Embed Size (px)
Citation preview

Clinical Radiology (1986) 37, 579-581 0009-9260/86/702579502.00 © 1986 Royal College of Radiologists
Soft Tissue Sarcoma: Two Cases of Solitary Lung More Than 15 Years After Diagnosis
Metastasis
J. J. G O I N G , T. B. B R E W I N * , G . K . C R O M P T O N t a n d J. M c L E L L A N D $
Department of Pathology, University of Edinburgh, * Glasgow Institute of Radiotherapeutics and Oncology, tNorthern General Hospital, Edinburgh and SWestern General Hospital, Edinburgh
Soft tissue sarcomas may behave unpredictably. We present two adult cases in which solitary pulmonary metastases have occurred, 18 and 16 years after diagnosis. In both cases the primary disease was successfully controlled by conservative surgery com- bined with radiotherapy.
C A S E 1
A 43-year-old female stenographer presented in March 1966 with a 1-year history of a static, painless swelling on the medial aspect of the left thigh. A dense vascular mass 9 cm×6 crux4 cm was 'shelled out' and diagnosed histologically as a moderately pleomorphic fibrosarcoma. Radiotherapy was given to reduce the chance of local recurrence. Using a single 20xl5cm beam of a 4MeV X-rays covering a 5 cm margin above and below the tumour bed, 20 daily fractions were given over a 4-week period, the subcutaneous dose being 6000 cGy and the 5 cm depth dose 5150 cGy.
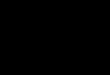
The chest radiograph in 1966 was normal apart from a calcified tuberculous opacity in the right lower zone, which was unchanged in 1978, when a routine employment radiograph showed a new small opacity in the left upper zone (Fig. 1). Six years later the new lesion had enlarged slightly and was surgically removed, for diagnosis. A benign lesion was considered likely on clinical grounds.
Address for correspondence and for offprints: Dr J. J. Going, Department of Pathology, University Medical School, Teviot Place, Edinburgh EH8 9AG.
Histology
The nodule (1.3 cmxl .0 cm×0.8cm) was a sarcoma identical to recut sections of the original lesion and was identified as a leiomyosarcoma by demonstrating intracellular myofibrils on elec- tron microscopy of the resected pulmonary nodule. There were necrotic areas in the primary and secondary lesions and mitotic figures were numerous in both (11.8, 10.6 and per 10-high power fields respectively) (Fig. 2).
C A S E 2
A 41-year-old male motor mechanic presented in July 1968 with an 8 crux5 cm swelling of the lower inner aspect of the left thigh. By February 1969 it was bigger and a lobulated tumour lying in the muscles was excised, apparently completely. Histology showed a myxoid liposarcoma with scanty mitoses.
In May 1974 a local recurrence with three tumour nodules was excised. At the same time a matted mass of lymph nodes was noted in the left groin. Radiotherapy was given to the primary site and to the groin nodes, and he received 4500 cGy of 6 MeV X-rays in 20 fractions over 4 weeks to each site.
In June 1984 a chest radiograph showed an ill-defined opacity in the left upper lobe (Fig. 3a), which was shown more clearly by tomography (Fig. 3b). The lesion was excised for diagnosis.
Histology
The lesion was a deposit of myxoid liposarcoma identical to the tumours excised in 1969 and 1974 (Fig. 4).
(a) (b) Fig. 1 - Case 1. (a) This radiograph taken in 1984, shows the dense calcified tuberculoma (unaltered since 1966) in the right lower zone and the new opacity in the left upper zone (arrow). (b) Detail of the lesion in the left upper zone.

580 CLINICAL RADIOLOGY
(a) (b) Fig. 2 - Case 1. The histological features of the primary leiomyosarcoma (a) and its pulmonary metastasis (b) are identical. Mitotic figures (indicated by arrows) are numerous (both haematoxylin and eosin, x320).
(a) (b) Fig. 3 - Case 2. (a) This radiograph taken in 1984, shows the new opacity in the left upper zone (arrow). (b) Tomogram showing the opacity more clearly.
DISCUSSION
Both patients are currently well with no evidence of disease. Such very late metastases f rom soft tissue sarcoma seem to be rare, though in most series patients have not been followed up for long enough to give the exact incidence.
Of interest is the indolent course of the first case despite numerous mitoses and necrosis, which are features generally regarded as unfavourable prognostic
indicators in le iomyosarcomas (Fields and Helwig, 1981; Enzinger and Weiss, 1983). Very l a t e metastasis by leiomyosarcomas is well recognised, but the pr imary and secondary deposits in these cases are usually well differentiated and lack the unfavourable characteristics seen in our case. Some cases of multiple pulmonary ' le iomyomas ' or ' smooth muscle hamarto- mas ' have almost certainly been metastases f rom very well differentiated le iomyosarcomas, arising for ex- ample in the uterus (Wolff et al., 1979). Also of interest are the unusual feature of apparent lymph

LATE PULMONARY METASTASES FROM SOFT TISSUE SARCOMA 581
(a) (b)
Fig. 4 - Case 2. The histological features of the primary myxoid liposarcoma (a) and its pulmonary metastasis (b) are identical. Mitotic figures are not seen (both haematoxylin and eosin, x320.)
node involvement in the second case, and the success- ful long-term local control achieved in both cases by conservative surgery and radiotherapy as reported in several series (Suit et al., 1975; Firth, 1979; Coe et al., 1981) but not always recognised in surgical and pathological textbooks.
REFERENCES
Coe, M. A., Madden, F. J. & Mould, R. F. (1981). The role of radiotherapy in the treatment of soft tissue sarcoma: a retrospec- tive study 1958-1973. Clinical Radiology, 32, 47-51.
Enzinger, F. M. & Weiss, S. W. (1983). Soft Tissue Tumours, pp. 304-308. The C. V. Mosby Co., St. Louis.
Fields, J. L. & Helwig, E. B. (1981). Leiomyosarcoma of the skin and subcutaneous tissue. Cancer, 47, 156-169.
Firth, L. A. (1979). The relative roles of surgery and radiotherapy in the management of soft tissue sarcomas of adults. Clinical Radiology, 30, 155-159.
Suit, H, D., Russell, W. O. & Martin, R. G. (1975). Sarcoma of soft tissue: clinical and histopathologic parameters and response to treatment. Cancer, 35, 1478-1483.
Wolff, M., Silva, F. & Kaye, G. (1979). Pulmonary metastases (with admixed epithelial elements) from smooth muscle neo- plasms. American Journal of Surgical Pathology, 3, 325-342.












![A dedifferentiated solitary fibrous tumor of the parotid gland: …...prediction of tumor metastasis [3]. Moreover, dedifferen-tiation, a phenomenon well-recognized in mesenchymal](https://img.dokumen.tips/doc/110x75/608fed1cc9c65f3510551dc1/a-dedifferentiated-solitary-fibrous-tumor-of-the-parotid-gland-prediction-of.jpg)














