Embed Size (px)
Citation preview

Slide Seminar
Drugs and Kidney
Case 3
Heinz Regele
Department of Pathology

Clinical history
•First renal transplant lost in 1995 due to infectious complications 4 weeks after TX
•Second allograft in October 1999. During the first post-transplantation year serum creatinine (sCr) ranged from 2.2-2.5 mg/dl (194-221 μmol/l).
•Maintenance immunosuppression: Cy-A, MMF, and low-dose steroids mg/day).
•Fourteen months after TX recruitment to a clinical trial of cyclosporine withdrawal in patients with chronic allograft dysfunction. Conversion to rapamycin was performed after ruling out rejection or glomerular disease (protocol biopsy).
•After 9 months of rapamycin therapy (12- 20 ng/ml), sCr increased from 2.5 mg/dl to 4.0 mg/dl (221-354 μmol/l), and proteinuria of 2.5 g/ 24 h developed.





Differential diagnosis
•Chronic TX Glomerulopathy
•Immune complex mediated GN
•Thrombotic microangiopathy

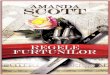
C4d

C4d C3



C4dC4d C4d




Diagnosis
•De novo IC mediated Glomerulonephritis (likely related to the switch from CNI to rapamycin)
•No convincing evidence of acute rejection (C4d negative)
•Medullary only mononuclear inflammatory infiltrate

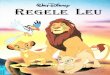
IC GN after rapamycin switch
MGN IgA-GN IgA-GN

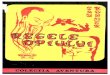
Clinical course
Dittrich E, Transpl Int 2004

C4d


Evidence for pro-inflammatory properties of rapamycin
Recurrent or de-novo GN develops in allografts after conversion to sirolimus and recovery can be achieved by re-introducing of CNI
Säemann MD, AJT 2009

Immunosuppression and transplant glomerulonephritis
A USRDS analysis of 41272 transplant recipients found recurrent GN causing graft loss in 2,6% of patients
The likelihood of developing a recurrent GN was not associated with a specific type of immunosuppressive regimen
Any change of immunosuppression however increased the risk of developing recurrent GN
Mulay AV, AJT 2009

Evidence for pro-inflammatory properties of rapamycin
Drug dependent occurrence of fever and inflammation (unrelated to infection) in different organs
Recurrent or de-novo GN in allografts after conversion to sirolimus and recovery after re-introduction of CNI
Sirolimus treatment leads to exacerbation of lesions in some experimental models of autoimmune disease.
Säemann MD, AJT 2009

Different effects of rapamycin in innate and adaptive immunity
Säemann MD, AJT 2009