Embed Size (px)
Citation preview
DrotpAostp
0
d
SURGICAL ONCOLOGY AND RECONSTRUCTION
J Oral Maxillofac Surg70:2440-2444, 2012
Sliding Anterior Hemitongue Flap forPosterior Tongue Defect Reconstruction
David K. Lam, DDS, PhD,* Allen Cheng, DDS,†
Karim E. Berty, DDS, MD,‡ and
Brian L. Schmidt, DDS, MD, PhD§
Posterior tongue defects present a unique reconstructive challenge. The various reconstructive optionsavailable for treating the defect created by a posterior hemiglossectomy frequently result in a distortedtongue and functional impairment. This paper describes a novel sliding anterior hemitongue flap to allowreconstruction of moderate resection defects (i.e. for T1-T2 tongue squamous cell carcinomas) of theposterior tongue. By mobilizing the anterior tongue, near normal mobility and tongue length aremaintained. This surgical technique may be performed alone intraorally or in combination with a neckdissection.© 2012 American Association of Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg 70:2440-2444, 2012tct
tsctlpn
robotottBlma
efects of the posterior tongue present a uniqueeconstructive challenge. Surgical treatment of T1r T2 squamous cell carcinoma involving the pos-erior third of the tongue involves removal of theosterior half of the involved side of the tongue.fter posterior hemiglossectomy, primary closuref the remaining tongue or skin grafting of the rawurface frequently results in a distorted tongue that isoo short or too narrow. These patients may also com-lain of salivary pooling, food trapping, and inefficient
Received from the Department of Oral and Maxillofacial Surgery,
University of California, San Francisco, CA.
*Postdoctoral Scholar and Former Maxillofacial Oncology Fellow,
Department of Oral and Maxillofacial Surgery, University of Califor-
nia, San Francisco, CA.
†Chief Resident, Department of Oral and Maxillofacial Surgery,
University of California, San Francisco, CA.
‡Former Chief Resident, Department of Oral and Maxillofacial
Surgery, University of California, San Francisco, CA.
§Professor, Department of Oral and Maxillofacial Surgery and
Director, Bluestone Center for Clinical Research, New York Uni-
versity, New York, NY.
Conflict of Interest Disclosures: None of the authors reported
any disclosures.
Address correspondence and reprint requests to Dr Schmidt:
Bluestone Center for Clinical Research, New York University Col-
lege of Dentistry, 345 East 24th Street, Clinic 2W, New York, NY
10010; e-mail: [email protected]
© 2012 American Association of Oral and Maxillofacial Surgeons
278-2391/12/7010-0$36.00/0
toi:10.1016/j.joms.2011.11.005
2440
ongue control of food and liquids in the posterior oralavity. By reconstructing a full-bodied, mobile posteriorongue, these problems may be prevented.
This report describes a novel sliding anterior hemi-ongue flap to allow reconstruction of moderate re-ection defects (ie, for T1 or T2 tongue squamous cellarcinomas) of the posterior tongue. By mobilizinghe anterior tongue, near normal mobility and tongueength are maintained. This surgical technique may beerformed alone intraorally or in combination with aeck dissection.
Surgical Technique
The tumor is resected in the usual manner and aneck dissection may be performed concomitantly,if indicated. Tumors with a surface dimension of 2to 4 cm with a 1- to 2-cm margin will result in adefect of 4 to 6 cm. An adult tongue has a length of12 to 14 cm when fully protruded.1 As such, theemaining ipsilateral tongue would have 6 to 8 cmf remaining usable tissue. The anterior tongue maye readily mobilized, rotated, and moved posteri-rly to reconstruct a full-bodied tongue. After pos-erior hemiglossectomy, the median fibrous septumf the remaining tongue is divided down throughhe genioglossus muscle, carrying this division an-eriorly to the anterior third of the tongue (Fig 1A).ecause the lingual neurovascular supply is found
aterally and the median fibrous septum contains noajor vessels,2 dividing the remaining tongue into sep-
rate halves is rapid, safe, and almost bloodless. With the
ongue divided, a curvilinear incision is extended to the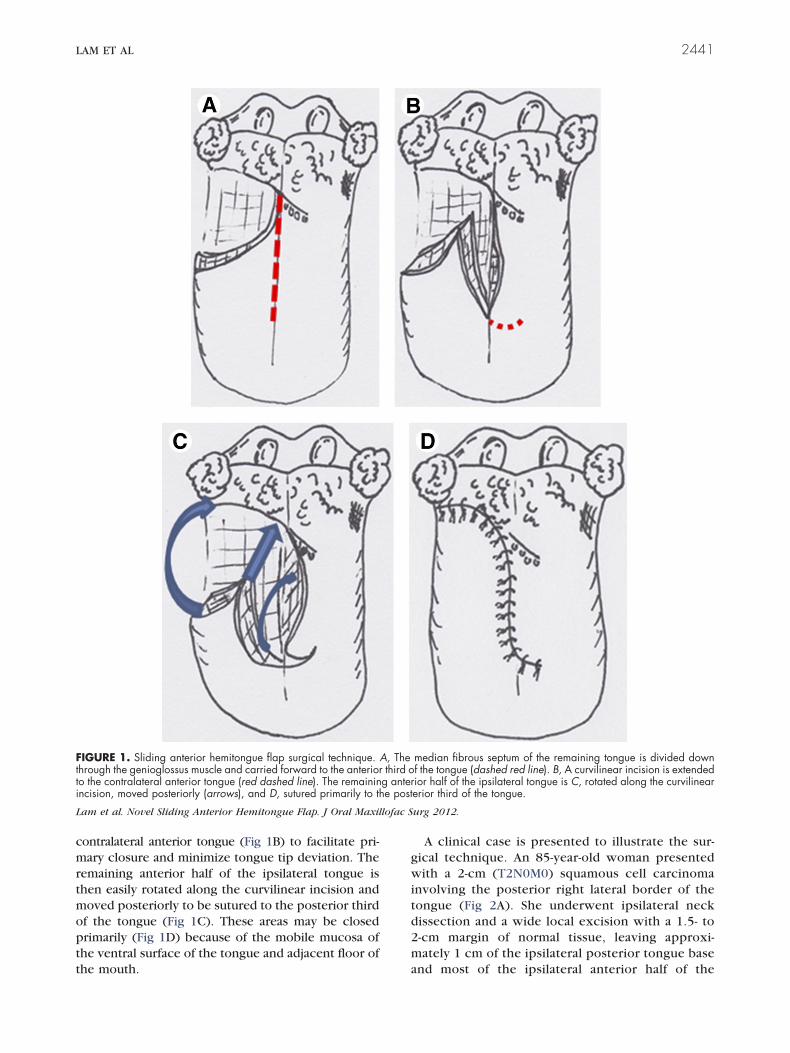
tt
lofac S
LAM ET AL 2441
contralateral anterior tongue (Fig 1B) to facilitate pri-mary closure and minimize tongue tip deviation. Theremaining anterior half of the ipsilateral tongue isthen easily rotated along the curvilinear incision andmoved posteriorly to be sutured to the posterior thirdof the tongue (Fig 1C). These areas may be closedprimarily (Fig 1D) because of the mobile mucosa ofthe ventral surface of the tongue and adjacent floor of
FIGURE 1. Sliding anterior hemitongue flap surgical technique.hrough the genioglossus muscle and carried forward to the anterioro the contralateral anterior tongue (red dashed line). The remaininincision, moved posteriorly (arrows), and D, sutured primarily to th
Lam et al. Novel Sliding Anterior Hemitongue Flap. J Oral Maxil
the mouth.
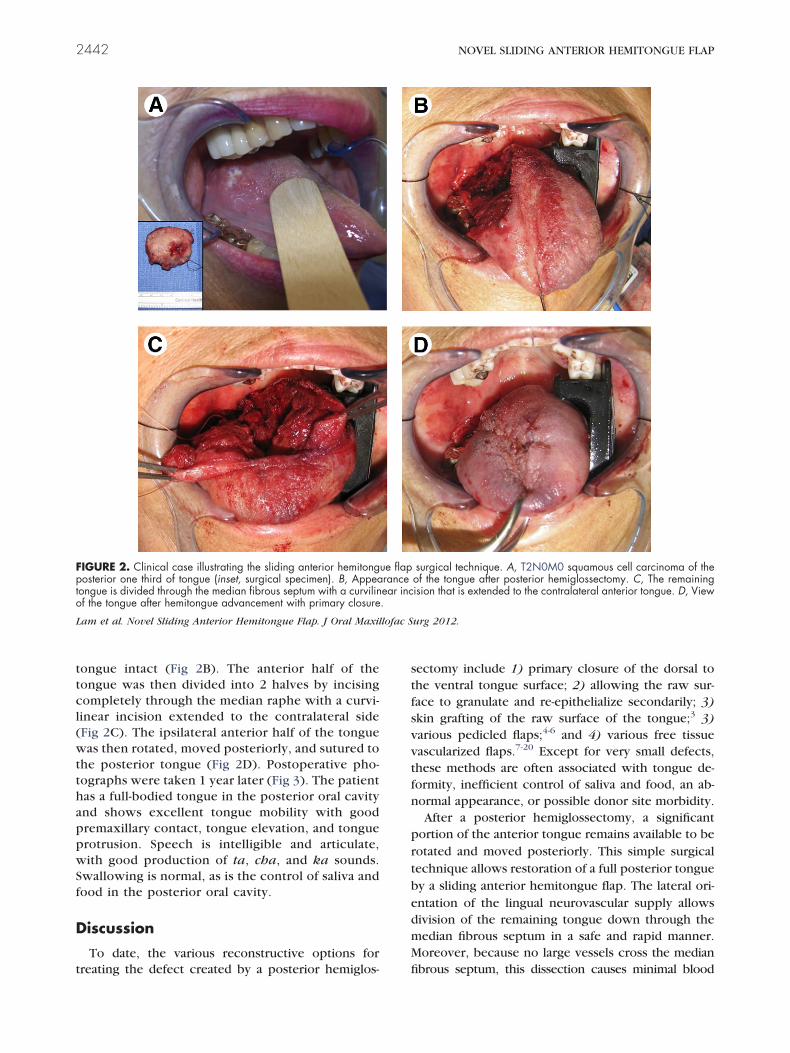
A clinical case is presented to illustrate the sur-gical technique. An 85-year-old woman presentedwith a 2-cm (T2N0M0) squamous cell carcinomainvolving the posterior right lateral border of thetongue (Fig 2A). She underwent ipsilateral neckdissection and a wide local excision with a 1.5- to2-cm margin of normal tissue, leaving approxi-mately 1 cm of the ipsilateral posterior tongue base
median fibrous septum of the remaining tongue is divided downf the tongue (dashed red line). B, A curvilinear incision is extendedior half of the ipsilateral tongue is C, rotated along the curvilinearerior third of the tongue.
urg 2012.
A, Thethird o
g antere post
and most of the ipsilateral anterior half of the
Sf
tfs
tfn
prtbedmM
pto
L lofac S
2442 NOVEL SLIDING ANTERIOR HEMITONGUE FLAP
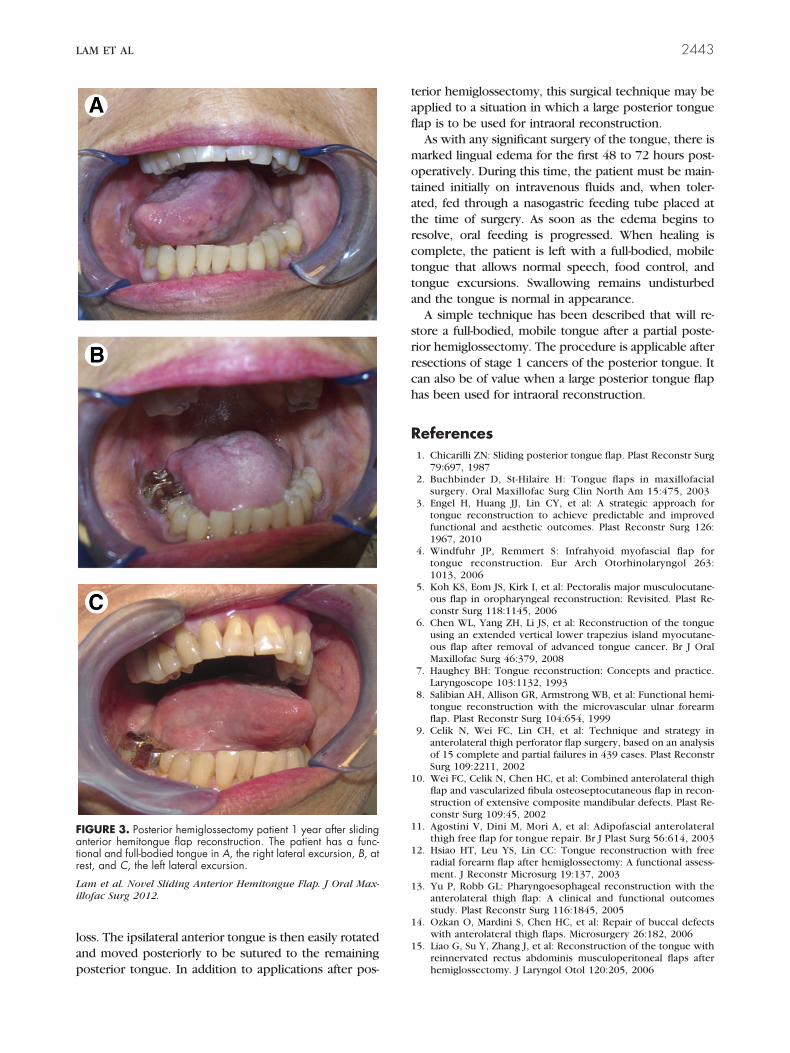
tongue intact (Fig 2B). The anterior half of thetongue was then divided into 2 halves by incisingcompletely through the median raphe with a curvi-linear incision extended to the contralateral side(Fig 2C). The ipsilateral anterior half of the tonguewas then rotated, moved posteriorly, and sutured tothe posterior tongue (Fig 2D). Postoperative pho-tographs were taken 1 year later (Fig 3). The patienthas a full-bodied tongue in the posterior oral cavityand shows excellent tongue mobility with goodpremaxillary contact, tongue elevation, and tongueprotrusion. Speech is intelligible and articulate,with good production of ta, cha, and ka sounds.wallowing is normal, as is the control of saliva andood in the posterior oral cavity.
Discussion
To date, the various reconstructive options for
FIGURE 2. Clinical case illustrating the sliding anterior hemitongosterior one third of tongue (inset, surgical specimen). B, Appea
ongue is divided through the median fibrous septum with a curvilinf the tongue after hemitongue advancement with primary closure
am et al. Novel Sliding Anterior Hemitongue Flap. J Oral Maxil
treating the defect created by a posterior hemiglos- fi
sectomy include 1) primary closure of the dorsal tohe ventral tongue surface; 2) allowing the raw sur-ace to granulate and re-epithelialize secondarily; 3)kin grafting of the raw surface of the tongue;3 3)
various pedicled flaps;4-6 and 4) various free tissuevascularized flaps.7-20 Except for very small defects,hese methods are often associated with tongue de-ormity, inefficient control of saliva and food, an ab-ormal appearance, or possible donor site morbidity.After a posterior hemiglossectomy, a significant
ortion of the anterior tongue remains available to beotated and moved posteriorly. This simple surgicalechnique allows restoration of a full posterior tonguey a sliding anterior hemitongue flap. The lateral ori-ntation of the lingual neurovascular supply allowsivision of the remaining tongue down through theedian fibrous septum in a safe and rapid manner.oreover, because no large vessels cross the median
surgical technique. A, T2N0M0 squamous cell carcinoma of theof the tongue after posterior hemiglossectomy. C, The remainingision that is extended to the contralateral anterior tongue. D, View
urg 2012.
ue flapranceear inc.
brous septum, this dissection causes minimal blood
r
Li
LAM ET AL 2443
loss. The ipsilateral anterior tongue is then easily rotatedand moved posteriorly to be sutured to the remaining
FIGURE 3. Posterior hemiglossectomy patient 1 year after slidinganterior hemitongue flap reconstruction. The patient has a func-tional and full-bodied tongue in A, the right lateral excursion, B, atest, and C, the left lateral excursion.
am et al. Novel Sliding Anterior Hemitongue Flap. J Oral Max-llofac Surg 2012.
posterior tongue. In addition to applications after pos-
terior hemiglossectomy, this surgical technique may beapplied to a situation in which a large posterior tongueflap is to be used for intraoral reconstruction.
As with any significant surgery of the tongue, there ismarked lingual edema for the first 48 to 72 hours post-operatively. During this time, the patient must be main-tained initially on intravenous fluids and, when toler-ated, fed through a nasogastric feeding tube placed atthe time of surgery. As soon as the edema begins toresolve, oral feeding is progressed. When healing iscomplete, the patient is left with a full-bodied, mobiletongue that allows normal speech, food control, andtongue excursions. Swallowing remains undisturbedand the tongue is normal in appearance.
A simple technique has been described that will re-store a full-bodied, mobile tongue after a partial poste-rior hemiglossectomy. The procedure is applicable afterresections of stage 1 cancers of the posterior tongue. Itcan also be of value when a large posterior tongue flaphas been used for intraoral reconstruction.
References1. Chicarilli ZN: Sliding posterior tongue flap. Plast Reconstr Surg
79:697, 19872. Buchbinder D, St-Hilaire H: Tongue flaps in maxillofacial
surgery. Oral Maxillofac Surg Clin North Am 15:475, 20033. Engel H, Huang JJ, Lin CY, et al: A strategic approach for
tongue reconstruction to achieve predictable and improvedfunctional and aesthetic outcomes. Plast Reconstr Surg 126:1967, 2010
4. Windfuhr JP, Remmert S: Infrahyoid myofascial flap fortongue reconstruction. Eur Arch Otorhinolaryngol 263:1013, 2006
5. Koh KS, Eom JS, Kirk I, et al: Pectoralis major musculocutane-ous flap in oropharyngeal reconstruction: Revisited. Plast Re-constr Surg 118:1145, 2006
6. Chen WL, Yang ZH, Li JS, et al: Reconstruction of the tongueusing an extended vertical lower trapezius island myocutane-ous flap after removal of advanced tongue cancer. Br J OralMaxillofac Surg 46:379, 2008
7. Haughey BH: Tongue reconstruction: Concepts and practice.Laryngoscope 103:1132, 1993
8. Salibian AH, Allison GR, Armstrong WB, et al: Functional hemi-tongue reconstruction with the microvascular ulnar forearmflap. Plast Reconstr Surg 104:654, 1999
9. Celik N, Wei FC, Lin CH, et al: Technique and strategy inanterolateral thigh perforator flap surgery, based on an analysisof 15 complete and partial failures in 439 cases. Plast ReconstrSurg 109:2211, 2002
10. Wei FC, Celik N, Chen HC, et al: Combined anterolateral thighflap and vascularized fibula osteoseptocutaneous flap in recon-struction of extensive composite mandibular defects. Plast Re-constr Surg 109:45, 2002
11. Agostini V, Dini M, Mori A, et al: Adipofascial anterolateralthigh free flap for tongue repair. Br J Plast Surg 56:614, 2003
12. Hsiao HT, Leu YS, Lin CC: Tongue reconstruction with freeradial forearm flap after hemiglossectomy: A functional assess-ment. J Reconstr Microsurg 19:137, 2003
13. Yu P, Robb GL: Pharyngoesophageal reconstruction with theanterolateral thigh flap: A clinical and functional outcomesstudy. Plast Reconstr Surg 116:1845, 2005
14. Ozkan O, Mardini S, Chen HC, et al: Repair of buccal defectswith anterolateral thigh flaps. Microsurgery 26:182, 2006
15. Liao G, Su Y, Zhang J, et al: Reconstruction of the tongue withreinnervated rectus abdominis musculoperitoneal flaps after
hemiglossectomy. J Laryngol Otol 120:205, 2006
2444 NOVEL SLIDING ANTERIOR HEMITONGUE FLAP
16. Chepeha DB, Teknos TN, Shargorodsky J, et al: Rectangletongue template for reconstruction of the hemiglossectomydefect. Arch Otolaryngol Head Neck Surg 134:993, 2008
17. Engel H, Gazyakan E, Cheng MH, et al: Customized reconstruc-tion with the free anterolateral thigh perforator flap. Microsur-gery 28:489, 2008
18. Chen SL, Yu CC, Chang MC, et al: Medial sural artery perforator
flap for intraoral reconstruction following cancer ablation. AnnPlast Surg 61:274, 200819. Kao HK, Chang KP, Wei FC, et al: Comparison of the medialsural artery perforator flap with the radial forearm flap forhead and neck reconstructions. Plast Reconstr Surg 124:1125, 2009
20. Huang JJ, Wallace C, Lin JY, et al: Two small flaps fromone anterolateral thigh donor site for bilateral buccalmucosa reconstruction after release of submucous fibrosis
and/or contracture. J Plast Reconstr Aesthet Surg 63:440,2010