Embed Size (px)
Citation preview
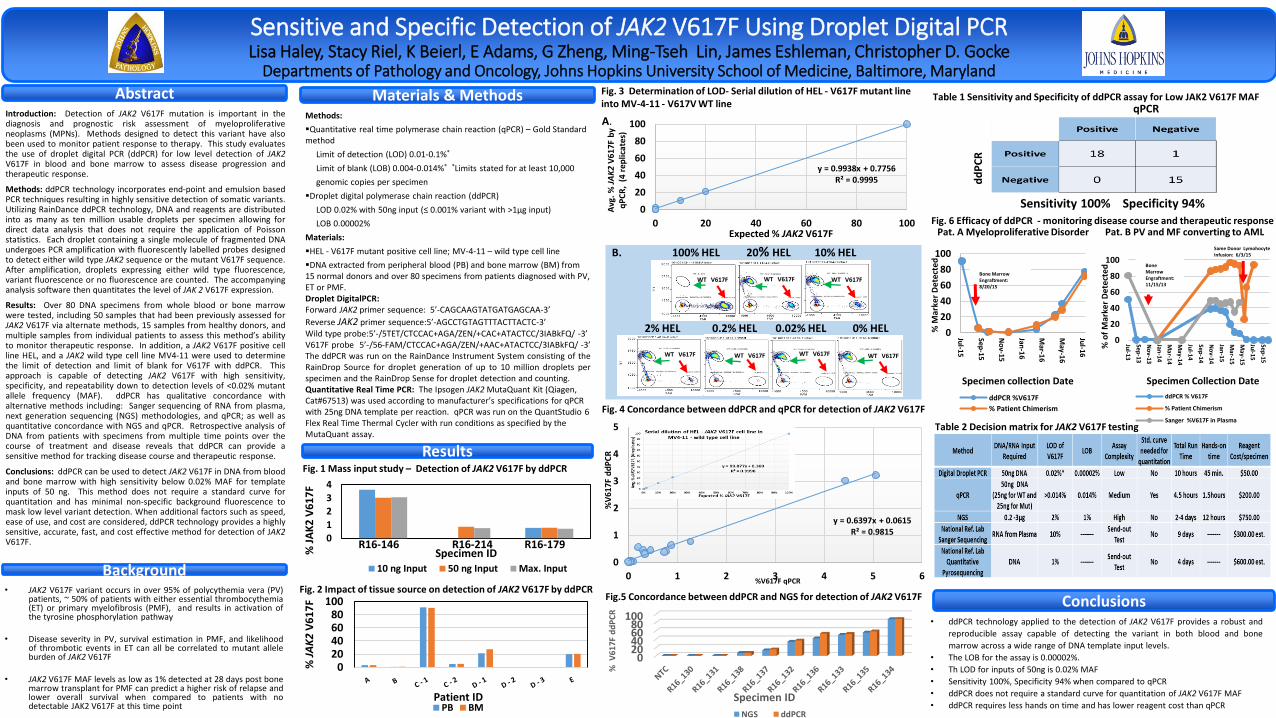
Sensitive and Specific Detection of JAK2 V617F Using Droplet Digital PCR Lisa Haley, Stacy Riel, K Beierl, E Adams, G Zheng, Ming-Tseh Lin, James Eshleman, Christopher D. Gocke
Departments of Pathology and Oncology, Johns Hopkins University School of Medicine, Baltimore, Maryland
Background
Abstract
Results
Materials & MethodsMethods:
Quantitative real time polymerase chain reaction (qPCR) – Gold Standard method
Limit of detection (LOD) 0.01-0.1%*
Limit of blank (LOB) 0.004-0.014%* *Limits stated for at least 10,000
genomic copies per specimen
Droplet digital polymerase chain reaction (ddPCR)
LOD 0.02% with 50ng input (≤ 0.001% variant with >1µg input)
LOB 0.00002%
Materials:
HEL - V617F mutant positive cell line; MV-4-11 – wild type cell line
DNA extracted from peripheral blood (PB) and bone marrow (BM) from 15 normal donors and over 80 specimens from patients diagnosed with PV, ET or PMF. Droplet DigitalPCR: Forward JAK2 primer sequence: 5’-CAGCAAGTATGATGAGCAA-3’
Reverse JAK2 primer sequence:5’-AGCCTGTAGTTTACTTACTC-3’Wild type probe:5’-/5TET/CTCCAC+AGA/ZEN/+CAC+ATACTCC/3IABkFQ/ -3’V617F probe 5’-/56-FAM/CTCCAC+AGA/ZEN/+AAC+ATACTCC/3IABkFQ/ -3’The ddPCR was run on the RainDance Instrument System consisting of theRainDrop Source for droplet generation of up to 10 million droplets perspecimen and the RainDrop Sense for droplet detection and counting.Quantitative Real Time PCR: The Ipsogen JAK2 MutaQuant Kit (Qiagen, Cat#67513) was used according to manufacturer’s specifications for qPCR with 25ng DNA template per reaction. qPCR was run on the QuantStudio 6 Flex Real Time Thermal Cycler with run conditions as specified by the MutaQuant assay.
Fig. 3 Determination of LOD- Serial dilution of HEL - V617F mutant line into MV-4-11 - V617V WT line
Fig.5 Concordance between ddPCR and NGS for detection of JAK2 V617F
Fig. 4 Concordance between ddPCR and qPCR for detection of JAK2 V617F
Conclusions
Table 1 Sensitivity and Specificity of ddPCR assay for Low JAK2 V617F MAF
Sensitivity 100% Specificity 94%
qPCR
dd
PC
R
Table 2 Decision matrix for JAK2 V617F testing
Fig. 6 Efficacy of ddPCR - monitoring disease course and therapeutic response
• ddPCR technology applied to the detection of JAK2 V617F provides a robust and
reproducible assay capable of detecting the variant in both blood and bone
marrow across a wide range of DNA template input levels.
• The LOB for the assay is 0.00002%.
• Th LOD for inputs of 50ng is 0.02% MAF
• Sensitivity 100%, Specificity 94% when compared to qPCR
• ddPCR does not require a standard curve for quantitation of JAK2 V617F MAF
• ddPCR requires less hands on time and has lower reagent cost than qPCR
Introduction: Detection of JAK2 V617F mutation is important in thediagnosis and prognostic risk assessment of myeloproliferativeneoplasms (MPNs). Methods designed to detect this variant have alsobeen used to monitor patient response to therapy. This study evaluatesthe use of droplet digital PCR (ddPCR) for low level detection of JAK2V617F in blood and bone marrow to assess disease progression andtherapeutic response.
Methods: ddPCR technology incorporates end-point and emulsion basedPCR techniques resulting in highly sensitive detection of somatic variants.Utilizing RainDance ddPCR technology, DNA and reagents are distributedinto as many as ten million usable droplets per specimen allowing fordirect data analysis that does not require the application of Poissonstatistics. Each droplet containing a single molecule of fragmented DNAundergoes PCR amplification with fluorescently labelled probes designedto detect either wild type JAK2 sequence or the mutant V617F sequence.After amplification, droplets expressing either wild type fluorescence,variant fluorescence or no fluorescence are counted. The accompanyinganalysis software then quantitates the level of JAK 2 V617F expression.
Results: Over 80 DNA specimens from whole blood or bone marrowwere tested, including 50 samples that had been previously assessed forJAK2 V617F via alternate methods, 15 samples from healthy donors, andmultiple samples from individual patients to assess this method’s abilityto monitor therapeutic response. In addition, a JAK2 V617F positive cellline HEL, and a JAK2 wild type cell line MV4-11 were used to determinethe limit of detection and limit of blank for V617F with ddPCR. Thisapproach is capable of detecting JAK2 V617F with high sensitivity,specificity, and repeatability down to detection levels of <0.02% mutantallele frequency (MAF). ddPCR has qualitative concordance withalternative methods including: Sanger sequencing of RNA from plasma,next generation sequencing (NGS) methodologies, and qPCR; as well asquantitative concordance with NGS and qPCR. Retrospective analysis ofDNA from patients with specimens from multiple time points over thecourse of treatment and disease reveals that ddPCR can provide asensitive method for tracking disease course and therapeutic response.
Conclusions: ddPCR can be used to detect JAK2 V617F in DNA from bloodand bone marrow with high sensitivity below 0.02% MAF for templateinputs of 50 ng. This method does not require a standard curve forquantitation and has minimal non-specific background fluorescence tomask low level variant detection. When additional factors such as speed,ease of use, and cost are considered, ddPCR technology provides a highlysensitive, accurate, fast, and cost effective method for detection of JAK2V617F.
• JAK2 V617F variant occurs in over 95% of polycythemia vera (PV)patients, ~ 50% of patients with either essential thrombocythemia(ET) or primary myelofibrosis (PMF), and results in activation ofthe tyrosine phosphorylation pathway
• Disease severity in PV, survival estimation in PMF, and likelihoodof thrombotic events in ET can all be correlated to mutant alleleburden of JAK2 V617F
• JAK2 V617F MAF levels as low as 1% detected at 28 days post bonemarrow transplant for PMF can predict a higher risk of relapse andlower overall survival when compared to patients with nodetectable JAK2 V617F at this time point
Fig. 1 Mass input study – Detection of JAK2 V617F by ddPCR
0
1
2
3
4
% J
AK
2 V
61
7F
Specimen ID10 ng Input 50 ng Input Max. Input
R16-146 R16-214 R16-179
Fig. 2 Impact of tissue source on detection of JAK2 V617F by ddPCR
020406080
100
% J
AK
2 V
61
7F
Patient IDPB BM
y = 0.9938x + 0.7756R² = 0.9995
0
20
40
60
80
100
0 20 40 60 80 100
Avg
. %
JA
K2
V6
17
F b
y q
PC
R,
(4 r
ep
licat
es)
Expected % JAK2 V617F
A.
B. 100% HEL 20% HEL 10% HEL
2% HEL 0.2% HEL 0.02% HEL 0% HEL
WT V617F WT V617F WT V617F
WT V617F WT V617F WT V617F WT V617F
y = 0.6397x + 0.0615R² = 0.9815
0
1
2
3
4
5
0 1 2 3 4 5 6
%V
617F
dd
PC
R
%V617F qPCR
020406080
100%
V61
7F d
dP
CR
Specimen ID
NGS ddPCR
Pat. A Myeloproliferative Disorder Pat. B PV and MF converting to AML
0
20
40
60
80
100
Jul-15
Sep-15
No
v-15
Jan-1
6
Mar-1
6
May-1
6
Jul-16
% M
arke
r D
ete
cted
Specimen collection Date
ddPCR %V617F
% Patient Chimerism
0
20
40
60
80
100
Jul-13
Sep
-13
No
v-13
Jan-14
Mar-14
May-14
Jul-14
Sep
-14
No
v-14
Jan-15
Mar-15
May-15
Jul-15
Sep
-15
% o
f M
arke
r D
ete
cted
Specimen Collection Date
ddPCR % V617F
% Patient Chimerism
Sanger %V617F in Plasma
Bone Marrow Engraftment: 8/20/15
Bone Marrow Engraftment: 11/15/13
Same Donor LymohocyteInfusion: 6/3/15





























