Embed Size (px)
Citation preview
Occupational Medicine 2014;64:417–420Advance Access publication 2 July 2014 doi:10.1093/occmed/kqu098
© The Author 2014. Published by Oxford University Press on behalf of the Society of Occupational Medicine. All rights reserved. For Permissions, please email: [email protected]
Self-reported and employer-recorded sickness absence in doctors
I. J. Murphy
Occupational Health Service, Nottingham University Hospitals NHS Trust, City Hospital Campus, Hucknall Road, Nottingham NG5 1PB, UK.
Correspondence to: I. J. Murphy, Occupational Health Service, Nottingham University Hospitals NHS Trust, City Hospital Campus, Hucknall Road, Nottingham NG5 1PB, UK. Tel: +44 (0)115 962 7646; e-mail: [email protected]
Background Doctors’ sickness absence reduces the quality and continuity of patient care and is financially costly. Doctors have lower rates of sickness absence than other healthcare workers.
Aims To compare self-reported with recorded sickness absence in doctors in a UK National Health Service hospital trust.
Methods A retrospective questionnaire study. The main outcome measures were self-reported and trust-recorded sickness absence episodes of 4 days or more in two consecutive 6-month periods.
Results The response rate was 82% (607/736). Self-reported sickness absence rates were 1.2% compared with a rate of 0.6% from trust-recorded data. There were 38 matched pairs of self-reported (mean duration: 18 days, standard deviation: 22 days) and trust-recorded (mean duration: 10 days, stand-ard deviation: 17 days) sickness absence episodes of 4 days or more in the 12 months studied. A matched pairs t-test determined that the difference between the two means was significant (t = 2.57, P < 0.05).
Conclusions Doctors’ sickness absence was significantly under-recorded in this study population.
Key words Doctors; doctors’ health; NHS; recorded; self-reported; sickness absence; sick leave.
Introduction
Sickness absence has been defined as absence from work attributed to illness or disease by the employee and accepted as such by the employer [1]. Sickness absence in UK National Health Service (NHS) doctors reduces the quality and continuity of patient care and is finan-cially costly [1–3]. In 1999, the UK government con-cluded that reducing sickness absence in the NHS would improve service delivery [4]. Doctors have less sickness absence than other healthcare workers [2,5–17]. There is good evidence for an inverse association between sickness absence and employment grade; the higher the grade the lower the rate of sickness absence [18]. Doctors may genuinely have less sickness absence than other occupational groups, or their sickness absence may be unreported or unrecorded. Doctors may not be asked to provide sickness certification or may be unaware of the requirement to do so. This study aimed to compare trust-recorded with self-reported sickness absence in doctors in a UK NHS hospital trust.
Methods
The study was undertaken at a large NHS acute district general hospital trust in the south of England in 2000 and 2001. At the time, the trust employed around 3500 staff and had 750 beds on two separate sites. There were 365 doctors (305 whole-time equivalents) employed on 21 September 2000 and 371 (311 whole-time equiva-lents) on 1 March 2001. Of the 365 doctors employed on 21 September 2000, 230 (63%) were male and the mean age was 40 (range: 23–67). The largest special-ties were anaesthetics (42 doctors), paediatrics (30) and obstetrics and gynaecology (29), and smallest were clini-cal biochemistry, microbiology, psychiatry and plastic surgery with only one doctor each. There were 12 differ-ent grades of doctor, the largest groups being consultants (114), senior house officers (74) and specialist registrars (54). The gender, age and grade profiles of the doctors employed on both dates were almost identical.
at University of G
uelph on August 21, 2014
http://occmed.oxfordjournals.org/
Dow
nloaded from

418 OCCUPATIONAl MEDICINE
A questionnaire was designed, piloted and modified before being posted with a covering letter to every doctor employed by the trust at the end of September 2000 and again at the beginning of March 2001. Non-responders were sent reminders after 2 and 4 weeks. Doctors were asked to provide their name and sickness absence taken (numbers of days and episodes and duration of each episode) in the previous 6 months (study period one: 1 March to 31 August 2000 and study period two: 1 September 2000 to 28 February 2001). Those employed <6 months at the trust were asked to provide details only of sickness absence during current employment. Doctors were also asked to rank their own health on a four-point scale (excellent, good, average or poor) and whether they would take sick leave given a particular scenario (‘If you had been up in the night with three episodes of vomiting and then developed diarrhoea at 7 a.m., would you take the day off work?’, with four possible responses: definitely yes, probably, possibly, definitely not). Finally, there was a space for comments. The questionnaire is available as Supplementary data at Occupational Medicine Online.
Trust-recorded sickness absence for all doctors elig-ible to participate in the study was obtained from records held by the payroll department (self-certificates and gen-eral practitioner certificates). The trust’s sickness absence policy [19] required a self-certificate for sickness absence lasting from 4 to 7 days (including Saturday, Sunday and public holidays), and a doctor’s certificate for sickness absence lasting >7 calendar days. For each certificated absence, the start and end date and the duration in cal-endar days were recorded by payroll on computer.
Data were analysed using Microsoft Excel. Pairs of self-reported and trust-recorded sickness absence epi-sodes of 4 days or more (ensuring a comparison of like with like) were matched for individual doctors, where such episodes of sick leave were identified from either self-reported or trust-recorded data. A matched pairs t-test was used to determine the significance of the dif-ference between the two means.
Permission to undertake the study was obtained from the trust, and ethical approval was obtained from the local research ethics committee.
Results
The response rate was 83% (304/365) for the first 6-month study period and 82% (303/371) for the second period. The overall response rate was 82% (607/736). The mean age of responders for both study periods was 41, and 61% were male. The mean age of non-respond-ers was 35, and 72% were male. One hundred and forty-eight doctors (24%) said they had taken sickness absence during the previous 6 months, with 125 reporting one episode, 21 reporting two, one reporting three and one four episodes. Overall doctors reported 174 episodes (mean duration: 5 days, range: 1–90 days) and 916 days
of sickness absence over both 6-month study periods. Thirty-four (20%) episodes lasted 4 days or more and totalled 689 (75%) days. The sickness absence rate based on self-reported data was 1.2% (916/76 700 calendar days of contracted time during the 12-month study period for the 607 responders to either questionnaire).
Trust-recorded sickness absence for all doctors eli-gible to participate in the study included responders and non-responders to the questionnaire. Thirty-seven (5%) doctors had at least one recorded episode during the two 6-month study periods and 28 were respond-ers to the questionnaire. Of the 28 responders, 24 had one recorded episode and 4 had two recorded episodes. Overall there were 32 episodes (mean duration: 12 days, range: 1–81 days) and 391 days of trust-recorded sick-ness absence over both 6-month study periods. Nineteen (59%) of these episodes lasted 4 days or more and totalled 375 (96%) days. The sickness absence rate based on trust-recorded data was 0.6% (558/94 070 calendar days of contracted time during the 12-month study period for all doctors employed by the trust on 21 September 2000 and 1 March 2001). The numerator (558 days) was the total days of all trust-recorded sickness absence from 1 March 2000 to 28 February 2001, including 167 days of recorded sickness absence in 9 doctors who were among the 129 non-responders to the questionnaire.
Thirty-eight matched pairs of self-reported (mean duration: 18 days, standard deviation: 22 days) and trust-recorded (mean duration: 10 days, standard devi-ation: 17 days) sickness absence episodes of 4 days or more were identified. This included absence episodes for four doctors who had trust-recorded episodes but who reported no absence. The difference between the two means was significant using an alpha level of 0.05 (t = 2.57, P < 0.05).
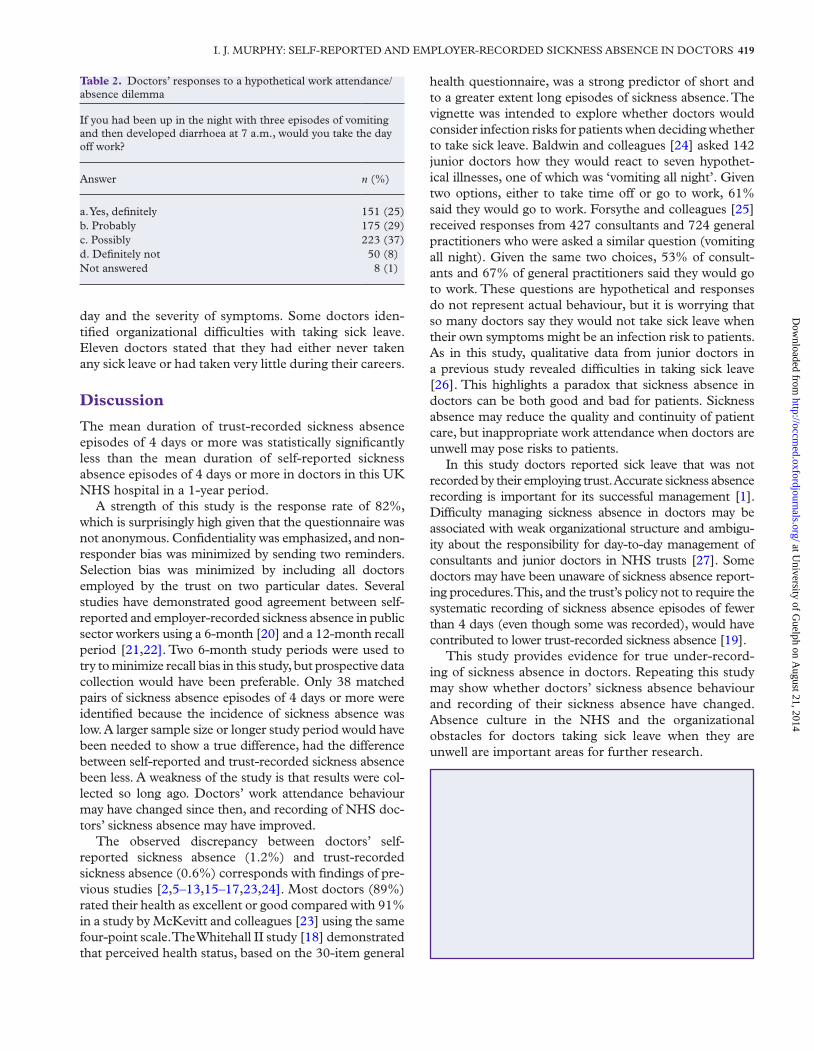
Most doctors (89%) rated their health as excellent or good. Five (1%) rated their health as poor (Table 1). A quarter (151) of responders said they would definitely take the day off after a night of diarrhoea and vomit-ing, whilst 8% (50) said they would definitely not do so (Table 2). Many added comments to explain that taking sick leave would depend on clinical commitments that
Table 1. Doctors’ self-rated health
How would you rank your own health on a four point scale—excellent, good, average or poor?’
Response n (%)
Excellent 273 (45)Good 265 (44)Average 58 (9)Poor 5 (1)Not answered 6 (1)Total 607 (100)
at University of G
uelph on August 21, 2014
http://occmed.oxfordjournals.org/
Dow
nloaded from
I. J. MURPHy: SElF-REPORTED AND EMPlOyER-RECORDED SICKNESS ABSENCE IN DOCTORS 419
day and the severity of symptoms. Some doctors iden-tified organizational difficulties with taking sick leave. Eleven doctors stated that they had either never taken any sick leave or had taken very little during their careers.
Discussion
The mean duration of trust-recorded sickness absence episodes of 4 days or more was statistically significantly less than the mean duration of self-reported sickness absence episodes of 4 days or more in doctors in this UK NHS hospital in a 1-year period.
A strength of this study is the response rate of 82%, which is surprisingly high given that the questionnaire was not anonymous. Confidentiality was emphasized, and non-responder bias was minimized by sending two reminders. Selection bias was minimized by including all doctors employed by the trust on two particular dates. Several studies have demonstrated good agreement between self-reported and employer-recorded sickness absence in public sector workers using a 6-month [20] and a 12-month recall period [21,22]. Two 6-month study periods were used to try to minimize recall bias in this study, but prospective data collection would have been preferable. Only 38 matched pairs of sickness absence episodes of 4 days or more were identified because the incidence of sickness absence was low. A larger sample size or longer study period would have been needed to show a true difference, had the difference between self-reported and trust-recorded sickness absence been less. A weakness of the study is that results were col-lected so long ago. Doctors’ work attendance behaviour may have changed since then, and recording of NHS doc-tors’ sickness absence may have improved.
The observed discrepancy between doctors’ self-reported sickness absence (1.2%) and trust-recorded sickness absence (0.6%) corresponds with findings of pre-vious studies [2,5–13,15–17,23,24]. Most doctors (89%) rated their health as excellent or good compared with 91% in a study by McKevitt and colleagues [23] using the same four-point scale. The Whitehall II study [18] demonstrated that perceived health status, based on the 30-item general
health questionnaire, was a strong predictor of short and to a greater extent long episodes of sickness absence. The vignette was intended to explore whether doctors would consider infection risks for patients when deciding whether to take sick leave. Baldwin and colleagues [24] asked 142 junior doctors how they would react to seven hypothet-ical illnesses, one of which was ‘vomiting all night’. Given two options, either to take time off or go to work, 61% said they would go to work. Forsythe and colleagues [25] received responses from 427 consultants and 724 general practitioners who were asked a similar question (vomiting all night). Given the same two choices, 53% of consult-ants and 67% of general practitioners said they would go to work. These questions are hypothetical and responses do not represent actual behaviour, but it is worrying that so many doctors say they would not take sick leave when their own symptoms might be an infection risk to patients. As in this study, qualitative data from junior doctors in a previous study revealed difficulties in taking sick leave [26]. This highlights a paradox that sickness absence in doctors can be both good and bad for patients. Sickness absence may reduce the quality and continuity of patient care, but inappropriate work attendance when doctors are unwell may pose risks to patients.
In this study doctors reported sick leave that was not recorded by their employing trust. Accurate sickness absence recording is important for its successful management [1]. Difficulty managing sickness absence in doctors may be associated with weak organizational structure and ambigu-ity about the responsibility for day-to-day management of consultants and junior doctors in NHS trusts [27]. Some doctors may have been unaware of sickness absence report-ing procedures. This, and the trust’s policy not to require the systematic recording of sickness absence episodes of fewer than 4 days (even though some was recorded), would have contributed to lower trust-recorded sickness absence [19].
This study provides evidence for true under-record-ing of sickness absence in doctors. Repeating this study may show whether doctors’ sickness absence behaviour and recording of their sickness absence have changed. Absence culture in the NHS and the organizational obstacles for doctors taking sick leave when they are unwell are important areas for further research.
Key points
• Doctors’ self-reported sickness absence was signif-icantly higher than that recorded by their employ-ing trust, suggesting that trusts under-record doctors’ sick leave.
• Most doctors rated their own health as excellent or good.
• A worrying proportion of doctors said they would not take sick leave even when their health may pose risks to patients.
Table 2. Doctors’ responses to a hypothetical work attendance/absence dilemma
If you had been up in the night with three episodes of vomiting and then developed diarrhoea at 7 a.m., would you take the day off work?
Answer n (%)
a. yes, definitely 151 (25)b. Probably 175 (29)c. Possibly 223 (37)d. Definitely not 50 (8)Not answered 8 (1)
at University of G
uelph on August 21, 2014
http://occmed.oxfordjournals.org/
Dow
nloaded from

420 OCCUPATIONAl MEDICINE
Funding
The work was supported by the Royal Berkshire and Battle Hospitals National Health Service Trust’s occupational health service. No external funding or grant was received.
Conflicts of interest
None declared.
References
1. Whitaker SC. The management of sickness absence. Occup Environ Med 2001;58:420–424
2. Seccombe I, Patch A. Health at Work in the NHS: Key Indicators. Institute for Employment Studies Final Report, 1994
3. Wright ME. long-term sickness absence in an NHS teach-ing hospital. Occup Med (Lond) 1997;47:401–406.
4. Department of Health. Working Together. Securing a Quality Workforce for the NHS. london, UK: Department of Health, 1998.
5. McKeown KD, Furness JA. Sickness absence patterns of 5000 NHS staff employed within Northallerton and South West Durham Health Authorities. J Soc Occup Med 1987;37:111–116.
6. Verow P, Hargreaves C. Healthy workplace indicators: cost-ing reasons for sickness absence within the UK National Health Service. Occup Med (Lond) 2000;50:251–257.
7. Kivimäki M, Sutinen R, Elovainio M et al. Sickness absence in hospital physicians: 2 year follow up study on determi-nants. Occup Environ Med 2001;58:361–366.
8. Mann KJ, Abramson JH, Camrass I, Alon J. Sickness absenteeism in a hospital in Israel. Hospital 1971; Sept: 307–311.
9. Pines A, Skulkeo K, Pollak E, Peritz E, Steif J. Rates of sick-ness absenteeism among employees of a modern hospital: the role of demographic and occupational factors. Br J Ind Med 1985;42:326–335.
10. Bamgboye EA, Adeleye AI. Sickness absenteeism in a Nigerian teaching hospital. East Afr Med J 1992;69:450–455.
11. Bamgboye EA, Olubuyide IO, al-Shammari S. The rate of sickness absenteeism among employees at King Khalid University Hospital, Riyadh, Saudi Arabia. East Afr Med J 1993;70:515–518.
12. al-Shammari SA, Bamgboye EA, Olubuyide IO. Sickness absenteeism among employees of a teaching hospital in Saudi Arabia. J R Soc Health 1994;114:6–10.
13. Ritchie KA, Macdonald EB, Gilmour WH, Murray KJ. Analysis of sickness absence among employees of four NHS trusts. Occup Environ Med 1999;56:702–708.
14. Mira JJ, Vitaller J, Buil JA, Aranaz JM, Herrero JF. Absenteeism as a symptom of occupational ill-health in hospitals and its repercussion on quality assurance. Qual Assur Health Care 1992;4:273–287.
15. Rees DW, Cooper Cl. Occupational stress in health ser-vice employees. Health Serv Manage Res 1990;3:163–172.
16. Hall AJ, Aw TC, Harrington JM. Morbidity survey of post mortem room staff. J Clin Pathol 1991;44:433–435.
17. Rees D, Cooper Cl. Occupational stress in health service workers in the UK. Stress Med 1992;8:79–90.
18. North F, Syme Sl, Feeney A, Head J, Shipley MJ, Marmot MG. Explaining socioeconomic differences in sickness absence: the Whitehall II Study. BMJ 1993;306:361–366.
19. Human Resources Procedure Managing Absence, 2nd edn. Reading, UK: Royal Berkshire and Battle Hospitals NHS Trust, August, 1999.
20. Rees D, Cooper Cl. Research note: reliability of self-report sickness absence data in the health service. Health Serv Manage Res 1993;6:140–141.
21. Ferrie JE, Kivimäki M, Head J, Shipley MJ, Vahtera J, Marmot MG. A comparison of self-reported sickness absence with absences recorded in employers’ registers: evidence from the Whitehall II study. Occup Environ Med 2005;62:74–79.
22. Voss M, Stark S, Alfredsson l, Vingård E, Josephson M. Comparisons of self-reported and register data on sick-ness absence among public employees in Sweden. Occup Environ Med 2008;65:61–67.
23. McKevitt C, Morgan M, Dundas R, Holland WW. Sickness absence and ‘working through’ illness: a com-parison of two professional groups. J Public Health Med 1997;19:295–300.
24. Baldwin PJ, Dodd M, Wrate RM. young doctors’ health—II. Health and health behaviour. Soc Sci Med 1997;45:41–44.
25. Forsythe M, Calnan M, Wall B. Doctors as patients: postal survey examining consultants and general practitioners adherence to guidelines. BMJ 1999;319:605–608.
26. Baldwin PJ, Dodd M, Wrate RM. Young Doctors: Work, Health and Welfare. A Class Cohort 1986–1996. london, UK: Department of Health, Research and Development Initiative on Mental Health of the NHS Workforce, 1997.
27. British Medical Association (Board of Science and Education). Stress and the Medical Profession. london: British Medical Association, 1992.
at University of G
uelph on August 21, 2014
http://occmed.oxfordjournals.org/
Dow
nloaded from








![Sickness Absence: a Pan-European Study[1] SICKNESS ABSENCE: A PAN-EUROPEAN STUDY 1. Introduction The incidence and the level of sickness absence in the workplace is an important labour](https://img.dokumen.tips/doc/110x75/5fa706b7ddba8073614af31e/sickness-absence-a-pan-european-study-1-sickness-absence-a-pan-european-study.jpg)










![[Academy Name] Management of Sickness Absence](https://img.dokumen.tips/doc/110x75/61f02422231170415e5c7e4a/academy-name-management-of-sickness-absence.jpg)








