Embed Size (px)
Citation preview

50
SHOULDER JOINT PATHOLOGY – IMPROVED DIAGNOSIS BY MAGNETIC RESONANCE IMAGING (MRI):
A PICTORIAL ESSAY AND REVIEW
Andreas NIDECKERIMAMED Radiologie Nordwest, Basel, Switzerland
ABSTRACTThis paper describes the personal experience of the author with Shoulder Arthro MR. This imaging method is put
into perspective with other, more widely used diagnostic methods, which also have their advantages. Indications for Shoulder Arthro MR are discussed and details on the technique and interpretaton are given. Also major shoulder pathol-ogy as impingement, rotator cuff tears and instability is discussed. Furthermore a review of the spectrum of pathology in 100 consecutively examined patients is made and treatment and outcome are listed. Lastly a pictorial review of typ-ical pathologies in MR pictures is supplemented. After x-ray, Shoulder MR is now considered the standard among the imaging methods to diagnose shoulder disorders, as it allows for optimal depiction of pathology and diagnosis in all major imaging planes. At the same time the method gives the arthroscopist an excellent roadmap for his intervention. All in all, the treatment outcome of shoulder trauma has been improved by shoulder MR in conjunction with modern surgical and arthroscopic therapies.Key words: shoulder joint anatomy; diagnosis of shoulder joint disease; shoulder arthro-MR method; imaging of shoul-der joint disease; imaging shoulder joint trauma
INTRODUCTION
The search for the cause of shoulder pain by imaging methods is usually initiated by conventional radiogra-phy. Radiography allows recognition of fractures, dislo-cation and degenerative joint disorders involving both the acromioclavicular and the glenohumeral joints. Also, soft tissue calcifications, result of tendon degeneration and possible cause for chronic pain are mostly well depicted in shoulder x-ray series, particularly if joints are exam-ined in internal and external rotation and abduction. The Y-projection allows better assessment of the subacromial /subcoracoid spaces and is a logical second plane supple-menting the traditional ap views [1]. Conventional shoul-der joint arthrography improves the diagnosis [2, 3] as it is able to demonstrate contrast media extravasation into the subacromial/subdeltoid bursa, which is indicative of a tear of the rotator cuff. Ultrasound studies add to the diagnostic accuracy and supplement the diagnostic arma-mentarium of the radiologist [4-8]. With ultrasound it is possible to directly demonstrate the substance of the rota-tor cuff and give direct evidence of joint and bursal effu-sions, as well as calcifications and larger tears. Still, only with a good understanding of the shoulder joint anatomy and pathology proper diagnostic results can be obtained. With computed tomography (CT) further advances in the diagnosis are possible [9-15]. Yet the diagnostic detail of the major structures at risk in the shoulder joint, the rota-tor cuff and the glenoid labrum, are less easily assessed properly in plain CT and mostly contrast enhanced CT studies are performed.
While excellent summaries on the topic of imaging of the shoulder are available [16-18], this paper will focus on the personal experience of the author with magnetic
resonance imaging (MRI) including intraarticular injec-tion of Contrast Media (Arthro-MR) of the shoulder joint. In a private group practice with 9 radiologists excellent results with this method have been attained over many years, also reflected by the steady referral practice and fre-quency. While we believe in our diagnostic accuracy, the large number of patients sent to our institute certainly is also due to increasingly sophisticated arthroscopic tech-niques. This has resulted in greatly improved therapeutic results and an overall better outcome in many patients. Both a statistical review of the spectrum of pathology found in 100 consecutive patients and a rough statistics of the therapeutic outcome in this group, as well as a pic-torial review of typical shoulder pathologies as seen on Arthro MR will be presented.
ANATOMY
Space does not allow a detailed description and illus-tration of the complex anatomy and study of the appropri-ate literature is suggested. In principle the glenohumeral joint is composed of the glenoid of the scapula and the humerus, with the contacting surfaced of these two bones being very small. This explains on one hand the extreme mobility of the shoulder joint, yet also the relative ease of sustaining joint luxation. It is the rotator cuff and the associated muscles which give this joint stability, while still ensuring a large motion range. The cuff is composed anteriorly by the subscapularis tendon and muscle, supe-riorly by the supraspinatus tendon and muscle and pos-teriorly by the infraspinatus tendon and muscle. These tendons in association with ligamentous reinforcements of the joint capsule by the superior, middle and inferior
REVIEW ARTICLES
BIBLID: 0370-8179, 136(2008) 1-2, p. 50-61
51
SRPSKI ARHIV ZA CELOKUPNO LEKARSTVO
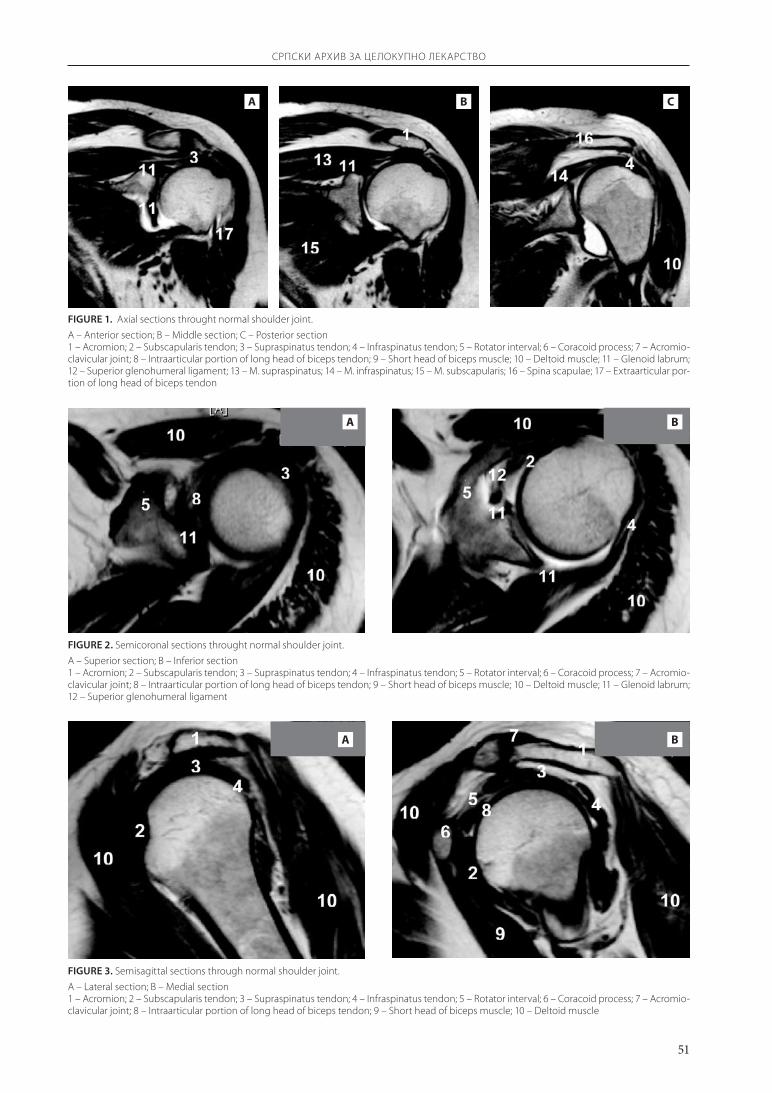
FIGuRE 1. Axial sections throught normal shoulder joint.
A – Anterior section; B – Middle section; C – Posterior section1 – Acromion; 2 – Subscapularis tendon; 3 – Supraspinatus tendon; 4 – Infraspinatus tendon; 5 – Rotator interval; 6 – Coracoid process; 7 – Acromio-clavicular joint; 8 – Intraarticular portion of long head of biceps tendon; 9 – Short head of biceps muscle; 10 – Deltoid muscle; 11 – Glenoid labrum; 12 – Superior glenohumeral ligament; 13 – M. supraspinatus; 14 – M. infraspinatus; 15 – M. subscapularis; 16 – Spina scapulae; 17 – Extraarticular por-tion of long head of biceps tendon
A B C
FIGuRE 2. Semicoronal sections throught normal shoulder joint.
A – Superior section; B – Inferior section1 – Acromion; 2 – Subscapularis tendon; 3 – Supraspinatus tendon; 4 – Infraspinatus tendon; 5 – Rotator interval; 6 – Coracoid process; 7 – Acromio-clavicular joint; 8 – Intraarticular portion of long head of biceps tendon; 9 – Short head of biceps muscle; 10 – Deltoid muscle; 11 – Glenoid labrum; 12 – Superior glenohumeral ligament
A B
FIGuRE 3. Semisagittal sections through normal shoulder joint.
A – Lateral section; B – Medial section1 – Acromion; 2 – Subscapularis tendon; 3 – Supraspinatus tendon; 4 – Infraspinatus tendon; 5 – Rotator interval; 6 – Coracoid process; 7 – Acromio-clavicular joint; 8 – Intraarticular portion of long head of biceps tendon; 9 – Short head of biceps muscle; 10 – Deltoid muscle
A B
52
SRPSKI ARHIV ZA CELOKUPNO LEKARSTVO
gleno-humeral ligaments, the glenoid labrum and the biceps tendon are the essential soft tissue structures which assure normal function of the joint. While fractures of the glenoid and humerus are rarely seen in private prac-tice, damage to anyone of the mentioned soft tissue struc-tures is frequent and is the cause of the bulk of referrals to imaging institutions. Figures 1-3 of specific sections of the joint in the axial, semicoronal and semisagittal planes give some information on the location of relevant ana-tomical structures.
METHODS (TECHNIQUE OF SHOULDER ARTHRO-MR)
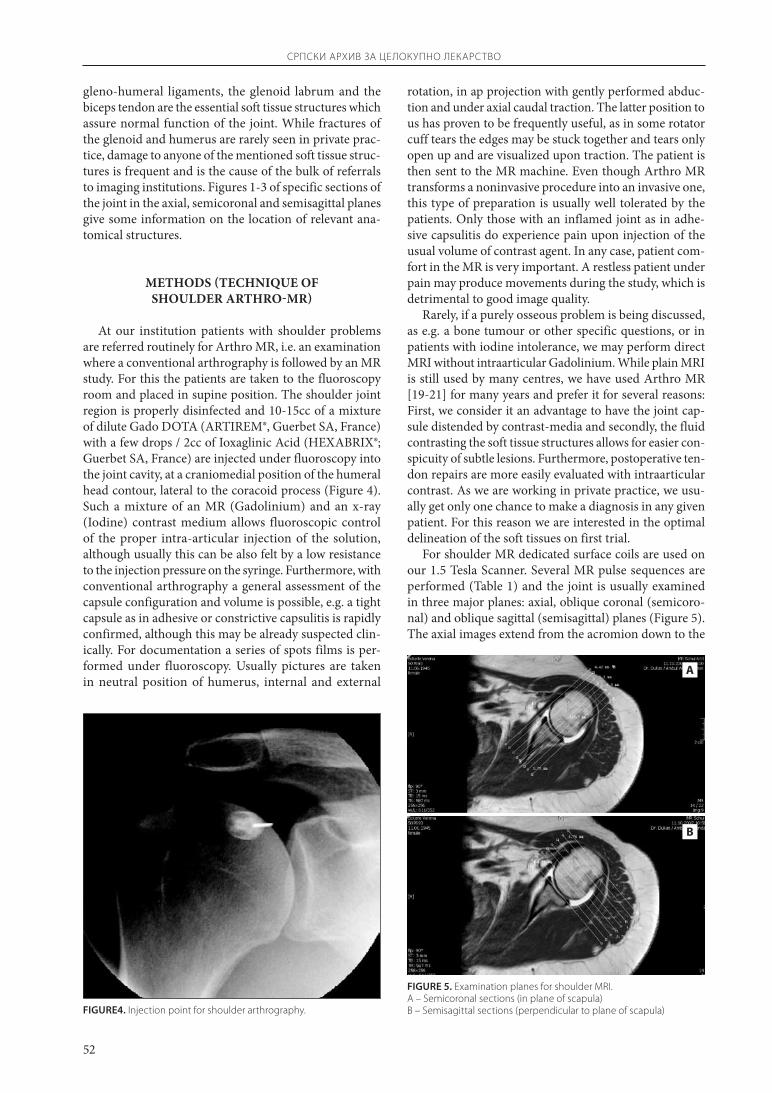
At our institution patients with shoulder problems are referred routinely for Arthro MR, i.e. an examination where a conventional arthrography is followed by an MR study. For this the patients are taken to the fluoroscopy room and placed in supine position. The shoulder joint region is properly disinfected and 10-15cc of a mixture of dilute Gado DOTA (ARTIREM®, Guerbet SA, France) with a few drops / 2cc of Ioxaglinic Acid (HEXABRIX®; Guerbet SA, France) are injected under fluoroscopy into the joint cavity, at a craniomedial position of the humeral head contour, lateral to the coracoid process (Figure 4). Such a mixture of an MR (Gadolinium) and an x-ray (Iodine) contrast medium allows fluoroscopic control of the proper intra-articular injection of the solution, although usually this can be also felt by a low resistance to the injection pressure on the syringe. Furthermore, with conventional arthrography a general assessment of the capsule configuration and volume is possible, e.g. a tight capsule as in adhesive or constrictive capsulitis is rapidly confirmed, although this may be already suspected clin-ically. For documentation a series of spots films is per-formed under fluoroscopy. Usually pictures are taken in neutral position of humerus, internal and external
FIGuRE4. Injection point for shoulder arthrography.
rotation, in ap projection with gently performed abduc-tion and under axial caudal traction. The latter position to us has proven to be frequently useful, as in some rotator cuff tears the edges may be stuck together and tears only open up and are visualized upon traction. The patient is then sent to the MR machine. Even though Arthro MR transforms a noninvasive procedure into an invasive one, this type of preparation is usually well tolerated by the patients. Only those with an inflamed joint as in adhe-sive capsulitis do experience pain upon injection of the usual volume of contrast agent. In any case, patient com-fort in the MR is very important. A restless patient under pain may produce movements during the study, which is detrimental to good image quality.
Rarely, if a purely osseous problem is being discussed, as e.g. a bone tumour or other specific questions, or in patients with iodine intolerance, we may perform direct MRI without intraarticular Gadolinium. While plain MRI is still used by many centres, we have used Arthro MR [19-21] for many years and prefer it for several reasons: First, we consider it an advantage to have the joint cap-sule distended by contrast-media and secondly, the fluid contrasting the soft tissue structures allows for easier con-spicuity of subtle lesions. Furthermore, postoperative ten-don repairs are more easily evaluated with intraarticular contrast. As we are working in private practice, we usu-ally get only one chance to make a diagnosis in any given patient. For this reason we are interested in the optimal delineation of the soft tissues on first trial.
For shoulder MR dedicated surface coils are used on our 1.5 Tesla Scanner. Several MR pulse sequences are performed (Table 1) and the joint is usually examined in three major planes: axial, oblique coronal (semicoro-nal) and oblique sagittal (semisagittal) planes (Figure 5). The axial images extend from the acromion down to the
FIGuRE 5. Examination planes for shoulder MRI. A – Semicoronal sections (in plane of scapula)B – Semisagittal sections (perpendicular to plane of scapula)
A
B
53
SRPSKI ARHIV ZA CELOKUPNO LEKARSTVO
inferior glenoid rim. Semicoronal planes are used because the scapula and glenohumeral joint are oriented at an angle of approximately 45° degrees in relation to the chest. Therefore straight sagittal and coronal imaging would cut the relevant soft tissue structures obliquely. These semi-coronal images are oriented parallel to the scapula and include the infraspinatus muscle posteriorly and the sub-scapularis muscle anteriorly. Finally semisagittal images in a perpendicular plane to the semicoronals range from the supraspinatus groove medially to the lateral aspect of the greater tuberosity. This protocol for shoulder MR studies is used routinely in most institutions. It allows for evalu-ation of all major soft tissue structures of the joint and a detailed MR analysis. The following pulse sequences have been found to be most revealing for depicting the anat-omy in 3 planes and are performed by our group on our 1.5T scanner (Table 1).
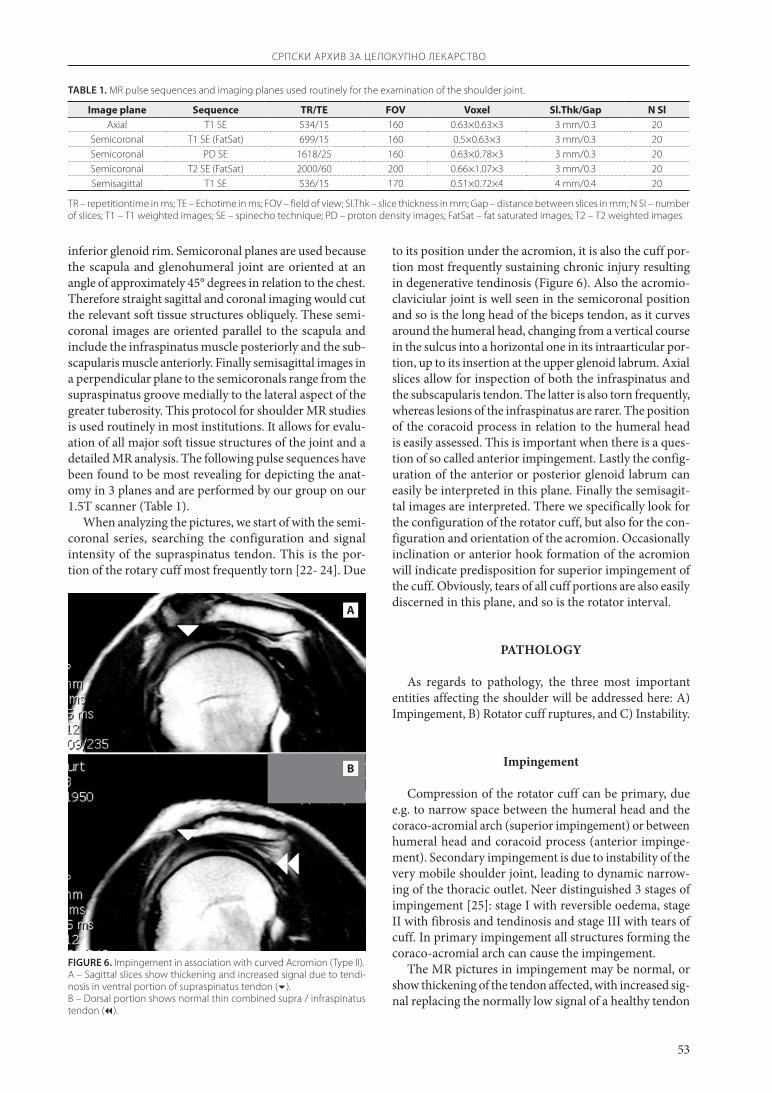
When analyzing the pictures, we start of with the semi-coronal series, searching the configuration and signal intensity of the supraspinatus tendon. This is the por-tion of the rotary cuff most frequently torn [22- 24]. Due
to its position under the acromion, it is also the cuff por-tion most frequently sustaining chronic injury resulting in degenerative tendinosis (Figure 6). Also the acromio-claviciular joint is well seen in the semicoronal position and so is the long head of the biceps tendon, as it curves around the humeral head, changing from a vertical course in the sulcus into a horizontal one in its intraarticular por-tion, up to its insertion at the upper glenoid labrum. Axial slices allow for inspection of both the infraspinatus and the subscapularis tendon. The latter is also torn frequently, whereas lesions of the infraspinatus are rarer. The position of the coracoid process in relation to the humeral head is easily assessed. This is important when there is a ques-tion of so called anterior impingement. Lastly the config-uration of the anterior or posterior glenoid labrum can easily be interpreted in this plane. Finally the semisagit-tal images are interpreted. There we specifically look for the configuration of the rotator cuff, but also for the con-figuration and orientation of the acromion. Occasionally inclination or anterior hook formation of the acromion will indicate predisposition for superior impingement of the cuff. Obviously, tears of all cuff portions are also easily discerned in this plane, and so is the rotator interval.
PATHOLOGY
As regards to pathology, the three most important entities affecting the shoulder will be addressed here: A) Impingement, B) Rotator cuff ruptures, and C) Instability.
Impingement
Compression of the rotator cuff can be primary, due e.g. to narrow space between the humeral head and the coraco-acromial arch (superior impingement) or between humeral head and coracoid process (anterior impinge-ment). Secondary impingement is due to instability of the very mobile shoulder joint, leading to dynamic narrow-ing of the thoracic outlet. Neer distinguished 3 stages of impingement [25]: stage I with reversible oedema, stage II with fibrosis and tendinosis and stage III with tears of cuff. In primary impingement all structures forming the coraco-acromial arch can cause the impingement.
The MR pictures in impingement may be normal, or show thickening of the tendon affected, with increased sig-nal replacing the normally low signal of a healthy tendon
TABLE 1. MR pulse sequences and imaging planes used routinely for the examination of the shoulder joint.
Image plane Sequence TR/TE FOV Voxel Sl.Thk/Gap N SlAxial T1 SE 534/15 160 0.63×0.63×3 3 mm/0.3 20
Semicoronal T1 SE (FatSat) 699/15 160 0.5×0.63×3 3 mm/0.3 20Semicoronal PD SE 1618/25 160 0.63×0.78×3 3 mm/0.3 20Semicoronal T2 SE (FatSat) 2000/60 200 0.66×1.07×3 3 mm/0.3 20Semisagittal T1 SE 536/15 170 0.51×0.72×4 4 mm/0.4 20
TR – repetitiontime in ms; TE – Echotime in ms; FOV – field of view; Sl.Thk – slice thickness in mm; Gap – distance between slices in mm; N Sl – number of slices; T1 – T1 weighted images; SE – spinecho technique; PD – proton density images; FatSat – fat saturated images; T2 – T2 weighted images
FIGuRE 6. Impingement in association with curved Acromion (Type II).A – Sagittal slices show thickening and increased signal due to tendi-nosis in ventral portion of supraspinatus tendon ().B – Dorsal portion shows normal thin combined supra / infraspinatus tendon ().
A
B
54
SRPSKI ARHIV ZA CELOKUPNO LEKARSTVO
(Figure 6). Most frequently osteophytes arising from the acromion or thickening of coracoacromial ligament cause supraspinatus compression i.e. impingement. There are three different configurations of acromia [26, 27] and type II and III may predispose to superior impingement. Also, os acromiale (Figure 7) or hypertrophy of AC joint osteo-phytes can cause impingement. Subcoracoid impingement occurs after fractures of coracoid or lesser tubercle. As mentioned, secondary extrinsic impingement occurs in cases of instability [28]. These patients are frequently ath-letes and their repetitive overhand activities as throwing may lead to posterosuperior glenoid impingement [29] and degeneration, as well as tearing of the articular fibres at the junction between the infraspinatus and supraspi-natus tendons. The damage occurs during abduction and external rotation and is often associated with posterosu-perior glenoid labral tears.
Rotator cuff tears
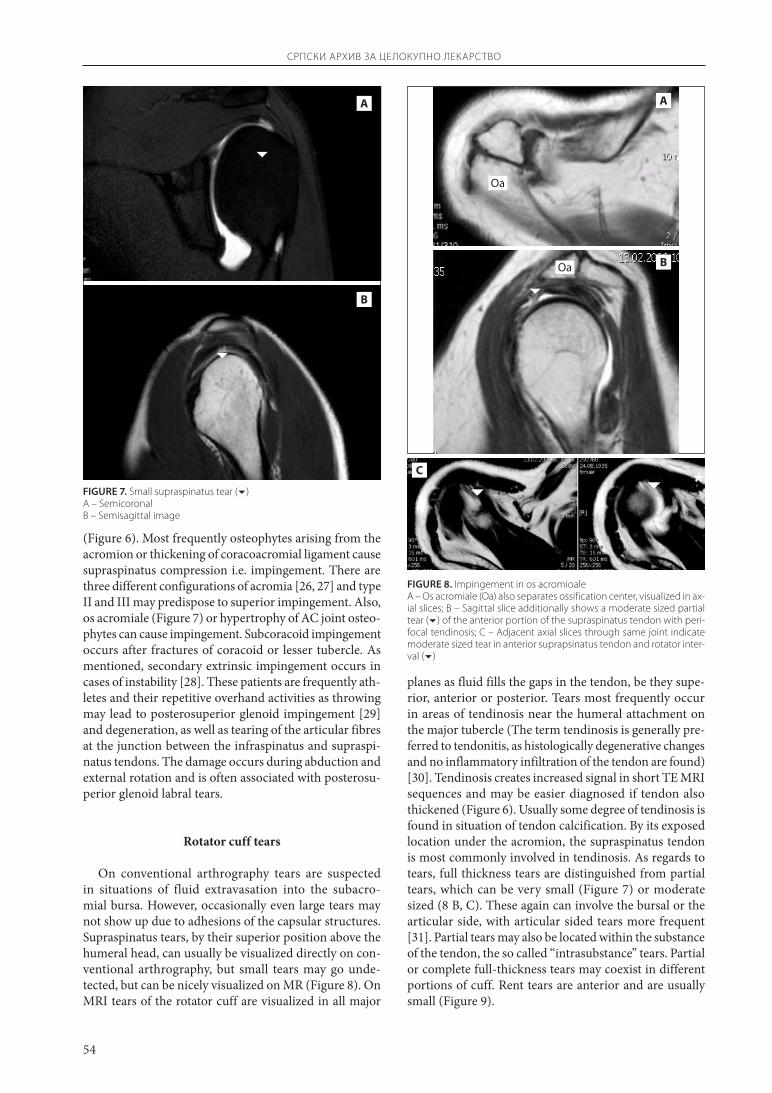
On conventional arthrography tears are suspected in situations of fluid extravasation into the subacro-mial bursa. However, occasionally even large tears may not show up due to adhesions of the capsular structures. Supraspinatus tears, by their superior position above the humeral head, can usually be visualized directly on con-ventional arthrography, but small tears may go unde-tected, but can be nicely visualized on MR (Figure 8). On MRI tears of the rotator cuff are visualized in all major
planes as fluid fills the gaps in the tendon, be they supe-rior, anterior or posterior. Tears most frequently occur in areas of tendinosis near the humeral attachment on the major tubercle (The term tendinosis is generally pre-ferred to tendonitis, as histologically degenerative changes and no inflammatory infiltration of the tendon are found) [30]. Tendinosis creates increased signal in short TE MRI sequences and may be easier diagnosed if tendon also thickened (Figure 6). Usually some degree of tendinosis is found in situation of tendon calcification. By its exposed location under the acromion, the supraspinatus tendon is most commonly involved in tendinosis. As regards to tears, full thickness tears are distinguished from partial tears, which can be very small (Figure 7) or moderate sized (8 B, C). These again can involve the bursal or the articular side, with articular sided tears more frequent [31]. Partial tears may also be located within the substance of the tendon, the so called “intrasubstance” tears. Partial or complete full-thickness tears may coexist in different portions of cuff. Rent tears are anterior and are usually small (Figure 9).
A
B
FIGuRE 7. Small supraspinatus tear () A – SemicoronalB – Semisagittal image
FIGuRE 8. Impingement in os acromioale A – Os acromiale (Oa) also separates ossification center, visualized in ax-ial slices; B – Sagittal slice additionally shows a moderate sized partial tear () of the anterior portion of the supraspinatus tendon with peri-focal tendinosis; C – Adjacent axial slices through same joint indicate moderate sized tear in anterior suprapsinatus tendon and rotator inter-val ()
Oa
Oa
A
B
C
55
SRPSKI ARHIV ZA CELOKUPNO LEKARSTVO
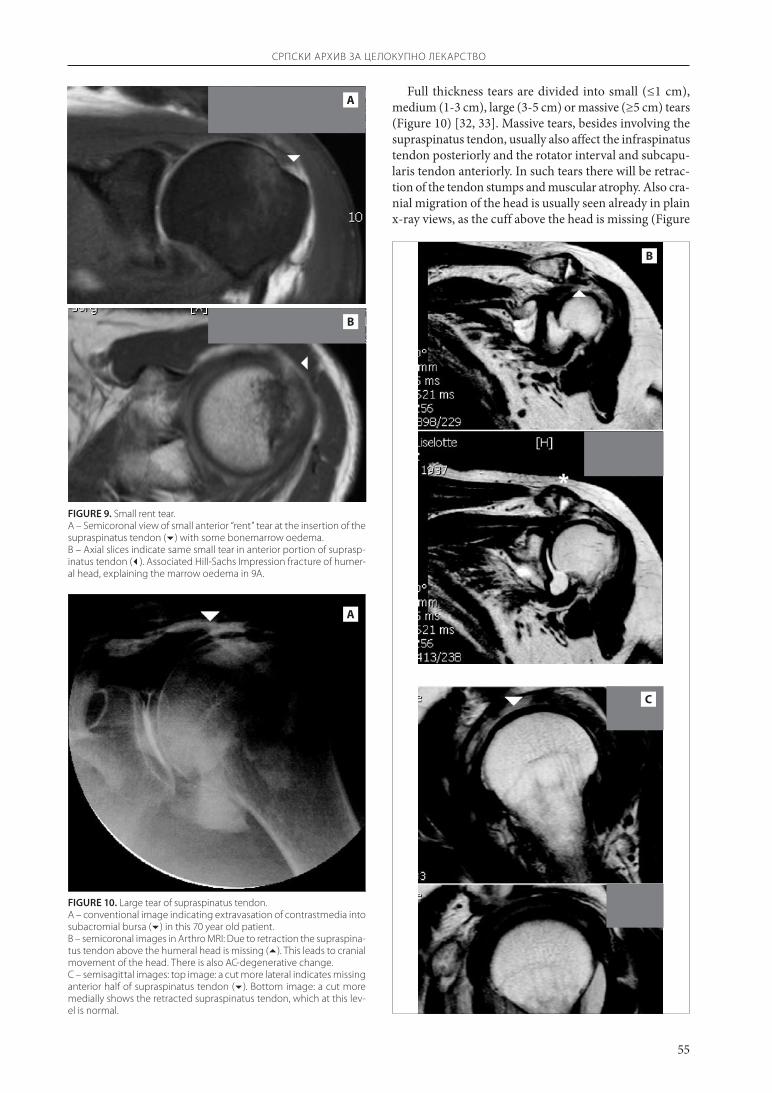
FIGuRE 10. Large tear of supraspinatus tendon.A – conventional image indicating extravasation of contrastmedia into subacromial bursa () in this 70 year old patient.B – semicoronal images in Arthro MRI: Due to retraction the supraspina-tus tendon above the humeral head is missing (). This leads to cranial movement of the head. There is also AC-degenerative change.C – semisagittal images: top image: a cut more lateral indicates missing anterior half of supraspinatus tendon (). Bottom image: a cut more medially shows the retracted supraspinatus tendon, which at this lev-el is normal.
FIGuRE 9. Small rent tear.A – Semicoronal view of small anterior “rent” tear at the insertion of the supraspinatus tendon () with some bonemarrow oedema.B – Axial slices indicate same small tear in anterior portion of suprasp-inatus tendon (). Associated Hill-Sachs Impression fracture of humer-al head, explaining the marrow oedema in 9A.
A
B
A
B
C
Full thickness tears are divided into small (≤1 cm), medium (1-3 cm), large (3-5 cm) or massive (≥5 cm) tears (Figure 10) [32, 33]. Massive tears, besides involving the supraspinatus tendon, usually also affect the infraspinatus tendon posteriorly and the rotator interval and subcapu-laris tendon anteriorly. In such tears there will be retrac-tion of the tendon stumps and muscular atrophy. Also cra-nial migration of the head is usually seen already in plain x-ray views, as the cuff above the head is missing (Figure
56
SRPSKI ARHIV ZA CELOKUPNO LEKARSTVO
10). Partial tears are graded into Grade I if less than one forth of the tendon or <3 mm, Grade II if less than one half (3-6 mm) and Grade III if more than one half of the tendon (>6 mm) is involved [31]. Not only the size of the tears, but also the degree of muscular atrophy (Figure 11) should be reported, as the chance for successful therapy i.e. re-anastomosis of torn tendons and ultimately good function are limited if there is significant atrophy and tendon retraction. Biceps pathology is frequently associ-ated with chronic tears of the supraspinatus tendon. All stages from tendinosis to full ruptures of the intraartic-ular portion of the bicepstendon are observed. In sub-scapularis tendon ruptures, the biceps tendon may sub-luxate medially into the body of the subscapularis ten-don or even completely luxate into the medial joint cav-ity (Figure 12) [34-36]. As the biceps tendon runs through the so called rotator interval, the term “intervallesion” has been coined and refers specifically to lesions of that ante-rior portion of the rotator cuff that includes the rotator interval, which itself is bare of tendons (Figures 3, 8B and C). More recently the value of some fine ligaments run-ning through the capsule in the interval have been recog-nized as stabilizing structures of the biceps tendon, which in the highly mobile joint must be dynamically stabilized as it dives from the joint cavity into the sulcus. Lesions of the rotator interval therefore are frequently associated with tears of the coraco-humeral and superior gleno-humeral ligaments, the so called rotator interval pulley of the biceps tendon [37]
The subscapularis tendon may also show tendinosis if there is the so called anterior or subcoracoid impinge-ment [38-41].
Occult subperiosteal fractures, frequently affecting the major tuberculum associated with rotator cuff tears, are easily diagnosed in MRI due to the associated bone mar-row oedema (Figure 13).
Instability
The shoulder joint, although featuring an extreme range of motion, exceeding the one of all other joints, under most circumstances is stable, due to the tendon reinforced joint capsule, several glenohumeral ligaments, various muscles, the glenoid labrum and least of all the osseous glenoid. An instable shoulder joint can be habit-ual or occur after an acute trauma of the mentioned struc-tures as after a dislocation, which possibly may lead to chronic instability. Instability can be anterior, posterior or multidirectional [42]. All soft tissue structures can be involved and accordingly need to be checked with imag-ing, with MRI usually particularly helpful.
The relative limited coverage of glenoid fossa by humeral head poses a risk for instability by itself. If there is a particular shallow or dysplastic glenoid, as in gle-noid hypoplasia or glenoid rim deficiency [43] or ret-roversion [44], this may further predispose to instabil-ity. Instability occurs furthermore, if the glenoid labrum
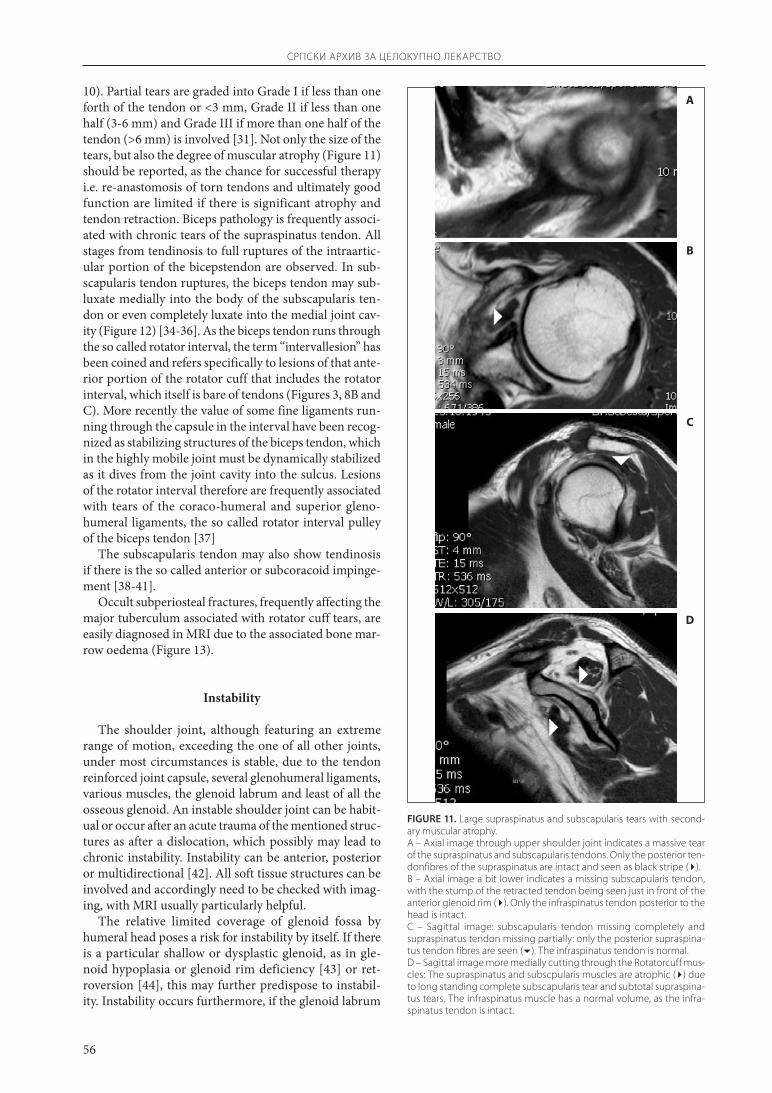
FIGuRE 11. Large supraspinatus and subscapularis tears with second-ary muscular atrophy.A – Axial image through upper shoulder joint indicates a massive tear of the supraspinatus and subscapularis tendons. Only the posterior ten-donfibres of the supraspinatus are intact and seen as black stripe ().B – Axial image a bit lower indicates a missing subscapularis tendon, with the stump of the retracted tendon being seen just in front of the anterior glenoid rim (). Only the infraspinatus tendon posterior to the head is intact.C – Sagittal image: subscapularis tendon missing completely and supraspinatus tendon missing partially: only the posterior supraspina-tus tendon fibres are seen (). The infraspinatus tendon is normal.D – Sagittal image more medially cutting through the Rotatorcuff mus-cles: The supraspinatus and subscpularis muscles are atrophic () due to long standing complete subscapularis tear and subtotal supraspina-tus tears. The infraspinatus muscle has a normal volume, as the infra-spinatus tendon is intact.
A
B
C
D
57
SRPSKI ARHIV ZA CELOKUPNO LEKARSTVO
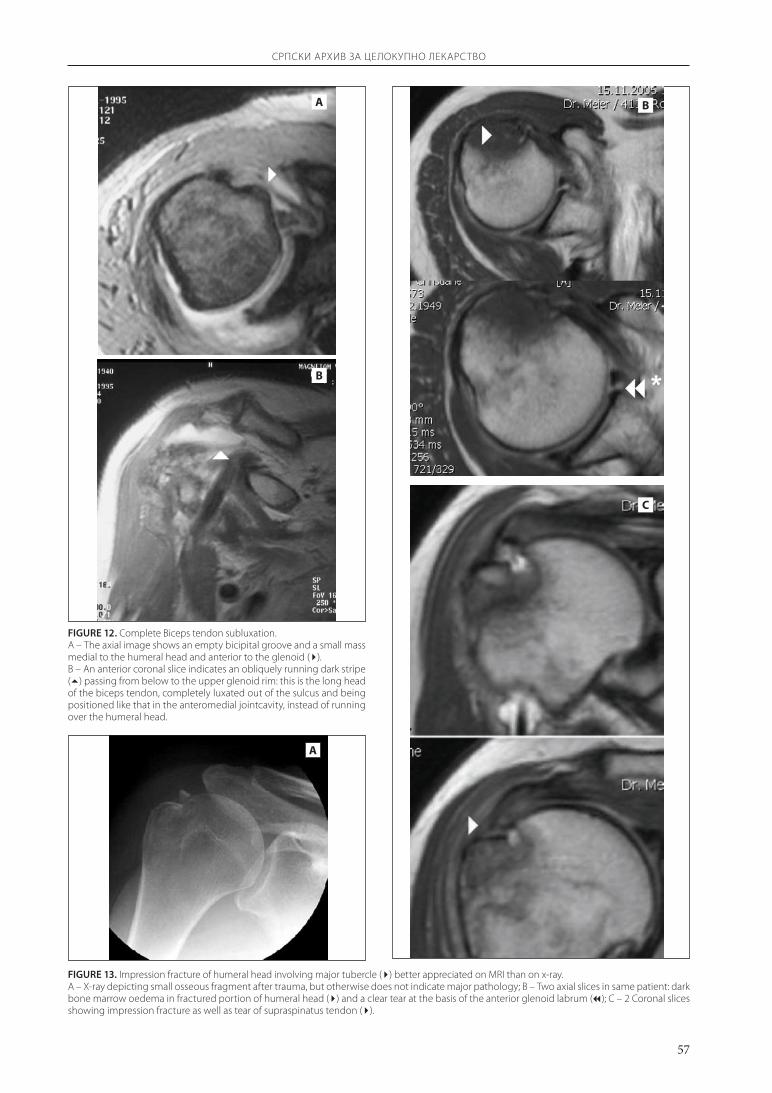
FIGuRE 12. Complete Biceps tendon subluxation.A – The axial image shows an empty bicipital groove and a small mass medial to the humeral head and anterior to the glenoid ().B – An anterior coronal slice indicates an obliquely running dark stripe () passing from below to the upper glenoid rim: this is the long head of the biceps tendon, completely luxated out of the sulcus and being positioned like that in the anteromedial jointcavity, instead of running over the humeral head.
A
B
FIGuRE 13. Impression fracture of humeral head involving major tubercle () better appreciated on MRI than on x-ray.A – X-ray depicting small osseous fragment after trauma, but otherwise does not indicate major pathology; B – Two axial slices in same patient: dark bone marrow oedema in fractured portion of humeral head () and a clear tear at the basis of the anterior glenoid labrum (); C – 2 Coronal slices showing impression fracture as well as tear of supraspinatus tendon ().
A
C
B
58
SRPSKI ARHIV ZA CELOKUPNO LEKARSTVO
and glenohumeral ligaments, especially the inferior gleno-humeral ligament, are injured [45-49].
As regards to imaging, in instability the plain x-rays have a role to play: usually a 5 view routine with ap pro-jections in internal (IR) and external rotation (ER), the Y-projection and the axillary and abduction projections are performed. With these x-rays the typical Hill-Sachs and Bankart lesions can be demonstrated. As, however, soft tissues are frequently also injured, there is nowa-days a role for cross-sectional imaging and for this we also use mostly MR, which is very accurate for diagnosis and as a roadmap (guide) for the arthroscopist. Usually patients do not reach us in the acute stage and therefore optimally need contrast media application. Besides the mentioned osseous fractures of the anterior glenoid rim (Bankart lesion) after ant. dislocation, the typical Hill-Sachs impression fracture [50] are easily observed in all, but best in the axial plane. After dislocations, frequently there is capsular stripping of the glenoid neck and tears of the anterior inferior glenohumeral ligament and ante-rior labrum. Posterior dislocations are rare and if present thez are frequently associated with multidirectional insta-bility. Beyond the obvious rotator cuff and labral tears, diagnosis of soft tissue pathology has become extremely refined. A spectrum of lesions are differentiated and described by at times incomprehensible abbreviations, depending on the injured structure. This includes the so called SLAP (Superior Labrum Anterior-Posterior) lesion of the biceps anchor at the superior labrum (Figure 14), the ALPSA-Lesion (Anterior Labroligamentous Periosteal Sleave Avulsion), the GARD-Lesion (Glenoid Articular Disruption), the HAGL-Lesion (Humeral Avulsion of the Glenohumeral Ligament) and the GLAD-Lesion (Glenolabral Articular Disruption Lesion) [51-53]. As regards to therapy TUBS (Trauma, Unidirectional, including Bankart defects) lesions are clinically differ-entiated from AMBRI (Atraumatic, Multidirectional, Bilateral, Rehabilitation) lesions. The former are surgi-cal and the latter are usually treated by rehabilitation. In
instability, the Arthro MRI offers again the advantage of a capsular distension with increased conspicuity of soft tissues. [47, 54-58]. Also to be mentioned is the use of MR Arthrography in the postoperative situation [59]. However, partial postoperative tears are less easily con-firmed than full thickness tears by MR.
RETROSPECTIVE REVIEW OF OWN CASE MATERIAL
In a retrospective review, 100 consecutive patients (58 men, 42 women, average age 54.1 years) referred to our institution for diagnostic workup for shoulder complaints in the months of November and December 2006 were analysed for the spectrum of diagnosed pathology. One or more diagnostic observations were made in each patient. All diagnoses are summarized in Table 2. The findings can grossly be grouped in lesions of the rotator cuff (with its three portions the supraspinatus, the subscapularis and the infraspinatus tendons plus the rotator-interval), lesions of the biceps tendon, lesions of the glenoid labrum and degenerative changes of the gleno-humeral and acro-mio-clavicular joint. Out of the 100 patients only 4 were without visible pathology, whereas in the remainder usu-ally degenerative or posttraumatic combined lesions were diagnosed. Not unexpectedly soft tissue pathology was abundant, being present in 22-55 % of the cases, whereas occult fractures were seen in only 8%.
An analysis regarding further diagnostic workup, ther-apy and final outcome was made in the patients. Out of the 100 patients we were able to contact 71 by telephone: 39/71 (55%) apparently did not require any further diag-nostic workup or surgical therapy, 11 (15%) were exam-ined and treated arthroscopically and 21 (30%) needed open surgery. Some 7 months after their MR studies, out of the 71 patients 43 (61%) felt better or had no more symptoms, whereas 22 (31%) were unchanged regarding their symptoms and 6 (8%) felt worse.
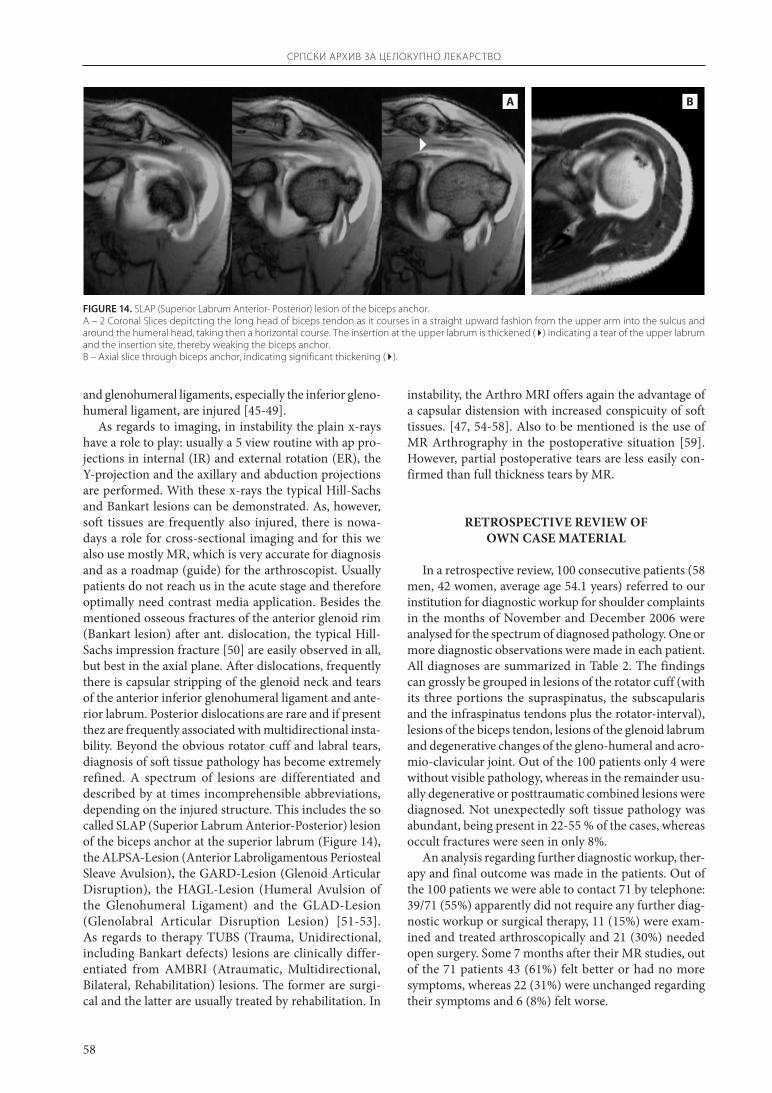
FIGuRE 14. SLAP (Superior Labrum Anterior- Posterior) lesion of the biceps anchor.A – 2 Coronal Slices depitcting the long head of biceps tendon as it courses in a straight upward fashion from the upper arm into the sulcus and around the humeral head, taking then a horizontal course. The insertion at the upper labrum is thickened () indicating a tear of the upper labrum and the insertion site, thereby weaking the biceps anchor.B – Axial slice through biceps anchor, indicating significant thickening ().
A B

59
SRPSKI ARHIV ZA CELOKUPNO LEKARSTVO
DISCUSSION
In medicine elaborate diagnosis obviously makes sense if there are means for adequate therapy and there is a good chance for better outcomes. In the field of muscu-loskeletal disease, arthroscopy nowadays fulfils these cri-teria and in many cases it replaces more invasive surgical therapies. It is in collaboration with trained arthroscopists, where a high resolution Arthro MR and diagnosis of early and subtle pathology allows for an optimal preoperative roadmap and gives best surgical results. As far as diagnos-tic interpretation is concerned, the potential and the lim-its of Arthro MR have to be realized both by the radiol-ogists and the referring surgeons. Detailed knowledge of the anatomical structures and their pathology is essen-tial for rational work with Arthro MR, just as an immac-ulate technique both for conventional arthrography and the subsequent MR study. Judging from the large num-ber of patients referred to our centre, we confirm what is generally known: soft tissue lesions after shoulder trauma are much more frequent than generally believed. And it is only an advanced diagnostic tool as Arthro MR which is capable to demonstrate the full spectrum of pathology.
CONCLUSION
We present our experience with shoulder MRI in a small group of patients. This review is supplemented by a pictorial review of typical pathologies, which for space
TABLE 2. Spectrum of pathology found in 100 consecutive patients examined with shoulder arthro MR.
Parameter Number of patients
SexMale 58Female 42
No pathology 4
Pathology
Suprasp. rupture / Partial rupture 54Suprasp. tendinosis 55Suprasp. atrophy 16Intervall lesion 12Subscap. rupture / Partial rupture 11Subscap. tendinosis 12Subscap. atrophy 4Infrasp. rupture / Partial rupture 12Infrasp. tendinosis 7Infrasp. atrophy 3Biceps rupture / Tendinosis 24SLAP lesion 8Labrum rupture 22Omarthrosis 8AC arthrosis 40Bonebruise / Fracture 8Superior impingement 12Anterior impingement 1Subacromial bursitis 6Adhesive capsulitis 8Postoperative changes 5Neurinome 1
reasons obviously has to be limited. Shoulder MR is now considered the standard among the imaging methods for optimal depiction of pathology, at the same time giving the arthroscopist an excellent road map for his interven-tion. While Arthro CT and ultrasound certainly also have their merits as examination methods, they also have their limitations. Ultrasound needs a very experienced sonog-rapher and CT needs reformatting of the axial pictures and is more limited in depicting subtle labral and tendon pathology and both sonography and CT are being sur-passed by MRI.
We hope to shall raise interest of Serbian colleagues for the method of Arthro MRI and are confident that in future more patients will benefit from this small invasive imaging method to study the shoulder joint.
REFERENCES
1. Neer CS, Poppen NK. Supraspinatus outlet. Orthop Trans 1987; 11:234.
2. Resnick, D. Shoulder arthrography. Radiol Clin North Am 1981; 19:243-53.
3. Mink JH, Harris E, Rappaport M. Rotator cuff tears: evaluation using double-contrast shoulder arthrography. Radiology 1985; 157:621-3.
4. Brennecke SL, Morgan CJ. Evaluation of ultrasonography as a diag-nostic technique in the assessment of rotator cuff tears. Am J Sports Med 1992; 20:287-9.
5. Crass JR, Craig EV, Feinberg SB. Ultrasonography of rotator cuff tears: a review of 500 diagnostic studies. JCU 1988; 16:313-27.
6. Hodler J, Fretz CJ, Terrier F, et al. Rotator cuff tears: correlation of sonographic and surgical findings. Radiology 1988; 169:791-4.
7. Mack LA, Nyberg DA, Matsen FR. Sonography of the postopera-tive shoulder. AJR 1988; 150:1089-93.
8. Middleton WD. Status of rotator cuff sonography. Radiology 1989; 173:307-9.
9. Deutsch AL, Resnick D, Mink JH. Computed and conventional arthrotomography of the glenohumeral joint: normal anatomy and clinical experience. Radiology 1984; 153:603-9.
10. Coumas JM, Waite RJ, Goss TP, et al. CT and MR evaluation of the labral capsular ligamentous complex of the shoulder. AJR 1992; 158:591-7.
11. Beltran J, Gray LA, Bools JC, et al. Rotator cuff lesions of the shoul-der evaluation by direct sagittal CT arthrography. Radiology 1986; 160:161-5.
12. McNiesh LM, Callaghan JJ. CT arthrography of the shoulder: vari-ations of the glenoid labrum. AJR 1987; 149:963-6.
13. Pennes DR. Shoulder joint: arthrographic CT appearance. Radiology 1990; 175:878-9.
14. Rafii M, Firooznia H, Bonamo JJ, et al. Athlete shoulder injuries: CT arthrographic findings. Radiology 1987; 162:559-64.
15. Wilson AJ, Totty WG, Murphy WA, et al. Shoulder joint: arthro-graphic CT and long-term follow-up, with surgical correlation. Radiology 1989; 173:329-33.
16. Stiles RG, Otte MT. Imaging the shoulder. Radiology 1993; 188:603-13.
17. Fritz RC. Magnetic Resonance Imaging of sports-related injuries to the shoulder: impingement and rotator cuff. Radiol Clin North Am 2002; 40(2):217-34.
18. Farber JS, Buckwalter KA. Sports-related injuries of the shoulder: instability. Radiol Clin North Am 2002; 40(2):235-49.
19. Flannigan B, Kursunoglu-Brahme S, Snyder S, et al. MR arthrogra-phy of the shoulder: comparison with conventional MR imaging. AJR 1990; 155:829-32.
20. Hodler J, Kursunoglu-Brahme S, Snyder SJ, et al. Rotator cuff dis-ease: assessment with MR arthrography versus standard MR imag-ing in 36 patients with arthroscopi confirmation. Radiology 1992; 182:431-6.
21. Pfirrmann CW, Zanetti M, Weishaupt D, et al. Subscapularis Tendon tears: detection and grading. At MR arthrography. Radiology 1999;

60
SRPSKI ARHIV ZA CELOKUPNO LEKARSTVO
213:709-14. 22. Quinn SF, Sheley RC, Demlow TA, et al. Rotator cuff tendon tears:
evaluation with fat-suppressed MR imaging with arthroscopic cor-relation in 100 patients. Radiology 1995; 195:497-501.
23. Rafii M, Firooznia H, Sherman O, et al. Rotator cuff lesions: signal patterns at MR imaging. Radiology 1990; 177:817-23.
24. Reinus WR, Shady KL, Mirowitz SA, et al. MR diagnosis of rotator cuff tears of the shoulder: Value of using T2-weighted fat-saturated images. Am J Roentgenol 1995; 164:1451-5.
25. Neer CS. Impingement lesions. Clin Orthop 1998; 173:70-7. 26. Morrison DS, Bigliani LU. The clinical significance of variations in
acromial morphology. Orthop Trans 1987; 11:234. 27. Morrison DS, Bigliani LU. Roentgenorgaphic analysis of acromial
morphology and its relationship to rotator cuff tears. Orthop Trans 1987; 11:439.
28. Jobe FW, Kvitne RS, Giangarra CE. Shoulder pain in the overhand or throwing athlete: the relationship of anterior instability and rota-tor cuff impingement. Orthop Rev 1989; 18:963-75.
29. Walch G, Boileau P, Noel E, et al. Impingement of the deep surface of the supraspinatus tendon on the postero-superior glenoid rim: an arthroscopic study. J Shoulder Elbow Surg 1992; 1:238-45.
30. Kannus P, Jozsa L. Histopathological changes preceding spontane-ous rupture of a tendon: a controlled study of 891 patients. J Bone Joint Surg Am 1991; 73:1507-25.
31. Gartsman GM, MilneJC. Articular surface partial- thickness rota-tor cuff tears. J Shoulder Elbow Surg 1995; 4:409-15.
32. Iannotti JP, Bernot MP, Kuhlman JR, et al. Postoperative assessment of shoulder function: a prospective study of full-thickness rotator cuff tears. J Shoulder Elbow Surg 1996; 5:449-57.
33. Post M, Silver R, Singh M. Rotator cuff tear: diagnosis and treat-ment. Clin Orthop 1983; 173:78-91.
34. Deutsch A, Alchek DW, Veltri DM, et al. Traumatic tears of the sub-scapularis tendon: clinical diagnosis, magnetic resonance imag-ing findings, and operative treatment. Am J Sports Med 1997; 25:13-22.
35. Gerber C, Hersche O, Farron A. Isolated rupture of the subscapu-laris tendon. J Bone Joint Surg Am 1996; 78:1015-23.
36. Patten RM. Tears of the anterior portion of the rotator cuff (the sub-scapularis tendon): MR imaging findings. Am J Roentgenol 1994; 162:351-4.
37. Weishaupt D, Zanetti M, Tanner A, et al. Lesions of the reflection pulley of the long biceps tendon: MR arthrographic finding. Invest Radio 1999: 34:463-9.
38. Dines D, Warren RF, Inglis AE, et al. The coracoid impingement syn-drome. J Bone Joint Surg Br 1990; 72:314-6.
39. Dumontier C, Saulet A, Lenoble E, et al. Antero-medial impinge-ment syndrome. J Shoulder Elbow Surg 1997; 6:198.
40. Gerber C, Terrier F, Ganz R. The role of the coracoid process in the chronic impingement syndrome. J Bone Joint Surg Br 1985; 67:703-8.
41. Patte D. The subcoracoid impingement. Clin Orthop 1990; 254: 55-9.
42. Wirth MA, Lyons FR, Rockwood Jr CA. Hypoplasie of the glenoid: a review of sixteen patients. J Bone Joint Surg 1993; 75A:1175-84.
43. Weishaupt D, Zanetti M, Nyffeler RW, et al. Posterior glenoid rim deficiency in recurrent (atraumatic) posterior shoulder instability. Skeletal Radiology 2000; 29(4):204-10.
44. Brewer BJ, Wubben RC, Carrera GF. Excessive retroversion of the glenoid cavity: a cause of non-traumatic posterior instability of the shoulder. J Bone Joint Surg 1986; 68A:724-31.
45. Ferrari DA. Capsular ligaments of the shoulder. Anatomical and functional study of the anterior capsule (case report). Am J Sport Med 1990; 18:20-4.
46. Bigliani LU, Pollock RG, Soslowsky LJ, et al. Tensile properties of the inferior glenohumeral ligament. J Ortho Res 1992; 10:187-97.
47. Sanders T, Morrison W, Miller M. Imaging techniques for the evaluation of glenohumeral instability. Am J Sports Med 2000; 28(3):414-34.
48. Schweitzer ME. MR arthrography of the labral- ligamentous com-plex of the shoulder. Radiology 1994; 190:641-3.
49. Turkel SJ, Panio MW, Marshall JL, et al. Stabilizing mechanism pre-venting anterior dislocation of the glenohumeral joint. J Bone Joint Surg 1998: 63A:1208-17.
50. Hill HA, Sachs MD. The grooved defect of the humeral head. A fre-quently unrecognized complication of dislocations of the shoulder joint. Radiology 1940; 35:690-700.
51. Neviaser TJ. The anterior labroligamentous periosteal sleeve avul-sion (ALPSA) lesion: a cause of anterior instability of the shoulder. Arthroscopy 1993; 9:17-22.
52. Chan KK, Skaff A, Roger E, et al. Glenoid articular rim disruption (GARD) and its relationship to ostechondritis dissecans: Routine radiography, standard arthrography, C arthrography and MR arthrography in eighteen patients. Radiology 1998; 209P:236.
53. Wolf EM, Cheng JC, Dickson K. Humeral avulsion of glenohumeral ligaments (HAGL) as a cause of anterior shoulder instability. Arthroscopy 1995; 11:600-7.
54. Palmer W, Caslowitz P. Anterior shoulder instability: diagnostic cri-teria determined from prospective analysis of 121 MR arthrograms. Musculoskeletal Radiology 1995; 197:819-25.
55. Shankman S, Bencardino J, Beltran J. Glenohumeral instability: eval-uation using MR arthrography of the shoulder. Skeletal Radiology 1999; 28(7):365-82.
56. Rafii M, Minkoff J. Advanced arthrography of the shoulder with CT and MR imaging. Interventional procedures in musculoskele-tal radiology. Radiol Clin North Am 1998; 36(4):609-33.
57. Palmer WE, Brown J, Rosenthal D. Labral-ligamentous complex of the shoulder: evaluation with MR arthrography. Muskuloskeletal Radiology 1994; 190(3):645-51.
58. Chandnani VP, Yeager T, DeBerardino, et al. Glenoid labral tears: prospective evaluation with MR imaging, MR arthrography and CT arthrography. Am Roentgen Ray Society 1993; 161(6):1229-35.
59. Duc SR, Mengiardi B, Pfirrmann CWA, et al. Diagnostic perfor-mance of MR arthrography after rotator cuff repair. AJR 2006; 186:237-41.

61
SRPSKI ARHIV ZA CELOKUPNO LEKARSTVO
KRATAK SADRŽAJUradujeopisanoautorovoličnoiskustvosprimenom
magnetnerezonancije(MR)ikontrastnogsredstva(Ar thro-MR)kodpregledaramenogzgloba (Sho ul der MR).Ovajmetodseupoređujesadrugimčešćeprimewivanimdijagnostičkimmetodima,kojitakođeimajunekeprednosti.DiskutujeseoindikacijamazaprimenumetodaSho ul der Ar-thro-MRidajudetaqanopisiobjašwewetehnike.Takođeserazmatrajunajvažnijepatološkepromeneramena,kaoštosurazličitiporemećajizgloba,rupturemišićainestabilnostizgloba.Izlažesecelokupnipregledpatološkihpromenautvrđenihkod100bolesnika,kaoiprimewenolečeweiishodlečewa.Dajeseslikovniprikaztipičnihpatološkihpromenautvrđenihprimenommagnetnerezonancije.Poredrendgenološkogpregleda,Sho ul der MRsedanassmatrastandardnomradiološkomtehnikomudijagnostikovawuporemećajaramenabudućidasewomeomogućujeoptimalniopispatološkihpromena,kaoipo
stavqawedijagnozenaosnovusnimakaramenaiznajvažnijihuglova.Istovremeno,ovajmetodpredstavqaartroskopistiodličanputokazprilikomsameintervencije.MožesezakqučitidajeSho ul der MR,uzsavremenohirurškoiartroskopskolečewe,znatnopoboqšaoishodlečewakodpovredaramena.
Kqučne reči:anatomijaramenogzgloba;dijagnozaoboqewaramenogzgloba;metodShoulder Arthro-MR;prikazoboqewaramenogzgloba;prikazpovrederamenogzgloba
Andreas NIDECKER IMAMED Radiologie Nordwest Unt. Rebgasse 18, CH 4058 Basel Switzerland Tel.: +41 61 686 42 42 E-mail: [email protected]
PATOLOGIJA RAMENOG ZGLOBA – BOQE DIJAGNOSTIKOVAWE POMOĆU MAGNETNE REZONANCIJE: SLIKOVNI PRIKAZ I PREGLED LITERATURE
Andreas NIDECKERIMAMED Radiologie Nordwest, Bazel,Švajcarska
*�Rukopis�je�dostavqen�Uredništvu�24.�9.�2007.�godine.
![SHOULDER JOINT PATHOLOGY – IMPROVED DIAGNOSIS BY … · the shoulder are available [16-18], this paper will focus on the personal experience of the author with magnetic resonance](https://img.dokumen.tips/doc/110x75/5f2d8ab5b7585b119423bab4/shoulder-joint-pathology-a-improved-diagnosis-by-the-shoulder-are-available-16-18.jpg)




























