Embed Size (px)
Citation preview

SHORT REPORT
Simultaneous Endovascular Exclusion of Thoracic AorticAneurysm with Open Abdominal Aortic Aneurysm Repair
J. Szmidt,1* O. Rowinski,2 Z. Gałazka,1 T. Jakimowicz,1 S. Nazarewski,1
T. Grochowiecki1 and R. Pacho2
Departments of 1General, Vascular and Transplant Surgery, and 2Radiology, Medical University of Warsaw,Warsaw, Poland
Background. The treatment of aneurysms at multiple sites within the aorta is problematic.Methods. Between March 2002 and June 2003 in the Department of General, Vascular and Transplant Surgery, MedicalUniversity of Warsaw six patients with coexisting abdominal and descending thoracic aortic aneurysms underwentsimultaneous open abdominal aortic aneurysm (AAA) repair and endoluminal thoracic aortic aneurysm (TAA) repair. Theindication for a combined procedure was a diagnosed descending TAA and AAA with no significant risk factors for openaortic surgery or technical contraindications for endovascular treatment of TAA.Results. One patient died in the peri-operative period while the other five patients all recovered well after surgery and weredischarged with both aneurysms excluded.Conclusion. Endovascular treatment of TAA combined with a simultaneous open AAA repair is an efficient and relativelysafe treatment modality in patients with TAA and AAA disqualified from endovascular repair. The fact that thoracotomy isnot a necessity significantly lowers the complication rate in these patients.
Key Words: Multilevel aortic aneurysm; Endovascular thoracic aortic aneurysm treatment; Open abdominal aorticaneurysm surgery.
Introduction
Multilevel aortic aneurysms poses a serious problemfor vascular surgeons in the terms of choice of anadequate surgical method of treatment. Open surgeryis still associated with significant morbidity andmortality especially in patients with thoracic aorticaneurysms (TAA).1–3 Ten to 29% of patients with TAAhave coexisting abdominal aortic aneurysms (AAA).2,4
Historically, multilevel aortic surgery was performedin these patients simultaneously or subsequently.5 Analternative to open surgery could be stentgraft place-ment for TAA and AAA.4 AAA morphology is notalways suitable for endovascular repair (short orconical neck, severe angulations of the neck or iliactortuosity). Additionally, in some patients a goodresult of open aneurysm repair can be predicted. Insuch cases simultaneous stentgraft placement for TAAcombined with open repair for AAA may be a viable
method of treatment. It allows for a lower compli-cation risk, than for a procedure associated with openthoracotomy and high aortic cross-clamping andexcludes both aneurysms from circulation.
Patients and Methods
Between March 2002 and June 2003 in the Departmentof General, Vascular and Transplant Surgery, MedicalUniversity of Warsaw six patients with coexistingAAA and TAA underwent simultaneous openabdominal aneurysm repair and stentgraft placementthrough the implanted gelatin-coated Dacron abdomi-nal vascular prosthesis side limb. This group ofpatients consisted of two females and four maleswith a mean age of 70 years, four of whomwere heavysmokers. Four patients from this group sufferedsignificant co-morbidities including hypertension (4),coronary artery disease (4), history of myocardialinfarction (2), COPD (1) and diabetes (1). Two patients
Eur J Vasc Endovasc Surg 28, 442–448 (2004)
doi: 10.1016/j.ejvs.2004.06.008, available online at http://www.sciencedirect.com on
*Corresponding author. J. Szmidt, Department of General, Vascularand Transplant Surgery, Banacha 1a, 02-097 Warszawa, Poland.
1078–5884/040442+ 07 $35.00/0 q 2004 Elsevier Ltd. All rights reserved.

had also occlusive iliac disease. Patient characteristicsare shown in Table 1.
The aneurysms were detected clinically (1), orincidentally on plain X-ray (2), abdominal ultrasound(1) or echocardiography (2). In all cases contrast-enhanced thoracoabdominal spiral computed tom-ography (3 mm slides) were performed to measureabdominal and thoracic aneurysm diameters withevaluation for stentgraft implantation. Three dimen-sional reconstruction and angio-CT were performed(Fig. 1). In addition in two cases digital subtractionangiography was performed to attain a clearermorphology of the aortic arch. The indication for acombined procedure was a diagnosed descendingTAA and AAA with technical contraindications forendovascular treatment or no significant risk factorsfor open abdominal aortic surgery (patient nos. 1 and5). All thoracic aneurysms began below the leftsubclavian artery ostium. All except one abdominalaneurysm were infrarenal, with one suprarenal aneur-ysm involving the celiac trunk and superior mesen-teric artery. Preoperative measurements are shown inTable 2.
For TAA exclusion, Talent (Medtronic) straight tubedevices were used. The graft length exceeded theaneurysm length by approximately 3–4 cm anddiameter oversizing was 10–15% (4–6 mm). In twopatients low molecular weight heparin was adminis-tered for 5 days preoperatively. Prior to surgery,informed consent was obtained from all patients forthoracotomy. The patients were prepared and drapedas for thoracoabdominal surgery. All procedures wereperformed in the operative theatre under generalanesthesia. In all cases a transperitoneal abdominalmidline approach was used. After heparinization(70 IU/kg), aortic cross-clamping was performed inthe infrarenal aortic segment except in the patient witha suprarenal aneurysm. In all patients a bifurcatedgelatin-coated Dacron prosthesis (Uni-graft; Braun)was used. After the upper and contralateral limbanastomosis was completed, the aorta was de-clamped and through the ipsilateral limb of thevascular prosthesis a Talent straight tube graft wasplaced under fluoroscopic guidance (Fig. 2). Finalangiography revealed complete exclusion of thoracicaneurysm with no endoleak (Fig. 3). After all catheterswere removed the ipsilateral limb was completed.Abdominal wall closure completed surgery and thepatient was transferred to intensive care unit.
Results
In one case the AAA involving the celiac trunk, Table
1.Patientch
aracteristics
Patient
Age
Sex
Coronary
disease
present
History
ofMI
Hypertension
Cereb
rovascu
lar
disease
COPD
Diabetes
Ren
aldysfunction
Obesity
Smoking
High
lipid
level
Occl.
iliacdis.
Preoperative
coag
ulopathy*
164
MNo
No
No
No
No
No
No
No
Yes
Yes
No
No
272
MYes
yes
No
No
No
No
No
No
No
No
No
No
377
FYes
No
Yes
No
No
Yes
No
Yes
Yes
Yes
Yes
Yes
473
MYes
Yes
Yes
Yes
No
No
No
Yes
No
Yes
Yes
No
569
FNo
No
Yes
No
No
No
No
No
Yes
Yes
No
No
667
MYes
No
Yes
No
Yes
No
No
No
Yes
No
No
Yes
Overall
702F
/4M
4/6
2/6
4/6
1/6
1/6
1/6
0/6
2/6
4/6
4/6
2/6
2/6
MI,myocardialinfarction;COPD,ch
ronic
obstructivepulm
onarydisease.
*Ifpresentlow
molecu
larweighthep
arin
was
administered5day
spreoperatively.
Simultaneous Endovascular Exclusion of Thoracic Aortic Aneurysm 443
Eur J Vasc Endovasc Surg Vol 28, October 2004

superior mesenteric artery and renal arteries. In thispatient an intraoperative coagulopathy developedwhich required plasma and blood transfusion andrecombinant human coagulation factor VIIa. Twohours after primary abdominal closure a relaparotomywas performed due to persistent intra-abdominalhemorrhage. Intensive management with blood trans-fusion, recombinant human coagulation factor VIIaand abdominal packing was ineffective and the patientdied 1 h after the second operation.
In all remaining cases, after a one day ICU stay thepatient returned to the Department ward. Pre-dis-charge CT-scan revealed complete thoracic aneurysmexclusion and no endoleak (Fig. 4). No other earlypostoperative complications occurred, in particularthere were no cases of spinal cord ischemia. In thefollow-up period (8–23 months) CT-scans wereperformed on the third, sixth and 12th monthspostoperatively. We detected one type I endoleak dueto thoracic stentgraft migration in a 6 months CT scan,which was treated by implanting an additionalproximal stentgraft segment. No other types of
endoleak were observed. There were no migration,aneurysm expansion, and any other complicationsassociated with thoracic stentgraft placement orabdominal aneurysmectomy. No neurological defectswere observed in this follow-up time. Detailed resultsare shown in Table 3.
Discussion
Since the first endovascular repair of a thoracic aorticaneurysm in 19926 there has been a significant increasein the numbers and indications for stentgraft implan-tation for diseases of the descending aorta. Thisprocedure has rapidly become a valuable alternativefor thoracic aneurysm treatment.6–9 If the patient isconsidered to be a candidate for endovascular treat-ment, careful assessment of TAA morphology shouldbe performed. The aneurysm should not exceed theleft subclavian artery proximally and there should bean adequate landing zone distally withoutinvolvement of major aortic branches. However,
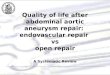
Fig. 1. CT of patient with TAA (A) and AAA (B) with 3D angio-reconstruction (C).
J. Szmidt et al.444
Eur J Vasc Endovasc Surg Vol 28, October 2004

multifenestrated devices may allow for a more wide-spread use of stentgafts in aneurysms involvingcollateral vessels.4
There is a very little data available for combinedthoracic and abdominal aneurysm repair. Accordingto Moon et al. historically, there were several ways ofsurgical treatment of multilevel aortic aneurysms.2
Simultaneous thoracic and abdominal aneurysmrepair is a challenging surgical procedure, which canalso be performed through separate incisions. Theoperation can be staged in time, and the order shouldbe determined in accordance to aneurysm size andT
able
2.Preoperativemeasu
rements
ofAAA
andTAA
accordingto
CT-scan
AAA
TAA
Patient
Diameter
Ren
ala.
involvem
ent
Proxim
alneck
diameter
Proxim
alnecklength
Proxim
alneck
angulation
Iliaca.
involvem
ent
Significant
iliactortuosity
Feasible
for
endovascrepair
Diameter
Len
gth
Proxim
alnecka
diameter
Proxim
alneckalength
145
bNo
2450
Yes
(608)
Right
common
No
Yes
6197
2913
5
265
No
2128
No
No
Yes
No
9110
431
423
51No
248
Yes
(908)
No
No
No
6521
034
164
74Yes
––
–No
No
No
8764
3513
75
69No
2431
No
No
No
Yes
7353
3114
26
71No
2247
Yes
(808)
Both
common
No
No
5957
3224
Alldim
ensionsarein
mm.
aas
measu
redfrom
theleftsu
bclav
ianartery
ostium.
bSymptomatic
AAA.
Fig. 2. Thoracic stentgraft placement through the limb of theabdominal vascular prothesis.
Simultaneous Endovascular Exclusion of Thoracic Aortic Aneurysm 445
Eur J Vasc Endovasc Surg Vol 28, October 2004

symptoms. Crawford suggested an initial repair of thethoracic aneurysm in asymptomatic patients.10,11 Onthe other hand 30% of deaths after descending thoracicaneurysm repair is associated with coexistinguntreated infrarenal aneurysm rupture.12 In accord-ance with this data, Crawford performed simul-taneous surgery in patients who continued to dowell in the operating room after the first replacement.The mortality rate for such a procedure was 10%.11 It isalso possible to exclude coexisting TAA and AAA bymeans of thoracic and abdominal stentgrafts. This canbe performed simultaneously or subsequently and is aviable alternative for high risk patients.4 According tomany authors there is no reason for endovascularAAA repair in patients without significant risk factors.In our opinion in patients with multilevel aneurysmalaortic disease the choice of treatment of the concomi-tant AAA should be the same as in patients with AAAonly. The presence of TAA should not modify thetreatment method of the AAA.
Eton reports a case of thoracic stentgraft implan-tation two weeks after open abdominal aneurysmect-omy in a patient with a suspected mycotic thoracicaneurysm.8 Nevertheless if there is no contraindica-tion, both aneurysms should be excluded simul-taneously. This seems a much simpler approach,with the straight tube thoracic graft inserted throughthe limb of the abdominal prosthesis, with noadditional groin incision.
When considering patients with thoracoabdominal
aneurysms it is obligatory to evaluate the patient’scardiopulmonary status. Many patients because oftheir poor cardiopulmonary reserve can still beconsidered for a combined procedure where theywould be otherwise unfit for open thoracotomy. In ourseries at least in two patients open thoracotomy couldnot be performed due to poor cardiopulmonary status.
A serious problem following endovascular andopen repair of thoracic aortic aneurysms is spinalcord ischemia. According to current literature thecomplication rates are equal in both methods oftreatment. Steroids, hypothermia, cerebrospinal fluiddrainage and prevention of hypertension may beoffered to lower the risk of this complication. Overall,the rate of this complication has been shown to rangebetween 0 and 21%.3,4,13–15
The spinal cord is predominantly supplied with
Fig. 3. Final intraoperative angiography of thoracic aorta-complete exclusion of the aneurysm with no endoleak.
Fig. 4. Pre-discharge CT-scan 3D reconstruction of the aorta.
J. Szmidt et al.446
Eur J Vasc Endovasc Surg Vol 28, October 2004

blood through the Adamkiewicz artery and also bythoracic intercostal arteries, which are usually throm-bosed through the aneurysm. Due to this fact thesebranches are very rarely reimplanted during opensurgery.16 In our study all grafts were placed relativelyhigh. Because of this placement and the short graftlength there was little risk in covering the Adamkie-wicz artery and therefore no need to use spinal cordprotection.
In conclusion, endovascular treatment of thoracicaortic aneurysm combined with a simultaneous openabdominal aneurysmectomy is an efficient and rela-tively safe treatment modality in patients with TAAand AAA disqualified from endovascular repair. Thefact that thoracotomy is not a necessity significantlylowers the complication rate after this procedure.However, long-term follow-up on a larger group ofpatients is necessary to assess the durability andeffectiveness of this method of therapy.
References
1 Svensson LG,Crawford ES,Hess KR et al. Experience with 1509patients undergoing thoracoabdominal aortic operations. J VascSurg 1993; 17:357–368.
2 Moon MR, Mitchell RS, Dake MD et al. Simultaneousabdominal aortic replacement and thoracic stent-graft placementfor multilevel aortic disease. J Vasc Surg 1997; 25:332–340.
3 Ballard JL, Abou-Zamzam AM, Teruya TH. Type III and IVthoracoabdominal aortic aneurysm results of a trifurcated/twograft technique. J Vasc Surg 2002; 36:211–216.
4 Meguid AA, Bove PG, Long GW et al. Simultaneous stent-graftrepair of thoracic and infrarenal abdominal aortic aneurysms.J Endovasc Ther 2002; 9(2):165–169.
5 Gloviczki P, Pairolero P, Welch T et al. Multiple aorticaneurysms: the results of surgical management. J Vasc Surg1990; 11:19–28.
6 Dake MD, Miller DC, Semba CP et al. Transluminal placementof endovascular stent-grafts for the treatment of descendingthoracic aortic aneurysms. NEJM 1994; 331:1729–1734.
7 Saccani S, Nicolini F, Beghi C et al. Thoracic aortic stents: acombined solution for complex cases. Eur J Vasc Endovasc Surg2002; 24:423–427. doi:10.1053/ejvs.2002.1687.
8 Eton D, Terramani T, Katz M. Staged thoracic and abdominalaortic aneurysm repair using stent graft technology and surgeryin a patient with acute renal failure. Ann Vasc Surg 2000; 14:114–117. doi: 10.1007/S100169910021.
9 Orend KH, Scharrer-Palmer Z, Kapfer X et al. Endovasculartreatment in diseases of the descending thoracic aorta: 6-yearresults of a single center. J Vasc Surg 2003; 37:91–99.
10 Crawford ES, DeNatale RW. Thoracoabdominal aortic aneur-ysm: observations regarding the natural course of the disease.J Vasc Surg 1986; 3:578–582.
11 Crawford ES. Aortic aneurysm: a multifocal disease. Arch Surg1982; 117:1393–1400.
12 Crawford ES,Walker HSJ, Saleh SA et al. Graft replacement ofaneurysm in descending thoracic aorta: results without bypass orshunting. Surgery 1981; 89:73–85.
13 Graveraux EC, Faries PL, Burks JA et al. Risk of spinal cordischemia after endograft repair of thoracic aortic aneurysms.J Vasc Surg 2001; 34:997–1003.
14 Azizzadeh A, Huynh TT, Miller CC et al. Postoperative riskfactors for delayed neurologic deficit after thoracic and thor-T
able
3.Operativedata
andresu
lts
Patient
Number
ofthoracicsten
tgraft
segmen
tsused
Intrao
per.
endoleak
Typeofab
dominal
distal
anastomosis
Durationof
procedure
(min)
Bloodlost
(ml)
Neu
rologic
defi
cit
30-day
sresu
lts
Follow-up
(months)
Complicationsin
follow-up
12
No
Comm.iliac
170
800
No
Cured
23None
22
No
R-comm.iliacL-ext.iliaca
200
1000
No
Cured
22None
32
No
Ext.iliaca
240
700
No
Cured
19None
41
No
Comm.iliac
330
5000
–Diedb
––
51
No
Comm.iliac
150
500
No
Cured
11None
62
Yes
cext.iliacd
180
1200
No
Cured
8Endoleak
typeIin
6thmonth
aDueto
severeatherosclerosis.
bDiedduringreoperationdueto
persisten
thaemorrhag
e.c Treated
byad
ditional
sten
tgraftsegmen
tplacemen
t.dDueto
aneu
rysm
alcommoniliacarteries.
Simultaneous Endovascular Exclusion of Thoracic Aortic Aneurysm 447
Eur J Vasc Endovasc Surg Vol 28, October 2004

acoabdominal aortic aneurysm repair: a case-control study. J VascSurg 2003; 37:750–754.
15 Kuniyoshi Y, Koja K,Miyagi K et al. Prevention of postoperativeparaplegia during thoracoabdominal aortic surgery. Ann ThoracSurg 2003; 2003(76):1477–1484. doi: 10.1016/S0003-4975(03)00871-3.
16 Jacobs MJ, de Moll BA, Elenbaas T et al. Spinal cord blood
supply in patients with thoracoabdominal aortic aneurysms.
J Vasc Surg 2004; 35(30):37. doi: 10.1067/mva.2002.120041.
Accepted 7 June 2004
Available online 29 July 2004
J. Szmidt et al.448
Eur J Vasc Endovasc Surg Vol 28, October 2004