Embed Size (px)
Citation preview
1565
Short Communications
Alcoholic Intracerebral HemorrhageLeon A. Weisberg, MD
Six alcoholic patients developed extensive cerebral hemispheric hemorrhages with bothintraventricular and subarachnoid blood. All patients had evidence of liver damage, low plateletcounts, and abnormal prothrombin and partial thromboplastin times. Four patients presentedwith seizures; in two of the four, these seizures were initially diagnosed as alcohol withdrawalseizures. Four patients were comatose with lateralizing neurologic deficit; two patients werecomatose without lateralizing neurologic deficit, suggesting a metabolic encephalopathy. In onepatient there was delayed neurologic deterioration. In all six patients, computed tomographyshowed large diffuse cerebral hemispheric hemorrhages, prominent intraventricular blood, andbreakthrough into the subarachnoid spaces, which was confirmed by necropsy findings. Therewas marked mass effect but minimal surrounding edema. All six patients died. In three, autopsyshowed no evidence of aneurysm, vascular malformation, neoplasm, or amyloid angiopathy andno arteriolar hypertensive changes. (Stroke 1988;19:1565-1569)
A lcohol has known acute and chronic cardio-Z A vascular effects'-4 that cause alcoholics to
A J L be at risk for stroke. Chronic alcoholicshave decreased concentrations of liver-producedcoagulation factors and platelet abnormalities thatpredispose them to hemorrhagic stroke. Chronicalcoholism may cause hypertension, and acute alco-holic episodes may precipitate an acute hyperten-sive state with return to normotension when thesubject stops drinking alcohol. Based on the poten-tial for hypertension and impaired coagulation, hem-orrhagic stroke develops with increased frequencyin alcoholics. I describe six patients with alcoholicnonhypertensive intracerebral hemorrhages (ICHs)that may have occurred as a consequence of thechronic and/or acute alcoholic state.
Case ReportsCase 1. A 52-year-old chronic alcoholic woman
developed headache and vomiting; she suddenlybecame unresponsive. Findings were stupor, hyper-ventilation, left hemiplegia, bilateral Babinski's signs,and a fixed dilated right pupil. Her hemoglobin was10 g/dl; stool guaiacs were positive. Platelet countwas 70,000/mm3. Her prothrombin time was 14.5(normal control 12) seconds and her partial throm-boplastin time was 38 (normal range 23-34) sec-onds. She had impaired liver function (SGOT 300
From the Department of Neurology and Psychiatry, TulaneMedical School, the Department of Neurology, Veterans Admin-istration Hospital, and the Department of Neurology, CharityHospital, New Orleans, Louisiana.
Address for correspondence: Leon A. Weisberg, MD, Depart-ment of Neurology and Psychiatry, 1430 Tulane Avenue, NewOrleans, LA 70112.
Received November 3, 1987; accepted July 6, 1988.
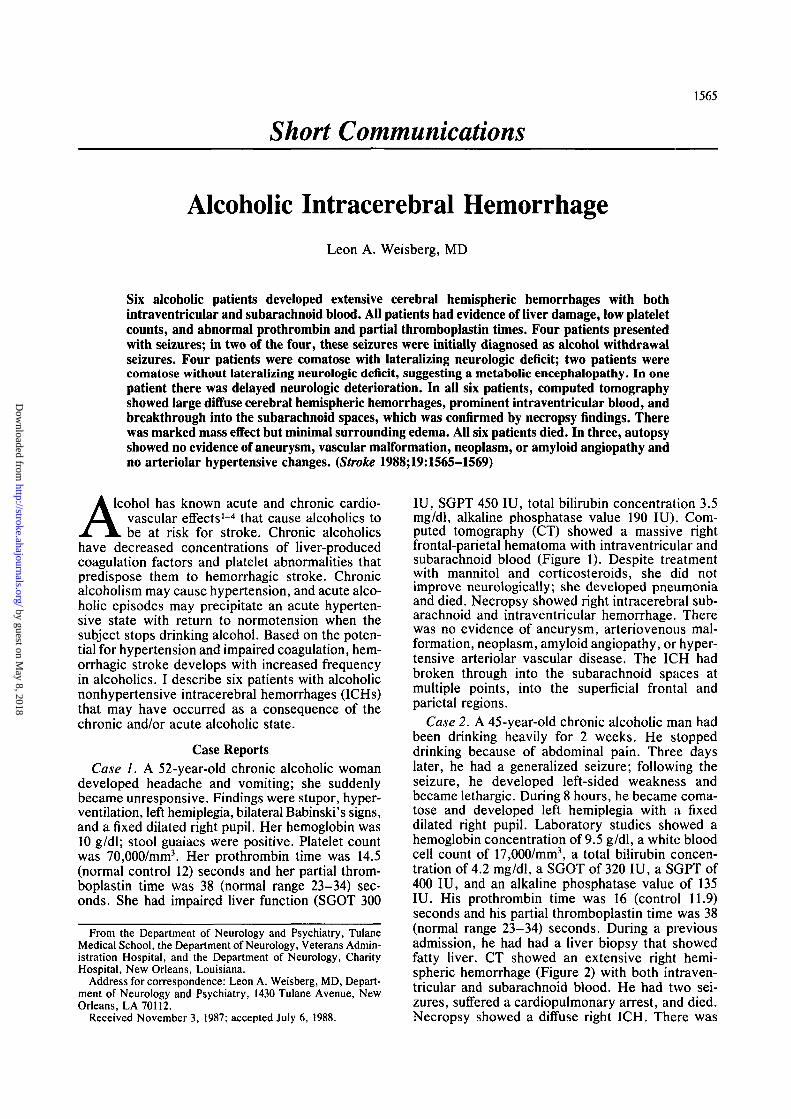
IU, SGPT 450 IU, total bilirubin concentration 3.5mg/dl, alkaline phosphatase value 190 IU). Com-puted tomography (CT) showed a massive rightfrontal-parietal hematoma with intraventricular andsubarachnoid blood (Figure 1). Despite treatmentwith mannitol and corticosteroids, she did notimprove neurologically; she developed pneumoniaand died. Necropsy showed right intracerebral sub-arachnoid and intraventricular hemorrhage. Therewas no evidence of aneurysm, arteriovenous mal-formation, neoplasm, amyloid angiopathy, or hyper-tensive arteriolar vascular disease. The ICH hadbroken through into the subarachnoid spaces atmultiple points, into the superficial frontal andparietal regions.
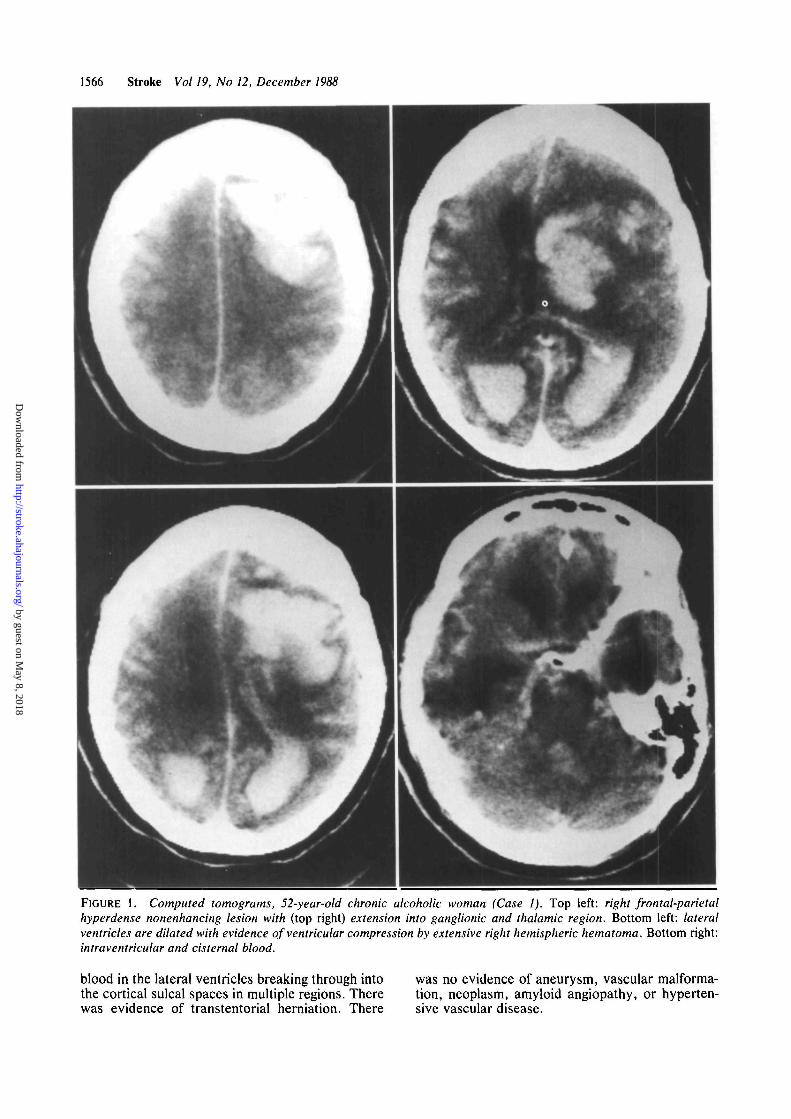
Case 2. A 45-year-old chronic alcoholic man hadbeen drinking heavily for 2 weeks. He stoppeddrinking because of abdominal pain. Three dayslater, he had a generalized seizure; following theseizure, he developed left-sided weakness andbecame lethargic. During 8 hours, he became coma-tose and developed left hemiplegia with a fixeddilated right pupil. Laboratory studies showed ahemoglobin concentration of 9.5 g/dl, a white bloodcell count of 17,000/mm3, a total bilirubin concen-tration of 4.2 mg/dl, a SGOT of 320 IU, a SGPT of400 IU, and an alkaline phosphatase value of 135IU. His prothrombin time was 16 (control 11.9)seconds and his partial thromboplastin time was 38(normal range 23-34) seconds. During a previousadmission, he had had a liver biopsy that showedfatty liver. CT showed an extensive right hemi-spheric hemorrhage (Figure 2) with both intraven-tricular and subarachnoid blood. He had two sei-zures, suffered a cardiopulmonary arrest, and died.Necropsy showed a diffuse right ICH. There was
by guest on May 8, 2018
http://stroke.ahajournals.org/D
ownloaded from
1566 Stroke Vol 19, No 12, December 1988
FIGURE 1. Computed tomograms, 52-year-old chronic alcoholic woman (Case 1). Top left: right frontal-parietalhyperdense nonenhancing lesion with (top right) extension into ganglionic and thalamic region. Bottom left: lateralventricles are dilated with evidence of ventricular compression by extensive right hemispheric hematoma. Bottom right:intraventricular and cisternal blood.
blood in the lateral ventricles breaking through into was no evidence of aneurysm, vascular malforma-the cortical sulcal spaces in multiple regions. There tion, neoplasm, amyloid angiopathy, or hyperten-was evidence of transtentorial herniation. There sive vascular disease.
by guest on May 8, 2018
http://stroke.ahajournals.org/D
ownloaded from
Weisberg Alcoholic Intracerebral Hemorrhage 1567
FIGURE 2. Computed tomograms, 45-year-old chronicalcoholic man (Case 2). Top left: heterogeneous righthemispheric hematoma. Bottom: blood is seen in basalcisternal and sulcal space. Top right: marked right hemi-spheric mass effect with intraventricular blood.
Summary of Clinical FindingsThe clinical and CT findings in these six patients
are summarized in Table 1. Five patients were intheir 40s. Five were men and one was a woman.None had a history of hypertension; none hadelevated blood pressure when initially examined,
and none were hypertensive during their hospitalcourse. All six patients had biopsy evidence of fattyliver or cirrhosis. All were anemic with low plateletcounts and abnormal prothrombin and partial throm-boplastin times. Four patients initially had seizures;in two, this initial seizure was believed to be an
by guest on May 8, 2018
http://stroke.ahajournals.org/D
ownloaded from
1568 Stroke Vol 19, No 12, December 1988
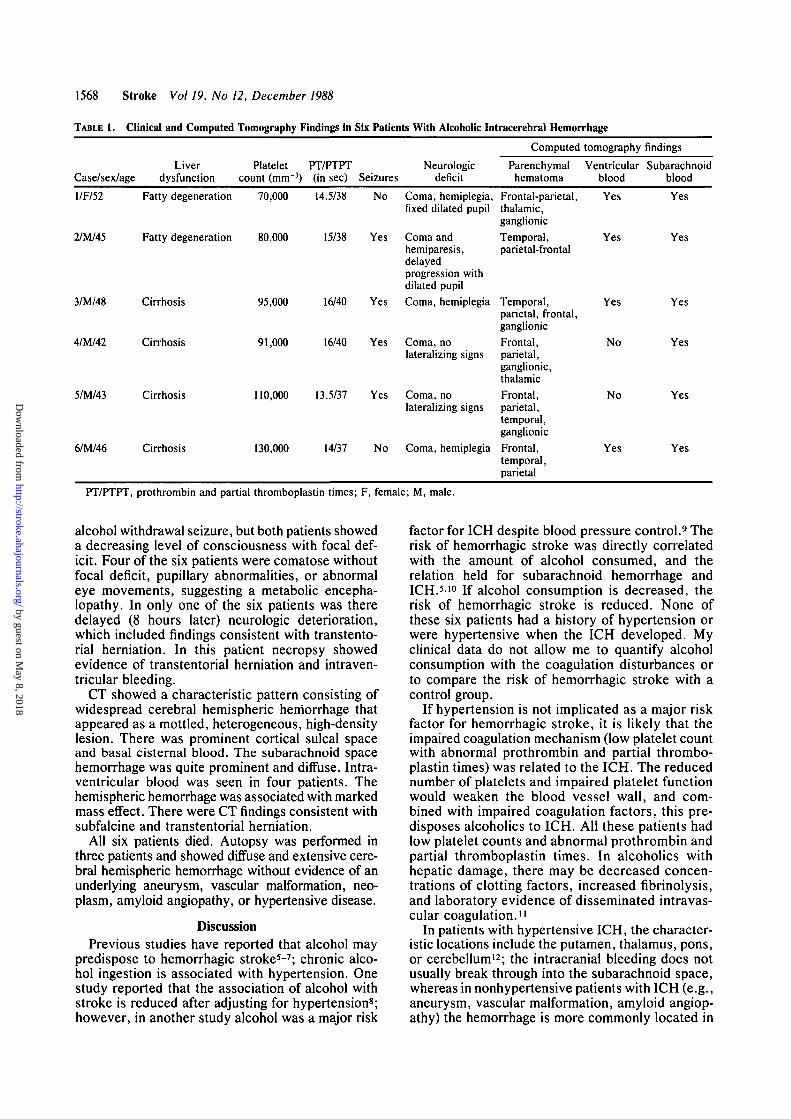
TABLE 1. Clinical and Computed Tomography Findings in Six Patients With Alcoholic Intracerebral Hemorrhage
Liver Platelet PT/PTPT NeurologicCase/sex/age dysfunction count (mm"3) (in sec) Seizures deficit
Computed tomography findings
Parenchymal Ventricular Subarachnoidhematoma blood blood
l/F/52 Fatty degeneration 70,000 14.5/38 No Coma, hemiplegia,fixed dilated pupil
2/M/45
3/M/48
4/M/42
5/M/43
6/M/46
Fatty degeneration 80,000
Cirrhosis
Cirrhosis
Cirrhosis
Cirrhosis
95,000
91,000
15/38 Yes Coma andhemiparesis,delayedprogression withdilated pupil
16/40 Yes Coma, hemiplegia
16/40 Yes Coma, nolateralizing signs
110,000 13.5/37 Yes Coma, nolateralizing signs
130,000 14/37 No Coma, hemiplegia
Frontal-parietal,thalamic,ganglionicTemporal,parietal-frontal
Temporal,parietal, frontal,ganglionicFrontal,parietal,ganglionic,thalamicFrontal,parietal,temporal,ganglionicFrontal,temporal,parietal
Yes
Yes
Yes
No
No
Yes
Yes
Yes
Yes
Yes
Yes
Yes
PT/PTPT, prothrombin and partial thromboplastin times; F, female; M, male.
alcohol withdrawal seizure, but both patients showeda decreasing level of consciousness with focal def-icit. Four of the six patients were comatose withoutfocal deficit, pupillary abnormalities, or abnormaleye movements, suggesting a metabolic encepha-lopathy. In only one of the six patients was theredelayed (8 hours later) neurologic deterioration,which included findings consistent with transtento-rial herniation. In this patient necropsy showedevidence of transtentorial herniation and intraven-tricular bleeding.
CT showed a characteristic pattern consisting ofwidespread cerebral hemispheric hemorrhage thatappeared as a mottled, heterogeneous, high-densitylesion. There was prominent cortical sulcal spaceand basal cisternal blood. The subarachnoid spacehemorrhage was quite prominent and diffuse. Intra-ventricular blood was seen in four patients. Thehemispheric hemorrhage was associated with markedmass effect. There were CT findings consistent withsubfalcine and transtentorial herniation.
All six patients died. Autopsy was performed inthree patients and showed diffuse and extensive cere-bral hemispheric hemorrhage without evidence of anunderlying aneurysm, vascular malformation, neo-plasm, amyloid angiopathy, or hypertensive disease.
DiscussionPrevious studies have reported that alcohol may
predispose to hemorrhagic stroke5-7; chronic alco-hol ingestion is associated with hypertension. Onestudy reported that the association of alcohol withstroke is reduced after adjusting for hypertension8;however, in another study alcohol was a major risk
factor for ICH despite blood pressure control.9 Therisk of hemorrhagic stroke was directly correlatedwith the amount of alcohol consumed, and therelation held for subarachnoid hemorrhage andICH.510 If alcohol consumption is decreased, therisk of hemorrhagic stroke is reduced. None ofthese six patients had a history of hypertension orwere hypertensive when the ICH developed. Myclinical data do not allow me to quantify alcoholconsumption with the coagulation disturbances orto compare the risk of hemorrhagic stroke with acontrol group.
If hypertension is not implicated as a major riskfactor for hemorrhagic stroke, it is likely that theimpaired coagulation mechanism (low platelet countwith abnormal prothrombin and partial thrombo-plastin times) was related to the ICH. The reducednumber of platelets and impaired platelet functionwould weaken the blood vessel wall, and com-bined with impaired coagulation factors, this pre-disposes alcoholics to ICH. All these patients hadlow platelet counts and abnormal prothrombin andpartial thromboplastin times. In alcoholics withhepatic damage, there may be decreased concen-trations of clotting factors, increased fibrinolysis,and laboratory evidence of disseminated intravas-cular coagulation."
In patients with hypertensive ICH, the character-istic locations include the putamen, thalamus, pons,or cerebellum12; the intracranial bleeding does notusually break through into the subarachnoid space,whereas in nonhypertensive patients with ICH (e.g.,aneurysm, vascular malformation, amyloid angiop-athy) the hemorrhage is more commonly located in
by guest on May 8, 2018
http://stroke.ahajournals.org/D
ownloaded from
Weisberg Alcoholic Intracerebral Hemorrhage 1569
the subcortical hemispheric white matter and breaksthrough into the subarachnoid spaces.1314 In hyper-tensive ICH, CT shows a homogeneous hyperdensenonenhancing lesion, usually with a surroundinghypodense region representing edema. Althoughmany patients with ICH have erythrocytes in thecerebrospinal fluid, CT rarely shows subarachnoidblood. All six alcoholic patients with cerebral hemi-spheric hemorrhage showed cisternal and corticalsulcal blood; however, autopsy showed no otheridentifiable cause of the ICH. In one patient therewas delayed neurologic deterioration consistent withtranstentorial herniation. Without an early CT atthe time the initial neurologic dysfunction devel-oped and a repeat CT after the delayed neurologicdeterioration, I could not precisely determine themechanism of the delayed deterioration. Potentialpathologic mechanisms include worsening of theedema, herniation, and intraventricular extensionof the bleeding. The infrequent finding of delayedneurologic deterioration in these six alcoholicpatients is consistent with the low incidence reportedin ICH series.1415
Based on the location, size, and the CT pattern ofthe alcoholic hemorrhage, it is most unlikely thatthis represented a hemorrhagic contusion or a trau-matic ICH. The CT pattern was also not consistentwith a hemorrhagic cerebral infarction. The intra-cranial blood was widely dispersed within the sub-arachnoid spaces. There was blood in the superfi-cial cortical and subcortical white matter, withextension into the basal ganglia and thalamus.Despite the large size and prominent mass effect(with evidence of subfalcine and transtentorial her-niation), surrounding hypodense areas representingedema were not seen. This lack of CT-visualizededema is contrasted with the findings of prominentedema in other large nonalcohol-related ICHs. Noneof these six alcoholic patients showed multipleICHs. I suggest that chronic alcohol exposure maylead to massive cerebral hemorrhage. Other studies
using large sample sizes and quantitative features ofalcohol ingestion and coagulation may settle thesignificance of this finding.
References1. Gorelick PB: Alcohol and stroke. Stroke 1987;18:268-2712. Arkwright PD, Beilin LJ, Rouse 1, Armstrong BK, Van-
dongen R: Effects of alcohol use and other aspects oflifestyle on blood pressure levels and prevalence of hyper-tension in a working population. Circulation 1982;66:60—66
3. Gill JS, Zezulka AV, Shipley MJ, Gill SK, Beevers DG:Stroke and alcohol consumption. N Engl J Med 1986;315:1041-1046
4. Kagan A, Popper JS, Rhoads GG: Dietary and other riskfactors for stroke in Hawaiian Japanese men. Stroke 1985;16:39-45
5. Donahue RP, Abbott RD, Reed DM.Yano K: Alcohol andhemorrhagic stroke: The Honolulu Heart Program. JAMA1986;255:2311-2314
6. Hillbom M, Kaste M: Alcohol intoxication: A risk factor forprimary subarachnoid hemorrhage. Neurology 1982;32:706-711
7. Hillbom M, Kaste M: Does alcohol intoxication precipitateaneurysmal subarachnoid hemorrhage? J Neurol NeurosurgPsychiatry 1981 ;44:523-526
8. Stokes GS: Hypertension and alcohol: Is there a link? JChronic Dis 1982 ;35:759-762
9. Kozararevic D, Vojvodic N, Dawbir N, McGee D, Racic Z,Gordon T, Zukel W: Frequency of alcohol consumption andmorbidity and mortality. The Yugoslavia CardiovascularDisease Study. Lancet 1980;l:613-616
10. Kagan A, Popper JS, Rhoads GG: Factors related to strokeincidence in Hawaii Japanese men: The Honolulu HeartStudy. Stroke 1980;l 1:14-21
11. Cowan DH: Effects of alcoholism on hemostasis. SeminHematol \9$0;\l:137-147
12. Weisberg LA: Computerized tomography in intracerebralhemorrhage. Arch Neurol 1979;36:422-426
13. McCormick WF, Rosenfield DB: Massive brain hemorrhage:A review of 144 cases and an examination of their causes.Stroke 1973;4:946-954
14. Weisberg LA: Subcortical lobar intracerebral hemorrhage:Clinical-computed tomographic correlations. J Neurol Neu-rosurg Psychiatry 1985;48:1078-1084
15. Weisberg LA: Primary putaminal hemorrhage: Clinical-CTcorrelations (abstract). Neurology 1988;38(suppl 1): 149
KEY WORDS • alcoholism• cerebral hemorrhage
blood coagulation • blood platelets
by guest on May 8, 2018
http://stroke.ahajournals.org/D
ownloaded from
L A WeisbergAlcoholic intracerebral hemorrhage.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1988 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.19.12.1565
1988;19:1565-1569Stroke.
http://stroke.ahajournals.org/content/19/12/1565World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 8, 2018
http://stroke.ahajournals.org/D
ownloaded from