted March 23, 2014; accepted for publication May 11, 2014
doi: 10.1902/cap.2014.140020
Clinical Advances in Periodontics, Vol. 5, No. 4, November 2015 235
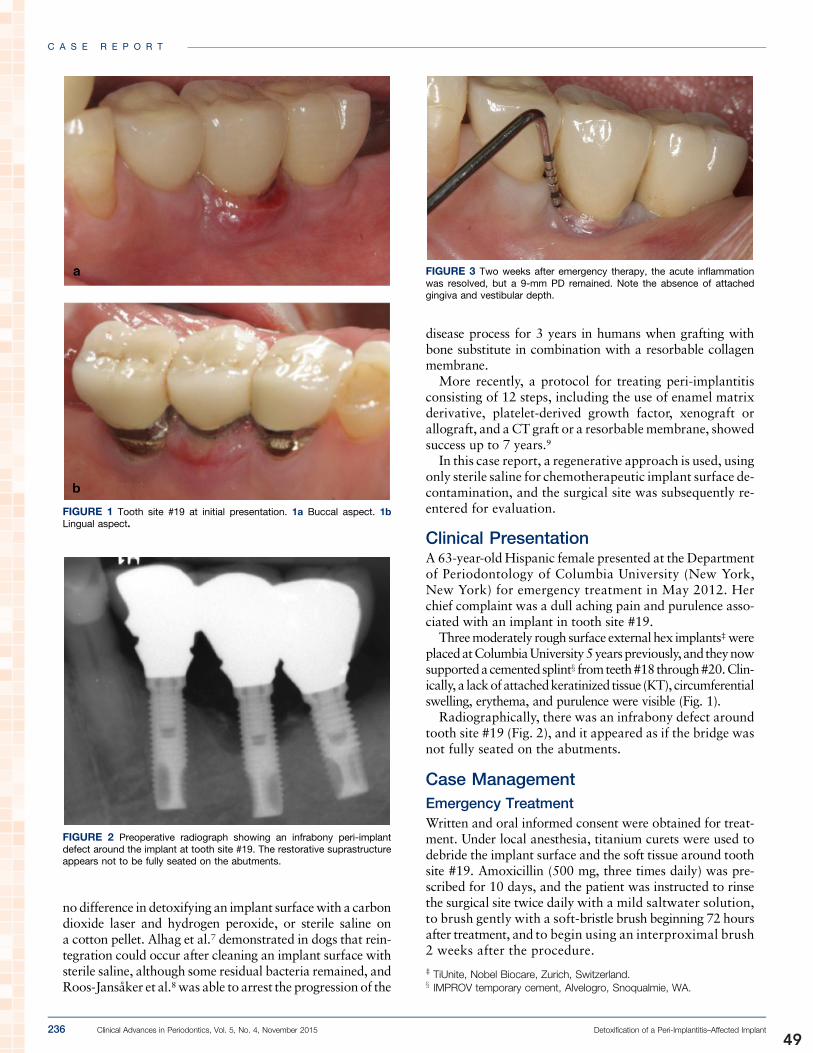
49
nodifference in detoxifying an implant surfacewith a carbondioxide laser and hydrogen peroxide, or sterile saline ona cotton pellet. Alhag et al.7 demonstrated in dogs that rein-tegration could occur after cleaning an implant surface withsterile saline, although some residual bacteria remained, andRoos-Jansaker et al.8was able to arrest the progression of the
disease process for 3 years in humans when grafting withbone substitute in combination with a resorbable collagenmembrane.
More recently, a protocol for treating peri-implantitisconsisting of 12 steps, including the use of enamel matrixderivative, platelet-derived growth factor, xenograft orallograft, and aCT graft or a resorbablemembrane, showedsuccess up to 7 years.9
In this case report, a regenerative approach is used, usingonly sterile saline for chemotherapeutic implant surface de-contamination, and the surgical site was subsequently re-entered for evaluation.
Clinical PresentationA 63-year-oldHispanic female presented at the Departmentof Periodontology of Columbia University (New York,New York) for emergency treatment in May 2012. Herchief complaint was a dull aching pain and purulence asso-ciated with an implant in tooth site #19.
Threemoderately rough surface external hex implants‡ wereplacedatColumbiaUniversity5yearspreviously, and theynowsupportedacementedsplintx fromteeth#18through#20.Clin-ically, a lackofattachedkeratinized tissue (KT), circumferentialswelling, erythema, and purulence were visible (Fig. 1).
Radiographically, there was an infrabony defect aroundtooth site #19 (Fig. 2), and it appeared as if the bridge wasnot fully seated on the abutments.
Case ManagementEmergency TreatmentWritten and oral informed consent were obtained for treat-ment. Under local anesthesia, titanium curets were used todebride the implant surface and the soft tissue around toothsite #19. Amoxicillin (500 mg, three times daily) was pre-scribed for 10 days, and the patient was instructed to rinsethe surgical site twice daily with a mild saltwater solution,to brush gently with a soft-bristle brush beginning 72 hoursafter treatment, and to begin using an interproximal brush2 weeks after the procedure.
FIGURE 1 Tooth site #19 at initial presentation. 1a Buccal aspect. 1bLingual aspect.
FIGURE 2 Preoperative radiograph showing an infrabony peri-implantdefect around the implant at tooth site #19. The restorative suprastructureappears not to be fully seated on the abutments.
FIGURE 3 Two weeks after emergency therapy, the acute inflammationwas resolved, but a 9-mm PD remained. Note the absence of attachedgingiva and vestibular depth.
‡ TiUnite, Nobel Biocare, Zurich, Switzerland.x IMPROV temporary cement, Alvelogro, Snoqualmie, WA.
C A S E R E P O R T
236 Clinical Advances in Periodontics, Vol. 5, No. 4, November 2015 Detoxification of a Peri-Implantitis–Affected Implant

50
Surgical ProcedureTwoweeks after the emergency treatment, the swellingwasreduced, and purulence was no longer evident. Becausethere was still a 9-mmprobing depth (PD), an incompletely
seated bridge (Fig. 3), and radiographic bone loss, it wasdecided to treat the area surgically in an attempt tomitigatethe effect of the subgingival open margin while simulta-neously resolving the pocketing and infrabony defect.
After an unsuccessful attempt to remove the crowns, buc-cal and lingual sulcular incisions were placed from teeth #18through #20, and full-thickness flaps were elevated. Tita-nium curets were used for soft tissue degranulation and tomechanically debride the implant surface, and copious irri-gationwith sterile saline from amonojet syringewas used todilute the microbial concentration in the defect and on theimplant to a subinflammatory level. The implant threadsand collar were then meticulously burnished with sterile sa-line on a small cotton pellet for additional detoxification.Af-ter degranulation, a circumferential infrabony defect wasvisible (Fig. 4). Because of the configuration of the defect,12
it was decided to use a regenerative approach to treat it.A microparticle size calcium sulfate (crystal range: 200
to 900 nm)|| was used as a grafting material (Fig. 5a).A porcine-derived collagen extracellular membrane{ wasused as an occlusive barrier and was placed buccally and
FIGURE 4 The configuration of the residual defect was amenable to grafting.A regenerative approach was used. 4a Buccal aspect. 4b Lingual aspect.
FIGURE 5a Calcium sulfate was placed in the defect. 5b A porcinecollagen barrier membrane was placed buccally and lingually.
|| NanoGen, Orthogen, Springfield, NJ.{ DynaMatrix, Keystone Dental, Burlington, MA.
C A S E R E P O R T
Fletcher, Constantinides Clinical Advances in Periodontics, Vol. 5, No. 4, November 2015 237

51
lingually (Fig. 5b). Because it was the patient’s preference notto replace the fixed splint, the flap was consequently posi-tioned apical to the crown margin to eliminate the con-tribution of the margin to the inflammatory process.Closure was achieved with 4-0 polyglactin interruptedsutures# (Fig. 6a). Amoxicillin (500 mg) and metronidazole(500 mg) were prescribed three times daily for 10 days. Thepatient was advised not to brush the surgical site for 2 weeksand to rinse with 0.12% chlorhexidine for 30 seconds twicedaily. Figure 6b shows an immediate postoperative radio-graph of the grafted site.
Clinical OutcomesThe patient was seen 2 and 4weeks after surgery and at sub-sequentmonthly follow-up appointments.Maintenancewasperformed every 3months. Her home care was excellent, be-cause there was no evidence of plaque around the implant atall post-treatment visits.
Clinically, the crown margins were supragingival; therewere 3-mm PDs, and there was no bleeding on probing(Fig. 7). A 12-month postoperative radiograph showed whatappeared to be a radiopaque fill of the infrabony componentof the lesion (Fig. 8).
At 12months after surgery, the patient began to complain ofsoft tissue soreness on the buccal aspect. The gingiva had re-ceded 2 mm, and the sulcular margin was slightly retractablebecause of the pull of the shallow vestibule. Because there wasa lack of attached KT, it was decided to deepen the vestibuleusinganapicallypositionedsplit-thickness flapand toaugmentthe attached gingiva with a free gingival graft, while simulta-neously clinically evaluating the results of the previous surgery.
After receiving thepatient’s informedconsent andafter theadministration of local anesthetic, a buccal sulcular incisionwith a mesial vertical release was placed. A split-thickness
FIGURE 6a Flap closure with 4-0 interrupted sutures. 6b Immediatepostoperative radiograph.
FIGURE 7a Twelve-month follow-up showing 3-mm PD on the buccalaspect but lack of attached KT and vestibular depth. 7b Less than 3-mmPD on the lingual aspect.
# Coated VICRYL, Ethicon, Johnson & Johnson, Somerville, NJ.
C A S E R E P O R T
238 Clinical Advances in Periodontics, Vol. 5, No. 4, November 2015 Detoxification of a Peri-Implantitis–Affected Implant

52
flap was elevated, with the periosteum on the buccal aspectof tooth site #19 being reflected to allow for visualization ofwhat appeared to be osseous fill of the infrabony componentof the original defect (Fig. 9)with abone-likematerial closelyabutting the implant surface.
DiscussionThe research is clear that implant surface detoxification is ofprimary importance if there is to be any chance of arrestingthe progression of inflammatoryperi-implantitis or of regen-erating bone that was lost previously as a result of the dis-ease.5 The best way to accomplish this is still a source ofcontroversy. In this case, debridement plus thorough cleans-ing of the implant surface with sterile saline seems to havebeen effective in reducing the endotoxin anddiluting thebac-terial concentration to a subinflammatory level so that osse-ous fill occurred and reintegration was possibly achieved.
Although histologic verification of osseous regenerationusing this surface detoxification protocol was shown in
animals,6 without histology, the best that can be claimedin this human case report is radiographic and clinical evi-dence of bone fill, as well as the visible clinical presence ofwhat appears to be close approximation of a bone-like ma-terial to the implant surface.
Calcium sulfate was shown to promote bone formationin both animal and human studies.13-15 It undergoes con-trolled degradation over a period of 10 to 12 weeks, is an-giogenic, and leads to the formation of calcium phosphate,which is the main inorganic component of bone. This sub-sequently serves as amatrix for additional bone deposition.After re-entering this surgical site, a bone-like material wasvisible closely abutting the surface of the implant.
It is hoped the results obtained using this protocol willstimulate additional research in finding a predictable, cost-effective means of decontaminating a peri-implantitis–affected implant surface that would ultimately lead tothe reintegration of bone around an implant. n
FIGURE 8 Twelve-month postoperative radiograph showing bone fill withhomogeneous radiographic appearance. FIGURE 9 Sulcular incision with a mesial vertical release and split-
thickness flap. The periosteum was reflected adjacent to the implant, andclose bone-to-implant contact was visible.
C A S E R E P O R T
Fletcher, Constantinides Clinical Advances in Periodontics, Vol. 5, No. 4, November 2015 239

53
Summary
Why is this case new information? j To the best of the authors’ knowledge, this is the first publishedhuman case report with re-entry clinically showing:
☐ Almost complete osseous fill of the infrabony component of a deepcircumferential peri-implantitis lesion
☐ Apparent close bone-to-implant approximation after mechanicaldebridement and chemotherapeutic surface detoxification with onlysterile saline
What are the keys to successfulmanagement of this case?
j Detoxification of the implant surface using mechanical andchemotherapeutic methods
j Stability of the graft and membranej Exclusion of the epitheliumj Meticulous oral hygiene
What are the primary limitations tosuccess in this case?
j Susceptibility of any exposed threads to plaque accumulation anddifficulty for the patient to keep them clean
j Need for patient compliance
AcknowledgmentThe authors report no conflicts of interest related to thiscase report.
CORRESPONDENCE:Dr. Paul Fletcher, Specialized Dentistry of New York, 150 E. 58th St., Suite3200, New York, NY 10155. E-mail: [email protected].
C A S E R E P O R T
240 Clinical Advances in Periodontics, Vol. 5, No. 4, November 2015 Detoxification of a Peri-Implantitis–Affected Implant

54
References1. Zitzmann NU, Berglundh T. Definition and prevalence of peri-implant
diseases. J Clin Periodontol 2008;35(Suppl. 8):286-291.
2. Mombelli A, van Oosten MA, Schurch E Jr, Land NP. The microbiotaassociated with successful or failing osseointegrated titanium implants.Oral Microbiol Immunol 1987;2:145-151.
3. Lindhe J, Berglundh T, Ericsson I, Liljenberg B, Marinello C.Experimental breakdown of peri-implant and periodontal tissues. Astudy in the beagle dog. Clin Oral Implants Res 1992;3:9-16.
4. Berglundh T, Zitzmann NU, Donati M. Are peri-implantitis lesionsdifferent from periodontitis lesions? J Clin Periodontol 2011;38(Suppl.11):188-202.
5. Esposito M, Grusovin MG, Worthington HV. Treatment of peri-implantitis: What interventions are effective? A Cochrane systematicreview. Eur J Oral Implantology 2012;5(Suppl.):S21-S41.
6. Persson LG, Mouhyi J, Berglundh T, Sennerby L, Lindhe J. Carbondioxide laser and hydrogen peroxide conditioning in the treatment ofperi-implantitis: An experimental study in the dog. Clin Implant DentRelat Res 2004;6:230-238.
7. Alhag M, Renvert S, Polyzois I, Claffey N. Re-osseointegration on roughimplant surfaces previously coated with bacterial biofilm: An experi-mental study in the dog. Clin Oral Implants Res 2008;19:182-187.
8. Roos-Jansaker AM, Lindahl C, Persson GR, Renvert S. Long-termstability of surgical bone regenerative procedures of peri-implantitislesions in a prospective case-control study over 3 years. J Clin Peri-odontol 2011;38:590-597.
9. Froum SJ, Froum SH, Rosen PS. Successful management of peri-implantitis with a regenerative approach: A consecutive series of 51treated implants with 3- to 7.5-year follow-up. Int J Periodontics Re-storative Dent 2012;32:11-20.
10. Subramani K, Wismeijer D. Decontamination of titanium implantsurface and re-osseointegration to treat peri-implantitis: A literaturereview. Int J Oral Maxillofac Implants 2012;27:1043-1054.
11. Schwarz F, John G, Mainusch S, Sahm N, Becker J. Combined surgicaltherapy of peri-implantitis evaluating two methods of surface de-bridement and decontamination. A two-year clinical follow up report. JClin Periodontol 2012;39:789-797.
12. Schwarz F, Sahm N, Schwarz K, Becker J. Impact of defectconfiguration on the clinical outcome following surgical regenera-tive therapy of peri-implantitis. J Clin Periodontol 2010;37:449-455.
13. Paolantonio M, Perinetti G, Dolci M, et al. Surgical treatment ofperiodontal intrabony defects with calcium sulfate implant andbarrier versus collagen barrier or open flap debridement alone: A 12-month randomized controlled clinical trial. J Periodontol 2008;79:1886-1893.
14. Pecora G, Andreana S, Margarone JE 3rd, Covani U, Sottosanti JS.Bone regeneration with a calcium sulfate barrier. Oral Surg Oral MedOral Pathol Oral Radiol Endod 1997;84:424-429.
15. Mazor Z, Mamidwar S, Ricci JL, Tovar NM. Bone repair in peri-odontal defect using a composite of allograft and calcium sulfate(DentoGen) and a calcium sulfate barrier. J Oral Implantol 2011;37:287-292.
indicates key references.
C A S E R E P O R T
Fletcher, Constantinides Clinical Advances in Periodontics, Vol. 5, No. 4, November 2015 241

55
SOFT TISSUE MANAGEMENT OF AESTHETIC FAILURE
Prof. Giovanni Zucchelli

56
Coronally advanced flap: amodified surgical approach forisolated recession-type defectsThree-year results
de Sanctis M, Zucchelli G. Coronally advanced flap: a modified surgical approachfor isolated recession type defects. Three-year results. J Clin Periodontol 2007;34: 262–268. doi: 10.1111/j.1600-051X.2006.01039.x.
AbstractBackground: Various modifications of the coronally displaced flap have beenproposed in the literature with the attempt of treating gingival recession with unevenpredictable results. The goal of the present study was to evaluate the effectiveness withrespect to root coverage of a modification of the coronally advanced flap procedure forthe treatment of isolated recession-type defects in the upper jaw.
Methods: Forty isolated gingival recessions with at least 1mm of keratinized tissueapical to the defects were treated with a modified approach to the coronally advancedflap. The main change in the surgical procedure consisted in the modification of flapthickness and dimension of surgical papillae during flap elevation. All recessions fallinto Miller class I or II. The clinical re-evaluation was performed 1 year and 3 yearsafter the surgery.
Results: At the 1-year examination, the average root coverage was 3.72 � 1.0mm(98.6% of the pre-operative recession depth) and 3.64 � 1.1mm (96.7%) at 3 years.The gain in probing attachment amounted to 3.65 � 1.10mm at 1 year and to3.70 � 1.09mm at 3 years. The average increase of keratinized tissue between thebaseline and the 3-year follow-up amounted to 1.78 � 0.90mm. All changes ofkeratinized tissue (difference between baseline and 1 year, baseline and 3 years, andbetween 1 and 3 years) were statistically significant.
Conclusion: The modified coronally advanced surgical technique is effective in thetreatment of isolated gingival recession in the upper jaw.
Key words: aesthetics; gingival recession; rootcoverage; surgery
Accepted for publication 31 October 2006
It has been assessed that gingival reces-sion can be successfully treated irrespec-tive of the technique utilized, providedthat the biologic conditions for accom-plishing root coverage are satisfied: noloss of inter-dental soft and hard tissueheight (Miller 1985).
The selection of the surgical techniquein an attempt to cover a root recessiondepends mainly on the local anatomicalcharacteristics and on the patient’s de-mands. Local characteristics to be evalu-ated are as follows: the dimensions(depth and width) of root exposure, theheight and width of the inter-dental softtissue, the number of recession defectson neighbouring teeth, the presence ofroot caries or cervical abrasions. Also,the height, thickness and colour of thekeratinized tissues apical and lateral tothe root exposure and of the inter-dentalpapillae neighbouring the recession must
be considered. Other soft-tissue charac-teristics to be evaluated in the selectionof the surgical procedure are the depthof the vestibulum and the presence ofmarginal frenuli or muscle insertions(de Sanctis & Zucchelli 1996).
In patients with a residual amount ofkeratinized tissue apical to the recessiondefect, the coronal advanced flap maybe recommended. Optimum root cover-age results, good colour blending of thetreated area with respect to adjacent softtissues and complete recovery of the ori-ginal (pre-surgical) soft tissue marginalmorphology can be predictably accom-
M. de Sanctis1 and G. Zucchelli2
1Departement of Periodontology, Siena
University, Siena, Italy; 2Department of
Stomatology, Bologna University, Bologna,
Italy
Conflict of interest and source of
funding statement
The authors declare that they have noconflict of interest.
The study was self-funded by theauthors and their institution.
J Clin Periodontol 2007; 34: 262–268 doi: 10.1111/j.1600-051X.2006.01039.x
262 r 2007 The Authors. Journal compilation r 2007 Blackwell Munksgaard

57
plished by means of this surgicalapproach (Roccuzzo et al. 2002). Further-more, the post-operative course is lesstroublesome for the patient as othersurgical sites distant from the toothwith recession defect are not involved.
Recently, the coronally advanced flaphas been demonstrated to be very effec-tive in the treatment of multiple reces-sion defects affecting adjacent teethwith obvious advantages for the patientin terms of aesthetics and morbidity(Zucchelli & de Sanctis 2000).
The coronal advanced flap was firstintroduced by Norberg (1926) as an aes-thetic surgical procedure for root cover-age. In a 1958 study, Patur and Glickmanreported that the coronal advancement ofa pedicle flap was not an effective meansof covering exposed root. Hall, in the1989 Proceeding of the World Workshopin Clinical Periodontology, stated that:‘‘these techniques never have achievedgeneral acceptance and fail on a predict-able basis; nevertheless, the goal of such aprocedure elusive as it has been, remainsthe dream of periodontists’’. The coron-ally advanced flap as a root coveragesurgical technique has been evaluatedmore recently by other authors withuncertain results or limited data (Tenen-baum et al. 1980, Allen & Miller 1989,Wennstrom & Zucchelli 1996). Surgicalrecommendation (Allen & Miller 1989)was to utilize such a technique only inthe presence of Miller’s class I rootrecession defect and in the presenceof residual keratinized tissue with thesame height of the depth of the reces-sion. This approach was thus limited toshallow recession depth, i.e. equal to orless than 3mm.
The technique as described by Allen& Miller (1989) consisted of two obli-que incisions, starting from the mesialand distal line angle of the affectedtooth and directed apically in the alveo-lar mucosa; the flap was then elevatedwith a split-thickness approach to pro-tect the underlying bone. Following rootdebridement, the flap was then coronallyadvanced and secured with interruptedsutures.
Zucchelli & de Sanctis (2000) haverecently introduced a modification ofthis procedure to treat multiple recessiondefects. A split–full–split approach wasused to elevate the flap; this permitted tomaintain the maximum soft tissue thick-ness above the root exposure. Coronalmobilization of the flap was achieved bymeans of a superficial incision eliminat-ing lip muscle insertion residing in the
thickness of the flap. The results report-ed from this study indicated that 64 of the73 defects treated for recession show-ed complete coverage (88%); on aver-age, 97% of previously exposed rootsurface was covered with soft tissue.
The aim of the present study wasto evaluate the efficacy of a modifiedapproach of the coronally advanced flapfor treating single-type recession defects.
Material and Methods
Subject and site selection
Forty young subjects (age range 20–38years), systemically and periodontallyhealthy with isolated recession-typedefects in the upper jaw, were enrolledin the study. The participants wereselected on a consecutive basis amongpatients consulting two private prac-tices: one located in Florence and theother in Bologna. A screening examina-tion revealed that all subjects showed anunremarkable medical history and nonehad loss of periodontal support at othertooth surfaces than those showing reces-sion defects.
In order to be included in the study,patients should have at least one recessiondefect with the following characteristics:(1) isolated defect (no recessions inthe neighbouring teeth), (2) class I or IIaccording to the definitions given byMiller (no loss of inter-dental soft andhard tissue height), and (3) recessiondepth (RD) equal to or greater than 2mm.
Following the screening examination,all subjects received a session of pro-phylaxis including instruction in properoral hygiene measures, scaling and pro-fessional tooth cleaning with the use of arubber cup and a low abrasive polishingpaste. At teeth with recession-typedefects, a coronally directed roll techni-que was prescribed, in order to mini-mize the tooth-brushing trauma to thegingival margin. Surgical treatment ofthe recession defects was not scheduleduntil the patient could demonstrate anadequate standard of supra-gingival pla-que control.
Clinical characterization of patients andselected sites
Full-mouth plaque score (FMPS) andlocal plaque score was recorded as thepercentage of total surfaces (four sidesper tooth) that revealed the presence ofplaque (O’Leary et al. 1972). Bleedingon probing was assessed dichotomously
at a force of 0.3N with a manualpressure-sensitive probe. Full-mouthbleeding score (FMBS) and local bleed-ing score was recorded as the percentageof total surfaces (four sides per tooth),that revealed the presence of bleedingupon probing.
The following clinical measurementswere taken 1 week before the surgeryand at the 1- and 3-year follow-up visitsat all treated teeth:
� Recession depth, measured from thecemento-enamel junction (CEJ) tothe most apical extension of thegingival margin.
� Probing pocket depth (PPD), mea-sured from the gingival margin tothe bottom of the gingival sulcus.
� Clinical attachment level (CAL),measured from the CEJ to the bot-tom of the gingival sulcus.
� Keratinized tissue height (KTH)measured from the most apicalextension of gingival margin to themucogingival line.
Surgeries and measurement were per-formed for all the locations by the sametwo operators.
The same single investigator per-formed the clinical measurements atbaseline, at 1 year and at 3 years. Hedid not perform the surgery and wasunaware of the goals of the study. Allmeasurements were performed by meansof a manual probe and were rounded upto the nearest millimetre.
Surgical technique
The design of the flap consisted of thefollowing incisions:
� Two horizontal bevelled incisions(3mm in length), mesial and distalto the recession defect located at adistance from the tip of the anato-mical papillae equal to the depth ofthe recession plus 1mm.
� Two bevelled oblique, slightly diver-gent, incisions starting at the end ofthe two horizontal incisions andextending to the alveolar mucosa.
The resulting trapezoidal-shaped flapwas elevated with a split–full–splitapproach in the coronal–apical direc-tion: the surgical papillae comprisedbetween the horizontal incisions andthe probeable sulcular area apical tothe root exposure were elevated splitthickness keeping the blade almost
Coronally advanced flap 263
r 2007 The Authors. Journal compilation r 2007 Blackwell Munksgaard

58
parallel to the root, and the soft tissueapical to the root exposure was elevatedfull thickness inserting a small perios-tium elevator in to the probeable sulcusand proceeding in the apical direction upto exposing 3–4mm of bone apical tothe bone dehiscence. This was done inorder to include the periostium in thethickness of that central portion of theflap covering the avascular root expo-sure. The releasing vertical incisionswere elevated split thickness keepingthe blade parallel to the bone plane,thus leaving the periostium to protectthe underlying bone in the lateral areasof the flap. Apical to bone exposure flapelevation continued split thickness andfinished when it was possible to movethe flap passively in the coronal direc-tion. In order to permit the coronaladvancement of the flap, all muscleinsertions present in the thickness ofthe flap were eliminated. This wasdone keeping the blade parallel to theexternal mucosal surface. Coronalmobilization of the flap was considered‘‘adequate’’ when the marginal portionof the flap was able to passively reach alevel coronal to the CEJ of the toothwith the recession defect. In fact, theflap should be stable in its final coronalposition even without the sutures.
The root surface was mechanicallytreated with the use of curettes. It mustbe considered that only the portion ofthe root exposure with loss of clinicalattachment (gingival recession1probe-able gingival sulcus/pocket) was instru-mented. Exposed root surfacesbelonging to the area of anatomic bonedehiscence were not instrumented not todamage connective tissue fibres stillinserted in to the root cementum.
The facial soft tissue of the anatomicinter-dental papillae coronal to the hor-izontal incisions was disepithelized tocreate connective tissue beds to whichthe surgical papillae of the coronallyadvanced flap were sutured.
By moving the flap coronally to reachthe tip of the disepitelized anatomicalpapillae, the vestibular soft tissue waspositioned 1mm coronal to the CEJ toaccount for soft tissue shrinkage. Thelocation of gingival margin after sutur-ing has been demonstrated to be posi-tively correlated to recession reduction(Pini Prato et al. 2005)
The suture of the flap started with twointerrupted periosteal sutures performedat the most apical extension of thevertical releasing incisions; then, it pro-ceeded coronally with other interrupted
sutures, each of them directed, from theflap to the adjacent buccal soft tissue, inthe apical–coronal direction. This wasdone to facilitate the coronal displace-ment of the flap and to reduce thetension on the last coronal sling suture.The sling suture permitted to stabilizethe surgical papillae over the inter-den-tal connective tissue bed and allowed fora precise adaptation of the flap marginover the underlying convexity of thecrown (Fig. 1). In fact, in all treatedcases, at the end of the surgery, the flapresided coronal to the cemento-enameljunction.
Post-surgical infection control
Patients were instructed not to brush theteeth in the treated area but to rinse withchlorhexidine solution (0.12%) twicedaily for 1min.
Fourteen days after the surgical treat-ment, the sutures were removed. Plaquecontrol in the surgically treated area wasmaintained by chlorhexidine rinsing foran additional 2 weeks. After this period,the patients were again instructed inmechanical tooth cleaning of the treatedtooth region using a soft toothbrush anda roll technique. All patients were
recalled for prophylaxis 1, 3 and 5weeks after suture removal and, subse-quently, once every 3 months until the1-year examination. In the period com-prised between the 1- and the 3-yearexaminations, patients undertook hygie-nic recall visits every 6 months.
Data analysis
Statistical analysis was performed usinga statistical application software (Stat-graphics 5 plus; Manugistic Inc., Rock-ville, MD, USA).
Two statistical analyses includingmultivariate methods were performed:
� After fitting a general linear model,a multiple regression ANOVA forrepeated measures was used to eval-uate any time-dependent difference(baseline, 1- and 3-year) regardingFMPS, FMBS, recession of the gin-gival margin (REC), PPD, CAL andKTH. The method used to discrimi-nate between the means was Fisher’sleast significant difference (LSD)procedure.
� The same general linear modelwas fitted to relate the difference
Fig. 1. (a) Upper right first pre-molar, pre-surgical. (b) Flap design; two horizontal bevelledincisions, mesial and distal to the recession defect, two bevelled oblique incisions comingfrom the two horizontal, extending to the alveolar mucosa are executed. (c) The flap is raisedwith a split–full–split thickness approach. (d) The anatomical papillae are disepithelized. (e)The flap is coronally advanced and the vertical incisions are sutured. (f) The surgical papillaeare secured to the underlying bed with a suspended suture.
264 de Sanctis & Zucchelli
r 2007 The Authors. Journal compilation r 2007 Blackwell Munksgaard

59
between baseline and 3-year KTH totwo categorical (smoke, and numberof sites/patient) and two continuous(baseline REC and KTH) factors ascovariates (ANCOVA).
Results
Following the initially provided oralhygiene phase as well as at the post-treatment examinations, all subjectsshowed low frequencies of plaque har-bouring tooth surfaces (o20%) andbleeding gingival units (o15%), indicat-ing an acceptable standard of supragin-gival plaque control during the studyperiod. Eight patients were identified assmokers (smoking more than 10 cigar-ettes/day); all other patients did notsmoke.
Forty isolated recession-type defects(in 40 patients) were treated with thecoronally advanced surgical technique.All gingival recessions were located inthe upper jaw. The tooth populationconsisted of incisors (6), cuspids (24)and pre-molars (10).
Clinical measurements
Table 1 gives the baseline, the 1-yearand 3-year mean data for the variousclinical parameters assessed.
At baseline, the average depth of therecession defects was 3.82 � 1.2mm,with a mean clinical attachment lossamounting to 4.96 � 1.3mm. The depthof the recessions ranged from 2 to 6mm.The height of the gingival keratinizedtissue apical to the recession was on theaverage 1.34 � 0.6mm. Fourty-eightpercent of the recession sites had 1mmor less of KTH.
One year and 3 years following theroot coverage procedure, the meanrecession depth was 0.10 � 0.3 and0.18 � 0.6mm, respectively. Hence,the average root coverage was
3.72 � 1.0mm (98.6% of the pre-operative recession) at 1 year and3.64 � 1.1mm (96.7%) at 3 years. Theresults of the multiple regression ANOVA
for repeated measures show a significant(F5 56.45; po0.01) relationship in thetime-dependent variations of RECdepth; in particular, both REC reduc-tions (difference between baseline RECand 1-year REC and between baselineREC and 3-year REC) were statisticallysignificant, while the increase in gingi-val recession that occurred between the1- and the 3-year follow-up visits(0.08 � 0.53mm) was not statisticallysignificant.
Additional information regarding thelong-term effectiveness of the surgicaltechnique used for soft tissue root cover-age comes from the following data: onthe average, 96.7% of the root surfaceinitially exposed due to recession wasstill covered with soft tissue at the3-year examination. At this time point,34 of the 40 treated recession defects(85%) showed complete coverage. Noneof the treated sites showed greaterremaining recession depth than 1.0mm.
PPD remained almost unchanged(mean value � 1mm) in the three(baseline, 1 and 3 years) observationperiods. The results of multiple regres-sion ANOVA for repeated measures showno significant (F5 2.45) relationship inthe time-dependent variations of PPD.
The gain in probing attachmentamounted to 3.65 � 1.1mm at 1 yearand to 3.60 � 1.2mm at 3 years. Theresults of the multiple regression ANOVA
for repeated measures show a significant(F5 30.70; po0.01) relationship in thetime-dependent variations of CAL; inparticular, a significant difference wasfound between the 1- and 3-year valuescompared with the baseline value; whilethe loss of clinical attachment occurredduring the 3-year observation period(0.05 � 0.6mm) was not statisticallysignificant.
Compared with the conditions beforesurgical treatment, the KTH showed anincrease of 0.70 � 0.8mm at 1 year anda further increment of 1.08 � 0.9mmduring the 2-year observation period andamounted to (on average) 3.12 � 0.5mmat 3-year post-treatment. The averageincrease of keratinized tissue betweenthe baseline and the 3-year follow-upamounted to 1.78 � 0.9mm. The resultsof the multiple regression ANOVA forrepeated measures show a significant(F511.79; po0.01) relationship in thetime-dependent variations of KTH. Allchanges of keratinized tissue (differencebetween baseline and 1 year, baseline and3 years and between 1 and 3 years) werestatistically significant.
The results from the ANCOVA showthat the difference between the baselineand 3-year KTH was significantly affect-ed by KTH (F5 137.01; po0.01) andREC (F5 3.71; po0.05) at baseline: inparticular, the 3-year increase in theamount of keratinized tissue was greaterin sites with greater recession depth andlower amount of keratinized tissue atbaseline.
The limited number of subjects smo-kers was not sufficient to perform anyanalysis on this variable.
Discussion
Treatment of gingival recession isbecoming an important issue in clinicalperiodontology due to the increasingdemand for cosmetic treatment. Problemsrelate particularly to the fact that veryoften, the patient exposes only the mostcoronal millimitres of the recession whensmiling. Thus, only surgical proceduresthat provide the clinician with a very highpercent of complete root coverage shouldbe included in the mucogingival plasticsurgical techniques. Moreover, excessivethickness or poor colour blending of thesurgically treated areas, as those resultingfrom soft tissue graft, should be avoided.
The only limiting criteria in utilizinga coronally advanced flap is the need ofa band of at least 1mm of keratinizedtissue; Wennstrom & Zucchelli (1996)have stated that the amount of rootcoverage utilizing coronally advancedflap with or without the presence of aconnective tissue graft will not show anysignificante difference at the 2-year inter-val. More recently, the results from asystematic review on periodontal plasticsurgery (Roccuzzo et al. 2002) statedthat the use of a barrier membrane or
Table 1. Results of the multiple regression ANOVA for repeated measures relating to oral hygieneand clinical parameters (MV � SD in mm)
Baseline 1 year 3 years
FMPS 10.45 � 2.1 (a) 10.28 � 2.3 (a) 10.12 � 1.8 (a)FMBS 12.70 � 2.2 (a) 10.48 � 2.3 (a) 12.18 � 1.8 (a)REC 3.82 � 1.2 (a) 0.10 � 0.3 (b) 0.18 � 0.6 (b)PPD 1.14 � 0.3 (a) 1.21 � 0.2 (a) 1.18 � 0.3 (a)CAL 4.96 � 1.3 (a) 1.31 � 0.5 (b) 1.36 � 0.6 (b)KTH 1.34 � 0.6 (a) 2.04 � 0.8 (b) 3.12 � 0.9 (c)
Different letters indicate a statistically significant difference between groups for each parameter.
FMPS, full-mouth plaque score; FMBS, full-mouth bleeding score; REC, recession of the gingival
margin; PPD, probing pocket depth; CAL, clinical attachment level, KTH, keartinized tissue height.
Coronally advanced flap 265
r 2007 The Authors. Journal compilation r 2007 Blackwell Munksgaard

60
connective tissue, together with a coron-ally advanced flap, do not give betterresults than coronally advanced flapalone when root coverage is considered.
Moreover, patient-related aestheticconsiderations would suggest the utili-zation of surgical techniques that canpredictably obtain complete root cover-age by using the soft tissue adjacentto the defect (de Sanctis & Zucchelli1996).
The results of the present case-seriesstudy indicate that the modified coron-ally advanced surgical approach washighly effective in obtaining root cover-age of isolated type of gingival reces-sion defects and that this successfuloutcome was well maintained for a3-year observation period (Fig. 2). Thistechnique, in fact, resulted, at 1 year, ina very high mean percentage of rootcoverage (98.6%) and complete softtissue root coverage (up to the CEJ)was obtained in the great majority(88%) of treated cases. No statisticallyand clinically significant changes in rootcoverage outcomes were demonstratedat the 3-year re-evaluation visit. At thistime point, 96.7% of the root surfaceinitially exposed due to gingival reces-sion was still covered with soft tissueand 85% of the treated recession defectsshowed complete coverage. The suc-cessful results in terms of root coverageachieved in the present study were asso-ciated with a clinically significant aver-age increase in KTH with no change inPPD; thus, the gain in clinical attach-ment was well maintained during theobservation period.
This rate of long-term successfuloutcomes of the treatment was simi-lar (Wennstrom & Zucchelli 1996,Zucchelli et al. 2004, Del Pizzo et al.2005, Zucchelli & de Sanctis 2005) oreven higher (Caffesse & Guinard 1980,Pini Prato et al. 1996, Al-Hamdan et al.2003, Trombelli et al. 2005) than thatpreviously reported in the literature forother root coverage procedures.
Some clinical and biological advan-tages of the technique adopted in thepresent study might be related to thesplit–full–split flap elevation as alreadysuggested by Zucchelli & de Sanctis(2000): the split-thickness elevation atthe level of the surgical papilla guaran-tees anchorage and blood supply in theinter-proximal areas mesial and distalto the root exposure; the full-thicknessportion, by including the periostium,confers more thickness, and thus betteropportunity to achieve root coverage, to
that portion of the flap residing over thepreviously exposed avascular root sur-face; the more apical split-thickness flapelevation facilitates the coronal displa-cement of the flap. Although the techni-que comprises vertical releasingincisions, these did not result in unaes-thetic scars. These incisions, in fact,were bevelled in such a way that thebone and periosteal tissues were notincluded in the superficial cut and thusdid not participate to the healing pro-cess. On the contrary, the surgical papil-lae, outlined by the horizontal 3mmincisions and by the vertical bevelledincision, were very wide and thus pro-vided a larger area for anchoring the flapto the underlying vascular bed and moretissue to place the coronal sling suture.Furthermore, the partial thickness of thesurgical papillae facilitated the nutri-tional exchanges between them and theunderlying disepitelized anatomicalpapillae and improved the blending (interms of colour and thickness) of thesurgically treated area with respect toadjacent soft tissues.
Another important modification ofthe present surgical technique, withrespect to the previously proposed ones(Patur & Glickman 1958, Allen & Mill-er 1989, Wennstrom & Zucchelli 1996),was that the coronal advancement ofthe flap was not obtained by meansof periosteal incisions but through theelimination of muscle insertionsincluded in the thickness of the flap.This permitted to eliminate lip tensionon the flap, and to displace passively thesoft tissue flap in the coronal position.The flap, in fact, was stable in a positioncoronal to the CEJ even without sutures,because of the absence of muscle pull.
The absence of a wide band of kera-tinized tissue apical to the recessiondefect was considered to be a limitationfor the coronally advanced technique.On the contrary, the present studydemonstrated an inverse relationshipbetween the apico–coronal dimensionof gingival tissue apical to the rootexposure and the increase of keratinizedtissue achieved with the surgery. Threeyears after the surgery, in fact, the
Fig. 2. (a) Upper right first pre-molar, pre-surgical. (b) Root coverage 1 year followingsurgery. (c) Clinical results 3 years after surgery: note the increase in keratinized tissue.
Fig. 3. (a) Upper left cuspid, pre-surgical: note the minimum amount of keratinized tissue.(b) Root coverage 1 year following surgery. (c) Clinical results 3 years after surgery: adramatic increment in keratinized tissue is evident.
266 de Sanctis & Zucchelli
r 2007 The Authors. Journal compilation r 2007 Blackwell Munksgaard

61
increase of keratinized tissue was great-er in sites with greater recession depthand lower amount of keratinized tissueat baseline (Fig. 3). Very similar resultswere obtained in a previous study eval-uating the 5-year outcomes of the cor-onally positioned flap for multiplegingival recession (Zucchelli & deSanctis 2005).
Some hypothesis can be made in anattempt to explain the 1- and 3-yearincrease of keratinized tissue after cor-onally advanced flap: the tendency ofthe mucogingival line, coronally dis-placed by means of surgery, to regainits original, ‘‘genetically determined’’position (Ainamo et al. 1992), or thecapability of the connective tissue,deriving from the periodontal ligament,to participate in the healing processestaking place at the dento-gingival inter-face (Karring et al. 1971, Lundberg &Wennstrom 1988, Pasquinelli 1995).
The long-term increase in KTH wasalso reported by Pini Prato et al. (1996)for GTR-treated gingival recession.Also, in this study, the 18-month growthin KTH was followed by a furtherincrease that occurred in the followingtwo and half years. The similarity in theamount and trend of keratinized tissuechanges obtained after a coronallyadvanced flap with and without the useof a barrier membrane seems to validatethe importance of the tendency of themucogingival junction to regain itsgenetically defined position rather thento attribute a significant role to thegranulation tissue deriving from theperiodontal ligament tissue to increasethe dimension of the gingiva.
Regardless of the biologic principlecapable of explaining the increase ofkeratinized tissue after coronallyadvanced flap, the present data indicatethat a residual wide band of attachedgingival apical to the root exposure isnot required to perform successfully thecoronally advanced flap as a root cover-age surgical technique. On the contrary,once the stability of the soft tissuemargin has been obtained at the levelof the CEJ, the keratinized tissue is ableto increase with time. However, a pre-surgical minimal amount of keratinizedtissue is advocated to provide marginalstability for the surgical flap.
In conclusion, the results of the pre-sent study demonstrated that the mod-ified approach of the coronally advancedflap technique was effective in treatingisolated-type gingival recessions in theupper jaw. Successful results were
achieved at 1 year, both in terms ofaesthetics (root coverage and colourblending with adjacent soft tissues) andincrease of keratinized tissue, and werewell maintained or even improved (interms of height of attached gingiva)during the subsequent 2-year observa-tion period.
References
Ainamo, A., Bergenholtz, A., Hugoson, A. &
Ainamo, J. (1992) Location of the muco-
gingival junction 18 years after apically
repositioned flap surgery. Journal of Clinical
Periodontology 19, 49–52.
Al-Hamdan, K., Eber, R., Sarment, D.,
Kowalski, C. & Wang, H. L. (2003) Guided
tissue regeneration-based root coverage:
meta-analysis. Journal of Periodontology
74, 1520–1533.
Allen, E. P. & Miller, P. D. (1989) Coronal
positioning of existing gingiva: short term
results in the treatment of shallow marginal
tissue recession. Journal of Periodontology
60, 316–319.
Caffesse, R. G. & Guinard, E. A. (1980) Treat-
ment of localized gingival recessions. Part
IV. Results after three years. Journal of
Periodontology 51, 167–170.
Del Pizzo, M., Zucchelli, G., Modica, F., Villa,
R. & Debernardi, C. (2005) Coronally
advanced flap with or without enamel
matrix derivative for root coverage: a 2-year
study. Journal of Clinical Periodontology 32,1181–1187.
de Sanctis, M. & Zucchelli, G. (1996) Soft
tissue plastic surgery in the treatment of
gingival recession. Successful criteria for
root coverage. Parodontologie et d’implanto-
logie orale 15, 7–18.
Hall, W. B. (1989) Gingival augmentation/
Mucogingival surgery. Proceedings of the
World Workshop in Clinical Periodontics;
Section VII:1-15, Princeton, NJ, USA.
Karring, T., Ostergaard, E. & Loe, H. (1971)
Conservation of tissue specificity after het-
erotopic transplantation of gingiva and alveo-
lar mucosa. Journal of Periodontal Research
6, 282–293.
Lundberg, M. & Wennstrom, J. L. (1988)
Development of gingival following surgical
exposure of a facially positioned unerupted
incisor. Journal of Periodontology 59, 652–
655.
Miller, P. D. (1985) A classification of marginal
tissue recession. International Journal
of Periodontics and Restorative Dentistry 5,9–13.
Norberg, O. (1926) Ar en utlakning utan vov-
nadsfortust otankbar vid kirurgisk behandling
av. S. K. Alveolarpyorrhoe? Svensk Tandlae-
kare Tidskrift 19, 171.
O’Leary, T. J., Drake, R. B. & Naylor, J. E.
(1972) The plaque control record. Journal of
Periodontology 43, 38.
Pasquinelli, K. L. (1995) The histology of new
attachment utilizing a thick autogenous
soft tissue graft in an area of deep recession:
a case report. International Journal of
Periodontics and Restorative Dentistry 15,
248–257.
Patur, B. & Glickman, I. (1958) Gingival pedi-
cle flaps for covering root surfaces denuded
by chronic destructive periodontal disease.
Journal of periodontalogy 29, 50.
Pini Prato, G., Clauser, C., Cortellini, P.,
Tinti, C., Vincenzi, G. & Pagliaro, U.
(1996) Guided tissue regeneration versus
mucogingival surgery in the treatment
of human buccal recessions. A 4-year
follow-up study. Journal of Periodontology
67, 1216–1223.Pini Prato, G. P., Baldi, C., Nieri, M.,
Franseschi, D., Cortellini, P., Clauser, C.,
Rotundo, R. & Muzzi, L. (2005) Coronally
advanced flap: the post-surgical position of
the gingival margin is an important factor for
achieving complete root coverage. Journal of
Periodontology 76, 713–722.Roccuzzo, M., Bunino, M., Needleman, I.
& Sanz, M. (2002) Periodontal plastic
surgery for treatment of localized gingival
recessions: a systematic review. Journal
of Clinical Periodontology 29 (Suppl. 3),
178–194.
Tenenbaum, H., Klewansky, P. & Roth, J. J.
(1980) Clinical evaluation of gingival reces-
sion treated by coronally repositioned flap
technique. Journal of Periodontology 51,686–690.
Trombelli, L., Minenna, L., Farina, R. &
Scabbia, A. (2005) Guided tissue regenera-
tion in human gingival recessions. A 10-year
follow-up study. Journal of Clinical Perio-
dontology 32, 16–20.
Wennstrom, J. L. & Zucchelli, G. (1996)
Increased gingival dimensions. A significant
factor for successful outcome of root cover-
age procedures? A 2-year prospective clinical
study. Journal of Clinical Periodontology 23,
770–777.
Zucchelli, G., Cesari, C., Amore, C., Monte-
bugnoli, L. & de Sanctis, M. (2004) Laterally
moved, coronally advanced flap: a modified
surgical approach for isolated recession-type
defects. Journal of Periodontology 75,1734–1741. Erratum in: Journal of Perio-
dontology 2005 76(8):1425.
Zucchelli, G. & de Sanctis, M. (2000) Treat-
ment of multiple recession-type defects in
patients with esthetic demands. Journal of
Periodontology 71, 1506–1514.Zucchelli, G. & de Sanctis, M. (2005) Long-
term outcome following treatment of multiple
class I and II recession defects in esthetic
areas of the mouth. Journal of Perio-
dontology 76, 2286–2292.
Address:
Prof. Massimo de Sanctis
Via Gustavo Modena 10
50121 Florence
Italy
E-mail: [email protected]
Coronally advanced flap 267
r 2007 The Authors. Journal compilation r 2007 Blackwell Munksgaard

62
Clinical Relevance
Scientific rationale for the study: It hasbeen shown that a split–full–splitapproach in coronally advanced flapis a reliable surgical modality toobtain coverage of multiple recessionsand to increase the amount of kerati-nized tissue. It is conceivable thatsimilar results could be obtained witha single tooth approach. Also, long-term results of coronal advanced flapare lacking in the literature. This studyreports the long-term clinical resultsfollowing a modification of the cor-onally advanced flap on single toothrecession type defects utilizing a split–full–split surgical technique.
Principal findings: The average rootcoverage with the modified coronallyadvanced flap was 98.6% of the pre-operative recession at 1 year and96.7% at 3 years. All changes ofkeratinized tissue (difference betweenbaseline and 1 year, baseline and 3years and between 1 and 3 years) werestatistically significant. At 3 years, theincrease in the amount of keratinizedtissue was greater in sites with greaterrecession depth and lower amount ofkeratinized tissue at baseline.Practical implications: This studysupports the effectiveness of a newsurgical approach in the coronal dis-placement of marginal tissue for root
coverage. The described technique ishighly effective in obtaining rootcoverage and maintaining the resultsover a 3-year time period. Also,during the time of observation, itwas possible to evidence an increasein keratinized tissue that was inver-sely related to the pre-surgicalamount. This finding tends to supportthe fact that the absence of a wideband of keratinized tissue apical tothe recession defect is not a limitingfactor in obtaining root coverage.
268 de Sanctis & Zucchelli
r 2007 The Authors. Journal compilation r 2007 Blackwell Munksgaard

63
Patient morbidity and rootcoverage outcome aftersubepithelial connective tissueand de-epithelialized grafts: acomparative randomized-controlled clinical trial
Zucchelli G, Mele M, Stefanini M, Mazzotti C, Marzadori M, Montebugnoli L, deSanctis M. Patient morbidity and root coverage outcome after subepithelial connectivetissue and de-epithelialized grafts: a comparative randomized-controlled clinical trial.J Clin Periodontol 2010; 37: 728–738. doi: 10.1111/j.1600-051X.2010.01550.x.
AbstractAims: The aim of this randomized-controlled clinical trial was to compare the patientmorbidity and root coverage outcomes of a coronally advanced flap (CAF) withconnective tissue (CTG) or de-epithelialized gingival (DGG) grafts.
Methods: Fifty patients with one recession each were treated. In the control group,the CTG was harvested using the trap-door approach while in the test group the CTGresulted from the de-epithelialization of a free gingival graft.
Results: No statistically significant differences were demonstrated between groups inpatients’s pain killer consumption, post-operative discomfort and bleeding. Lowerstress and better ability to chew were demonstrated in the CTG group. Analgesicconsumption increased with increasing height of the graft and in the case ofdehiscence/necrosis of the primary flap. Pain was negatively correlated with theresidual thickness of soft tissue covering the palatal bone. A statistically greaterincrease in buccal soft tissue thickness was observed in the DGG group.
Conclusions: No differences were demonstrated in the post-operative pain and rootcoverage outcome in patients subjected to CAF with CTG or DGG.
Key words: connective tissue graft; esthetics;free gingival graft; gingival recession;mucogingival surgery
Accepted for publication 9 January 2010
A soft tissue graft is a withdrawal of softtissue that is completely detached fromits original donor site and placed in aprepared recipient bed (American Acad-emy of Periodontology 2001). The
palate is the most frequent donor sitefor intra-oral connective tissue (CTG)and epithelialized free gingival (FGG)grafts used for root coverage purpose.
Palatal fibromucosa is characterizedby a dense connective tissue (laminapropria) covered by an orthokeratinizedepithelium (Muller et al. 2000). A layerof fatty and glandular tissue (submuco-sa) of varied thickness is presentbetween the palatal fibromucosa andthe periosteum covering the palatalbone (Harris 2003). A remarkable varia-tion in the histologic makeup of CTG
has been observed (Harris 2003), interms of both the thickness and thepercentage of lamina propria and sub-mucosa. The thickness of palatal fibro-mucosa varies from patient to patientand, in the same patient, from site to siteof the palate (Muller et al. 2000). Palatalthickness (PT) can be clinically deter-mined, at the time of anaesthesia, bypenetrating with an endodontic reamer/needle perpendicular to the palatal boneplate (Studer et al. 1997, Paoloantonioet al. 2002, da Silva et al. 2004, Jolyet al. 2007) The penetration depth can
Giovanni Zucchelli1, Monica Mele1,Martina Stefanini1, ClaudioMazzotti1,Matteo Marzadori1, LucioMontebugnoli1 and Massimo deSanctis2
1Department of Odontostomatology, Bologna
University, Bologna, Italy; 2Department of
Periodontology, Siena University, Siena, Italy
Conflict of interest and source offunding
The authors declare that there is no con-flict of interest concerning the contents ofthe study.This study has been self-supported by theauthors.
J Clin Periodontol 2010; 37: 728–738 doi: 10.1111/j.1600-051X.2010.01550.x
728 r 2010 John Wiley & Sons A/S

64
be measured, by using an endodonticsilicon disk applied to the reamer/nee-dle, as the distance between the siliconring and the tip of the reamer/needle. Anultrasonic device has also been used todetermine soft tissue thickness aroundteeth and implants (Eger et al. 1996,Muller et al. 1999, 2000). A study byEger et al. (1996) showed that a needleand an ultrasonic device yield verysimilar results. In addition to the mea-surement of the distance between theexternal palatal surface and the palatalbone plate, from a clinical standpoint,it is even more important to evaluatethe degree of the palatal soft tissuesresistance to needle penetration. Infact, while the fibromucosa (epitheliumand connective tissue) has a firm con-sistency and thus a resistance is feltduring needle penetration, the fattyand glandular tissues do not offer oppo-sition to the needle and resistance isfelt only at the bone level. This evalua-tion is critical, particularly when con-nective tissue-harvesting procedures arechosen.
Different connective tissue-harvest-ing procedures with the purpose ofachieving primary intention palatalwound healing have been described inthe literature: the most common are thetrap-door approach (Edel 1974) and thesingle-incision technique (Hurzeler &Weng 1999, Lorenzana & Allen 2000).These procedures have the followingcommon characteristics: a primarysplit-thickness access flap elevation,the withdrawal of CTG and the com-plete closure of the palatal wound withthe access flap. The primary objective ofthese techniques is to reduce patientmorbidity by alleviating the post-opera-tive course; however, they need anadequate thickness of the palatal fibro-mucosa to avoid desquamation of theundermined superficial flap due to com-promised vascularization (Edel 1974,Langer & Langer 1985, Jahnke et al.1993).
The FGG surgical wound heals bysecondary intention within 2–4 weeks(Farnoush 1978) and has been consis-tently associated with greater discomfortfor the patient due to post-operativepain and/or bleeding (Farnoush 1978,Jahnke et al. 1993, Del Pizzo et al.2002). However, this technique is easyto perform and can be utilized evenin the presence of a thin palatal fibro-mucosa.
The evidence in the literature evalu-ating differences in patient outcomes
following the CTG and FGG, used forroot coverage procedures, is minimal.Few prospective comparative studies(Del Pizzo et al. 2002, Griffin et al.2006, Wessel & Tatakis 2008) reportedpoorer patient outcomes, specifically, agreater incidence of post-operative pain,for FGG compared with CTG proce-dures. No randomized study has beenperformed comparing both patient androot coverage outcomes after the use ofCTG and de-epithelialized gingival(DGG) grafts for the treatment of gingi-val recessions.
The aim of the present randomized-controlled clinical study was to comparepost-operative morbidity and root cover-age outcomes in patients subjected totrap-door connective tissue (controlgroup) and epithelialized (test group)graft-harvesting techniques for the treat-ment of gingival recession with thebilaminar procedure.
The primary objective of the studywas to demonstrate the superiority interms of the post-operative course andpain of the connective tissue-harvestingtechnique. The secondary goal was tocompare the effectiveness, in terms ofroot coverage and increase in buccalgingival thickness (GT), of CTG, har-vested with the trap-door approach orresulting from the de-epithelialization ofa free gingival graft, used in combina-tion with a coronally advanced flap(CAF) for the treatment of gingivalrecessions.
Material and Methods
Fifty subjects, 22 males and 28 females(age range 21–50 years, mean age34.7 � 6.0 years), were enrolled inthe study. The patients were selected,on a consecutive basis, among indivi-duals referred to the University ofBologna and the University of Siena,Dental School, in the period betweenFebruary 2006 and March 2007. Thestudy protocol, questionnaires andinformed consent, in full accordancewith the ethical principles of theDeclaration of Helsinki of 1975, asrevisited in 2000, were approved bythe Institutional Review Board andreceived the approval by of the localethic committee. All patients agreed toparticipate in the study and signed awritten informed consent according tothe above-mentioned principles. All par-ticipants met the study inclusion criter-ia: single or multiple Miller’s Class I
and II recession defects (X2mm indepth); presence of identifiable cemen-to-enamel junction (CEJ); presence of astep 41mm at the CEJ level and/or thepresence of a root abrasion, but with anidentifiable CEJ, were accepted; perio-dontally and systemically healthy; nocontraindications for periodontal sur-gery and not taking medications knownto interfere with periodontal tissuehealth or healing; no anti-inflammatorydrugs or antibiotics for at least 6months; and no periodontal surgery onthe involved sites. Subjects smokingmore than 10 cigarettes a day wereexcluded. Recession defects associatedwith caries or restoration as well as teethwith evidence of a pulpal pathologywere not included. Molar teeth werealso excluded.
Study design
The study was a double-centre (one inBologna and the other one in Siena),double-blinded, randomized-controlledclinical trial, with a parallel design,comparing CAF with CTG or withDGG for the treatment of gingival reces-sions. In the control group, the CTG washarvested with the trap-door approachwhile in the test group, the CTG resultedfrom the de-epithelialization, using ascalpel blade, of a free gingival graft.Both types of grafts were harvestedfrom the palate.
The study protocol involved a screen-ing appointment to verify eligibility,followed by initial therapy to establishoptimal plaque control and gingivalhealth conditions, surgical therapy, eva-luation of patient morbidity 1 week afterthe surgery, maintenance phase andpost-operative clinical evaluation 1year after the surgery.
Sample size
The study was powered to detect aminimum clinically significantly differ-ent pain killer consumption of 1800mgusing a5 0.05, a power5 85%, ahypothesized within-group sigma of2000mg, obtained from the only pre-vious randomized comparative studies(Wessel and Tatakis) with patient mor-bidity as the primary outcome. As aminimum, 24 patients per treatmentarm would have been required.
Patient morbidity and root coverage outcome after grafts 729
r 2010 John Wiley & Sons A/S

65
Investigator training
All participating investigators wererequired to attend two training andcalibration meetings. The aims of themeetings were to review the objectivesof the study and the protocol, and stan-dardize the case selection, the measure-ment techniques and the surgicalprocedures.
Randomization
Patients were assigned to one of the twotreatment groups using a computer-gen-erated randomization table. All patientsparticipated in the study with a singletooth. Twenty-five teeth were assignedto the control group and 25 teeth to thetest group. In the case of patients pre-senting with multiple recessions, thedeepest one was selected; in the caseof two or more recessions of the samedepth, the selection was performed bytossing a coin. Allocation concealmentwas achieved using a sealed coded opa-que envelope containing the treatmentof the specific subject. The sealed envel-ope containing treatment assignmentwas opened during the surgery immedi-ately before the graft harvesting.
Initial therapy and clinical measurements
Following the screening examination,all subjects received a session of pro-phylaxis including instruction in properoral hygiene measures, scaling and pro-fessional tooth cleaning with the use of arubber cup and a low abrasive polishingpaste. A coronally directed roll techni-que was prescribed for teeth with reces-sion-type defects in order to minimizetoothbrushing trauma to the gingivalmargin. Surgical treatment of the reces-sion defects was not scheduled untilthe patient could demonstrate an ade-quate standard of supragingival plaquecontrol.
All clinical measurements were car-ried out by a single masked examiner(M. M.) at baseline and 1 year after thesurgery. MM did not perform surgeryand was unaware of the treatmentassignment. Before the study, the exam-iner was calibrated to reduce intra-examiner error (k40.75) to establishreliability and consistency.
Full-mouth (FMPS) and the localplaque scores were recorded as thepercentage of total surfaces (fouraspects per tooth) that revealed the pre-sence of plaque (O’Leary et al. 1972).
Bleeding on probing was assesseddichotomously at a force of 0.3N usinga manual pressure-sensitive probe[(PCP-UNC 15 probe tip, Hu Friedy,Chicago, IL), equipped with a Brodonticspring device (Dentramar, Waalwijk,the Netherlands)]. Full-mouth (FMBS)and local bleeding scores were recordedas the percentage of total surfaces (fouraspects per tooth) that revealed the pre-sence of bleeding upon probing.
The following clinical measurementswere taken 1 week before surgery and atthe 1-year follow-up at the midbuccalaspect of the study teeth:
(1) gingival recession depth (RD), mea-sured from the CEJ to the mostapical extension of the gingivalmargin;
(2) probing depth (PD), measured fromthe gingival margin to the bottom ofthe gingival sulcus;
(3) clinical attachment level (CAL),measured from the CEJ to the bot-tom of the gingival sulcus;
(4) height of keratinized tissue (KTH):the distance between the gingivalmargin and the mucogingival junc-tion (MGJ). The MGJ was identifiedby means of Lugol staining
All measurements were performed bymeans of the manual probe and wererounded up to the nearest millimetre:
(5) GT: determined 1.5mm apical tothe gingival margin with a shortneedle for anaesthesia and a 3-mm-diameter silicon disk stop. Theneedle was inserted perpendicular tothe mucosal surface, through thesoft tissues with light pressure untila hard surface was felt. The silicondisk stop was then placed in tightcontact with the soft tissue surfacewith the coronal border overlappingthe soft tissue margin. As the needlewas located in the centre of thesilicon disk, measurement of GTwas performed 1.5mm apical fromthe gingival margin. Once in thecorrect position, the disk was fixedwith a drop of cyanocrylic adhesive;after careful removal of the needle,the penetration depth was measuredwith a calliper accurate to the near-est 0.1mm (Paoloantonio et al.2002, da Silva et al. 2004, Jolyet al. 2007).
Intra-surgical measurement
After local anaesthesia, PT in the areaselected for harvesting the graft wasmeasured. The measurement was madeat the mid palatal location about 1.5mmapical to the gingival margin of theadjacent tooth, by means of the needleused for anaesthesia and a silicon diskstop. The needle was inserted perpendi-cular to the mucosal surface, through thesoft tissues with light pressure until ahard surface was felt. The silicon diskstop was then placed in tight contactwith the soft tissue surface and fixed bya drop of cyanocrylic adhesive; aftercareful removal of the needle, the pene-tration depth was measured with thecalliper.
The thickness of the grafts was mea-sured in both test and control groups justafter being harvested (GRT) and justbefore being sutured (GRTs), after de-epithelialization (in the test group) andremoval of fatty tissue when present. Inthe control group, the thickness of theprimary flap (FT) was measured. Allmeasurements were made 1.5 apical tothe coronal border with the calliper. Thewidth (GRW) (mesial–distal dimension)and the height (GRH) (apical coronaldimension) of the CTG were measuredjust before being sutured with the man-ual probe and rounded up to the nearestmillimetre.
Graft measurements were performedby a different examiner (C. M.).
Patient morbidity
Post-operative pain was indirectly eval-uated on the basis of the mean consump-tion (in mg) of analgesics (ibuprofene)(Wessel & Tatakis 2008, Sanz et al.2009).
Patients’ post-operative discomfort,bleeding, stress and inability to chewwas evaluated with a questionnairegiven to patients 1 week following sur-gery. The questionnaire included theevaluation of the intensity of the givenevent on a visual analogic scale (VAS)of 100mm (Cortellini et al. 2001, 2009).
Discomfort was defined as the levelof soreness/pain experienced by thepatients during the first post-operativeweek due to the palatal wound. Bleedingwas considered to be the prolongedhaemorrhaging during the post-surgicalweek reported by the patients. Stresswas evaluated based on the level ofapprehension and fear experienced bythe patients of jeopardizing the palatal
730 Zucchelli et al.
r 2010 John Wiley & Sons A/S

66
wound. Inability to chew was describedas the level of variation of the patient’seating habits due to the presence of thepalatal wound.
Surgical techniques
All surgeries were performed by twocalibrated expert periodontologists (G.Z. and M. D. S.). G. Z. performed 26surgeries (13 tests and 13 controls) andM. D. S. performed the remaining 24(12 tests and 12 controls). During localanaesthesia (2% lidocain with epinephr-ine at a concentration of 1:100,000), thesurgeon chose the harvesting site on thepalate (pre-molar or molar) on the basisof the amount (PT) and quality (softtissues resistance) of needle penetration.The surgeons were then informed as towhich type of graft harvesting techniqueto perform, trap-door or epithelialized,by opening the envelope labelled, whichcontained the patient’s number with theassigned treatment.
Control group
The surgical technique adopted for har-vesting the CTG in the control groupwas a modification of the trap-doorapproach described by Edel (1974)(Fig. 1). In brief, one horizontal incisionof the same length of the mesial–distaldimension of the graft was traced 1–1.5mm apical to the gingival margin ofthe adjacent teeth. Two vertical releas-ing incisions were performed at the endof the horizontal incisions and wereextended in the apical direction 1mmmore than the apical–coronal dimensionof the graft. The primary flap waselevated split-thickness to maintain auniform thickness throughout the flap.The horizontal incision of the graft wasmade along the horizontal incision ofthe flap with the blade almost perpendi-cular to the underlying bone. Once anadequate soft tissue thickness wasobtained, the blade was rotated in orderto be almost parallel to the externalsurface. The thickness of the graft was
maintained uniform while proceedingapically with the blade. Care was takennot to remove the periosteum protectingthe underlying bone. Once the graft wasremoved, the fatty tissue (yellow incolour) was eliminated. The primaryflap was repositioned and interruptedsingle 6-0 sutures (Vicryl, Johnson &Johnson, Woluwe, Belgium) were madeto achieve complete closure of the pala-tal wound.
Test group
A free (epithelialized) gingival graft washarvested in the test patients (Fig. 2).Two horizontal (the coronal incisionwas performed 1–1.5mm apical to thesoft tissue margin of the adjacent teeth)and two vertical incisions were traced todelimitate the area to be grafted. Alongthe coronal horizontal incision, theblade was oriented almost perpendicularto the bone plate and once an adequatesoft tissue thickness was obtained, it was
Fig. 1. The connective tissue graftharvesting technique. (a) The incision design of the primary access flap. (b) The blade proceeds apicallyparallel to the external palatal surface. (c) Split-thickness flap elevation. (d) The graft is being harvested. The blade proceeds parallel to theexternal surface of the graft in order to maintain a uniform thickness in the graft and to preserve as much soft tissue covering the periosteum aspossible. (e) Soft tissue protecting the bone is left. (f) External surface of the graft facing the covering flap. (g) Internal surface of the graftfacing the root surface. All fatty and glandular tissue has been removed. (h) Complete closure of the palatal wound has been achieved. (i) Aslight dehiscence of the primary flap can be noticed 7 days after the surgery.
Patient morbidity and root coverage outcome after grafts 731
r 2010 John Wiley & Sons A/S

67
rotated in order to be almost parallel tothe superficial surface. The thickness ofthe graft was maintained uniform whileproceeding apically with the blade. Carewas taken not to remove the periosteumprotecting the underlying bone. Oncethe graft was separated, the fatty tissue(yellow in colour) was eliminated. Thepalatal wound was protected withequine-derived collagen (GABA Vebas,San Giuliano Milanese, MI, Italy) main-tained in situ with compressive sling 5-0sutures anchored to the soft tissue apicalto the palatal wound area. The graft wasde-epithelialized with a 15c blade. Thegraft was positioned on a sterile gauzeor a surgical cloth and its surface wasmade wet with a saline solution. A lightwas oriented to be perpendicular to thegraft. The different consistency (epithe-lium is harder and more rough while theconnective tissue is softer and smoother)allowed removal of the epithelium whencutting with the blade kept parallel tothe external surface. The different lightreflection (the epithelium reflects morethan the connective tissue) enabled to
clinically distinguish when the epithe-lium was removed. The de-epithelializa-tion of the graft and the control forepithelium removal were performedunder magnification (4 �) vision.
A bilaminar (CAF1CTG) technique(Zucchelli et al. 1998, 2003) was per-formed in both patient groups to accom-plish root coverage. In brief, exposedroot surfaces were mechanically treatedwith the use of curettes, a trapezoidal flapwas raised split thickness and CTG weresutured at the level of the CEJ. The widthof the graft was chosen according to theamount of tissue required to cover theexposed root and 3mm of connectivetissue mesial and distal to it. The heightof the graft was based on the distancefrom the CEJ to the buccal bone crest.No attempt was made to cover the peri-osteum apical to the bone dehiscence.The remaining buccal soft tissue of theanatomic interdental papillae was de-epithelalized to create connective tissueareas to which the surgical papillae of thecovering flap were sutured. The flap wascoronally advanced, by cutting muscle
insertions present in the thickness of theflap, and sutured with sling suturedanchored around the palatal cingulumof teeth with gingival recessions. At thetime of suturing, the flap should cover thegraft and the flap margin should becoronal to the CEJ of all teeth includedin the flap design. No periodontal dres-sing was applied.
Surgical chair time was measuredusing a chronometer from the first inci-sion to the last suture in both groups.
Post-surgical infection control
Post-operative pain and oedema werecontrolled with ibuprofen. Patientsreceived 600mg at the beginning ofthe surgical procedure. Subsequentdoses were taken only if necessary tocontrol pain. Patients had to record thequantity of analgesics taken during thefirst week post-surgery.
Patients were instructed not to brushtheir teeth in the treated area but to rinsewith chlorhexidine solution (0.12%)three times a day for 1min. One week
Fig. 2. The epithelialized gingival graft harvesting technique. (a) The incision design of the free gingival graft. (b) The blade proceedsapically parallel to the external palatal surface in order to maintain a uniform thickness in the graft. (c) Soft tissue thickness covering theperiosteum has been preserved during the harvesting procedure. (d) Minimal bleeding after removal of the graft due to the superficial wound.(e) External surface of the graft before de-epithelialization. Note the reflection of the light due to the presence of the epithelium. (f) De-epithelialization made with the blade kept parallel to the external surface of the graft. (g) External surface of the graft after de-epithelialization. Note the different light reflection. (h) The palatal wound has been protected with equine-derived collagen maintained in situwith a sling mattress suture. (i) Secondary intention palatal healing 7 days after the surgery. Note the rapid tissue healing.
732 Zucchelli et al.
r 2010 John Wiley & Sons A/S

68
after the surgery, patients were recalledfor a control visit and for the post-operative course evaluation. Fourteendays after the surgical treatment, thesutures were removed. Plaque controlin the surgically treated area was main-tained by chlorhexidine rinsing for anadditional 1 week after suture removal.After this period, patients were againinstructed in mechanical tooth cleaningof the treated tooth using an ultra-softtoothbrush and a roll technique for 1month. During this month, chlorhexi-dine rinsing was used twice a day.Then the patient started to use a soft-toothbrush and chlorhexidine once a dayfor another month. All patients wererecalled for prophylaxis 2 and 4 weeksafter suture removal and, subsequently,once every 2 months until the finalexamination (12 months).
Data analysis
A statistical application software (SAS,version 6.09, SAS Institute, Cary,NC, USA) was used for the statisticalanalysis.
Descriptive statistics were expressedas mean � SD.
Complete coverage was evaluatedafter 1 year by calculating the percen-tage of cases, in each treatment group,with the gingival margin at the level orcoronal to the CEJ.
Percentage of root coverage was cal-culated after 12 months according to thefollowing formula:
ðBaseline RDÞ � ð12-month RDÞðBaseline RDÞ �100
One-way ANOVA was used to evaluatedifferences between the test and thecontrol groups regarding the mean age,mean baseline values of RD, CAL, PD,KTH, GT and the mean surgical chair-time
One-way ANOVA was also used toevaluate differences between the testand the control groups in PT, GRTs,GR width, GR length, depth of thewithdrawal (WD) and residual soft tis-sue thickness (RTT) covering the palatalbone.
General linear models were fittedrelating pain killer consumption (inmg), discomfort (VAS), bleeding(VAS), inability to chew (VAS) andstress (VAS) to the surgical proceduresand the centres as predictive factors, andthe interaction between surgical proce-dures and centres.
One-way ANOVA was used to evaluatethe presence of any significant differ-ence in pain, alarm, bleeding, chewingand discomfort, between the sevenpatients experiencing primary flapdehiscence/necrosis and the test patientsand control patients who did not experi-ence primary flap dehiscence/necrosis.
A general linear statistical model wasfitted relating analgesic consumption toRTT, GR width, GR height and area(molar versus pre-molar) of the with-drawal.
General linear models were alsofitted, and multiple regression ANOVA
for repeated measures with a split-plotdesign was used to evaluate the exis-tence of any significant differenceregarding RD, CAL, PD, KTH and GTbetween techniques (CAF with CTGversus CAF with DGG), time (1 yearversus baseline) and the interactionbetween techniques and time. In caseof significance, the Bonferroni t test wasapplied as a multiple comparison test.
A logistic regression model was fittedto relate complete root coverage as theoutcome variable and techniques (CAFwith CTG versus CAF with DGG),including baseline RD as a confoundingfactor.
A multifactorial ANOVA was per-formed to evaluate the inter-group dif-ference between GT increase at 1 yearand GRTs with GRTs as a covariate.
A linear model was fitted to describethe relationship between pain killer con-sumption (in mg) and surgical time.
Results
Following the initial oral hygiene phaseas well as at the post-treatment exam-inations, all subjects showed low per-centages of plaque harbouring toothsurfaces (FMPSo20%) and bleedinggingival units (FMBSo15%), indicat-ing a good standard of supragingivalplaque control during the study period.
All 50 patients completed the study.In the control group, the mean age of the25 patients (10 males and 15 females)was 32.2 � 7.2 years (range 20–40).Ten maxillary (six canines and fourpre-molars) and 15 mandibular (sixcanines, seven pre-molars and two lat-eral incisor) teeth with gingival reces-sion were treated.
In the test group, the mean age of the25 patients (12 males and 13 females)was 34.2 � 6.8 years (range 22–46).Twelve maxillary (six canines, one lat-eral incisor and five pre-molar) and 13mandibular (seven canines and six pre-molars) teeth with gingival recessionwere treated.
Intra-surgical measurements (Table 1)
The mean PT in the area of the with-drawal, in the control and test groups,were 3.1 � 0.47mm (range 2–4.5mm)and 3.06 � 0.46mm (range 2–4mm),respectively. The difference was notstatistically significant (F5 0.9,p5NS). In the control group, 12 graftswere taken from the pre-molar area(mean PT was 3.32 � 0.38mm, range3–4.5mm) and the remaining 13 fromthe molar area (mean PT was2.89 � 0.50mm, range 2–3.5mm). Inthe test group, 10 grafts were takenfrom the pre-molar area (mean PT was3.2 � 0.53mm; range 2.5–4mm) andthe remaining 15 from the molar area(mean PT was 2.96 � 0.32mm; range2.5–4mm).
In the control group, the mean thick-ness of the graft (GRT) immediately afterbeing harvested was 1.34 � 0.26mm(range 1–1.8mm). After removing thefatty and glandular tissues, the thicknessof the CTG, at the time of suturing(GRTs), was 0.88 � 0.17mm (range0.5–1.2mm). The mean thickness ofthe primary flap was 0.72 � 0.13mm(range 0.5–0.9mm). The mean heightof the CTG (GRH) was 6.16 �0.89mm (range 5–8mm), while the
Table 1. Intra-surgical measurements
Parameters (in mm) Control group Test group F p
PT 3.1 � 0.47 3.06 � 0.46 0.9 NSGRT 1.34 � 0.26 1.32 � 0.16 0.8 NSGRTs 0.88 � 0.17 0.83 � 0.12 1.5 NSGRH 6.16 � 0.89 6.28 � 0.97 0.2 NSGRW 10.72 � 0.84 10.96 � 0.37 1.3 NSWD 2.06 � 0.27 1.32 � 0.16 132.2 o0.01RTT 1.04 � 0.49 1.73 � 0.47 25.6 o0.01
See text for abbreviations.
Significance was obtained from one-way ANOVA statistical analysis.
Patient morbidity and root coverage outcome after grafts 733
r 2010 John Wiley & Sons A/S

69
mean width (GRW) was 10.72 � 0.84mm(range 9–12mm). Complete closure ofthe palatal wound was accomplished inall patients.
In the test group, the mean thicknessof the epithelialized graft (GRT) was1.32 � 0.16mm (range 1–1.6mm). Themean thickness of the graft after de-epithelialization and removal of fattytissue (GRTs) was 0.83 � 0.12mm(range 0.6–1mm). The mean GRH was6.28 � 0.97mm (range 5–8mm), whilethe mean GRW was 10.96 � 0.37mm(range 10–12mm).
No statistically significant differencewas demonstrated between the test andthe control groups in any of the consid-ered dimensions of the CTG at the timeof suturing: thickness (F51.5), width(F51.3) and height (F5 0.2). The depthof the withdrawal (WD), correspondingto the sum between the thickness of theprimary flap and the thickness of the graftimmediately after being harvested(FT1GRT5 2.06 � 0.27mm) in thecontrol group, and to the thickness ofthe epithelialized graft (GRT5 1.32� 0.16mm) in the test group, was sta-tistically greater in the control group(F5132.2, po0.01). In contrast, thedifference between PT and WD, that isthe RTT covering the palatal bone, wasstatistically lower in the control group(F525.6, po0.01). These data indicatedthat, in the control group, a greater depthwas reached in the palate and a lower softtissue thickness covering the bone wasleft during the harvesting procedure.
Surgical chair time
The overall surgical chair-time was sig-nificantly shorter for the test group. Inparticular, the average time needed forperforming the CAF with DGG was35.8 � 3.4min. (range 30–42min.),while the mean time for completing theCAF with CTG was 45.0 � 4.3min.(range 38–55min.). The differencewas statistically significant (F563.8,po0.01). Surgical time was significantlycorrelated with pain killer consumption(in mg) (F5 11.9; po0.01; correlationcoefficient 0.44): analgesic consumptionincreased on increasing the time neededto complete the surgery.
Patient morbidity (Table 2)
Healing was uneventful for all testpatients. In seven (28%) controlpatients, a dehiscence/necrosis of the
primary palatal flap occurred duringthe first healing period (7 days).
The mean pain killer consumption (inaddition to the 600mg ibuprofen givenbefore the surgery) in the control andthe test groups was 2016 � 1896.4mg(range 0–5400mg) and 1656 � 1532.2mg (range 0–4200mg), respectively. Thedifference was not statistically significant(F50.5, p5NS). A separate analysisdemonstrated statistically greater analge-sic consumption in the seven patientsexperiencing primary flap dehiscence/necrosis (4028.5 � 828.8mg) than testpatients with secondary intention palatalhealing and control patients (1233.3 �1587, 8mg) with primary intention pala-tal wound healing (F59.3, po0.01). Incontrast, the difference in analgesic con-sumption between the test patients andthe control patients experiencing primaryintention wound healing was not statisti-cally significant.
A general linear statistical model wasfitted relating analgesic consumption toGRW, GRH, area (molar versus pre-molar) of the withdrawal and to theRTT covering the palatal bone. The R2
statistic indicates that the model as fittedis highly significant and explains 54.9%of the variability in analgesic consump-tion. A significant relationship was foundregarding RTT (F5 14.5, po0.01), GRH(F523.1, po0.01) but not regarding thearea of the withdrawal (F5 1.3, p5NS)and the GRW (F51.1, p5NS). Painkiller consumption increased withincreasing height of the withdrawal andby reducing the thickness of the softtissue still covering the palatal bone.
Very limited post-operative morbid-ity was reported by both patient groups.
No statistically significant differencewas demonstrated between the controland the test patients in terms of post-operative discomfort, (F5 0.1, p5NS)and bleeding (F5 1.2, p5NS)-relatedVAS values.
Statistically significant better resultsin terms of post-operative inability tochew (F5 9.1, po0.01)- and stress
(F5 29.5, po0.01)-related VAS valueswere demonstrated in the control com-pared with the test patients.
Clinical parameters
The descriptive statistics for the clinicalparameters measured at baseline and 12months after surgery for both groups, aswell as the mean differences within andbetween groups, are shown in Table 3.At baseline, there were no statisticallysignificant differences between the twogroups for any of the considered clinicalparameters, indicating that the randomi-zation process had been effective. In thecontrol group, the mean RD was3.4 � 0.86 (range 2–5mm) and themean GT was 0.71 � 0.15. In the testgroup, the mean RD and GT were3.56 � 0.86 (range 2–5mm) and0.75 � 0.15, respectively.
One-year clinical outcome
RD
The results of fitting a general linearstatistical model relating RD to techni-ques, time and the interaction betweentechniques and time showed a high R2
statistic, indicating that the model asfitted is highly significant and explains95.5% of the variability. A significantrelationship was found regarding time(baseline versus 1 year) (F5 904.9,po0.01) in both groups, but not regard-ing the techniques (F5 2.21, p5NS).No statistically significant differencewas demonstrated in the amount ofroot coverage (in mm) between thetwo bilaminar procedures.
The percentage of root coverageamounted to 96.2 � 8.93% in the testgroup and to 92.28 � 13.06% in thecontrol group. Complete root coveragewas achieved in 21 (84%) of the test andin 18 of the control (72%) treateddefects. The results of fitting a logisticregression model, including baselineRD as a confounding factor, showed no
Table 2. Post-operative morbidity
Parameters Control group Test group F p
Pain killer (in mg) 2016 � 1896.4 1656 � 1532.2 0.5 NSDiscomfort (VAS) 2.65 � 2.18 3.1 � 1.99 0.1 NSBleeding (VAS) 2.9 � 2.12 3.65 � 1.89 1.2 NSInability to chew (VAS) 1.95 � 1.87 3.85 � 2.0 9.1 o0.01Stress (VAS) 2.1 � 1.25 4.5 � 1.53 29.5 o0.1
See text for abbreviations.
Significance was obtained from General linear model statistical analysis.
734 Zucchelli et al.
r 2010 John Wiley & Sons A/S

70
significant difference (w2 2.2, p5NS)between the procedures.
CAL
The results of fitting a general linearstatistical model relating CAL to tech-niques, time and the interaction betweentechniques and time showed a high R2
statistic, indicating that the model asfitted is significant and explains 94%of the variability. A significant relation-ship was found regarding time (base-line versus 1 year) (F5 651.2, po0.01)in both groups, but not regarding thetechniques (F5 0.99, p5NS). No sta-tistically significant difference wasdemonstrated in the amount of CALgain between the two bilaminar proce-dures.
PD
The results of fitting a general linearstatistical model relating PD to techni-ques, time and the interaction betweentechniques and time showed a high R2
statistic, indicating that the model asfitted is significant and explains 68.9%of the variability. A significant relation-ship was found regarding time (baselineversus 1 year) (F5 5.77, po0.05) inboth groups, but not regarding the tech-niques (F5 0.36, p5NS).
KTH
The results of fitting a general linearstatistical model relating KTH to tech-
niques, time and the interaction betweentechniques and time showed a high R2
statistic, indicating that the model asfitted is significant and explains 95%of the variability. A significant relation-ship was found regarding time (baselineversus 1 year) (F5 784.5, po0.01) inboth groups, but not regarding the tech-niques (F5 1.92, p5NS). No statisti-cally significant difference wasdemonstrated in the increase in KTHbetween the two bilaminar procedures.
GT
The results of fitting a general linearstatistical model relating GT to techni-ques, time and the interaction betweentechniques and time showed statisticallysignificant differences considering bothtime (F5 915.7, po0.01) (baseline ver-sus 1 year) and the interaction betweentechniques and time (F5 16.2,po0.01). A greater increase in GT wasobserved in the test compared with thecontrol group.
The difference between GT increaseat 1 year and graft thickness at the timeof suturing was statistically significant(F5 56.6, po0.01) between the twogroups independent of the thickness ofthe graft at the time of suturing.
Discussion
Sub-epithelium CTG is the most effec-tive and predictable root coverage sur-gical procedure for the treatment of
gingival recession (Roccuzzo et al.2002, Cairo et al. 2008). CTG harvest-ing techniques are widely recommendedso as not to expose patients to the morepainful post-operative course associatedwith secondary intention palatal woundhealing (Farnoush 1978, Jahnke et al.1993, Del Pizzo et al. 2002, Griffin et al.2006, Wessel & Tatakis 2008). Never-theless, before performing a CTG har-vesting technique, it is mandatory toevaluate the palatal anatomic character-istics and in particular the thickness ofthe palatal fibromucosa avoiding uselessor even harmful surgical procedures.The primary access flap must includeboth epithelium and connective tissuethat is critical for its viability. In someclinical situations, there is not enoughconnective tissue thickness for both theprimary flap and the graft. Based on theclinical experience of the authors, this istrue in the palatal pre-molar area of mostof the patients, where, under a thin layerof connective tissue, there is a thick areaof fatty and glandular tissue, as well asin the molar area of a few patients,where the entire palatal fibromucosa isnot thick enough for obtaining a doublelayer (one for the flap and one for thegraft) of connective tissue. In thesesituations, if the primary access flap isof a proper thickness, there is no con-nective tissue left for performing thegraft. The risk lies in the incorporationof fatty and glandular tissue, inadequatefor root coverage, instead of the con-nective tissue in the buccal aspect ofteeth affected by gingival recession.Sullivan & Atkins (1968) emphasizedthe importance of removing all fattytissue included in the graft that ‘‘couldfunction as a barrier both to diffusionand vascularization’’. On the otherhand, if the primary flap is too thin, itconsists only or prevalently of epithe-lium and might result in necrosis/dehis-cence during the first healing phase. Asa result, the palatal wound heals bysecondary intention. This eventful out-come was reported frequently in theliterature when the trap-door approachwas used as the CTG harvesting techni-que (Edel 1974, Broome & Taggart1976, Jahnke et al. 1993, Harris 1997,Del Pizzo et al. 2002). The present studydemonstrated a statistically significantgreater analgesic consumption in theseven patients (28%) experiencing pri-mary flap dehiscence/necrosis, withrespect to test patients healed by sec-ondary intention and control patientshealed by primary intention. This is in
Table 3. Clinical parameters (mean � SD) at baseline and 12 months post-surgery
Parameter (in mm) Control group (n5 25) Test group (n5 25)
RDBaseline 3.4 � 0.86 3.56 � 0.8612 months 0.32 � 0.55 0.16 � 0.37Difference 3.08 � 0.70 3.4 � 0.81
CALBaseline 4.52 � 0.87 4.72 � 0.8412 months 1.56 � 0.65 1.52 � 0.58Difference 2.96 � 0.78 3.2 � 0.91
PDBaseline 1.12 � 0.33 1.16 � 0.3712 months 1.24 � 0.43 1.36 � 0.48Difference 0.12 � 0.43 0.2 � 0.5
KTHBaseline 1.36 � 0.48 1.52 � 0.5012 months 3.28 � 0.54 3.64 � 0.48Difference 1.92 � 0.49 2.12 � 0.52
GTBaseline 0,71 � 0.15 0.75 � 0.1512 months 1.32 � 0.22 1.55 � 0.21Difference 0.61 � 0.16 0.80 � 0.17
See text for abbreviations.
Patient morbidity and root coverage outcome after grafts 735
r 2010 John Wiley & Sons A/S

71
line with the opinion of several authorsthat indicated the sloughing of the pri-mary flap as the main cause of markedpost-operative discomfort following atrap-door approach (Edel 1974, Jahnkeet al. 1993) and with the study by Harris(1997), which reported an associationbetween extensive flap necrosis andpost-operative pain. More specifically,the data of the present study indicatedmore analgesic intake by patients duringsecondary intention palatal wound heal-ing as a result of flap necrosis/dehis-cence than when it is the result of thewithdrawal of an epithelialized graft.The reasons for this difference areunknown; it can be speculated that themore painful post-operative coursemight derive from sovra infection ofthe wound favoured by tissue necrosisand/or from the greater depth reachedduring the harvesting technique. In fact,when a CTG harvesting technique isperformed, because some connectivetissue has to be left to maintain thevitality of the primary flap, it is neces-sary to extend the dissection deeper intothe palatal soft tissues.
The critical role of the depth of thewithdrawal and in particular of thedifference between PT and the depthof the withdrawal in influencing post-operative pain was one of the mainresults of the present study. The presentstudy demonstrated that the RTT cover-ing the palatal bone was negativelycorrelated with pain killer consumption.These data were statistically significantconsidering both the entire patient sam-ple and the single treatment groups. Inother words, patient analgesic consump-tion was greater in those patients inwhom lower soft tissue thickness cover-ing the bone was left during the harvest-ing procedure. Specifically, all patientsconsuming more than three analgesictablets throughout the post-operativeweek had o2mm thickness of softtissue covering the palatal bone afterthe harvesting procedure.
It can be suggested that when 2mmor more of soft tissue thickness can beleft to cover the palatal bone, CTGharvesting techniques are preferredbecause primary intention wound heal-ing results in very limited pain and abetter post-operative course in terms ofpatient stress and ability to chew. Other-wise, if palatal soft tissue is not thickenough, connective tissue harvestingtechniques are not recommendedbecause of the risk of primary flapnecrosis and/or the inadequacy of the
graft due to the presence of fatty andglandular tissues instead of connectivetissue. In this situation, harvesting anFGG that is subsequently de-epithelia-lized with the use of the blade is recom-mended.
When a FGG is harvested, a lowerthickness of palatal fibromucosa isrequired to obtain both an adequateconnective tissue graft and a residualthickness of soft tissue covering thebone. With the use of the blade, infact, it is possible to clinically check(based on the difference in light reflec-tion and tissue consistency) the removalof the epithelium and thus the mostsuperficial connective tissue can be uti-lized in the graft. This approach allowsfor incorporating into the graft the por-tion of connective tissue closer to theepithelium. This tissue is denser, firmer,more stable and presumably more sui-table for root coverage purpose (Harris2003). This was confirmed by the pre-sent study data, which demonstrated agreater increase in GT at the buccalaspect of the test-treated patients despitethe fact that no difference was found inthe thickness of the graft at the time ofsuturing between the two treatmentgroups. Furthermore, the differencebetween GT increase at 1 year and graftthickness at the time of suturingwas statistically significant (F5 56.6,po0.01) between the two groups, indi-cating that in the test group, almost theentire thickness of the graft becamebuccal GT at 1 year, while in the controlgroup, a significant part of the graftthickness was lost during the healingperiod. It can be speculated that differ-ences in the quality of the connectivetissue between the two treatment groupswere responsible for the different per-formance of the grafts during the heal-ing phase. A negative aspect of theadopted de-epithelialization techniquecould be the remnant of some epithe-lium in the graft. However, the inclusionof some epithelium did not seem toaffect the clinical results in terms ofroot coverage (Harris 2003).
The negative aspect of the epithelia-lized graft harvesting technique wasreported to be the less favourable andmore painful patient’s post-operativecourse due to the secondary intentionpalatal wound healing (Farnoush 1978,Jahnke et al. 1993, Del Pizzo et al. 2002,Griffin et al. 2006, Wessel & Tatakis2008). This does not seem to be con-firmed by the present data. This study infact failed to demonstrate any increase
in terms of post-operative pain, discom-fort and bleeding in patients subjected tothe epithelialized graft harvesting pro-cedure compared with patients under-going the connective tissue harvestingtechnique. Furthermore, no statisticallysignificant difference in pain killer con-sumption was demonstrated betweencontrol patients experiencing primaryintention wound healing (thus excludingthose with necrosis/dehiscence of theprimary flap) and test patients healingby secondary intention. The reasons forthe difference can only be speculatedon; a possible explanation can be foundin the surgical techniques and in particu-lar in the dimensions of the graft or in theprotection of the wound area withequine-derived collagen in the test group.In the studies comparing patients’ post-operative outcomes after different graft-harvesting procedures (Farnoush 1978,Jahnke et al. 1993, Del pizzo et al.2002, Griffin et al. 2006, Yen et al.2007, Wessel & Tatakis 2008), no dataare available on the thickness and heightof the FGG. However, in some of thesestudies (Griffin et al. 2006, Yen et al.2007) a periosteum elevator was used tofree the graft from the underlying boneand the graft was extended apical to thebuccal bone crest. It is conceivable thatin the present study, shallower (in theapical–coronal dimension) and thinnerFGG were harvested. The present studydata demonstrated that the height anddepth of the withdrawal and not thetype (primary versus secondary) of pala-tal wound healing influence post-opera-tive analgesic consumption. It can bespeculated that in the studies reportedin the literature, the more painful post-operative course in patients experiencingFGG procedures might be due to thegreater height of the graft as well as thegreater depth reached in the palatal softtissue during the harvesting techniqueand not (or not only) due to the differenttype (primary or secondary) of palatalwound healing. A possible explanation isthat by inserting the blade into the depthof the palatal soft tissue and/or towardsthe palatal vault (height of the withdra-wal), the probability of severing a large-sized nerve/vessel increases, causinggreater pain. In addition, it cannot beexcluded that the limited patient morbid-ity in the test group of the present studycan be ascribed to the protection of thesecondary intention wound area with anequine-derived collagen matrix, whichcould have minimized post-operative dis-comfort and bleeding (Farnoush 1978,
736 Zucchelli et al.
r 2010 John Wiley & Sons A/S

72
Saroff et al. 1982). Nevertheless, Wessel& Tatakis (2008), despite using palatalstents to protect free gingival graft donorsites, reported a greater incidence ofdonor site pain compared with CTG.
Finally, a lack of statistical signifi-cance between groups in a trial designedto demonstrate superiority does notmean that equivalence exists betweenthe two treatment techniques Gunsolleyet al. 1998). In the present data, the lackof significance between the two groupsmight be due to the great within-groupvariability, which would have required alarger then expected sample size. Astudy, with a larger number of patients,is ongoing to confirm the present data.
Another finding of the present studywas the statistically significant longermean surgical chair time in patientsundergoing the bilaminar procedurewith the trap-door harvesting technique.Because the duration of the surgicalgrafting procedure has been correlatedwith post-surgical pain in both the pre-sent and the previous studies (Griffin etal. 2006, Cortellini et al. 2009), thismight have contributed to balance painkiller consumption between the twopatient groups. In other words, it canbe hypothesized that longer surgicaltime and lower soft tissue thicknesscovering the bone in the trap-door con-trol group might have balanced thesecondary intention wound healingexperienced by the test group in termsof post-operative pain suffered by thepatients. The increased time to completethe CAF with CTG can be explained bythe additional time required to harvestthe graft (in particular, in dissecting thesplit thickness primary access flap) andto perform multiple interrupted suturesto achieve complete closure of the pala-tal wound.
Better results in terms of post-opera-tive ability to chew and patient stresswere demonstrated in patients subjectedto the CTG harvesting technique. Apossible explanation is that the openpalatal wound may render the patientmore anxious; hence, he/she avoidschewing for fear of jeopardizing woundhealing. It is surprising that the differ-ence in stress and ability to chew issignificant also including controlpatients experiencing dehiscence/necro-sis of the primary flap. It can be specu-lated that the presence of soft tissueclosing the donor site, at least in firstpost-operative day/s, could minimizepatient stress and help forget the pre-sence of the wound palatal area. Never-
theless, this seems to be in contrast withthe increased intake of anti-inflamma-tory drags in the patients with a failingtrap-door approach. This rather contro-versial issue was also reported by DelPizzo et al. (2002), and further studiesare needed to clarify it.
The results of this study also indi-cated that both types of CTG can besuccessfully used under a CAF to covergingival recession, with no statisticallysignificant difference between them.One year post-treatment, 91.6% of thecontrol gingival defects and 96.5% ofthe test gingival recessions were cov-ered with the soft tissue. Furthermore,complete root coverage was achieved in70% of the control and 85% of the testtreated cases.
The only statistically significant dif-ference in the clinical outcomesbetween the two treatment groups ofthe present study was the greaterincrease in the GT in the patients treatedwith the de-epithelialized graft. Anyattempt to explain this difference isspeculative in nature, but it might berelated to the quality (better stability andless shrinkage) of the connective tissueresulting from the de-epithelialization ofa free gingival graft with respect to thatharvested with the trap-door approach.
Conclusions
No difference in post-operative analge-sic consumption, discomfort and bleed-ing was demonstrated in patientssubjected to CTG or epithelializedgraft-harvesting techniques. However,the lack of difference could be ascribedby the considerable within-group varia-bility. Studies with a larger number ofpatients are needed to confirm the pre-sent data.
Better results in terms of post-opera-tive stress and ability to chew weredemonstrated in patients undergoingthe CTG harvesting technique.
Secondary intention palatal woundhealing due to dehiscence/necrosis ofthe primary flap was associated withgreater consumption of analgesics.
Pain killer consumption increasedwith increasing height of the withdrawaland decreasing RTT covering the palatalbone.
Both types of grafts were effective inroot coverage and clinical attachmentgain when associated with a CAF for thetreatment of gingival recession.
A greater increase in GT wasachieved in the test patients; this maybe due to the better post-operative sta-bility of connective tissue resulting fromthe de-epithelialization of free gingivalgrafts.
References
American Academy of Periodontology. (2001)
Glossary of Periodontal Terms, 4th edition,
p. 23. Boston: American Academy of Perio-
dontology.
Broome, W. C. & Taggart, E. J. (1976) Free
autogenous connective tissue grafting. Report
of two cases. Journal of Periodontology 47,
580–585.
Cairo, F., Pagliaro, U. & Nieri, M. (2008)
Treatment of gingival recession with coron-
ally advanced flap procedures. A systematic
review. Journal of Clinical Periodontology
35, 141–167.
Cortellini, P., Tonetti, M., Baldi, C., Francetti,
L., Rasperini, G., Rotundo, R., Nieri, M.,
Franceschi, D., Labriola, A. & Prato, G. P.
(2009) Does placement of a connective tissue
graft improve the outcomes of coronally
advanced flap for coverage of single gingival
recessions in upper anterior teeth? A multi-
centre, randomized, double-blind, clinical
trial. Journal of Clinical Periodontology 36,68–79.
Cortellini, P., Tonetti, M. S., Lang, N. P.,
Suvan, J. E., Zucchelli, G., Vangsted, T.,
Silvestri, M., Rossi, R., McClain, P., Fonzar,
A., Dubravec, D. & Adriaens, P. (2001) The
simplified papilla preservation flap in the
regenerative treatment of deep intrabony
defects: clinical outcomes and postoperative
morbidity. Journal of Periodontology 72,
1702–1712.
da Silva, R. C., Joly, J. C., de Lima, A. F. &
Tatakis, D. N. (2004) Root coverage using
the coronally positioned flap with or without
a subepithelial connective tissue graft. Jour-
nal of Periodontology 75, 413–419.
Del Pizzo, M., Modica, F., Bethaz, N., Priotto,
P. & Romagnoli, R. (2002) The connective
tissue graft: a comparative clinical evaluation
of wound healing at the palatal donor site.
Journal of Clinical Periodontology 29, 848–854.
Edel, A. (1974) Clinical evaluation of free
connective tissue grafts used to increase the
width of keratinised gingival. Journal of
Clinical Periodontology 1, 185–196.
Eger, T., Muller, H. P. & Heinecke, A. (1996)
Ultrasonic determination of gingival thick-
ness. Subject variation and influence of tooth
type and clinical features. Journal of Clinical
Periodontology 23, 839–845.Farnoush, A. (1978) Techniques of protection
and coverage of the donor sites in free soft
tissue graft. Journal of Periodontology 49,403–405.
Griffin, T. J., Cheung, W. S., Zavras, A. I. &
Damoulis, P. D. (2006) Postoperative com-
Patient morbidity and root coverage outcome after grafts 737
r 2010 John Wiley & Sons A/S

73
plications following gingival augmentation
procedures. Journal of Periodontology 77,2070–2079.
Gunsolley, J. C., Elswick, R. K. & Davenport, J.
M. (1998) Equivalence, superiority, and
negative clinical trials. Journal of Perio-
dontology 69, 521–527.
Harris, R. J. (1997) A comparison of two
techniques for obtaining o connective tissue
graft from the palate. The International Jour-
nal of Periodontics and Restorative Dentistry
17, 261–271.Harris, R. J. (2003) Histologic evaluation of
connective tissue graft in humans. The Inter-
national Journal of Periodontics and
Restorative Dentistry 23, 575–583.
Hurzeler, M. B. & Weng, D. (1999) A single-
incision technique to harvest subepithelial
connective tissue grafts from the palate. The
International Journal of Periodontics and
Restorative Dentistry 19, 279–287.
Jahnke, P. V., Sandifer, J. B., Gher, M. E., Gray,
J. L. & Richardson, A. C. (1993) Thick free
gingival and connective tissue autografts for
root coverage. Journal of Periodontology 64,315–322.
Joly, J. C., Carvalho, A. M., da Silva, R. C.,
Ciotti, D. L. & Cury, P. R. (2007) Root
coverage in isolated gingival recessions using
autograft versus allograft: a pilot study. Jour-
nal of Periodontology 78, 1017–1022.
Langer, B. & Langer, L. (1985) Subepithelial
connective tissue graft technique for root
coverage. Journal of Periodontology 56,
715–720.
Lorenzana, E. R. & Allen, E. P. (2000) The
single-incision palatal harvest technique: a
strategy for aesthetics and patient comfort.
The International Journal of Periodontics
and Restorative Dentistry 20, 297–305.
Muller, H. P., Schaller, N. & Eger, T. (1999)
Ultrasonic determination of thickness of mas-
ticatory mucosa: a methodologic study. Oral
Surgery, Oral Medicine, Oral Pathology,
Oral Radiology, and Endodontics 88, 248–
253.
Muller, H. P., Schaller, N., Eger, T. & Hei-
necke, A. (2000) Thickness of masticatory
mucosa. Journal of Clinical Periodontology
27, 431–36.
O’Leary, T. J., Drake, R. B. & Naylor, J. E.
(1972) The plaque control record. Journal of
Periodontology 43, 38.
Paoloantonio, M., Dolci, M., Esposito, P.,
Darchivio, D., Lisanti, L., Di Luccio, A. &
Perinetti, G. (2002) Subpedicle acellular der-
mal matrix graft and autogenous connective
tissue graft in the treatment of gingival
recessions: a comparative 1-year clinical
study. Journal of Periodontology 73, 1299–
1307.
Roccuzzo, M., Bunino, M., Needleman, I. &
Sanz, M. (2002) Periodontal plastic surgery
for treatment of localized gingival recessions:
a systematic review. Journal of Clinical
Periodontology 29, 178–194.
Sanz, M., Lorenzo, R., Aranda, J. J., Martin, C.
& Orsini, M. (2009) Clinical evaluation of a
new collagen matrix (Mucografts prototype)
to enhance the width of keratinized tissue in
patients with fixed prosthetic restorations: a
randomized prospective clinical trial. Journal
of Clinical Periodontology 36, 868–876.Saroff, S. A., Chasens, A. I., Eisen, S. F. &
Levey, S. H. (1982) Free soft tissue auto-
grafts. Hemostasis and protection of the
palatal donor site with a microfibrillar col-
lagen preparation. Journal of Periodontology
53, 425–428.
Studer, S. P., Allen, E. P., Rees, T. C. & Kouba
A, . (1997) The thickness of masticatory
mucosa in the human hard palate and tuber-
osity as potential donor sites for ridge aug-
mentation procedures. Journal of
Periodontology 68, 145–151.
Sullivan, H. C. & Atkins, J. H. (1968) Free
autogenous gingival grafts. I. Principles of
successful grafting. Periodontics 6, 121–129.Wessel, J. R. & Tatakis, D. N. (2008) Patient
outcomes following subepithelial connective
tissue graft and free gingival graft proce-
dures. Journal of Periodontology 79, 425–
430.
Yen, C. A., Griffin, T. J., Cheung, W. S. &
Chen, J. (2007) Effects of platelet concentrate
on palatal wound healing after connective
tissue graft harvesting. Journal of Perio-
dontology 78, 601–610.Zucchelli, G., Amore, C., Sforza, N. M., Mon-
tebugnoli, L. & De Sanctis, M. (2003) Bila-
minar techniques for the treatment of
recession type defects. A comparative clin-
ical study. Journal of Clinical Perio-
dontology 30, 862–870.Zucchelli, G., Clauser, C., De Sanctis, M. &
Calandriello, M. (1998) Mucogingival versus
GTR procedures in the treatment of deep
recession type defects. Journal of Period-
ontolology 69, 139–145.
Address:
Giovanni Zucchelli
Dipartimento di Scienze Odontostomatologiche
University of Bologna
Via S. Vitale 59, 40125 Bologna
Italy
E-mail: [email protected]
Clinical Relevance
Scientific rationale for the study:Randomized studies comparing bothpatient morbidity and root coverageoutcomes after the use of CTG andDGG for the treatment of gingivalrecessions are currently not availablePrincipal findings: This study indi-cated no difference in post-operative
pain, discomfort and bleedingbetween the two groups. Lowerstress and better ability to chewwere demonstrated in the CTGgroup. Pain increased with increasingheight and depth of the withdrawaland in the case of necrosis of theprimary palatal flap. A greater
increase in buccal soft tissue thick-ness was achieved in the DGG group.Practical implications: In sites withthick palatal fibromucosa, a trap-doorapproach is more patient friendly,while with thin palatal tissues, thereis a greater risk of a failure of thetrap-door, thereby indicating a DGG.
738 Zucchelli et al.
r 2010 John Wiley & Sons A/S

74
The International Journal of Periodontics & Restorative Dentistry

75
Volume 32, Number 4, 2012
3
Implant restoration is a common practice for tooth loss rehabilita-tion in esthetic areas. The main goals are functionality and esthet-ics for patient satisfaction. The clinician chooses from a variety of surgical approaches such as im-mediate, early, or delayed implant placement.1,2 After tooth extrac-tion, the hard and soft tissues un-dergo substantial changes as a result of healing.3 Many factors in-fluence the soft tissue level around dental implants but only a handful have been studied: peri-implant biotype, height and width of the fa-cial bone, orofacial position of the implant head.4,5 A major concern from an esthetic point of view are soft tissue defects around implant restorations, which often result in a extra long prosthetic crowns with disharmony of the marginal soft tis-sue scallop in respect to the adja-cent teeth. The increased esthetic demands require peri-implant soft tissue color and contour in harmo-ny with the neighboring teeth for patient satisfaction, thus, surgical reduction of the peri-implant soft tissue defect may be indicated. Results after surgical root coverage are well reported in the literature,6–9
1 Department of Odontostomatology, Bologna University, Bologna, Italy. [Au: Please provide titles for all authors at Bologna University, eg, Professor, Lecurer, Researcher, etc.] Correspondence to: Profesoor Giovanni Zucchelli, Department of Odontostomatology, Bologna University, Via S. Vitale 59, 40125 Bologna, Italy; fax: +39051225208; email: [email protected].
Giovanni Zucchelli1, /Claudio Mazzotti1, /Ilham Mounssif1, /Matteo Mar-zadori1, /Martina Stefanini1
[Au: Please provide academic degrees for all authors, eg, DDS, MD, PhD, DMD, etc]
A major concern from the esthetic point of view is soft tissue defects around implant restorations that often result in a too long prosthetic crown. This report describes a modified prosthetic–surgical approach for the treatment of peri-implant horizontal and vertical soft tissue defects in an esthetically demanding patient. One month before surgery, the implant crown restoration was removed, the preexisting implant abutment was reduced, and a short temporary crown, at the level of the homologous controlateral incisor, was applied. A bilaminar technique, consisting in an envelope coronally advanced flap covering two connective tissue grafts was used to treat the soft tissue defects around the implant site. Four months after surgery, a new implant abutment and temporary crown were applied for soft tissue conditioning before the final impression. Nine months after surgery, the peri-implant soft tissue margin was 4 mm more coronal compared with baseline and at the same soft tissue margin level of the right central incisor. A 2.2-mm increase in buccal soft tissue thickness measured 1.5 mm apical to the soft tissue margin was accomplished. The emergence profile of the replaced tooth faithfully reproduced that of the healthy homologous controlateral central incisor. Two years after surgery, the soft tissue margin was stable and the esthetic appearance of the implant site was well maintained. This report demonstrates the possibility of fully correcting severe vertical and horizontal peri-implant soft tissue defects and achieving high patient satisfaction through a combined mucogingival and prosthetic treatment. (Int J Periodontics Restorative Dent 2013;33:XXX–XXX.)
Esthetic Treatment of Peri-implant Soft Tissue Defects: A Case Report of a Modified Surgical–Prosthetic Approach

76
The International Journal of Periodontics & Restorative Dentistry
4
unlike peri-implant soft tissue de-fect reduction. Recently, a case se-ries reported successful coverage with a bilaminar technique of soft tissue dehiscence defects around single implant restorations with es-thetically satisfactory outcomes.10 This case report describes a modi-fied prosthetic–surgical approach for the treatment of peri-implant horizontal and vertical soft tissue defects in an esthetically demand-ing patient.
Clinical case
A 33-year-old woman was referred to the Department of Oral Science of Bologna University, Bologna, Italy, for evaluation of a single im-plant supported crown at the max-illary left central incisor. Her chief complaint was the unesthetic ap-pearance during smile (Fig 1a). The tooth was lost 18 months prior af-ter failure of previous endodontic therapy and was treated with im-
mediate implant placement after tooth extraction. The patient was very upset with the referring den-tist who performed the implant therapy, but was very concerned about the treatment proposed by another oral surgeon consisting of implant removal, provisional partial denture, reconstructive bone sur-gery, and new implant and crown placement. The patient’s medical history revealed no systemic con-traindications for dental treatment.
Fig 1a (left) Patient’s smile showing a “long” implant-supported crown on the maxillary left incisor.
Fig 1b (right) Disharmony of the scal-loping of the buccal gingival margin of the maxillary central incisors and buccal trans-parency of the underlying implant surface.
Fig 1c (left) Presurgical emergence pro-file of implant-supported crown.
Fig 1d (right) Radiograph showing im-plant’s proximity to the root of the maxillary left lateral incisor.
Fig 1e (left) Soft tissue margins and thin buccal keratinized tissue showing by trans-parency the underlying implant surface.
Fig 1f (right) Occlusal view showing extremely thin soft tissue covering the buc-cally positioned implant.

77
Volume 32, Number 4, 2012
5
Clinical examination showed the disharmony in scalloping of the buccal gingival margin (Fig 1b) with the marginal soft tissue of the implant restoration in a more apical position (4 mm) with respect to the adjacent natural tooth. In addition, there was a horizontal soft tissue defect with an inadequate emer-gence profile of the implant crown (Fig 1c). The buccal soft tissue was so thin that transparency of the un-derlying implant surface was visible in the patient’s smile (Figs 1e and 1f). No interproximal attachment loss was present at the neighbor-ing teeth. The overall periodontal examination showed no pathologic probing depths and low full mouth bleeding (7%) and plaque (8%) scores.11 Radiographic examination (Fig 1d) revealed that the implant head was located 5 mm apical to the cementoenamel junction (CEJ) of the adjacent incisors and no sign of peri-implant bone loss was pres-ent. The implant was very close to the lateral incisor with a great risk of damaging the supporting bone in case of implant extraction. The primary goal of treatment was to reduce the vertical soft tissue de-fect and eliminate the marginal soft tissue discrepancy between the implant restoration and the right central incisor to improve the es-thetic appearance. The secondary goal was to increase buccal soft tissue thickness to mask the im-plant transparency and to give the implant-supported crown a correct emergence profile. The patient re-ceived a session of prophylaxis to remove microbial deposits with ultrasonic points, a rubber cup,
and polishing paste, including in-structions on using a coronally di-rected roll technique to minimize toothbrushing trauma to the peri-implant soft tissue margin.
Provisional prosthetic phase
The implant crown restoration was removed 1 month before surgery (Fig 2a) and the underlying zirconia abutment was milled and reduced (Fig 2b) to eliminate the shoul-ders/chamfers and diminish the abutment proclination, creating a conic shape and a vertical finishing line with respect to the soft tissue. The present abutment was therefo-re used as a provisional abutment to build a short provisional restora-tive crown and to leave the buccal and interdental soft tissues to fill the space previously occupied by the abutment shoulder/chamfers and implant crown (Fig 2c). The distance between soft tissue mar-gin and head of the implant was 1.5 mm, measured after removal of the abutment with a manual probe (PCP-UNC 15 probe tip, Hu Frie-dy). The soft tissue thickness (0.6 mm as measured with an electronic gauge [Digital calliper C041 0–150 mm, Kennon Instruments]) was de-termined 1.5 mm apical to the soft tissue margin with a short needle for anesthesia and a 3-mm diame-ter silicon disk.12 [Au: Correct?] The provisional restoration was performed with a similar shape and height to the adjacent right central incisor and fixed with provisionally cement.
Surgical procedure
The soft tissue defect was treated with a coronally advanced flap (CAF) (Fig 2c),13 with a connective tissue graft (CTG)10,14,15 on the buc-cal surface of the implant (Fig 2d). Following local anesthesia, a hori-zontal incision was made to design an envelope flap extending from the maxillary right to left canines. This opening consisted of oblique submarginal incisions in the inter-dental area directed toward the midline and passing through the interincisal papilla and intrasulcu-lar incisions at the buccal aspect. The flap was raised with a split-full-split approach in the coronal-apical direction. Surgical papillae were dissected split-thickness up to the buccal bone crest, than the flap was elevated at full-thickness to expose at least 2 to 3 mm of buc-cal bone apical to the root expo-sures and to the bone dehiscence at the implant site. Finally, the most apical portion of the flap was el-evated split-thickness to permit the coronal displacement of the flap. The remaining facial portion of the anatomical papillae was de-epithelialized to create connective tissue beds to which the surgical papillae of the coronally advanced buccal flap were secured at time of suturing. The absence of a contact point and augmented interdental soft tissues between the implant abutment and the adjacent teeth allowed for extending the de-epithelialization of the interdental papillae at the implant site occlu-saly towards the palatal aspect. Two different CTG were harvested

78
The International Journal of Periodontics & Restorative Dentistry
6
from the palate: the thicker coronal CTG was used to compensate the soft tissue defects and the thin-ner apical CTG was used to mask the colored and buccaly exposed implant surface (Figs 2d and 2e). Both grafts were derived from the de-epithelialization with the knife blade of two mesial-distal adjacent palatal free gingival grafts.12 This technique was chosen with respect to the other connective tissue graft harvesting procedures16–19 because the palatal fibromucosa was not thick enough for both the primary access flap and the connective tis-
sue graft. Two adjacent grafts were harvested to minimize the patient’s postoperative pain and discomfort. A recent study12 demonstrated that patient postoperative pain and discomfort were correlated with harvesting depth and height (api-cal-coronal dimension) and not with the width (mesialdistal dimension) of the withdrawal. The mesiodistal length of the coronal CTG was 6 mm greater than the width of the implant abutment, the apico-coro-nal dimension was 6 mm and the thickness was 1.8 mm as measured with an electronic gauge. This CTG
was positioned over the implant abutment surface 1 mm apical to the CEJ of the central incisor and sutured at the base of the anatomi-cal papillae with two resorbable in-terrupted sutures. The apical CTG (8 mm wide, 4 mm high, and 1.0 mm thick) was positioned above the colored implant surface and se-cured with interrupted resorbable sutures anchored to the adjacent periosteum. Coronal advancement of the buccal flap was obtained by means of two split-thickness incisions: one “deep,” cutting the muscle insertions on the perios-
Fig 2a (left) Preexisting zirconia abutment after implant-supported crown removal.
Fig 2b (right) One month before surgery the reduction of the abutment by elinima-tion of shoulders/chamfers was performed.
Fig 2e (left) Evidence of the greater thickness of the coronal with respect to the apical CTG. Fig 2f (right) Sling sutures of the coro-nally advanced envelope flap; note the good fit between the surgical papillae of the flap and the underlying anatomical de-epithelialized papillae at the implant site and at the neighboring teeth.
Fig 2c (left) Envelope flap and implant exposure; note the increase in width and volume of the interdental soft tissue be-tween the abutment and adjacent teeth.
Fig 2d (right) The two CTG are sutured: the coronal one to compensate for soft tissue loss around the implant site and the apical one to mask the colored implant exposure.

79
Volume 32, Number 4, 2012
7
tium, and the other “superficial,” detaching the muscle inserting into the inner aspect of the mucosa lin-ing of the flap. Flap mobilization was considered adequate when the soft tissue margin was able to passively reach a level coronal to the CEJ at all teeth included in the flap design without tension. At the implant site, care was taken to achieve passive superimposi-tion between the surgical papillae of the flap and the occlusaly de-epithelialized papillae mesial and distal to the implant abutment. The flap was anchored in a coronal po-sition with sling sutures (6/0 PGA, Stoma) (Fig 2f). These sutures were also used to anchor the surgical papillae to the corresponding de-epithelialized anatomical papillae for a precise adaptation of the ke-ratinized tissue margin flap on the crowns and implant abutment. At the end of surgery, the provision-al prosthetic crown was reduced to avoid contact with the soft tis-sue and fixed with provisional ce-ment. Two weeks later, the sutures were removed. The patient was in-structed not to brush in the treated area, but to rinse for 1 minute with a 0.12% chlorhexidine solution three times a day. After suture re-moval, plaque control in the surgi-cally treated area was maintained by rinsing with chlorhexidine for an additional 2 weeks. The patient was instructed in mechanical tooth cleaning using an ultrasoft tooth-brush for 1 month and told to rinse with chlorhexidine twice a day. Af-ter, the patient was instructed to use a soft toothbrush and rinse with chlorhexidine once a day for an-
other month. When chlorhexidine was discontinued, full mechanical interproximal cleaning was reinsti-tuted. The patient was recalled for prophylaxis once a month until the definitive restoration was delivered.
Change of the abutment and provisional crown
Four months after surgery (Fig 3a), the modified abutment was replaced with a new zirconia abut-ment. The increased size of the subgingival portion of the abut-ment, due to the presence of shoulders/chamfers, compressed the soft tissue between the implant abutment and the adjacent teeth and provided a horizontal finish-ing line for the new provisional prosthetic crown built with a shape similiar to the homologous contro-lateral central incisor. The change in the crown emergence profiles together with the restored contact points contributed to soft tissue conditioning and growth of inter-dental papillae.
Final prosthetic phase
Nine months after surgery, a fi-nal impression was made and the resulting cast used for definitive crown design. A lithium disilicate restoration was used to rehabilitate the implant (Fig 3d) with the same shape of the right central incisor and a correct emergence profile with respect to the new soft tissue height and shape (Fig 3f).
Results
At time of definitive impression, the distance between the soft tissue margin and head of the implant was 5 mm (Fig 3b). A com-parison between baseline and the 9-month follow-up showed a peri-implant soft tissue margin 4 mm more coronal, at the same level of the soft tissue margin of the right central incisor. The soft tissue thick-ness (Fig 3c) was 2.8 mm. Thus, a 2.2 mm increase in buccal soft tis-sue thickness was accomplished with the surgical procedure. The probing depth around the implant-supported crown was within the physiologic limit (< 4 mm) and no bleeding on probing was present. The color and height of the keratin-ized tissue of the implant was well integrated with the adjacent gingi-val tissue (Fig 3d). The peri-implant soft tissue scalloping was well har-monized with the adjacent gingival margin and no disalignment of the mucogingival junction was pres-ent. The emergence profile of the crown was easy to clean and re-produced faithfully the emergence of a natural tooth from its soft tis-sue (Fig 3f). The implant restora-tion had a natural appearance. The patient showed good compliance with low full-mouth plaque (4%) and bleeding scores (4%) and no pathologic probing depths. The patient was very satisfied with her new esthetic appearance. Two years after surgery (Fig 3e), the soft tissue margin was stable, the esthetic appearance at the implant site was well maintained, probing depths were physiologic (< 4 mm),

80
The International Journal of Periodontics & Restorative Dentistry
8
and no signs of mucositis or perim-plantitis were present.
Discussion
Soft and hard tissue modifications are common after tooth extraction. Implant rehabilitation without soft/hard tissue defect correction or pre-vention may result in poor esthetic satisfaction for patients. The bilami-nar technique (CAF plus CTG) has been reported to be a suitable procedure to achieve highly pre-
dictable results in terms of com-plete root coverage.6,7 This patient was treated with a technique used in a recent pilot study10 where iso-lated peri-implant soft tissue dehis-cences were covered, with results as succesfull as those reported for gingival recession treatment with the bilaminar technique. The pro-cedure described in the present study completely solved the verti-cal and horizontal peri-implant soft tissue defects; in fact, at 9 months, the peri-implant soft tissue margin was at the same level as the gin-
gival margin of the homologous controlateral tooth and the increase in buccal soft tissue thickness al-lowed for masking of the implant’s transparency and restored a correct implant-supported crown emer-gence profile. Both graft type and flap design played a critical role in achieving this outcome. The CTGs used in this patient derived from the de-epithelialization of free gin-gival grafts.12 Advantages derived from this technique included more dense and stable connective tissue closer to the epithelium and less
Fig 3a (left) Four months postsurgery the soft tissue margin at the implant site is more coronal than the gingival margin of the homologous controlateral central inci-sor. The temporary crown was left “short” to not interfere with the healing process.
Fig 3b (right) Nine months follow-up, 5mm transmucosal height was measured from the head of the implant to the soft tissue margin.
Fig 3c (left) Occlusal view showing the increase in buccal soft tissue thickness at the implant site.
Fig 3d (right) One year postsurgery, the color and height of the keratinized tissue of the implant site is well integrated with the adjacent gingival tissue.
Fig 3e (left) Two years postsurgery the esthetic appearance of the implant site was maintained.
Fig 3f (right) The emergence profile of the crown faithfully reproduced that of a natural tooth from its soft tissue.

81
Volume 32, Number 4, 2012
9
prone to contraction, and closer to the bone that is rich in fatty and glandular tissue. The difference in the quality of the CTG could be particularly significant when thick grafts, such as those used to treat soft tissue defects around implants, are harvested. In a thick graft, the proportion of glandular and fatty tissue included increases with re-spect to the denser connective tis-sue closer to the epithelium that is left in the primary flap when har-vesting techniques are performed. The stability of the CTG used in the present study was demonstrated by the increase in buccal soft tissue thickness that was larger than the thickness of the CTG at time of sur-gery, suggesting not only stability but a further thickness increase over time of de-epithelialized free gingi-val graft. The envelope flap design used in this report was similar to the coronally advanced flap for the treatment of multiple recession de-fects in the upper anterior teeth.13
Vertical releasing incisions may damage the blood supply to the
flap and often result in unpleasant visible white scars.20 The absence of vertical releasing incisions is even more important when the surgi-cal papillae of the flap have to be shifted palatally as well as coronally to reach the de-epithelialized papil-lae between the implant abutment and the adjacent teeth. With such a palatal dislocation, vertical releas-ing incisions would have shifted mesially and farther from the adja-cent firm soft tissues with a greater risk of damaging flap blood supply and inducing gingival defects at the adjacent teeth. Procuring a wide envelope flap free from deep (peri-osteal) and superficial (submucosal) muscle insertions allowed for the surgical papillae of the flap to pas-sively reach the palatally shifted de-epithelialized papillae neighboring the implant abutment, despite the presence of two CTG, with no dam-age to the flap or adjacent teeth. On the contrary gingival recessions present at the neighboring teeth, the implant could be corrected by means of a coronally advanced
flap. This led to a significant im-provement in the overall esthetic appearance of the treated area with high patient satisfaction.
Conclusions
The successful esthetic result achieved in the present case was associated with more than the surgical procedure. A great con-tribution was derived from the modifications of the prosthetic components performed before and after surgical intervention. Concerning the presurgical pros-thetic phase, the removal of the implant crown together with reduc-tion of the implant abutment pro-vided wider interdental connective tissue beds between the implant abutment and the adjacent teeth for the graft and surgical papillae of the covering flap.10 In particular, the reduction of the abutment, per-formed 1 month before surgery, al-lowed for the interdental soft tissue to occupy the space previously in-
Fig 4 Views at (a) baseline and (b) 2 years postsurgery.
a b

82
The International Journal of Periodontics & Restorative Dentistry
10
habited by zirconia. This reduction increased the width and volume of the peri-implant soft tissues at time of surgery and improved the vas-cular exchange with the graft and the surgical papillae of the cover-ing flap. The increased width of the papillae mesial and distal to the abutment and the possibility of occlusaly extending de-epitheli-alization toward the palatal aspect allowed for precise stabilization of the surgical papillae of the cover-ing flap despite the coronal po-sitioning of the CTG. The lack of graft exposure during healing on one side reduced graft resorption and shrinkage and on the other improved the esthetic outcome by avoiding the white scar appear-ance and disalignment of the mu-cogingival line typical of the free gingival graft posthealing. Besides, presurgical abutment modification by reducing abutment proclination may have contributed to minimiz-ing the apical shift of the marginal soft tissue. Postsurgical (4 months) replacement of the implant abut-ment together with the new provi-sional crown played a critical role in conditioning interdental soft tissue and facilitating the growth of inter-dental papillae. Within the limits of a clinical case report, this study showed the possibility of fully cor-recting severe vertical and horizon-tal peri-implant soft tissue defects and achieving high patient satis-faction through combined muco-gingival and prosthetic treatment; however, long-term maintenance of the successful outcome is not yet demonstrated.
Acknowledgment
The authors reported no conflicts of interest related to this study.
References
1. Esposito M, Grusovin MG, Polyzos IP, Fe-lice P, Worthington HV. Timing of implant placement after tooth extraction: Imme-diate, immediate-delayed or delayed implants? A Cochrane systematic review. Eur J Oral Implantol 2010;3:189–205.
2. Chen ST, Buser D. Clinical and esthetic outcomes of implants placed in postex-traction sites. Int J Oral Maxillofac Im-plants 2009;24(suppl):186–217.
3. Tan WL, Wong TL, Wong MC, Lang NP. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin Oral Implants Res 2012;23(suppl 5):1–21.
4. Nisapakultorn K, Suphanantachat S, Silkosessak O, Rattanamongkolgul S. Factors affecting soft tissue level around anterior maxillary single-tooth implants. Clin Oral Implants Res 2010;21:662–670.
5. Sorni-Broker M, Penarrocha-Diago M, Penarrocha-Diago M. Factors that influ-ence the position of the peri-implant soft tissues: A review. Med Oral Patol Oral Cir Bucal 2009;14:e475–e479.
6. Chambrone L, Sukekava F, Araujo MG, Pustiglioni FE, Chambrone LA, Lima LA. Root coverage procedures for the treat-ment of localised recession-type defects. Cochrane Database Syst Rev 2009: CD007161.
7. Cairo F, Pagliaro U, Nieri M. Treatment of gingival recession with coronally advanced flap procedures: A systematic review. J Clin Periodontol 2008;35:136–162.
8. Oates TW, Robinson M, Gunsolley JC. Surgical therapies for the treatment of gingival recession. A systematic review. Ann Periodontol 2003;8:303–320.
9. Roccuzzo M, Bunino M, Needleman I, Sanz M. Periodontal plastic surgery for treatment of localized gingival reces-sions: A systematic review. J Clin Peri-odontol 2002;29(suppl 3):178–194.
10. Zucchelli G, Mazzotti C, Mounssif I, Mele M, Stefanini M, Montebugnoli L. A novel surgical–prosthetic approach for soft tis-sue dehiscence coverage around single implant. Clin Oral Implants Res 2012 Aug 27, doi: 10.1111/clr.12003 [epub ahead of print].
11. O’Leary TJ, Drake RB, Naylor JE. The plaque control record. J Periodontol 1972;43:38.
12. Zucchelli G, Mele M, Stefanini M, et al. Patient morbidity and root coverage out-come after subepithelial connective tissue and de-epithelialized grafts: A compara-tive randomized-controlled clinical trial. J Clin Periodontol 2010;37:728–738.
13. Zucchelli G, De Sanctis M. The coronally advanced flap for the treatment of mul-tiple recession defects: A modified surgi-cal approach for the upper anterior teeth. J Int Acad Periodontol 2007;9:96–103.
14. Zucchelli G, Amore C, Sforza NM, Mon-tebugnoli L, De Sanctis M. Bilaminar techniques for the treatment of recession-type defects. A comparative clinical study. J Clin Periodontol 2003;30:862–870.
15. Pini-Prato GP, Cairo F, Nieri M, Frances-chi D, Rotundo R, Cortellini P. Coronally advanced flap versus connective tissue graft in the treatment of multiple gingi-val recessions: A split-mouth study with a 5-year follow-up. J Clin Periodontol 2010;37:644–650.
16. Edel A. Clinical evaluation of free con-nective tissue grafts used to increase the width of keratinised gingiva. J Clin Peri-odontol 1974;1:185–196.
17. Langer B, Langer L. Subepithelial con-nective tissue graft technique for root coverage. J Periodontol 1985;56:715–720.
18. Hurzeler MB, Weng D. A single-inci-sion technique to harvest subepithe-lial connective tissue grafts from the palate. Int J Periodontics Restorative Dent 1999;19:279–287.
19. Lorenzana ER, Allen EP. The single-incision palatal harvest technique: A strategy for esthetics and patient com-fort. Int J Periodontics Restorative Dent 2000;20:297–305.
20. Zucchelli G, Mele M, Mazzotti C, Mar-zadori M, Montebugnoli L, De Sanctis M. Coronally advanced flap with and without vertical releasing incisions for the treatment of multiple gingival reces-sions: A comparative controlled random-ized clinical trial. J Periodontol 2009; 80:1083–1094.

83






















![Presentation Name - Lenoir-Rhyne Universitycsc-studentweb.lr.edu/swp/Berg/articles/ASUG/ASUG_2… · · 2010-06-26Presentation Name] Insert Speaker Names [SHERRYANNE MEYER ... §](https://img.dokumen.tips/doc/110x75/5abfb8937f8b9add5f8e1091/presentation-name-lenoir-rhyne-universitycsc-2010-06-26presentation-name-insert.jpg)







