Embed Size (px)
Citation preview

Septic ArthritisS. Shadmanfar .M.D
Rheumatologist
pathogens
• Bacterial
• Spirochetes• Fungi• viruses
Septic arthritis =Infectious Arthritis =Bacterial arthritis
Etiology (microbiology)
• Gram positive cocci (80%)– S. aureus
• Gram-negative bacilli (20%)
Bacterial arthritis
Gonoccocal
Non gonoccal
Pathogens • Young adult and adolescents:• N. gonorrhoeae ( most common )
• S. aureus accounts for most
nongonococcal isolates in adults of all ages
EPIDEMIOLOGY
• Incidence:– 40-68/100000/ yr in Prosthetic joint
– 28-38/ 100000/ yr in RA
– 5- 12/ 100000/ yr in Children
– 2-10/ 100000/ yr in General population
EPIDEMIOLOGY• Incidence: 2-10 cases per 100000 in
general population • Ages peak: younger than 5 years and
older 64 years• 1/3 were previously healthy children and
in contrast only 15% were previously healthy adult
Risk Factors• Old age (>80 Y)
• Rheumatoid arthritis• DM• Glucocorticoid therapy• Hemodialysis• Malignancy• TNF inhibitors• IV drug users
Acute bacterial infection
• Acute• Monarticular• Hematogenous• S.aureus• knee
Site of involvement
Site of involvement
• Mono (80-90%)• Knee: 55%• Ankle: 10%• Wrist: 9%• Shoulder: 7%• Hip: 5%• Elbow: 5%• SC: 5%- IV drug abuser• SI: 2%- IV drug abuser• Foot joints: 2%
• Poly (more than 1 joint): – RA
Clinical manifestation
• Mod-sever pain• Effuion• Erythem, swollen joint• Decreased range of motion• fever
Clinical manifestation
• Joint pain• Joint tenderness• Joint swelling• Joint stiffness• Joint warmth• Joint redness• Difficulty moving joint



The most important test
–Direct joint aspiration
• Should be performed in every caseof suspected infection as a
• Diagnostic or therapeutic maneuver

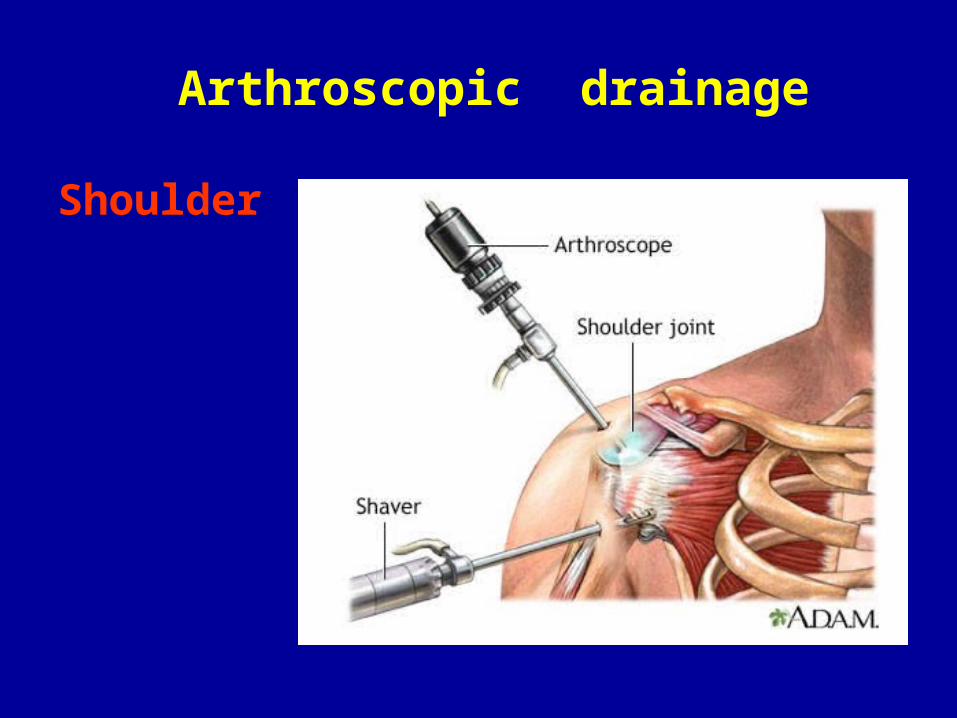
Arthroscopic drainage
Shoulder
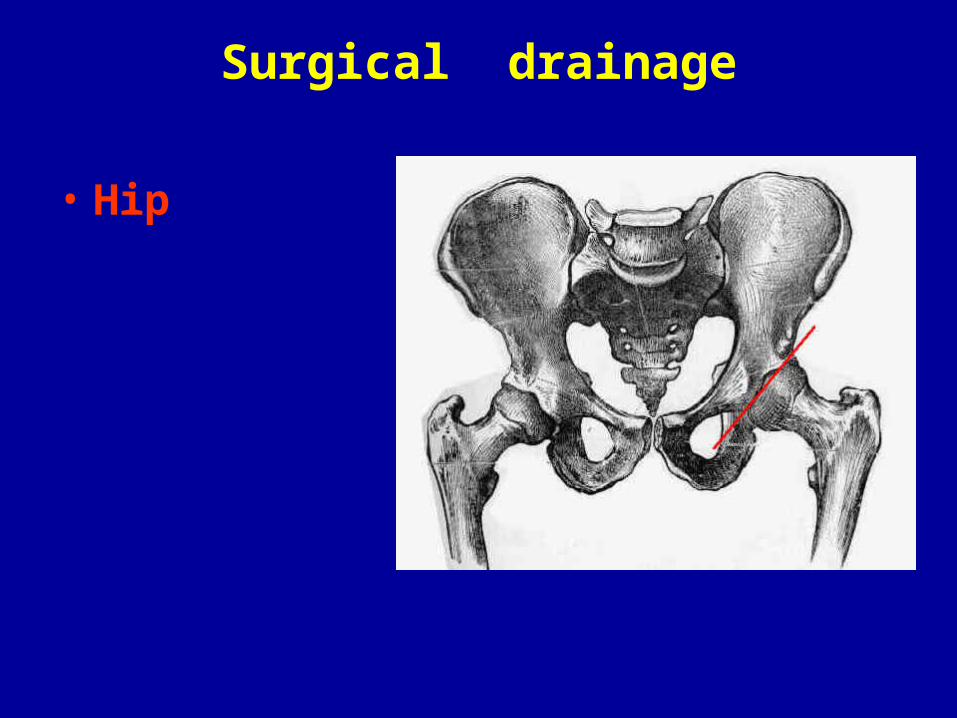
Surgical drainage
• Hip
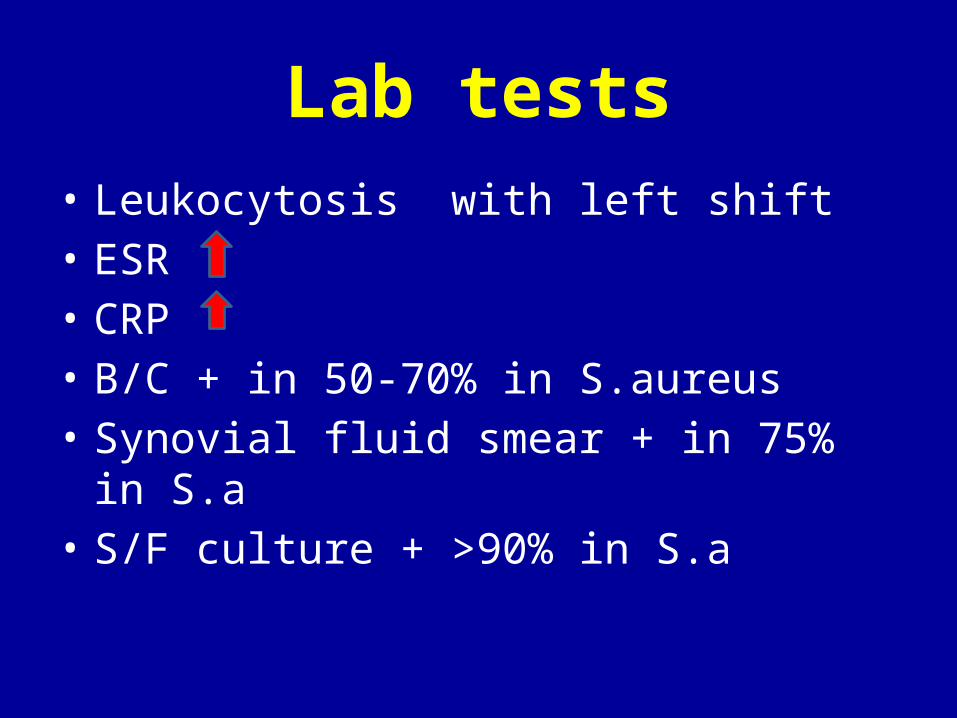
Lab tests• Leukocytosis with left shift• ESR• CRP• B/C + in 50-70% in S.aureus• Synovial fluid smear + in 75% in S.a• S/F culture + >90% in S.a
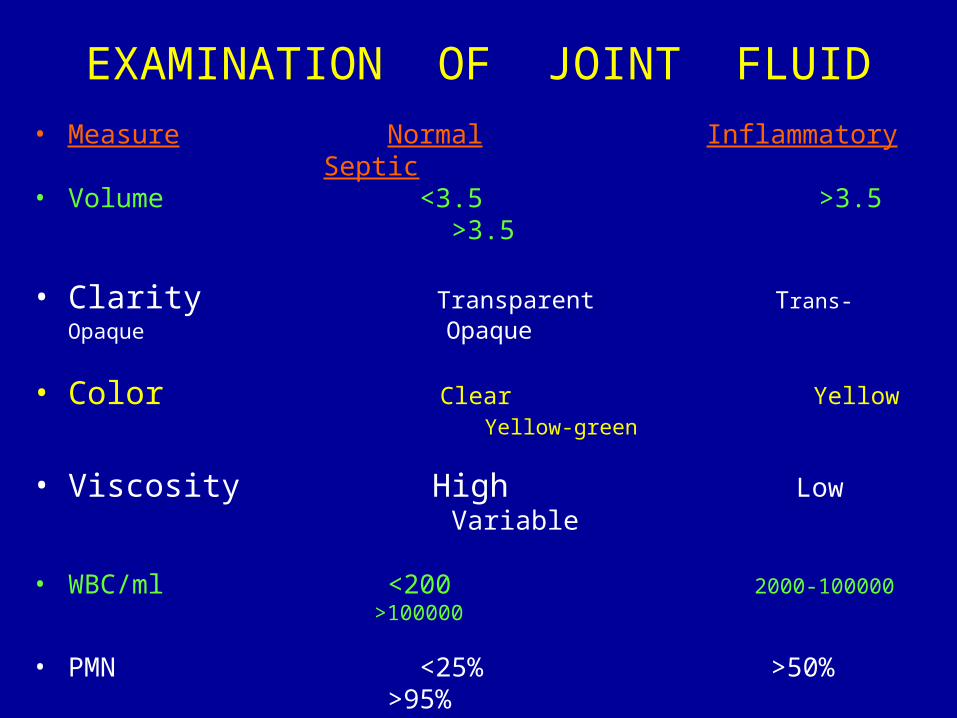
EXAMINATION OF JOINT FLUID• Measure Normal Inflammatory
Septic• Volume <3.5 >3.5 >3.5
• Clarity Transparent Trans-Opaque Opaque
• Color Clear Yellow Yellow-green
• Viscosity High Low Variable
• WBC/ml <200 2000-100000 >100000
• PMN <25% >50% >95%
• Culture Neg Neg Pos
• Smear Neg Neg Pos
Radiography
• Early:– Predisposing agent – Soft tissue swelling – Joint space widening
• Late (2-3 w):– Erosion – Joint space narrowing
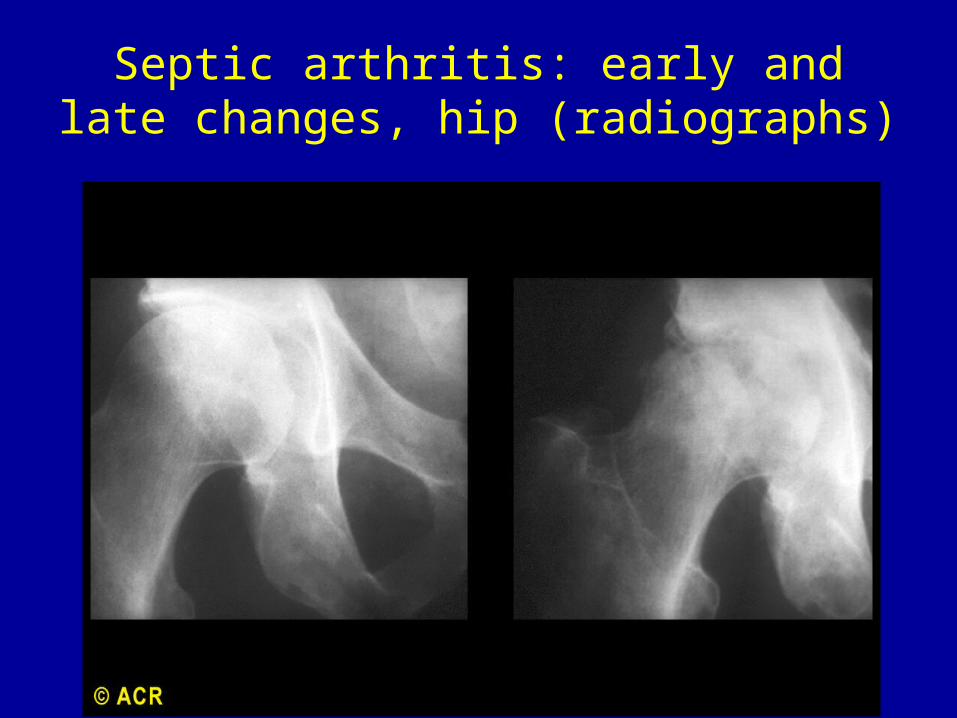
Septic arthritis: early and late changes, hip (radiographs)
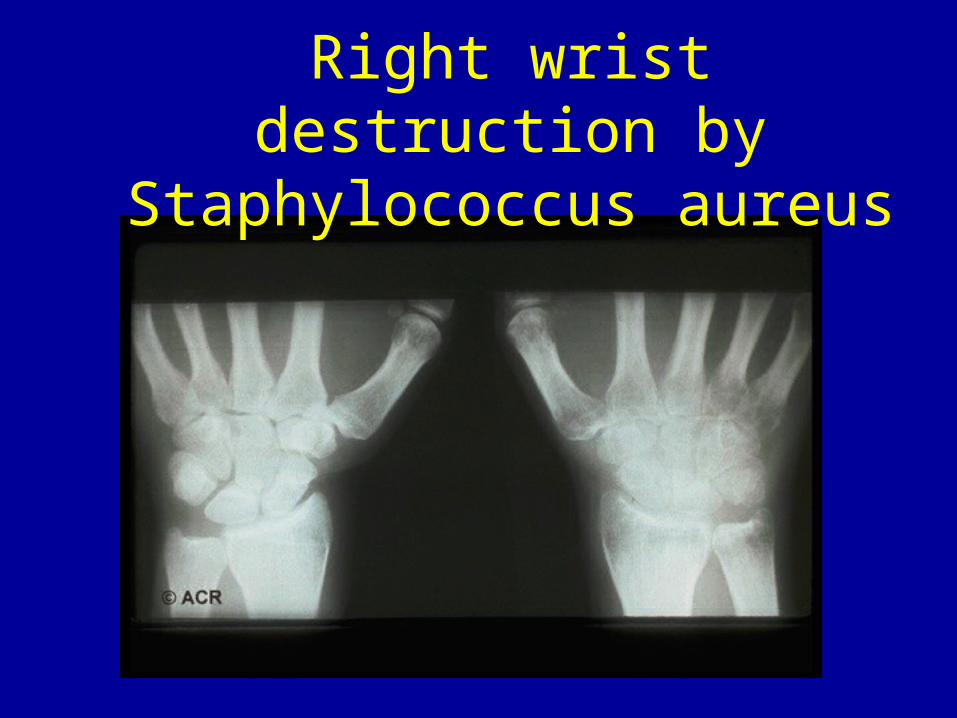
Right wrist destruction by Staphylococcus aureus
Treatment :nongonococcal
******Drainage of the pus******
******IV antibiotics are essential******
Treatment :nongonococcal
• B/C & synovial/C• Empirical antibiotic• Direct antibiotic into joint is not
necessary• Drainage of pus arthroscopic drainage for hip,
shoulder
treatment
• Immobilization?
do not require
except for pain control
GONOCOCCAL INFECTION
Gonoccocal arthritis
Epidemiology :
70% infectious arthritis in persons< 40Y
In united states
Gonoccocal arthritis
• DGI: disseminated gonococcal infection• Purulant arthritis
disseminated gonococcal infection (DGI)
• 1-3% N. gonorrhoeae• Women 3 times of men• Fever• Chills• Vesiculopustular skin lesion• Tenosynovitis• migratory polyarthritis
DGI
• S/F : 10,000-20,000 WBC• S/F culture: negative• B/C culture : <45% +• Culture should be obtained : mucosal sites


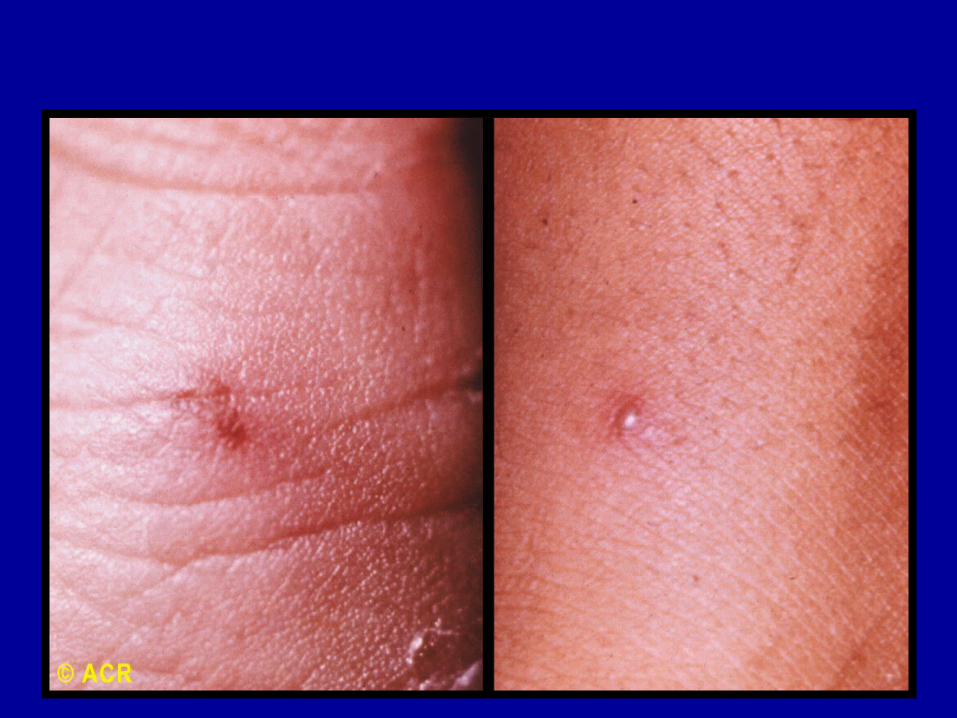

Gonorrhea: pustule
DGI• Immune reaction to circulating gonococci
• Immune complex deposition in tissues
Gonoccocal septic arthritis
• Monarticular knee ,ankle ,wrist• S/F culture positive• S/F >50000• B/C negative
treatment
Ceftriaxone + ciprofloxacin 7 days
Mycobacterial infection
• Musculoskeletal TB • 1% all TB• 10% extrapulmonary TB
Tuberculous Arthritis
Reactivation of a hematogenously seeded focus
Musculoskeletal TB
• Spine thoracic , lumbar• Peripheral joint hip
knee
wrist
• Bone osteomyelitis• Soft tissue
Tuberculous Arthritis
• Chronic monarthis• Large, weight –bearing hip, knee• Middle-age or older• Underlying disease• Onset insidious• Joint pain, swelling• Sign of inflammation limited
Tuberculous Arthritis
• Constitutional symptoms unusual• PPD test positive• CXR NL• XR erosion , narrowing, osteoporpsis
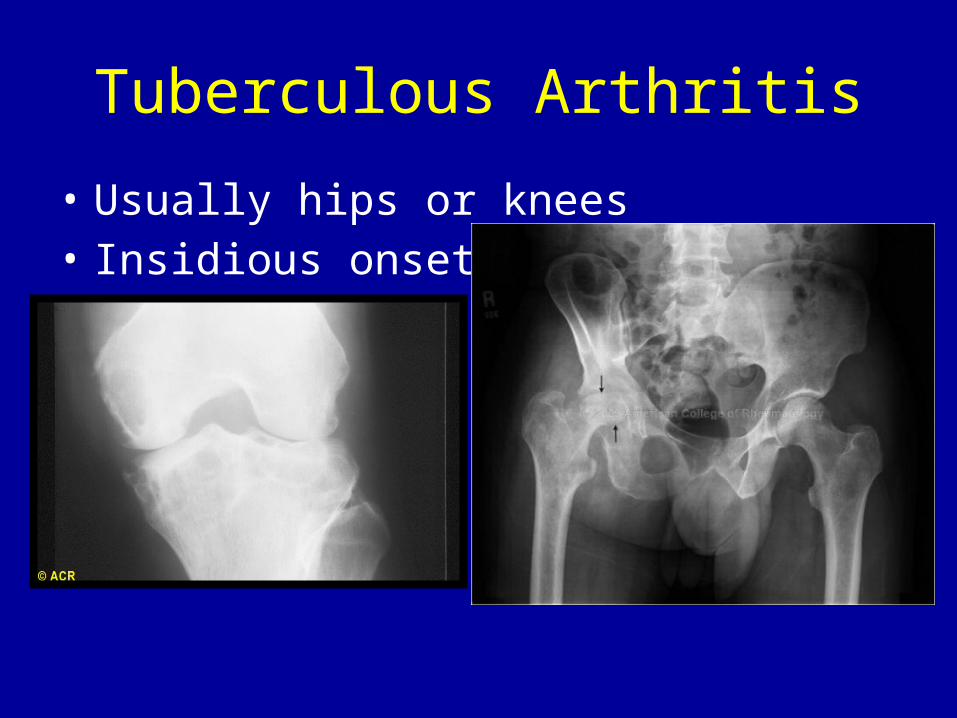
Tuberculous Arthritis
• Usually hips or knees• Insidious onset
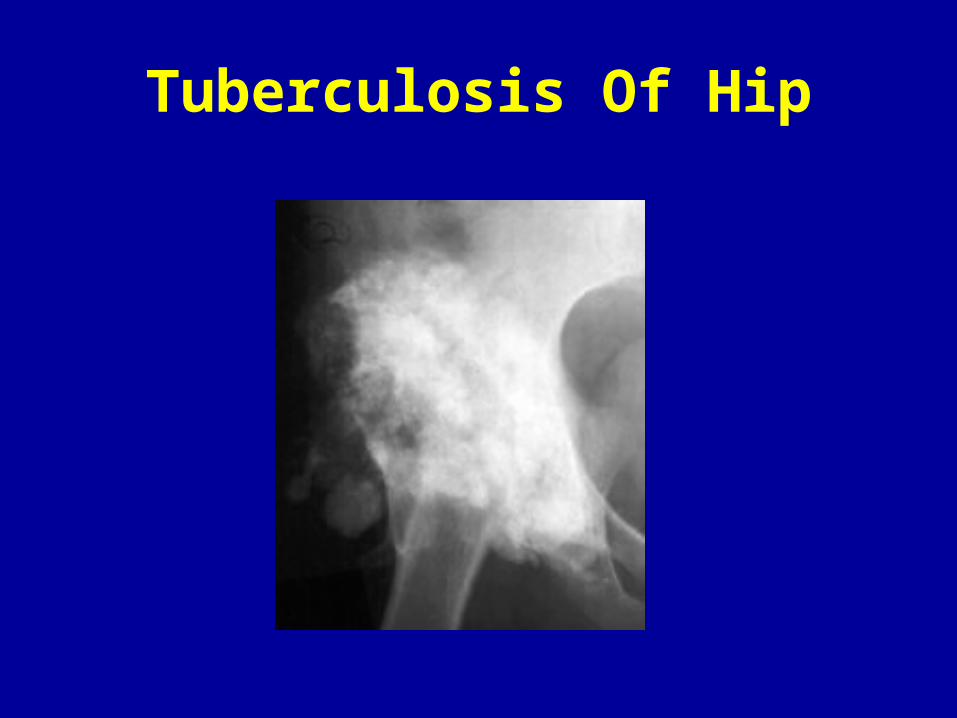
Tuberculosis Of Hip
Tuberculous Arthritis
• S/F 20000 PMN• Synovial AFB Smear positive 20%• Synovial culture positive 80%• Synovial tissue culture “”’’’” 90%
Tuberculous Arthritis
• Diagnose
Best made by :
Histologic and microbiologic examination of synovium
Caseating or noncaseating granulomas
Tuberculous Arthritistreatment
Combination chemotherapy
INH , RIF, ETB, PZA
Viral arthritis
• acute self limited pattern
Respiratory virus ( Parvo virus B19 ) , Rubella
• Chronic infection
Hepatitis B,C- HIV
• Latent infection with potential reactivation
Herpes virus ( Varicell Zoster )
Viral Arthritis
• Parvovirus B19 ,Fifth’s disease in children• Mumps• Rubella and postvaccination( Arthralgia,
Lumbar radiculoneuropathy)
• Hepatitis (B,C)• HIV
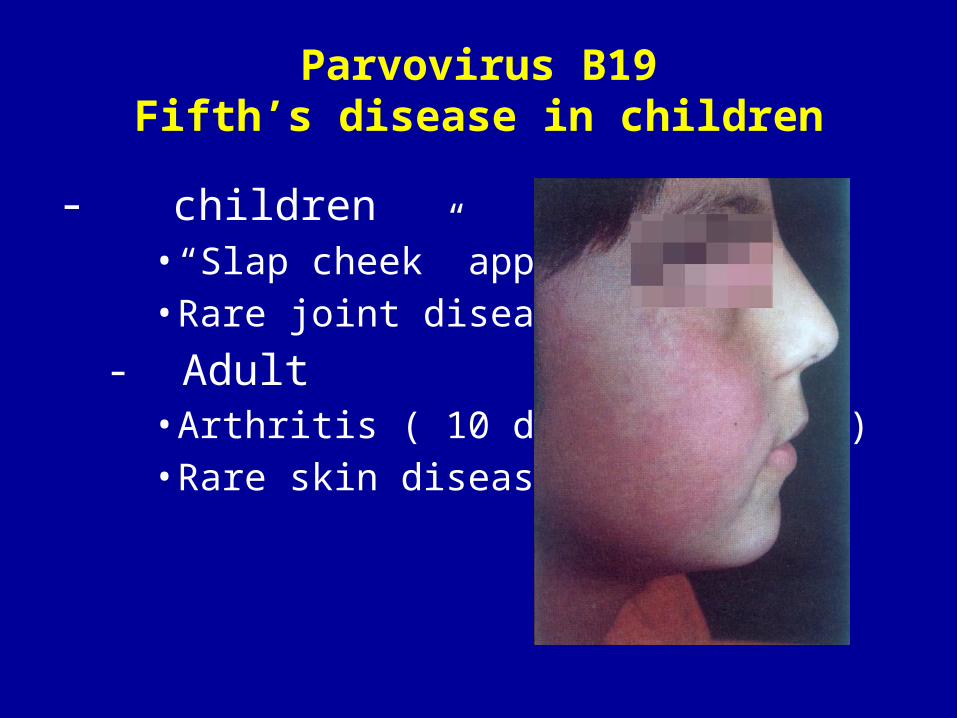
Parvovirus B19Fifth’s disease in children
- children• “Slap cheek” appearance• Rare joint disease-
- Adult• Arthritis ( 10 days to 1 month)• Rare skin disease
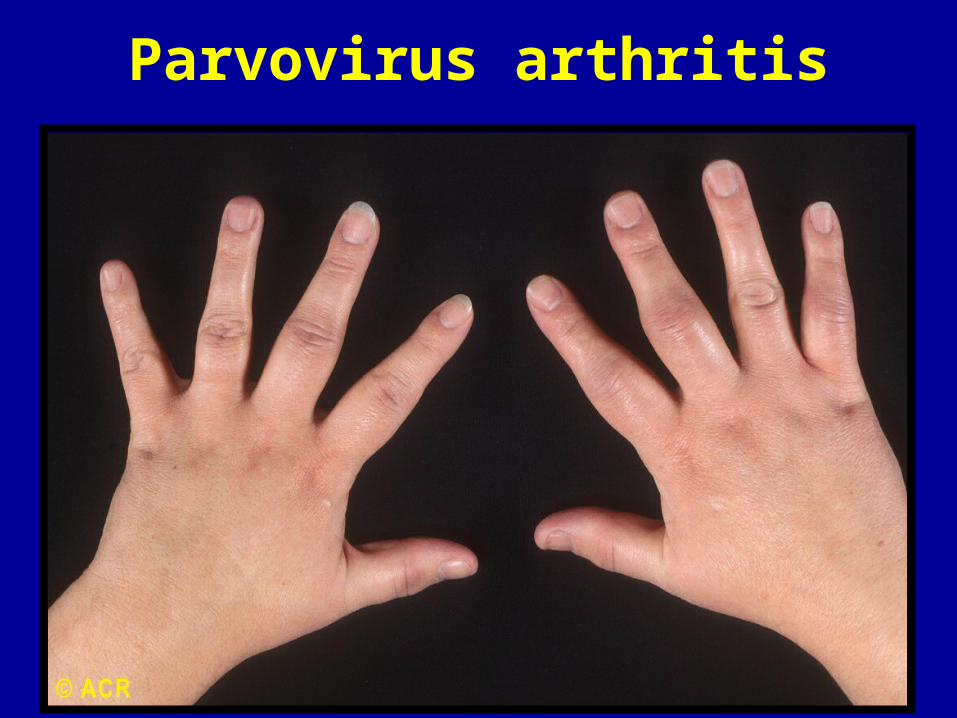
Parvovirus arthritis
treatment
• Symptomatic• Chronic IVIG































