Embed Size (px)
Citation preview
Sickness Insurance Management Contributions for Improving Efficiency
Jos£ RRAZ m.rm s"
ABSTRACT
Successful rehabilitation programs are important for the performance of a firm, the welfare of workers, and productivity in society. Researchers have only considered absenteeism caused by injuries and sickness in accordance with Swedish social insurance for sickness, that is, absenteeism classified as such as a result of bad health. Case managers make a judgement regarding each individual classified as long-term sick. Managers assess the possibility of rehabilitation at a given time, indicating the probability for the worker to become healthy under the condition that the individual receives the prescribed interventions. In this article, the degree of success of rehabilitation programs will be measured, comparing the goals specified with the performance achieved. This evaluation seeks to contribute to the improvement of cost effectiveness. (JEL J20)
INTRODUCTION
This article examines an experiment designed to reduce long-term absemeeism due to sickness and injury in a large Swedish industrial firm in G0teborg. The goal of that experiment was to implement techniques to access conduct and performance of the rehabilitation process, analyzing how to measure effectiveness of rehabilitation managers and why effectiveness is also important to economic efficiency. During the period examined (1990-93), approximately 15 percent of the work force was absent due to sickness at any given time in this company. Absenteeism is higher for women and blue-collar workers and increases with age. The average age of a blue-collar worker with long periods of absence due to sickness is about 40 years. The situation in this company is nearly identical to society in general. About 8 percent of the adult population between 18 and 65 years of age is absent from work with sick leaves longer than 60 days, and an additional 8 percent receive early pensions due to bad health and market-related problems.
Successful rehabilitation programs are important for the performance of a firm, the welfare of workers, and productivity in society. Work injuries can result in poorer health and prevent injured individuals from pursuing their usual tasks at their workplace, in addition to disrupting home and social life. Sickness may also cause impairments that lead to work-disability and diminished well- being in general. The work place and the production process may affect sickness. However, the degree of correlation between the production process and sickness is not always so straightforward. Neither is the degree of relationship between injuries, sickness, and work-disability. The author only considered absenteeism caused by injuries and sickness in accordance with Swedish social insurance for sickness, that is, absenteeism classified as such as a result of bad health.
Assessment of Rehabilitation Programs Rehabilitation services aim, in this context, to remove impairments in any degree in order to get
individuals with sick-leave to return to work. Social insurance in Sweden covers the entire working
*G0teborg University, Sweden.
288
AUGUST 1995, VOL. 1, NO. 3 289
population. If the number of sick cases or the length of sick leave increases, the total outlay in social insurance increases too. At the same time, the number of individuals in the work force in relation to the total number of insured individuals decreases and, consequently, the revenue in social insurance also decreases. This situation will affect either the level of contribution to social insurance or the level of compensation to sick individuals. Another alternative is to use rehabilitation actions to try to decrease the number of sick days that are compensated by social insurance. Local social insurance officers consider the special rehabilitation programs for individuals by purchasing services in addition to health care services that are financed by other funds. The expectation is that a greater number of individuals shall return to the labor market, either to their former work place or anothe,r. The rehabilitation philosophy has a strong vocational emphasis, rather than a strong medical one. This reflects that disability due to work is not only a question of health status, but also the degree of adjustment between individuals' characteristics and the demands of the labor market.
Nevertheless, the author uses the expression "healthy" as the degree of ability to work which will depend on improvements in health states as well as other factors within the labor market and the organization of social insurance. In this context, the goal of evaluation is to measure the effectiveness of case managers as purchasers of services within a budget constraint. Allocation of the scarce resources depends on the ability of case managers to decide which type and quantity of services shall be delivered or not to each sick individual.
The degree of success of rehabilitation programs will be measured, comparing the goals specified with the performance achieved. The measure of outcome shall not be controlled by case managers and shall correspond with the expectations of the insurance payers, both individuals and the firms. Of primary concern is the question of efficiency of the rehabilitation programs. In this context, efficiency is essentially improving the success of rehabilitation programs, contributing to an increase in the ratio between the value of what is produced and what is given up in rehabilitation services.
THE REHABILITATION PROGRAMS
Case managers are the subjects of this assessment. It means that there is some officer or a team of officials making an assessment of the possibilities for the sick person to return to work within a given period of time. This assessment depends upon the ability to implement a rehabilitation program. Case managers should have a good knowledge of the problem and how to solve it. Moreover, the necessary program must be applied at the right time. There are three stages that must be included in the assessment:
1) Prognosis: Case managers make a judgement regarding each individual classified as long- term sick. Managers assess the possibility of rehabilitation at a given time, indicating the probability for the worker to become healthy under the condition that the individual receives the prescribed interventions. 2) Actions: These are supposed to be necessary for the rehabilitationprocess. Different types of interventions within different rehabilitation approaches consume resources to different degrees. These actions correspond to services purchased by rehabilitation managers. 3) Performance: Outcomes have to be defined and registered. They constitute measures of performance for rehabilitation approaches. In this study, a special unit of the Rehabilitation Department of Sickness Insurance in
Gothenburg, Sweden was observed. This unit has some peculiarities as compared to others. A group of officials was placed at a large firm. Their aim was to work closely with the firm and the union in order to achieve a better performance in the process of rehabilitation. Thus, it was possible to follow all the cases subjected to rehabilitation approaches. Looking at the Special Unit
290 INTERNATIONAL ADVANCES IN ECONOMIC RESEARCH
of Sickness Insurance (SUSI) of the industrial firm at a given date, one sees that there are approximately 300 individuals with long-term, ongoing sickness periods submitted for rehabilitation programs. These individuals are "cases" for officials in SUSI.
Officials of SUSI, also known as case managers, make assessments of the degree of possible rehabilitation one year after the date of observation, under the condition that any of the following activities take place:
1) Social insurance's own activities; 2) Medical and hospital care; 3) Therapist services; 4) Social activities organized by the municipalities; 5) Organizational actions at the firm; 6) Physical training at the firm; 7) Vocational education programs at the firm; 8) Labor market actions outside the firm; and 9) Further general education programs. For one entire year after the assessment day, the author followed all cases and noted the actions
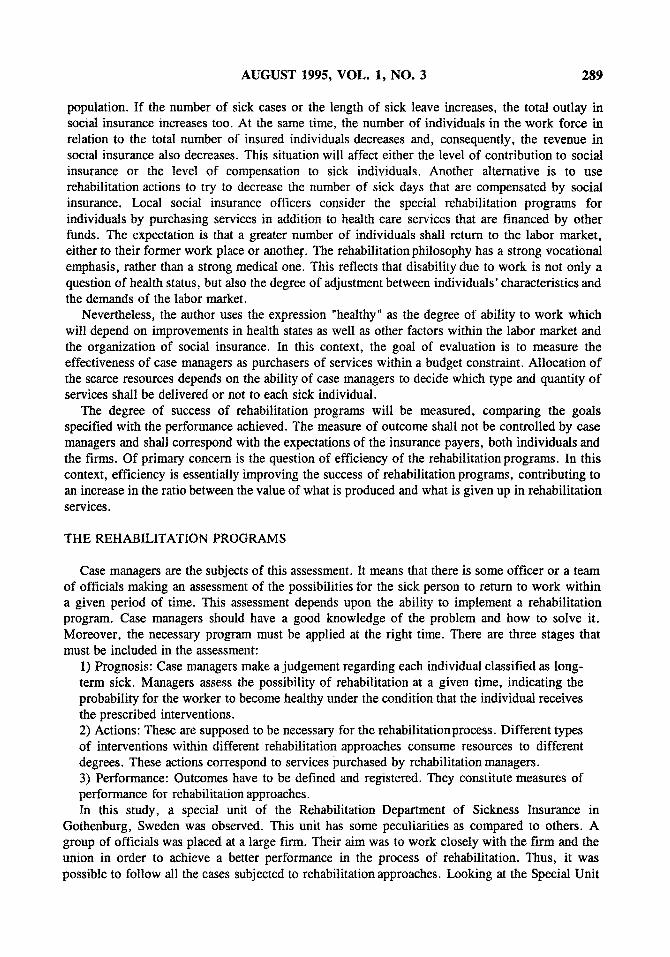
actually taken, thereby knowing about the type of intervention, the number of interventions of each type, and the costs per unit of intervention (for each individual). In order to measure outcomes, the author registered the loss of working days for each individual for a period of six months, beginning one year after the assessment day. Thus, an index could be constructed that reveals the degree of participation in the labor force during a six-months period. This "healthy day's index" is a measure of performance. A more efficient organization of rehabilitation approaches should improve the healthy day's index. If the healthy day's index improves for a given budget, the cost effectiveness ratio also shows an improvement.
FIGURE 1 The Registration of Data
Prognosis Assessment day
Performance
12 months 6 months
Actions Healthy days
• •
Prognosis i is the probability of becoming healthy under the condition that action i is undertaken with values between 0 and 1. Actionj exists if intervention of type j is taken or not. Its values can be either 0 or 1. Performance is the degree of participation in the labor force, including unemployed individuals during a period of six months, with values between 0 and 1.

AUGUST 1995, VOL. 1, NO. 3 291
THE PAP MODEL
A model based on the prognosis, the actions taken, a~d performance (PAP) was tested for SUSI during 1991-92 and 1992-93 at the chosen large firm. Three hundred rehabilitation cases each year are represented in this investigation.
The state of an individual at time t is defined by a selector function:
E (t) = { 1 if the individual receives action k, { 0 otherwise.
A healthy day's index measuring the degree of return to work is defined for periods (tl, t2) as:
t 2 E,=~, E ( t ) S -
t 2 - t 1
For the treatment of a sick individual K, possible actions A k, k = 1 .. . . . K are undertaken, so that:
A k = { 1 if the individual receives action k, { 0 otherwise.
For each of these actions, a prognosis is given by assessing the likelihood of rehabilitation for the observed individual. The assessment is expressed as the subjective probability P, of return to work (being healthy) at time t, subject to the condition that specific measures k are taken, as assessed by the manager.
The actual prognosis is given by the formula:
k k
F [ E ( t ) = O ] = E A , 1 P ' ~ t - ~, A , z p a 2 A , ~ 1 P '~1 a l = 1 a 2 > a l = 1
k
+ E A 3 P ~ 3 A ~ 2 P ~ Z A I P al a 3 > o r2 > a l = 1
- ( - 1 ) k - l A ~ k P'~kA,~ 1 p ' ~ .
This formula expresses the probability as assessed by the rehabilitation manager for the worker to become healthy, given all possible actions. Thus, one may estimate the model:
S i : oz + ~ F i + e i . ( 1 )
Note that this is not a qualitative response model, because variable S/can take all values between 0 and 1. In fact, this is a variable truncated above t and below 0. An alternative specification would be:
e a + ~ F i S i - (2)
i + e °z+13Fi +Ei "
292 INTERNATIONAL ADVANCES IN ECONOMIC R E S E A R C H
This specification will always give estimates 0 < S i < 1 for all values of F t. However, given that for the actual value of F i in the sample, it is always 0 < S i < 1. Then by estimating (2), one has no real gains. On the other hand, one gets estimates with small sample properties.
The model (1) can be extended in order to allow for other effects that influence the outcome healthy days. It was not possible to consider more than two characteristics that are supposed to be explanatory variables. The empirical analysis is based on the total population of individuals in a large enterprise with similar characteristics such as work conditions, skills, wage, education, and union status. Other relevant characteristics that can be used are age and gender. The first one is quite obvious, but the condition of being male or female is more controversial. It is known that women represent a relatively larger part of long-term sick individuals. On the other hand, there is no immediate rationale to believe that it is more difficult to rehabilitate individuals with those characteristics. One may estimate another model that is an expansion of (t) , where X is a vector of individual characteristics:
S i : a + B F i + , ~ X + e i . (3)
RESULTS
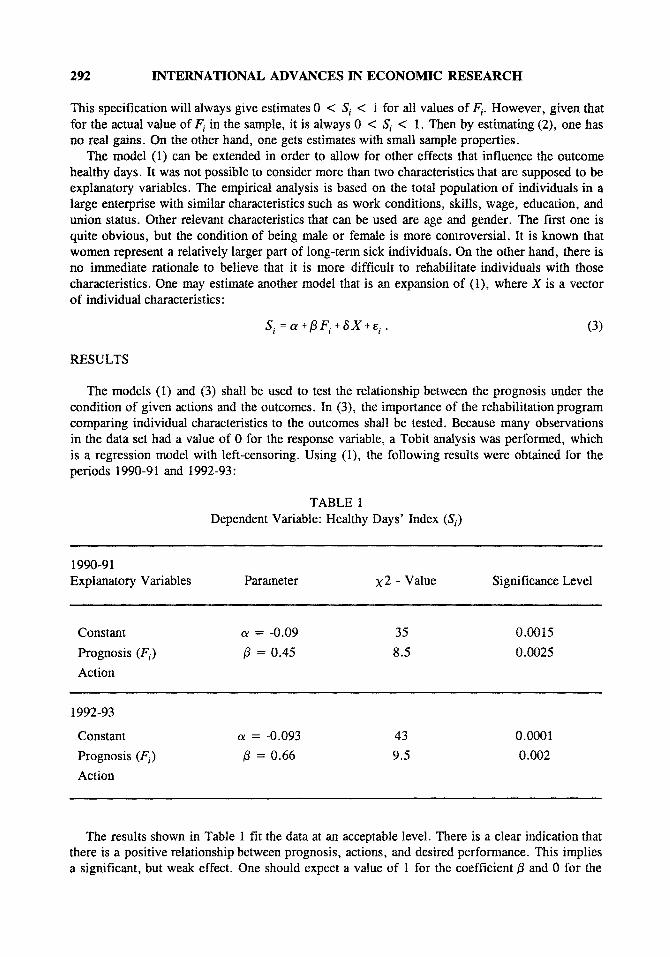
The models (1) and (3) shall be used to test the relationship between the prognosis under the condition of given actions and the outcomes. In (3), the importance of the rehabilitation program comparing individual characteristics to the outcomes shall be tested. Because many observations in the data set had a value of 0 for the response variable, a Tobit analysis was performed, which is a regression model with left-censoring. Using (1), the following results were obtained for the periods 1990-91 and 1992-93:
TABLE 1 Dependent Variable: Healthy Days' Index (Si)
1990-91 Explanatory Variables Parameter X 2 - Value Significance Level
Constant ~ = -0.09 35 0.0015
Prognosis (Fi) # = 0.45 8.5 0.0025
Action
1992-93
Constant c¢ = -0.093 43 0.0001
Prognosis (F~.) /3 = 0.66 9.5 0.002
Action
The results shown in Table 1 fit the data at an acceptable level. There is a clear indication that there is a positive relationship between prognosis, actions, and desired performance. This implies a significant, but weak effect. One should expect a value of 1 for the coefficient/3 and 0 for the
AUGUST 1995, VOL. 1, NO. 3 293
coefficient o~. That would represent the "perfect manager." The constant is highly significant in both years. It indicates that other variables explain the capacity of successful rehabilitation rather than those used in rehabilitation programs. The value of the constant is higher for 1991, which means that the problem is greater in this year. Prognosis overvalues the probability of becoming healthy as a result of rehabilitation activities, and undervalues the possibility of individuals becoming healthy without these activities. This is particularly relevant for the years 1990-91.
An improvement can be observed between 1991 and 1993. Especially important is the change in the value of the parameter/3. It implies a stronger relationship between prognosis/activities and outcome. The assessment made by managers was better in 1992 as compared to 1990, reflecting a more accurate judgement and allocation of the budget among purchased rehabilitation services in a more efficient way. In this case, the change in the value of /3 can be interpreted by an improvement because the prognosis made by managers was quite the same in the two observed periods. Otherwise, one should be careful in interpreting changes in the values of parameters because they could be a consequence of lower values in the assessment of the likelihood of rehabilitation activities that are purchased. In this experiment, increased values in the outcomes explain the observed changes in parameter/3, while parameter tx remains unchanged. Technology was changed between 1990-91 and 1992-93, by reallocation in the vector of inputs in the rehabilitation program, varying by individuals and type of activity.
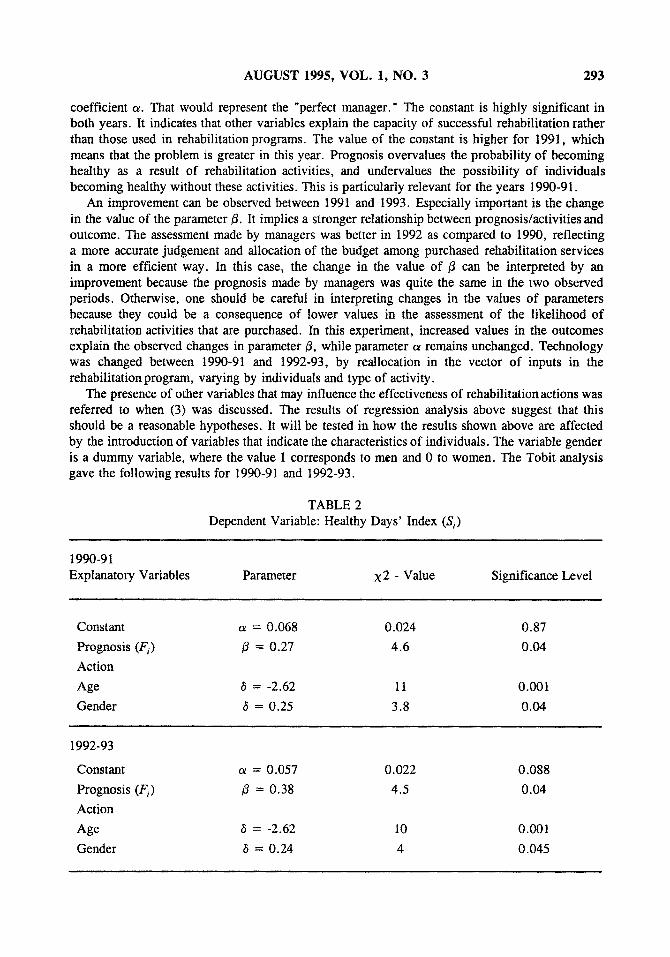
The presence of other variables that may influence the effectiveness of rehabilitation actions was referred to when (3) was discussed. The results of regression analysis above suggest that this should be a reasonable hypotheses. It will be tested in how the results shown above are affected by the introduction of variables that indicate the characteristics of individuals. The variable gender is a dummy variable, where the value 1 corresponds to men and 0 to women. The Tobit analysis gave the following results for 1990-91 and 1992-93.
TABLE 2 Dependent Variable: Healthy Days' Index (Si)
1990-91 Explanatory Variables Parameter X2 - Value Significance Level
Constant c¢ = 0.068 0.024 0.87
Prognosis (Fi) /3 = 0.27 4.6 0.04
Action
Age t5 = -2.62 1t 0.001
Gender 6 = 0.25 3.8 0.04
1992-93
Constant ot = 0.057 0.022 0.088
Prognosis (F i) /3 = 0.38 4.5 0.04
Action
Age 6 = -2.62 10 0.001
Gender 6 = 0.24 4 0.045

294 INTERNATIONAL ADVANCES IN ECONOMIC RESEARCH
The results in Table 2 suggest that age and gender are, in this case, the important variables outside rehabilitation actions that influence outcome. There is some evidence that men are rehabilitated more successfully to a higher degree than women. One explanation for this may be based on the stronger position of men in the labor market. It is also important to point out that this model confirms the differences of effectiveness due to rehabilitation actions between 1991 and 1993.
CONCLUSION
The results of the PAP model presented above may be interpreted within the framework of improvements in economic efficiency. The budget for the rehabilitation program did not increase between the two observed periods. As long as total costs of the rehabilitation program remain unchanged, and the outcomes of the entire program improved in 1993 as compared to 199t, the cost effectiveness increased as a result of reaUocations in purchasing rehabilitation services. The analysis presented is essentially an assessment of case managers as one important part of studies that aim at economic and social efficiency. The model may explain the degree of effectiveness in the process of purchasing services, which depends on two aspects: the ability of case managers to understand individuals' problems and to know which allocation of resources is the best to achieve the goals.
The consequences of rehabilitation actions in different periods, or between programs in different places, can be caused by variables that have not been included in the purchased services. The interpretation of the model is, therefore, dependent on the assumption of vector X explained in (3). In the analysis presented here, the influence of gender and age is clear in both years with the same results. Other variables are possible to include in vector X, especially if other conditions can be assumed to be important for explaining variations among individuals.
These considerations are of vital importance to the purchasers in order to determine the actions that are relevant for achieving the goals of rehabilitation programs. One important point is that the outcomes shall be defined in a way that fits the main goal of rehabilitation. This goal may differ depending on the context of the purchaser or on the level on which the problem will be considered. The techniques to analyze cost effectiveness can be the same, independent of the variables that are used.
REFERENCES
Baumol, W. "Towards a Theory of Public Enterprise," Atlantic Economic Journal, 1984. Cullis, J. Benefit-Cost Analysis of Government Programs, New York, 1986. Evans, R. "Public Health Insurance," Health Policy, 1987. Holloway, C. A. Decision Making Under Uncertainty, Prentice-Hall, 1979. Hunt, S. M. Measuring Health Status, London: Croom Helm, 1986. Maynard, A. The Economic Evaluation of Rehabilitation, York, 1992. Olson, M. Evaluating Performance in the Public Sector, New York, 1973. Palmer, E. "The Implications of Social Change to Social Security," in Quantitative Analysis and Planning of
Social Protection, Geneva, 1992. Tobin, J. "Estimation of Relationships for Limited Dependent Variables," Econometrica, 26, 1958. Torrance, G. W. "Toward a Utility Theory Foundation for Health Status Index Models," Health Services
Research, 1976. Williams, A. Ethics and Efficiency in the Provision of Health Care, Cambridge, 1988. . "Quality-Adjusted Life-Years," Lancet, 1987.
![INDEX [vnit.ac.in]vnit.ac.in/wp-content/uploads/2018/08/bookletvnitmedical.pdf · improving concentration and immunity thus preventing sickness and absenteeism. 4. Hygiene and related](https://img.dokumen.tips/doc/110x75/5f0ac2a57e708231d42d350d/index-vnitacinvnitacinwp-contentuploads201808-improving-concentration.jpg)