Embed Size (px)
Citation preview

Sexually Transmitted Diseases• Chlamydia*• Gonorrhea* • Syphilis*• Genital herpes*• Condyloma
acuminatum (genital warts)* HPV
• Chancroid
• Infectious Mononucleosis**
• HIV – AIDS• Trichomoniasis • Granuloma inquinale • Hepatitis B, C, D• Others

Chlamydia Infections • Genital infections caused by
Chlamydia trachomatis represent the most common bacterial sexually transmitted disease in the United States

Chlamydia Infections• Incidence and prevalence • About 4 million cases occur each year• Peak incidence is in the late teens and early
twenties• Prevalence of chlamydia urethral infection
among young men seen in general medial settings is 3% to 5%
• Prevalence of chlamydia cervical infection for asymptomatic college students and prenatal patients is 5%

Chlamydia InfectionsMen Women Nongonococcal urethritis Postgonococcal urethritis (develops 2 to 3 weeks after single drug Rx for gonococcal urethritis) Epididymitis Proctitis Conjunctivitis Reiter’s syndrome (consists of conjunctivitis, urethritis and mucocutaneous lesions)
Acute urethral syndromeBartholinitis Cervicitis Proctitis Endometritis Salpingitis Conjunctivitis Perihepatitis Reiter’s syndrome (consists of conjunctivitis, cervicitis and mucocutaneous lesions)

Gonorrhea• Gonorrhea is the second-most-
common reported infectious disease in the United States behind chlamydia
Neiseria gonorrhoeae –
gram-negative diplococcus

Gonorrhea - • Incidence (reported) • 1979 – 1,000,000 cases• 1990 - 900,000 cases• 1998 - 355,642 cases
• During the last 3 years the reported incidence has been increasing among adolescents, gay and bisexual men and African Americans

QuickTime™ and a decompressor
are needed to see this picture.
QuickTime™ and a decompressor
are needed to see this picture.

STDs• Gonorrhea and syphilis
in just 2 years( 2002-2004) > 45 % increase in selected U.S. cities
( e.g. Detroit and St. Louis)

Transmission of Gonorrhea • Transmission is
almost exclusively by sexual contact
• Disseminated gonococcal infection (DGI) may occur
• Transmission by inanimate objects is very rare
• Vertical transmission during parturition
Mandell GL; Atlas of Infectious Diseases, Vol. V, Churchill Livingstone, p 1.5, 1996

Gonorrhea • Signs and
symptoms• 1 to 3 % of men are
asymptomatic • In men symptoms usually
occur after incubation period of 2 to 5 days
• Mucopurulent urethral discharge
• Pain on urination• Urgency and increased
frequency of urination• Pharyngeal infection in up
to 50% of cases
• Signs and symptoms• About 50% of women are
asymptomatic • Tenderness and swelling of
the meatus can occur • Vaginal or urethral discharge• Pain on urination• Urgency and increased
frequency of urination• Anal canal infection common
in both males and females

Gonorrhea• Gonococcal
pharyngitis • Is seen in both men
and women who have had oral sexual exposure
• Impossible clinically to differentiate from pharyngitis caused by other bacteria – must culture
• Left untreated it will resolve within 6 weeks
Mandell GL; Atlas of Infectious Diseases, Vol. V, Churchill Livingstone, p 1.10, 1996

Gonorrhea• Disseminated
gonococcemia (dermatitis)
• Most common signs of dissemination are myalgia, arthralgia, polyarthritis and dermatitis
Harrison’s Online, hppt://www.harrisonsonline.com, plate 11D-60, 2002

Gonorrhea• Risk factors• Adolescence • Multiple sexual partners• Nonbarrier contraception • Low socioeconomic status• Use of IV drugs or crack cocaine• Previous history of gonorrhea

Syphilis• Syphilis is the fourth-most-
frequently reported sexually transmitted disease surpassed only by chlamydia, gonorrhea, and AIDS

Syphilis•Etiology • Etiologic agent is Treponema pallidum • It is a slender, fragile, anaerobic
spirochete• T. pallidum is easily killed by heat,
drying, disinfectants, and soap and water• The organism is difficult to stain, except
for certain silver impregnation methods

Syphilis• Pathophysiology • T. pallidum does not invade intact skin• It can gain entry via minute abrasions or hair follicles • It can invade intact mucosal epithelium• Within hours after invasion it spreads to the
lymphatics and blood stream• Early response to the bacterial invasion is endarteritis
and periarteritis • Risk of transmission occurs during primary,
secondary, and early latent stages of the disease but not in late syphilis

Course of Untreated Syphilis
Mandell GL; Atlas of Infectious Diseases, Vol. V, Sexually Transmitted Diseases, Churchill Livingstone, p10.2, 1996

Course of Untreated Syphilis
Mandell GL; Atlas of Infectious Diseases, Vol. V, Sexually Transmitted Diseases, Churchill Livingstone, p10.2, 1996
Syphilis - Primary• Classic manifestation of
primary syphilis is the chancre
• It consists of a solitary granulomatous lesion at the site of contact with the infectious organism
• The chancre occurs usually within 2 to 3 weeks after exposure
• Patient is infectious before the appearance of the chancre
• Lesion begins as a small papule and enlarges to form a surface erosion or ulceration
• Associated with the chancre are enlarged, painless, hard regional lymph nodes
• The chancre subsides in 3 to 6 weeks
• The genitalia, lips, tongue, fingers, nipples, and anus are common sites for chancres

Syphilis• Chancre of
primary syphilis• Ulceration of
tongue on left dorsal surface
Neville BW: Oral & Maxillofacial Pathology, 2nd edition, Mosby, p168, 2002

Syphilis – Secondary• Maculopapular
rash of secondary syphilis on the trunk
• The symptoms of secondary syphilis appear about one month after the onset of primary syphilis
Mandell GL; Atlas of Infectious Diseases, Vol. V, Sexually Transmitted Diseases, Churchill Livingstone, p 9.10, 1996
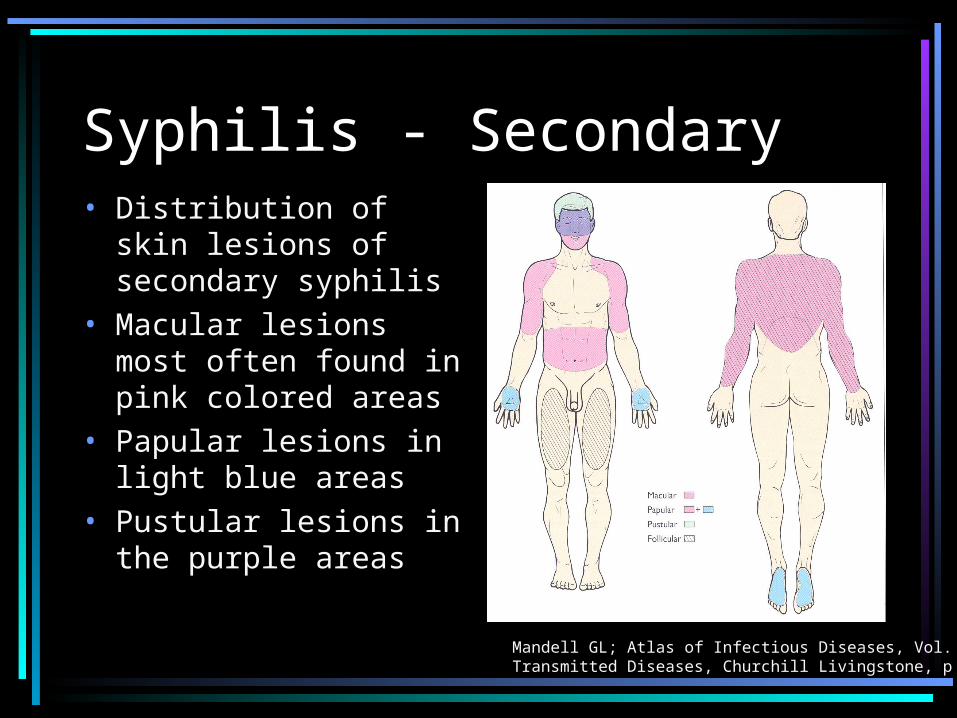
Syphilis - Secondary• Distribution of skin
lesions of secondary syphilis
• Macular lesions most often found in pink colored areas
• Papular lesions in light blue areas
• Pustular lesions in the purple areas
Mandell GL; Atlas of Infectious Diseases, Vol. V, Sexually Transmitted Diseases, Churchill Livingstone, p 9.10, 1996

Syphilis• Secondary
syphilis• Erythematous
rash affecting the palm of the hand
Neville BW: Oral & Maxillofacial Pathology, 2nd edition, Mosby, p169, 2002

Syphilis• Mucous patch of
secondary syphilis(lips)
• Whitish zone of exocytosis and spongiosis of lower labial mucosa
Neville BW: Oral & Maxillofacial Pathology, 2nd edition, Mosby, p169, 2002

Syphilis – Tertiary • Tertiary (late) stage of
syphilis occurs in up to 40% of untreated patients
• Patients are noninfectious• Is the destructive stage of
the disease• Any organ of the body can
be involved• Classic lesion is the
gumma, thought to be the end result of a hypersensitivity reaction
• All other manifestations of tertiary syphilis are vascular in nature and result from an obliterative endarteritis
• Aneurysm of the aorta• Neurosyphilis can consist
of altered tendon reflexes, meningitis, general paresis, or tabes dorsalis
• Oral lesions are a diffuse interstitial glossitis and the gumma

Syphilis • Tertiary syphilis• Palatal gumma
Regezi JA: Atlas of Oral and Maxillofacial Pathology, W.B. Saunders, p 6, 2000

Syphilis• Congenital
syphilis• Hutchinson’s
incisors (greatest mesiodistal width in the middle third of the crown)
Neville BW: Oral & Maxillofacial Pathology, 2nd edition, Mosby, p170, 2002

Syphilis• Congenital
syphilis• Mulberry molar
(maxillary molar demonstrating occlusal surface with numerous globular projections
Neville BW: Oral & Maxillofacial Pathology, 2nd edition, Mosby, p170, 2002

Syphilis – Treatment • Primary, secondary, early latent • Single injection of long-acting benzathine penicillin
(penicillin G, 2.4 million units)• Allergic to penicillin • Oral doxycycline (100 mg bid for two weeks)• Oral erythromycin (500 mg, qid for two weeks)• IM ceftriazone sodium
• Screen for HIV infection
• Congenital syphilis• Test all pregnant women for syphilis by serology• If Positive treat expectant mother with penicillin

Syphilis• Primary syphilis• Chancre of the
tongue

Syphilis – Dental Transmission• Lesions of untreated primary and
secondary syphilis are infectious as are the patient’s blood and saliva
• Patients being treated or have a positive serology test for syphilis should be viewed as potentially infectious
• Necessary dental care may be provided unless oral lesions are present
• Once the oral lesions have cleared the patient can commence dental treatment

Genital Herpes• Genital herpes is a recurrent,
incurable viral infection of the genitalia caused by one of two closely related types of herpes simplex virus (HSV) types 1 & 2
• Most genital infections are caused by HSV type 2

Genital Herpes• Incidence and prevalence• Not a reportable disease• Many cases are mild or asymptomatic• 45 million in USA are infected• More than 750,000 seroconvert/year• 70% to 90% of first case infections caused by
HSV-2• Prevalence is 45% in African Americans and
18% in whites• Prevalence has increased by 30% since the
late 1970s

Genital Herpes – Signs and Symptoms• HSV-2 infections• 60% are asymptomatic • Incubation period 2-7 days• Lesions appear – papules,
vesicles, ulcers, crusts, and fissures
• Lesions in moist areas ulcerate early and are painful
• Painful lymphadenopathy, fever, malaise, myalgia occur
• Recurrent lesions usually less severe
• A prodrome of localized itching, tingling, pain, and burning precedes vesicular eruption
• Healing of recurrent lesions occurs in 10 to 14 days
• Constitutional symptoms are generally absent
• Between recurrences infected persons shed virus intermittently in the genital tract

Genital Herpes• HSV keratitis • A nonhealing
corneal ulcer of the right eye in a 15-year old girl with AIDS
• Culture showed HSV-1 infection
Mandell GL; Atlas of Infectious Diseases, Vol. V, Sexually Transmitted Diseases, Churchill Livingstone, p 15.13, 1996

Genital Herpes• Autoinoculation of the
thumb (herpetic whitlow) after primary genital herpes
• Autoinoculation of distant sites is often seen during primary HSV infection
• Once latency is established periodic reactivation can occur
Mandell GL; Atlas of Infectious Diseases, Vol. V, Sexually Transmitted Diseases, Churchill Livingstone, p 15.10, 1996

Genital Herpes - Treatment• First Clinical episode • Antiviral therapy – acyclovir 400 mg orally 3
times daily for 7 to 10 days • Counseling regarding natural history of genital
herpes, sexual and perinatal transmission, and how to reduce transmission
• Frequent recurrences (6 or more/year)
• Daily suppressive antiviral therapy can be used• Acyclovir 400 mg orally 2 times daily

Genital Herpes

Genital Herpes• Recurrent
herpetic whitlow • HSV infection may
be acquired on the finger as sometimes is seen in dentists and medical personal
Mandell GL; Atlas of Infectious Diseases, Vol. V, Sexually Transmitted Diseases, Churchill Livingstone, p 15.13, 1996

HPV Infection• Condyloma
acuminatum

HPV Infection• Incidence and prevalence • HPV infections are one of the three most common
sexually transmitted diseases in the United States• An estimated 20 million Americans have genital
HPV infections that can be transmitted by sexual contact
• About 18% of women and 8% of men carry genital HPV
• Highest infection rate is found in 19 to 26 year old individuals

HPV Infection • Dental management • Genital condylomata acuminatum do
not affect dental management • Oral lesions are infectious• Universal precautions must be used• Presence of oral lesions necessitates
referral to rule out genital lesions• Excisional biopsy is recommended for
HPV-associated oral lesions

HPV Infection• Oral condyloma
acuminatum
• Microscopic appearance of lesion shown above

STDs • Dental management • Patients may come to the dentist because of oral signs and
symptoms• The dentist can screen the patient or refer to a physician for
diagnosis and Rx • Caution because of transmission to others• Be aware of other conditions• If the dentist screens the patient a complete blood count,
heterophil antibody test (Monospot), and EBV-antigen testing are indicated
• Delay routine dental treatment until patient has recovered (3 to 6 weeks)

Infectious Mononucleosis • Not classically defined as a
sexually transmitted disease• However transmission is by
intimate personal contact• Most cases caused by Epstein-Barr
virus (a lymphotropic herpes virus)

Infectious Mononucleosis • Incidence and prevalence• More than 90% of adults worldwide have been
infected with EBV• In the United States 50% of 5 year old children
and 70% of College freshman show evidence
of prior infection with EBV
• 10% to 20% of asymptomatic, seropositive adults (antibodies to EBV) carry the virus in their oropharyngeal region

Infectious Mononucleosis • Pathophysiology • Transmitted through exposure to oropharyngeal
secretions and on occasion by infected blood products• Incubation period is 30 to 50 days• Infection of B lymphocytes induces large reactive
lymphocytes (T lymphocytes) which make up about 10% lymphocytes on blood smears
• Acute infection involves reactive lymphocytes, cytokines they produce and B-cell produced antibodies (heterophile) against EBV
• Enlargement of the spleen occurs in 40% to 50% of cases• Rupture of the spleen occurs in 0.1% to 0.2% of all cases

Infectious Mononucleosis• Signs and symptoms• Asymptomatic when found in children • In young adults about 50% will be symptomatic• Fever, sore throat, and lymphadenopathy occur in most
of the symptomatic patients• Other clinical features include malaise, fatigue, an
absolute lymphocytosis (more than 10% reactive lymphocytes) and a positive heterophil antibody test
• Palatal petechiae are found in about 33% of the patients during the first week of the illness
• About 30% of the symptomatic patients develop an exudative pharyngitis and 10% develop a skin rash and/or petechiae

Infectious Mononucleosis •Oral manifestations • Fever• Severe sore throat• Palatal and lip petechiae• Enlarged, tender anterior and
posterior cervical lymph nodes

Infectious Mononucleosis• Hyperplastic
pharyngeal tonsils with yellowish crypt exudates in a patient with infectious mononucleosis Neville BW; Oral & Maxillofacial Pathology, 2 ed, W.B. Saunders Co.
p 225, 2002

Infectious Mononucleosis• Numerous
petechiae of the soft palate in a patient with infectious mononucleosis
• Petechiae are found in up to 25% of the patients

Infectious Mononucleosis • Medical management • Symptomatic treatment consisting of bed rest,
acetaminophen or NSAIDs for pain control, and gargling and irrigation with saline solution
• Avoid vigorous activities to avoid rupture of spleen• Short course of prednisone for patients with exudative
pharyngotonsillitis, pharyngeal edema, and upper airway obstruction
• 20% of symptomatic patients develop streptococcal infection and need to be treated with penicillin V if they are not allergic to it (avoid ampicillin as more than 90% of these patients will develop an allergic skin rash to the drug)

Infectious Mononucleosis • Dental management • Patients may come to the dentist because of oral
signs and symptoms• The dentist can screen the patient or refer to a
physician for diagnosis and Rx • If the dentist screens the patient a complete
blood count, heterophil antibody test (Monospot), and EBV-antigen testing are indicated
• Delay routine dental treatment until patient has recovered (3 to 6 weeks)

Gonorrhea • Pelvic inflammatory
disease (PID) • PID occurs in about 30%
of women who have untreated gonococcal infection
• Complications are infertility (10%) incidence for each episode of PID
Mandell GL; Atlas of Infectious Diseases, Vol. V,Churchill Livingstone, p 1.9, 1996





























