Embed Size (px)
Citation preview

ORIGINAL PAPER
Self-compassion and Fear of Self-compassion: MechanismsUnderlying the Link between Child Maltreatment Severityand Psychological Distress in College Women
Terri L. Messman-Moore1& Prachi H. Bhuptani1
Published online: 17 April 2020# Springer Science+Business Media, LLC, part of Springer Nature 2020
AbstractObjectives Women are at increased risk for depression and anxiety associated with child maltreatment, given higher rates ofexposure to childhood maltreatment and a greater sensitivity resulting in maltreatment-related distress. Thus, there is a need toidentify mechanisms of resilience among female survivors of child maltreatment. Self-compassion may promote resilience,whereas fear of self-compassion may diminish this protective effect. Moreover, distinct facets of self-compassion (e.g., self-kindness) versus self-coldness (e.g., self-judgment) may differentially explain risk or resilience for child maltreatment outcomes.Methods College women (N = 586) completed anonymous online surveys assessing the severity of different types of childmaltreatment, self-compassion, fear of self-compassion, depression, anxiety, and stress.Results Severity of sexual, physical, and emotional abuse, and emotional and physical neglect, was positively associated withelevated fear of self-compassion and the absence of self-compassion (i.e., self-coldness). In contrast, emotional abuse and neglectseverity were the only maltreatment variables negatively associated with self-compassion. Models indicated an indirect relationbetween increased maltreatment severity and heightened psychological distress via fear of self-compassion and self-coldness(i.e., isolation, overidentification). Statistical patterns indicative of suppression among the positive facets of self-compassionoccurred.Conclusions The centrality of emotional maltreatment, along with fear of self-compassion, isolation, and overidentification,emerged across analyses. Findings suggest the absence of self-compassion (i.e., self-coldness) is associated with specific formsof distress. Additional research with child maltreatment survivors should examine self-compassion components rather than aunidimensional construct.
Keywords Child abuse . Child neglect . Self-compassion . Depression . Anxiety . Stress
A meta-analysis of longitudinal studies demonstrated thatexperiencing child maltreatment is associated with increasedrisk of depression and anxiety in adulthood, with the magnitudeof risk varying by maltreatment type (e.g., odds ratios rangedfrom 1.7 for neglect to 2.7 for sexual abuse) (Li et al. 2016).Maltreated individuals diagnosed with depressive or anxietydisorders have an earlier age of onset, greater symptom severity,more comorbidity, greater risk for suicide, and poorer treatmentresponse than non-maltreated individuals with the same
diagnoses (Teicher and Samson 2013). Exposure to childhoodmaltreatment and negative outcomes associated with it differaccording to the victim’s gender. In the NESARC study of34,653 US adults, women had significantly higher rates ofchildhood physical, sexual, and emotional abuse comparedwith men (Hartford et al. 2014). Research considering the co-existence of different types of childhood maltreatment indicateswomen experience higher rates of child emotional abuse, emo-tional neglect, and sexual abuse, and higher rates of physicalabuse in the context of emotional or sexual abuse comparedwith men (Rehan et al. 2017; Scher et al. 2004; Taillieu et al.2016). Thus, women are more likely than men to experiencemultiple types of child maltreatment, and also experiencehigher rates of most forms of child maltreatment in isolation.
Psychiatric correlates of child maltreatment also vary bygender, with women more sensitive to the negative impact
* Terri L. [email protected]
1 Department of Psychology, Miami University, Oxford, OH 45056,USA
Mindfulness (2020) 11:1446–1459https://doi.org/10.1007/s12671-020-01361-2
of childhood maltreatment. Among college students exposedto childhood maltreatment, a greater proportion of womenshow poor psychological adjustment compared with men(35.2% vs. 17.6%) (Maples et al. 2014). Moreover, amongadults reporting childhood sexual abuse, emotional neglect,and physical neglect, women are more likely than men to bediagnosed with clinically elevated levels of depression andanxiety (Rehan et al. 2019). There also is evidence that fe-males are negatively affected by less severe child maltreat-ment. Among female, compared with male, adolescents, childemotional maltreatment had a more severe negative impact onsymptoms of depression and anxiety at lower levels of abuseseverity (Hagborg et al. 2017). In sum, the threshold for dis-tress associated with child maltreatment is lower among ado-lescent females, as less severe levels of maltreatment are re-quired to trigger depression and anxiety. These findings indi-cate a need for additional research focused on factors thatexplain the impact of child maltreatment on women, givengender disparities in exposure to, and outcomes associatedwith, child maltreatment. Self-compassion may be such amechanism.
High levels of self-compassion are associated with lowerrates of depression, anxiety, and general stress (MacBeth andGumley 2012). Initial longitudinal studies suggest a bufferingeffect of self-compassion on depression, with improvement inself-compassion leading to decreases in depression (Kriegeret al. 2016). Diminished self-compassion as well as elevationsin shame and self-criticism explains higher rates of depres-sion, anxiety, and stress associated with child maltreatment(Naismith et al. 2019; Ross et al. 2019). Self-compassionmay be one mechanism that underlies resilience followingexposure to child maltreatment because it promotes effectiveemotion regulation among female survivors of interpersonalviolence (Scoglio et al. 2018), and mediates the link betweenchild maltreatment and emotion dysregulation (Reffi et al.2019). Moreover, lack of self-compassion explains the signif-icant association between child maltreatment and heightenedinternalized shame (Ross et al. 2019). Self-compassion is as-sociated with transdiagnostic mechanisms such as shame andself-criticism (MacBeth and Gumley 2012), which underlierisk for numerous psychiatric outcomes. Importantly, self-compassion is amenable to change (Fritz et al. 2018; Wilsonet al. 2019).
Self-compassion involves treating oneself with kindnessand encouragement, and the tendency to be warm, caring,and understanding in the face of personal difficulties (Lópezet al. 2018; Muris and Petrocchi 2017; Neff 2003). One of themost widely adopted definitions of self-compassion in theresearch literature was developed by Neff (2003), who con-ceptualized self-compassion as consisting of two core dimen-sions. These two dimensions reflect opposite poles that signifyeither the presence of self-compassion or its absence (e.g.,self-coldness). These opposite poles do not coexist within an
individual’s experience at any one point in time; rather self-compassion is experienced in the absence of self-coldness orvice versa, from moment to moment. For assessment, Neffoperationalized these bipolar dimensions into six separatefacets of self-compassion, three of which assess a compassion-ate approach to one’s suffering (i.e., self-kindness, commonhumanity, and mindfulness) and three of which assess a harshand critical attitude towards oneself (i.e., self-judgment, isola-tion, and overidentification). Self-kindness involves the ten-dency to be caring and understanding in the context of diffi-culties or failure, in contrast to self-criticism, self-condemna-tion, blaming, and rumination, which are associated with de-pression and other forms of psychopathology (Van Dam et al.2011). Common humanity reflects our ability to recognize ourstruggles as an inherently universal aspect of the human ex-perience, in contrast to feelings of isolation upon perceivingone’s struggles as unusual, abnormal, or uncommon. Finally,mindfulness is one aspect of self-compassion which involvesa stance of equanimity towards difficult and uncomfortableexperiences, rather than overidentifying with, or fixating up-on, such difficulties (Van Dam et al. 2011).
The buffering impact of self-compassion is argued to occurbecause its components (e.g., self-kindness) shift cognitivefactors associated with stress and anxiety, such as self-blameand rumination (Van Dam et al. 2011). Yet, research to dateprimarily focuses on an overarching self-compassion con-struct. The overarching concept of self-compassion is com-prised of the presence of positive self-compassion facets(e.g., self-kindness) and the absence of the negative facets(i.e., self-coldness). However, the measurement of self-compassion with the Self-Compassion Scale, an instrumentdeveloped by Neff (2003), uses reverse-scored self-coldnessitems, which may artificially inflate the negative associationbetween self-compassion and psychological distress. Moreresearch is needed to determine whether facets of self-compassion show this buffering effect. This is especially per-tinent given that self-coldness (i.e., self-judgment, isolation,and overidentification) shows stronger relations with distressthan positive self-compassion facets (e.g., self-kindness),which show weak or negligible associations with psychopa-thology (Körner et al. 2015; López et al. 2018).
The seeds of self-compassion are planted in early childrelationships with caregivers and attachment figures (Gilbertand Procter 2006; Ross et al. 2019). Because of this, self-compassion may be compromised among children who grewup in environments lacking adequate warmth and compassion.Indeed, diminished self-compassion is associated with criticalparents, familial dysfunction, and child maltreatment(Naismith et al. 2019; Vettese et al. 2011; Wu et al. 2018).Children who experience verbal or emotional abuse by par-ents, including being called names such as “stupid” or “bad,”appear especially vulnerable to developing self-criticism(Naismith et al. 2019; Sachs-Ericsson et al. 2006). Yet few
Mindfulness (2020) 11:1446–1459 1447

studies focus specifically on the association between childmaltreatment (abuse or neglect) and self-compassion. Moststudies that do examine this connection demonstrate that childmaltreatment is associated with decreased self-compassion(Miron et al. 2016; Ross et al. 2019; Tanaka et al. 2011;Vettese et al. 2011; Wu et al. 2018), and that such relationsare particularly pronounced for emotional abuse and emotion-al neglect. For example, in a study of 117 youth in foster care(Tanaka et al. 2011), self-compassion was significantly loweramong survivors of child physical and emotional abuse (andphysical and emotional neglect), although emotional abusewas the only type of maltreatment associated with self-compassion in multivariate models. In a sample of Chinesecollege students, only emotional maltreatment (abuse and ne-glect) was associated with self-compassion in a model thatincluded all forms of child maltreatment (Wu et al. 2018).Similarly, among female US college students, childhood emo-tional abuse, but not sexual or physical abuse, was associatedwith self-compassion (Miron et al. 2014). Together, thesestudies suggest emotional maltreatment has a more significantrole in development of self-compassion (or lack thereof) thanother types of maltreatment.
Several studies documenting an association between childmaltreatment and self-compassion focus on female collegestudents (Boykin et al. 2018; Miron et al. 2014; Miron et al.2016), linking child maltreatment, lower self-compassion, andnegative outcomes such as problematic alcohol use, posttrau-matic stress symptoms, and depression. Such findings suggestself-compassion may be a particularly appropriate target forwomen. Additional research is needed to focus on self-compassion among women, especially considering that fe-males (adolescents and women) report lower levels of self-compassion than males (Bluth et al. 2017; Yarnell et al.2015). Moreover, women are more likely to employ negativecognitive emotion strategies, such as self-blame, suppression,rumination, and catastrophizing (Nolen-Hoeksema and Aldao2011), that can be ameliorated by increasing self-compassion.
Fear of self-compassion is also relevant to distress amongchild maltreatment survivors. Even if survivors of maltreat-ment understand how to engage in self-compassion, there arebarriers to doing so. Collectively referred to as fear of self-compassion, such beliefs include thinking that self-compassion would make one weak or vulnerable to others,or that it would lower one’s standards and reveal one’s flawsor inadequacies, or that one is underserving of self-compas-sion. Experiences of child abuse and neglect contribute tosuch belief systems that interfere with the capacity for self-compassion, culminating in a fear of self-compassion (Gilbertet al. 2011). Factors that contribute to fear of self-compassioninclude increased sensitivity to threat, critical self-beliefs, andextensive shame (Gilbert and Procter 2006; Ross et al. 2019).Early interpersonal trauma (e.g., child abuse and neglect, pa-rental criticism, or peer bullying) is highly salient to
development of fears of rejection and internalized harsh criti-cism, as well as a feeling of being underserving of compassion(from others and the self). Such experiences may cultivate fearand a lack of perceived safety in abuse survivors, andcompassionate acts from others or towards the self maytrigger this sense of vulnerability. Gilbert and Procter (2006)noted, “…such individuals often come from neglectful or trau-matic backgrounds and have rarely felt safe or reassured.Indeed, we have found that feelings of warmth or gentle reas-surance were often frightening for them” (p. 355).
Importantly, fear of self-compassion is not synonymouswith self-coldness (e.g., self-criticism) or a lack of skill inself-compassion; it is a fearful reaction or avoidance of theprovision of self-compassion, due to the negative associationsdescribed earlier. Fear of self-compassion explains the associ-ation between child maltreatment and posttraumatic stress dis-order (PTSD) as well as depression (Boykin et al. 2018;Mironet al. 2016). Moreover, in models examining both self-compassion and fear of self-compassion, only fear of self-compassion was directly associated with child sexual abuse,and mediated the association between sexual abuse and dis-tress (depression and PTSD symptoms). Although both self-compassion and fear of self-compassion are associated withchild maltreatment, fear of self-compassion may show a stron-ger connection to psychopathology outcomes.
There is evidence that self-compassion is a mechanism thatexplains child maltreatment outcomes. Low levels of self-compassion explain the association of child maltreatmentand negative outcomes, including the link between juvenilevictimization (e.g., exposure to community violence andcrime, bullying, and child maltreatment) and psychologicaldistress (Játiva and Cerezo 2014), as well as between childmaltreatment and emotion dysregulation (Reffi et al. 2019;Vettese et al. 2011). More specifically, low self-compassionmediates the association between child emotional maltreat-ment (emotional abuse or neglect) and depressive symptomsin Chinese college students and adult community members inthe Southwestern United States (Ross et al. 2019; Wu et al.2018). Only two studies have examined the severity of childmaltreatment in relation to self-compassion (Tanaka et al.2011; Wu et al. 2018). However, a focus on severity is impor-tant given that abuse severity (versus presence) is one of thesingle best predictors of psychological distress such as PTSDand depression (Bifulco et al. 2002; Evans et al. 2013).
The overarching purpose of the current investigation was toexpand our understanding of self-compassion in relation tochild maltreatment. Assessment of maltreatment severity,rather than the presence of abuse, allows for a more nuancedunderstanding of the association between child maltreatmentand self-compassion. We hypothesized self-compassion, self-coldness, and fear of self-compassion would mediate the rela-tion between child maltreatment severity and distress.Specifically, we expected that increased severity of all types
1448 Mindfulness (2020) 11:1446–1459

of child maltreatment would be significantly associated withlower self-compassion, but that the strongest relations wouldemerge for emotional maltreatment (emotional abuse and ne-glect). We hypothesized that child maltreatment severitywould be positively associated with self-coldness (i.e., nega-tive components of self-compassion: self-judgment, isolation,and overidentification) and fear of self-compassion.
Method
Participants
Participants were 586 female undergraduates at a mid-sizedpublic university in the Midwestern United States, ages 17–26(mean age = 18.71, SD = 0.97). The vast majority wereCaucasian (85.5%), with an additional 10.4% Asian, 4.9%Black, 1.9% biracial, and 0.9% Pacific Islander; 5.5% identi-fied as Latina/Hispanic. The majority were from upper-middleclass households based upon reported family household in-comes. We recruited female college students for the studyfor several reasons. First, women are more likely than mento be exposed to multiple forms of child maltreatment (Rehanet al. 2017; Taillieu et al. 2016), as well as specific forms ofmaltreatment previously correlated with self-compassion(e.g., Tanaka et al. 2011; Wu et al. 2018), such as emotionaland sexual abuse (Hagborg et al. 2017; Rehan et al. 2019).Second, women and female adolescents show an increasedrisk for anxiety and depression, including major depressivedisorder, compared with males (Merikangas et al. 2010), andreport lower levels of self-compassion than males (Bluth et al.2017; Yarnell et al. 2015).
Procedures
Participants were recruited from a research participant pool(for Introduction to Psychology), and earned research creditfor study completion. Informed consent was obtained from allparticipants included in the study. All participants met in thelaboratory for informed consent/study instructions, but com-pleted the online surveys outside the laboratory. Participantdata were tracked with a unique identification number. Noadverse effects were reported.
Measures
Child Maltreatment The Childhood Trauma Questionnaire(CTQ), a 28-item questionnaire, was used to assess five typesof child maltreatment severity: sexual abuse, physical abuse,emotional abuse, physical neglect, and emotional neglect(Bernstein and Fink 1998). Each subscale is comprised of fiveitems with responses ranging from 1 (never true) to 5 (veryoften true); severity was measured with the continuous sum
score. Example items include the following: “Someone triedto touch me in a sexual way, or tried to make me touch them”(sexual abuse), “People in my family called me things like“stupid,” “lazy” or “ugly”” (emotional abuse), “People inmy family hit me so hard that it left me with bruises or marks”(physical abuse), “There was someone in my family whohelped me feel important or special” (emotional neglect, re-verse scored), and “I had to wear dirty clothes” (physical ne-glect). The CTQ is a widely used screener for child maltreat-ment, but does not specifically assess abusive acts.Comparisons of the CTQ and behaviorally derived assessmentshowed high levels of agreement (92.4% for sexual abuse and80% for physical abuse), although the CTQ identified higherrates of sexual abuse and lower rates of physical abuse com-pared with a computer-administered interview that assessedchild maltreatment (DiLillo et al. 2010). In the current study,subscales generally demonstrated good internal consistency;Cronbach’s alpha ranged from .80 to .92, with the exception ofphysical neglect (Cronbach’s alpha = .56), similar to that re-ported byWu et al. (2018). Three items, not used in the currentstudy, may assess response styles reflecting minimization.
Self-compassion Self-compassion was assessed with the Self-Compassion Scale, a 28-item questionnaire with six subscaleswhich assesses self-compassion (self-kindness, commonhumanity, and mindfulness) and self-coldness (self-judgment, isolation, and overidentification) (Neff 2003).Example items include “I try to be loving towards myselfwhen I’m feeling emotional pain” (self-kindness), or “WhenI’m feeling down I tend to obsess and fixate on everythingthat’s wrong” (overidentification). Response options on Likertscale range from 1 (almost never) to 5 (almost always).Subscale scores were computed by calculating the mean ofsubscale item responses. The SCS has good reliability andvalidity (Neff 2003). In the current sample, internal consisten-cy Cronbach’s alpha for subscales were good, and rangedfrom .82 to .87.
Fear of Self-compassion Fear of self-compassion was assessedwith the Fear of Compassion Scales-Self-Compassion (FSC-SC), a 15-item questionnaire (Gilbert et al. 2011). Exampleitems include “I feel that I don’t deserve to be kind and for-giving to myself,” or “I fear that if I am more self-compassionate I will become a weak person.” Responses areon a Likert scale, indicating degree of agreement with eachstatement on a scale ranging from 0 (“do not agree at all”) to 4(“completely agree”). Higher scores indicate greater fear ofself-compassion. Internal consistency in the current samplewas good (Cronbach’s alpha = .95).
Psychological Distress Depression, anxiety, and stress wereassessed with three subscales of the DASS-21, a 21-item sur-vey (Lovibond and Lovibond 1995). Example items include
Mindfulness (2020) 11:1446–1459 1449
“I felt that I had nothing to look forward to” (depression), “Ifelt scared without any good reason” (anxiety), and “I tendedto overreact to situations” (stress). Each subscale is comprisedof seven items, with responses rated on a 4-point Likert scaleranging from 0 (“did not apply all”) to 3 (“applied to me verymuch, ormost of the time”) with a focus on the previousweek.Higher scores are indicative of greater distress. In the currentstudy, internal consistency was good for each of the subscales,with Cronbach’s alpha ranging from .83 (anxiety) to .90 (de-pression). Above-threshold scores on the DASS-21 are asso-ciated with corresponding DSM-5 diagnostic conditions incollege students (Bravo et al. 2018).
Results
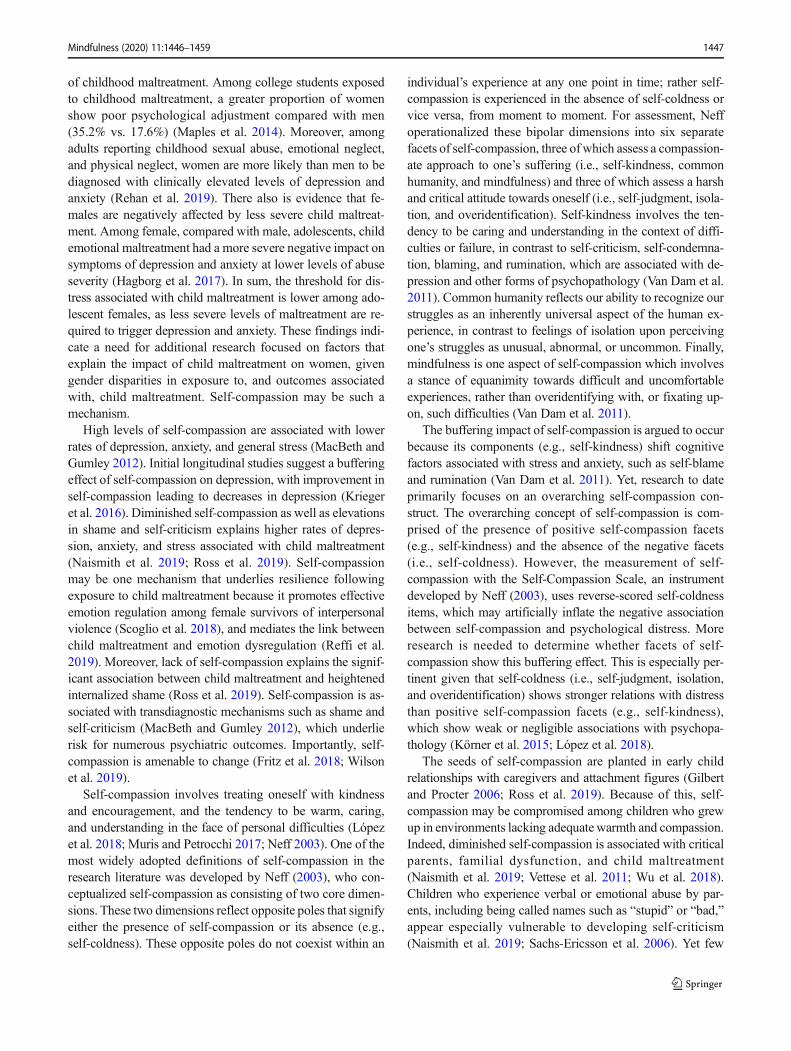
Data were examined for normality, completeness, and thepresence of outliers or impossible values. Bivariate correla-tions were computed to examine general patterns of associ-ation. Path analysis using the maximum likelihood estima-tion method in MPlus version 7.3 tested five distinct paral-lel mediation models, one for each childhood maltreatmenttype. Given the overlap between the distinct forms of psy-chological distress, error variances for the three dependentvariables (depression, anxiety, and stress) were correlated.Similarly, the error variances for the mediators were corre-lated as they shared overlap. We tested the hypothesizedindirect effect of facets of self-compassion, self-coldness,and fear of self-compassion, in addition to focusing on
individual pathways, consistent with current recommenda-tions (e.g., Hayes 2013). Specifically, we tested the overallindirect effect for each model (e.g., child emotional abuseseverity → facets of self-compassion, self-coldness, and fearof self-compassion → depression, anxiety, and stress) andused bootstrapping techniques to construct confidence inter-vals around the indirect effects (Hayes 2013; Preacher andHayes 2004) (see Fig. 1). Path analysis in MPlus allows formultiple simultaneous parallel mediators in the same modeland provides magnitude as well as significance of the indi-rect effect via each mediator. Missing Value Analysis(MVA) in SPSS revealed missing values ranging from 0.2to 1% across key study variables. Little’s MCAR test (Little1988) indicated that data were not significantly differentfrom the missing completely at random pattern (χ2 (11) =6.05, p = .53). Based on guidelines to manage less than 2%missing data, single imputation was used (Widaman 2006).
Bivariate Associations
As hypothesized, all forms of child maltreatment severitywere associated positively with psychological distress (i.e.,depression, anxiety, stress) and fear of self-compassion (seeTable 1). Only certain types of maltreatment severity wereassociated with self-compassion. Child emotional maltreat-ment severity (emotional abuse and emotional neglect)showed the strongest correlations to SCS subscales.Emotional abuse and neglect severity and physical abuse se-verity were positively associated with self-coldness (e.g.,
Fig. 1 Overarching model to test indirect effects of self-compassion facets and fear of self-compassion as mediators of the link between childmaltreatment severity and psychological distress. Five independent models were were conducted, one for each type of maltreatment
1450 Mindfulness (2020) 11:1446–1459

Table1
Bivariatecorrelations
EA
EN
PAPN
SA
SK
CH
MD
SJIS
OI
FSC
Depression
Anxiety
Stress
EA
-.62***
.53***
.43***
.27***
−.13**
−.02
−.07
.29***
.31***
.29***
.39***
.38***
.36***
.38***
EN
--
.47***
.59***
.24***
−.20***
−.13**
−.13**
.18***
.21***
.16***
.40***
.34***
.29***
.26***
PA-
--
.49***
.34***
−.01
.04
−.02
.09*
.12**
.10*
.20***
.23***
.23***
.17***
PN-
--
-.34***
−.08
−.02
−.06
.07
.08*
.08*
.28***
.20***
.19***
.16***
SA
--
--
-−.04
.02
.02
.07
.04
.04
.20***
.11**
.12**
.07
SK-
--
--
-.69***
.78***
−.31***
−.22***
−.21***
−.31***
−.23***
−.13***
−.17***
CH
--
--
--
-.75***
−.09
−.02
−.01
−.12***
−.09**
−.01
−.02
MD
--
--
--
--
−.14**
−.15***
−.17***
−.22***
−.21***
−.14**
−.18***
SJ-
--
--
--
--
.80***
.82***
.50***
.47***
.43***
.50***
IS-
--
--
--
--
-.81***
.51***
.52***
.42***
.51***
OI
--
--
--
--
--
-.48***
.47***
.45***
.54***
FSC
--
--
--
--
--
--
.52***
.46***
.46***
Dep
--
--
--
--
--
--
-.65***
.74***
Anx
--
--
--
--
--
--
--
.71***
Stress
--
--
--
--
--
--
--
-
%30.9%
27.5%
11.9%
21.8%
9.4%
Mean
8.01
8.01
5.98
6.37
5.50
2.80
2.85
2.97
3.07
2.91
2.89
11.88
7.84
7.50
11.15
SD3.87
3.66
2.37
2.41
2.00
0.91
0.94
0.88
1.05
1.02
1.00
12.91
8.72
7.90
8.80
Range
2020
2017
204.80
4.50
4.25
4.60
4.75
4.00
57.39
42.00
42.00
42.00
*p<.05,**p<.01,and***p
<.001.E
Aem
otionalabuse
severity,E
Nem
otionalneglectseverity,PAphysicalabuseseverity,P
Nphysicalneglectseverity, SAsexualabuseseverity,SKself-kindness,CH
common
humanity,M
Dmindfulness,SJself-judgm
ent,IS
isolation,OIoveridentification,FSC
fear
ofself-com
passion,Dep
DASS
-Depression,Anx
DASS
-Anxiety,StressDASS-Stress,%
prevalence
(presence/absence)
ofmaltreatm
ent(mild
,moderate,or
severe
abuse/neglect)
Mindfulness (2020) 11:1446–1459 1451

isolation), and emotional neglect severity was negatively as-sociated with self-compassion (self-kindness, common hu-manity, and mindfulness). Sexual abuse and physical neglectseverity showed little to no association with self-compassion.
Suppression
We noted potential multicollinearity due to high correlationsamong some facets of self-compassion (see Table 1). Ininitial mediation models, there was evidence of suppression,with the direction of correlations switching in the multivar-iate model compared with bivariate correlations.Specifically, common humanity and self-kindness were cor-related negatively with psychological outcomes at the bivar-iate level, yet showed a positive relation with these out-comes (b paths) in the presence of other variables. To ad-dress this issue, we conducted an additional set of analyseswith models that excluded mindfulness given its high cor-relations with the other two positive subscales, and com-pared the patterns to determine the impact of suppressionon the models based upon recommendations by Beckstead(2012). Both sets of results are presented below.
The Role of Self-compassion
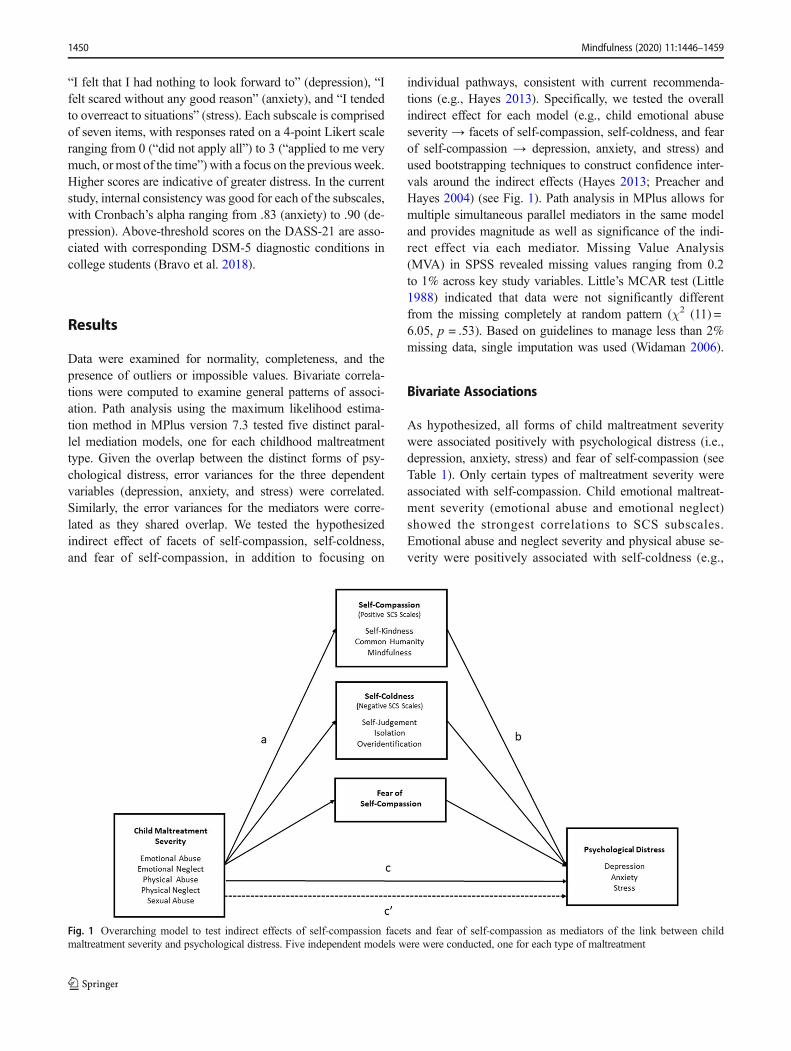
Three facets of self-compassion were examined: self-kind-ness, common humanity, and mindfulness. Self-kindnesswas a significant mediator of the relationship between (a)emotional abuse and anxiety, (b) emotional neglect and anxi-ety, and (c) emotional neglect and stress (see Table 2). In allthese models, increased severity of childhood emotional abuseand emotional neglect was associated with lower self-kind-ness. However, higher self-kindness was associated withhigher anxiety and stress. To address suppression effects,mindfulness was removed from the models, after which self-kindness was no longer a significant mediator. Common hu-manity was a significant mediator of the relationship between(a) emotional neglect and anxiety and (b) emotional neglectand stress (see Table 2). In these models increased severity ofemotional neglect was associated with lower common human-ity. Further, higher levels of common humanity were associ-ated with increased anxiety and stress. After mindfulness wasremoved from the models, common humanity was no longer asignificant mediator. Mindfulness was a significant mediatorof the relationship between (a) emotional neglect and depres-sion, (b) emotional neglect and anxiety, and (c) emotionalneglect and stress (see Table 2). In all models greater severityof emotional neglect was associated with decreased mindful-ness, which in turn was associated with higher depression,anxiety, and stress.
The Role of Self-coldness
Three facets of self-coldness were examined: self-judgment,isolation, and overidentification. Self-judgment was a signifi-cant mediator of the relationship between (a) emotional abuseand anxiety, (b) emotional neglect and anxiety, and (c) phys-ical abuse and anxiety (see Table 2). In all these models, in-creased childhood abuse and neglect severity were associatedwith higher self-judgment, which in turn was associated withhigher anxiety. After mindfulness was removed from the me-diation models, self-judgment was no longer a significant me-diator. Isolation was a significant mediator of the relationshipbetween (a) emotional abuse and depression, (b) emotionalneglect and depression, (c) emotional neglect and stress, (d)physical abuse and depression, (e) physical abuse and stress,(f) physical neglect and depression, and (g) physical neglectand stress (see Table 2). In all these models, increased child-hood abuse and neglect severity were associated with higherisolation, which in turn was associated with higher depressionand stress. After mindfulness was removed from the models,these results remained unchanged, except isolation emerged asa significant mediator of the relationship between emotionalabuse severity and stress. Overidentification was a significantmediator of the relationship between (a) emotional abuse andanxiety, (b) emotional abuse and stress, (c) emotional neglectand anxiety, (d) emotional neglect and stress, (e) physicalabuse and anxiety, and (f) physical abuse and stress (seeTable 2). In all these models, increased childhood abuse andneglect severity were associated with increased overidentifi-cation, which in turn was associated with increased anxietyand stress. After mindfulness was removed from the models,results remained largely unchanged, except overidentificationemerged as a significant mediator of the relationship betweenphysical neglect and anxiety.
The Role of Fear of Self-compassion
Fear of self-compassion mediated the relationship between(a) emotional abuse and depression, (b) emotional abuseand anxiety, (c) emotional abuse and stress, (d) emotionalneglect and depression, (e) emotional neglect and anxiety,(f) emotional neglect and stress, (g) physical abuse anddepression, (h) physical abuse and anxiety, (i) physicalabuse and stress, (j) physical neglect and depression, (k)physical neglect and anxiety, (l) physical neglect and stress,(m) sexual abuse and depression, (n) sexual abuse and anx-iety, and (o) sexual abuse and stress (see Table 2). In allthese models, increased severity of childhood maltreatmentwas associated with increased fear of self-compassion,which in turn was associated with higher depression, anxi-ety, and stress. After mindfulness was removed from themodels, results remained unchanged.
1452 Mindfulness (2020) 11:1446–1459
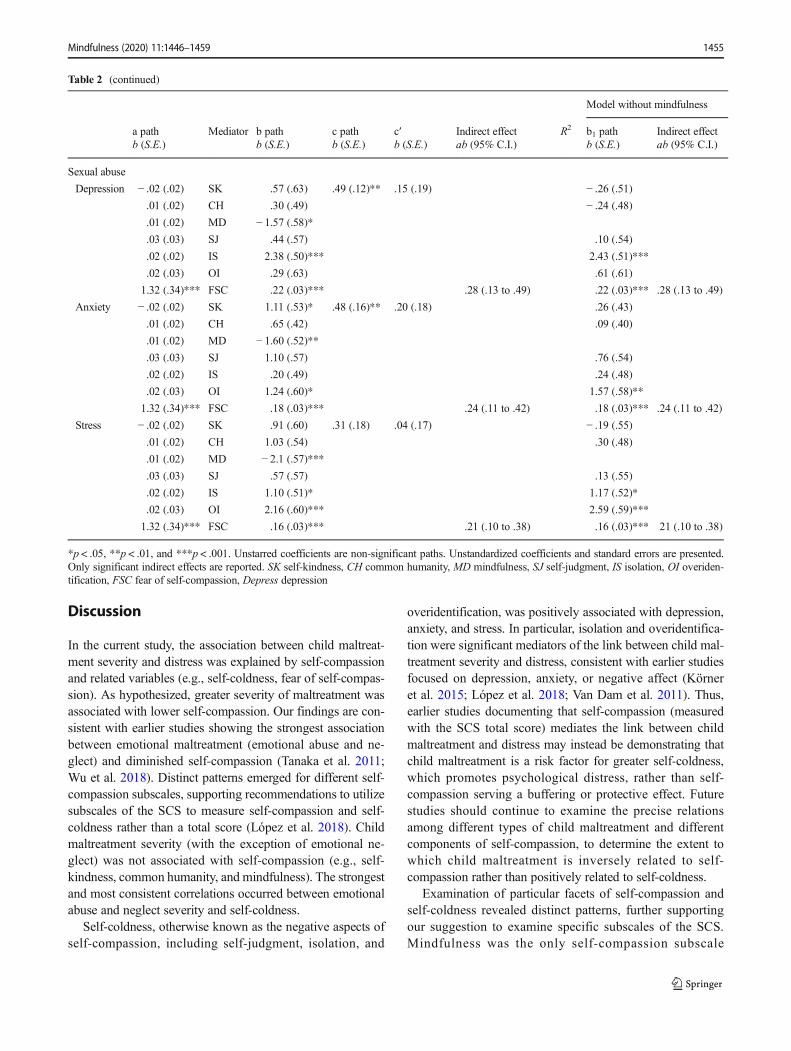
Table 2 Mediation models for childhood maltreatment severity
Model without mindfulness
a pathb (S.E.)
Mediator b pathb (S.E.)
c pathb (S.E.)
c′b (S.E.)
Indirect effectab (95% C.I.)
R2 b1 pathb (S.E.)
Indirect effectab (95% C.I.)
Emotional abuse
Depression − .03 (.01)** SK .63 (.63) .86 (.09)*** .39 (.10)*** − .23 (.51)
− .01 (.01) CH .30 (.48) − .27 (.47)
− .01 (.01) MD − 1.64 (.58)**.08 (.01)*** SJ .43 (.55) 08 (.53)
.08 (.01)*** IS 2.19 (.48)*** .18 (.10 to .27) 2.25 (.49)*** .18 (.10 to .28)
.07 (.01)*** OI .24 (.62) .57 (.60)
1.31 (.19)*** FSC .19 (.04)*** .24 (.14 to .38) .19 (.03)*** .24 (.14 to .38)
Anxiety − .03 (.01)** SK 1.16 (.52)* .73 (.08)*** .38 (.08)*** − .03 (− .09 to − 01) .28 (.42)
− .01 (.01) CH .65 (.41) .07 (.40)
− .01 (.01) MD − 1.66 (.50)**.08 (.01)*** SJ 1.09 (.54)* .08 (.006 to .19) .74 (.52)
.08 (.01)*** IS .01 (.46) .06 (.46)
.07 (.01)*** OI 1.2 (.58)* .09 (.009 to .18) 1.5 (.56)** .11 (.03 to .21)
1.31 (.19)*** FSC .15 (.03)*** .20 (.19 to .32) .15 (.02)*** .20 (.11 to .33)
Stress − .03 (.01)** SK 1.00 (.57) .86 (.09)*** .44 (.09)*** − .16 (.53)
− .01 (.01) CH 1.02 (.53) .24 (.47)
− .01 (.01) MD − 2.21 (.56)***.08 (.01)*** SJ .56 (.53) .09 (.52)
.08 (.01)*** IS .91 (.49) .99 (.49)* .08 (.004 to .17)
.07 (.01)*** OI 2.11 (.58)*** .15 (.07 to .26) 2.57 (.57)*** .18 (.10 to .30)
1.31 (.19)*** FSC .12 (.03)*** .16 (.07 to .27) .12 (.03)*** .16 (.07 to .26)
Emotional neglect
Depression − .05 (.01)*** SK .70 (.62) .80 (.09)*** .37 (.11)** − .19 (.50)
− .03 (.01)** CH .43 (.49) − .16 (.47)
− .03 (.01)** MD − 1.68 (.58)** .05 (.01 to .13)
.05 (.01)*** SJ .53 (57) .18 (.54)
.06 (.01)*** IS 2.21 (.48)*** .13 (.07 to .22) 2.27 (.49)*** .13 (.07 to .22)
.04 (.01)*** OI .35 (.62) .69 (.60)
1.42 (.17)*** FSC .18 (.03)*** .26 (.14 to .40) .18 (.04)*** .26 (.14 to .40)
Anxiety − .05 (.01)*** SK 1.21 (.53)* .62 (.07)*** .32 (.11)** − .06 (− .14 to − .01) .32 (.43)
− .03 (.01)** CH .77 (.42) − .03 (− .07 to − .001) .17 (.40)
− .03 (.01)** MD − 1.6 (.51)** .05 (.01 to .12)
.05 (.01)*** SJ 1.19 (.57)* .06 (.008 to .15) .83 (.54)
.06 (.01)*** IS .04 (.45) .10 (.47)
.04 (.01)*** OI 1.30 (.59)* .06 (.01 to .13) 1.64 (.57)** .07 (.02 to .15)
1.42 (.17)*** FSC .15 (.04)*** .21 (.11 to .35) .15 (.04)*** .21 (.11 to .36)
Stress − .05 (.01)*** SK 1.01 (.58) .61 (.26)*** .25 (.09)** − .05 (− .12 to − .002) − .14 (.54)
− .03 (.01)** CH 1.11 (.54)* − .04 (− .10 to − .004) .34 (.48)
− .03 (.01)** MD − 2.19 (.57)*** .07 (.02 to .15)
.05 (.01)*** SJ .64 (.57) .17 (.57)
.06 (.01)*** IS 1.00 (.51) .06 (.004 to .14) 1.08 (.52)* .06 (.008 to .14)
.04 (.01)*** OI 2.21 (.60)*** .10 (.04 to .19) 2.66 (.59)*** .06 (.05 to .22)
1.42 (.17)*** FSC .13 (.03)*** .19 (.10 to .31) .14 (.03)*** .19 (.10 to .32)
Mindfulness (2020) 11:1446–1459 1453

Table 2 (continued)
Model without mindfulness
a pathb (S.E.)
Mediator b pathb (S.E.)
c pathb (S.E.)
c′b (S.E.)
Indirect effectab (95% C.I.)
R2 b1 pathb (S.E.)
Indirect effectab (95% C.I.)
Physical abuse
Depression − .005 (.02) SK .50 (.61) .85 (.23)*** .46 (.20)*** − .26 (.50)
.01 (.02) CH .20 (.49) − .31 (.47)
− .007 (.02) MD − 1.45 (.57)*.04 (.02)* SJ .53 (.57) .22 (.54)
.05 (.02)* IS 2.26 (.48)*** .12 (.04 to .23) 2.30 (.49)*** .12 (.04 to .24)
.04 (.02)* OI .29 (.63) .59 (.61)
1.10 (.23)*** FSC .20 (.03)*** .23 (.10 to .40) .20 (.03)*** .23 (.10 to .40)
Anxiety − .005 (.02) SK 1.04 (.51)* .78 (.13)*** .49 (.12)*** .26 (.42)
.01 (.02) CH .55 (.42) .03 (.40)
− .007 (.02) MD − 1.48 (.50)*.04 (.02)* SJ 1.19 (.56)* .04 (.002 to .15) .89 (.54)
.05 (.02)* IS .07 (.46) .11 (.46)
.04 (.02)* OI 1.24 (.59)* .05 (.001 to .15) 1.54 (.57)** .06 (.006 to .17)
1.10 (.23)*** FSC .17 (.03)*** .19 (.08 to .34) .17 (.03)*** .19 (.08 to .34)
Stress − .005 (.02) SK .89 (.59) .62 (.17)*** .25 (.12)*** − .19 (.54)
.01 (.02) CH .97 (.50) .25 (.48)
− .007 (.02) MD − 2.04 (.57)***.04 (.02)* SJ .62 (.57) .19 (.56)
.05 (.02)* IS 1.04 (.51)* .06 (.007 to .14) 1.10 (.52)* .06 (.009 to .15)
.04 (.02)* OI 2.17 (.60)*** .09 (.01 to .21) 2.59 (.59)*** .11 (.01 to .24)
1.10 (.23)*** FSC .15 (.03)*** .17 (.07 to .31) .15 (.03)*** .17 (.07 to .31)
Physical neglect
Depression − .03 (.01) SK .56 (.63) .71 (.14)*** .27 (.16) SK − .24 (.51)
− .01 (.02) CH .28 (.49) CH − .25 (.48)
− .02 (.02) MD − 1.52 (.57)** MD
.03 (.02) SJ .50 (.57) SJ .18 (.55)
.04 (.02) IS 2.38 (.50)*** .08 (.003 to .20) IL 2.43 (.50)*** .09 (.003 to .20)
.03 (.02) OI .26 (.63) OI .57 (.61)
1.51 (.25)*** FSC .20 (.03)*** .31 (.17 to .49) FC .20 (.03)*** .31 (.18 to .49)
Anxiety − .03 (.01) SK 1.10 (.53)* .64 (.14)*** .30 (.15) SK .29 (.43)
− .01 (.02) CH .63 (.42) CH .09 (.41)
− .02 (.02) MD − 1.54 (.52)** MD
.03 (.02) SJ 1.18 (.58)* SJ .85 (.55)
.04 (.02) IS .19 (.48) IL .24 (.49)
.03 (.02) OI 1.21 (.60)* OI 1.53 (.58)** .05 (.001 to .15)
1.51 (.25)*** FSC .17 (.03)*** .26 (.14 to .42) FC .17 (.03)*** 26 (.14 to .42)
Stress − .03 (.01) SK .92 (.59) .57 (.15)*** .20 (.12) SK − .17 (.55)
− .01 (.02) CH 1.01 (.54) CH .27 (.48)
− .02 (.02) MD − 2.08 (.56)*** MD
.03 (.02) SJ .62 (.58) SJ .18 (.56)
.04 (.02) IS 1.12 (.51)* .04 (.001 to .12) IL 1.18 (.52)* .04 (.002 to .12)
.03 (.02) OI 2.15 (.60)*** OI 2.57 (.59)***
1.51 (.25)*** FSC .15 (.03)*** .23 (.12 to .38) FS .15 (.03)*** .22 (.12 to .38)
1454 Mindfulness (2020) 11:1446–1459
Discussion
In the current study, the association between child maltreat-ment severity and distress was explained by self-compassionand related variables (e.g., self-coldness, fear of self-compas-sion). As hypothesized, greater severity of maltreatment wasassociated with lower self-compassion. Our findings are con-sistent with earlier studies showing the strongest associationbetween emotional maltreatment (emotional abuse and ne-glect) and diminished self-compassion (Tanaka et al. 2011;Wu et al. 2018). Distinct patterns emerged for different self-compassion subscales, supporting recommendations to utilizesubscales of the SCS to measure self-compassion and self-coldness rather than a total score (López et al. 2018). Childmaltreatment severity (with the exception of emotional ne-glect) was not associated with self-compassion (e.g., self-kindness, common humanity, and mindfulness). The strongestand most consistent correlations occurred between emotionalabuse and neglect severity and self-coldness.
Self-coldness, otherwise known as the negative aspects ofself-compassion, including self-judgment, isolation, and
overidentification, was positively associated with depression,anxiety, and stress. In particular, isolation and overidentifica-tion were significant mediators of the link between child mal-treatment severity and distress, consistent with earlier studiesfocused on depression, anxiety, or negative affect (Körneret al. 2015; López et al. 2018; Van Dam et al. 2011). Thus,earlier studies documenting that self-compassion (measuredwith the SCS total score) mediates the link between childmaltreatment and distress may instead be demonstrating thatchild maltreatment is a risk factor for greater self-coldness,which promotes psychological distress, rather than self-compassion serving a buffering or protective effect. Futurestudies should continue to examine the precise relationsamong different types of child maltreatment and differentcomponents of self-compassion, to determine the extent towhich child maltreatment is inversely related to self-compassion rather than positively related to self-coldness.
Examination of particular facets of self-compassion andself-coldness revealed distinct patterns, further supportingour suggestion to examine specific subscales of the SCS.Mindfulness was the only self-compassion subscale
Table 2 (continued)
Model without mindfulness
a pathb (S.E.)
Mediator b pathb (S.E.)
c pathb (S.E.)
c′b (S.E.)
Indirect effectab (95% C.I.)
R2 b1 pathb (S.E.)
Indirect effectab (95% C.I.)
Sexual abuse
Depression − .02 (.02) SK .57 (.63) .49 (.12)** .15 (.19) − .26 (.51)
.01 (.02) CH .30 (.49) − .24 (.48)
.01 (.02) MD − 1.57 (.58)*
.03 (.03) SJ .44 (.57) .10 (.54)
.02 (.02) IS 2.38 (.50)*** 2.43 (.51)***
.02 (.03) OI .29 (.63) .61 (.61)
1.32 (.34)*** FSC .22 (.03)*** .28 (.13 to .49) .22 (.03)*** .28 (.13 to .49)
Anxiety − .02 (.02) SK 1.11 (.53)* .48 (.16)** .20 (.18) .26 (.43)
.01 (.02) CH .65 (.42) .09 (.40)
.01 (.02) MD − 1.60 (.52)**
.03 (.03) SJ 1.10 (.57) .76 (.54)
.02 (.02) IS .20 (.49) .24 (.48)
.02 (.03) OI 1.24 (.60)* 1.57 (.58)**
1.32 (.34)*** FSC .18 (.03)*** .24 (.11 to .42) .18 (.03)*** .24 (.11 to .42)
Stress − .02 (.02) SK .91 (.60) .31 (.18) .04 (.17) − .19 (.55)
.01 (.02) CH 1.03 (.54) .30 (.48)
.01 (.02) MD − 2.1 (.57)***
.03 (.03) SJ .57 (.57) .13 (.55)
.02 (.02) IS 1.10 (.51)* 1.17 (.52)*
.02 (.03) OI 2.16 (.60)*** 2.59 (.59)***
1.32 (.34)*** FSC .16 (.03)*** .21 (.10 to .38) .16 (.03)*** 21 (.10 to .38)
*p < .05, **p < .01, and ***p < .001. Unstarred coefficients are non-significant paths. Unstandardized coefficients and standard errors are presented.Only significant indirect effects are reported. SK self-kindness, CH common humanity, MD mindfulness, SJ self-judgment, IS isolation, OI overiden-tification, FSC fear of self-compassion, Depress depression
Mindfulness (2020) 11:1446–1459 1455

associated with depression, anxiety, and stress. However, thehigh degree of relatedness of self-compassion subscales, par-ticularly betweenmindfulness and self-kindness (and to a less-er degree, common humanity), likely affected multivariatemodels via statistical suppression. Thus, the hallmark compo-nents of self-compassion, such as self-kindness and commonhumanity, did not predict distress in multivariate models. Incontrast, mediation effects for self-coldness (e.g., negativefacets of self-compassion) revealed a specific pattern basedupon type of distress: depression was related only to isolation,anxiety was related only to overidentification, and stress wasrelated to both overidentification and isolation. Previous stud-ies support this pattern, suggesting a significant associationbetween overidentification (a negative facet of self-compassion) and increased fear of negative and positive eval-uation among individuals diagnosed with social anxiety dis-order (Werner et al. 2012). Overidentification may be a par-ticularly pernicious and potentially transdiagnostic thoughtprocess that mediates the links between multiple types of childmaltreatment severity and multiple outcomes (e.g., anxiety,stress). Notably, self-judgment, a variable potentially relatedto the self-esteem criterion of chronic depression (e.g., dys-thymia), was not a significant mediator. Instead, isolation andoveridentification, alongside fear of self-compassion, explainthe link between maltreatment severity and distress, but onlyfor particular forms of child maltreatment.
Our findings suggest that the type of child maltreatmentmatters, at least in terms of associations with self-compassion and self-coldness. Self-compassion is stronglyand negatively associated with emotional maltreatment (par-ticularly emotional abuse). Although the negative self-compassion components (i.e., self-coldness) were linked tophysical abuse severity as well, the magnitude was weaker,and there were no links to child sexual abuse severity, consis-tent with earlier research that examined different forms ofmaltreatment (Miron et al. 2014; Ross et al. 2019; Tanakaet al. 2011; Wu et al. 2018). Severity of emotional abuse andemotional neglect was correlated in this and other samples,and the two types of maltreatment have been conceptualizedas a composite variable in other studies (e.g., emotionalmaltreatment, see Wu et al. 2018). Emotional maltreatmentexperiences may bemore likely to involve particular elements,such as harsh criticism or name-calling, detrimental to devel-opment of self-compassion (Gilbert and Procter 2006). In ad-dition, emotional maltreatment frequently co-occurs with oth-er forms of child abuse, and thus carries a potential cumulativeimpact (Edwards et al. 2003). Finally, emotional or psycho-logical abuse has been posited to be a fundamental and poten-tially inseparable component of all forms of abuse and neglect(Edwards et al. 2003; Ross et al. 2019); thus, this form ofmaltreatment may be the most robust predictor of abuse-related outcomes because it pervades almost all types of childmaltreatment. This may speak to the complexity of emotional
maltreatment, especially that emotional abuse may coexistalongside more positive and caring parental interactions. Incontrast, emotional neglect is defined by the absence of pos-itive emotional interactions with a caregiver; therefore, thistype of maltreatment may be especially detrimental to devel-opment of self-compassion skills such as self-kindness andmindfulness. Indeed, emerging longitudinal research indicatesthat risk for depression is associated with specific symptoms,such as anhedonia, that varies as a function of abuse versusneglect (Cohen et al. 2019).
Fear of self-compassion mediated the link between childmaltreatment severity and distress. This pattern held for alltypes of child maltreatment and across types of distress (e.g.,depression, anxiety, and stress). Our findings are consistentwith another study that reported child abuse (emotional, phys-ical, and sexual measured together as one construct) was as-sociated with greater fear of self-compassion, and that fear ofself-compassion predicted posttraumatic stress symptoms(Boykin et al. 2018). Earlier studies did not examine specifictypes of child maltreatment and fear of self-compassion. Ourfindings suggest that regardless of type, as child maltreatmentseverity increases, there is also an increase in fear of beingcompassionate towards oneself. However, emotional abuseand emotional neglect severity show the strongest associationswith fear of self-compassion. Empirical investigations are justemerging on this topic; thus, the field needs more studies toexamine fear of self-compassion among survivors of differenttypes of child abuse and neglect. However, our findings areconsistent with theoretical arguments regarding child abuseand neglect as a pathway to fear of self-compassion (Gilbertand Procter 2006).
Limitations and Future Research
Our findings contribute to an emerging empirical consensusregarding the deleterious impact of child maltreatment on self-compassion. Several methodological strengths bolster ourconfidence in the current findings, including a large sample,inclusion of widely used and psychometrically sound mea-sures that facilitate direct comparisons across studies, and,most importantly, the investigation of a comprehensive modelthat examines components of self-compassion, self-coldness,and fear of self-compassion to identify specific predictors ofdistress. However, our results should be considered in thecontext of several limitations, including the focus on predom-inantly Caucasian female college students, which limits gen-eralization to non-college students, women of other ages,races, and ethnicities, and to men. The pattern of findingsreported here may also differ in other samples, particularlyamong community or clinical populations where the rangeof distress levels may be wider and absolute levels of distressmore severe. Research must continue to examine racial andethnic minority groups and intersectionality, factors which
1456 Mindfulness (2020) 11:1446–1459

have been commonly overlooked in research on the effects oftrauma and its treatment (Bryant-Davis 2019). One studyfound that female African American college students hadhigher levels, and female EuropeanAmerican college studentslower levels, of self-compassion (Miron et al. 2014). We mayfind that self-compassion operates differently among diversepopulations, interacting with strength and resilience factorssuch as religion and spirituality, as well as social support andadherence to communal values. Age is another factor that maymoderate patterns reported here. In a study of depressionamong individuals living with AIDS in the USA and PuertoRico, age was negatively associated with self-judgment andpositively associated with self-kindness (Eller et al. 2014).Studies of adolescents also indicate that age and gender aredifferentially associated with self-compassion and depression.Older adolescent females report the lowest levels of self-compassion compared with younger adolescents and all males(Bluth et al. 2017). Continued studies, on all individuals, areneeded to clarify the patterns found here. The interaction ofrace, age, and gender may be particularly important to exam-ine. A recent report from a nationally representative sample ofover 600,000 adolescents and adults in the USA suggests asignificant and steady rise in mood disorder and suicide-related outcomes (suicidal ideation, plans, attempts, anddeaths by suicide) among White, upper-middle class,college-aged women (Twenge et al. 2019).
We utilized a retrospective questionnaire to assess childmaltreatment that may be susceptible to memory bias, mini-mization, or poor recall. Although the CTQ includes a mini-mization and denial subscale, we did not compute such scores,consistent with earlier studies that utilized the same measure(Boykin et al. 2018; Miron et al. 2014, 2016; Tanaka et al.2011; Vettese et al. 2011; Wu et al. 2018). There is evidencethe CTQ may underestimate the incidence and impact of childmaltreatment when minimization is not taken into account(MacDonald et al. 2016). However, another study of theCTQ found few individuals minimized responses on theCTQ, but those with high minimization/denial scores wereunlikely to completely deny histories of abuse (Schmidtet al. 2018). Therefore, the pattern of findings reported heremay be a more conservative estimate of the true associationbetween child maltreatment and self-compassion. The CTQmay identify milder cases of sexual abuse or actual non-abusive experiences. In one study, comparison with a behav-iorally specific computerized interview showed significantagreement, but higher rates of sexual abuse on the CTQ(DiLillo et al. 2010). More detailed behaviorally specific as-sessment of child sexual abuse may reveal nuanced associa-tions with self-compassion based upon abuse characteristicsincluding nature of the abusive acts, frequency and duration,and relationship to the perpetrator (e.g., family member,trusted adult). The use of survey methods to assess all vari-ables and use of multiple subscales in several instruments
(e.g., CTQ, SCS) may lead to common method bias, whichcould produce spurious correlations among some variables(Podsakoff et al. 2003). Most importantly, the retrospective,cross-sectional design limits conclusions regarding the direc-tionality of effects as well as the causal and proximal nature ofrelations found. It is unclear whether the presence of distressaffects reports of fear of self-compassion, self-compassion,and child maltreatment severity rather than vice versa.
Child maltreatment predicts elevated risk of recurrent andpersistent depressive episodes resistant to treatment (Nanniet al. 2012); thus, we must continue to explore factors thatcultivate recovery and resilience among child maltreatmentsurvivors. Although fear of self-compassion is associated withchild maltreatment, we cannot assume that all survivors ofchild maltreatment will report difficulties described here.Continued research exploring child maltreatment and otherforms of interpersonal trauma is critical to expanding our un-derstanding of self-compassion and potential unique implica-tions for traumatized populations.
Acknowledgments Terri Messman-Moore would like to acknowledgegeneral professional support for this and all scholarly activities from anendowed professor position, The O’Toole, Family Professor, at MiamiUniversity.
Author Contributions Terri Messman-Moore and Prachi Bhuptani jointlydesigned the study. Prachi Bhuptani conducted data analyses and wrotepart of the results. Terri Messman-Moore wrote the introduction,methods, part of the results, and the discussion. All authors approvedthe final version of the manuscript for submission.
Compliance with Ethical Standards
Conflict of Interest The authors declare that they have no conflict ofinterest.
Ethical Approval All procedures were approved by the Committee forUse of Human Subjects in Research at Miami University. All proceduresperformed in studies involving human participants were in accordancewith the ethical standards of the institutional research committee atMiamiUniversity and with the 1964 Helsinki declaration and its later amend-ments or comparable ethical standards.
Informed Consent Informed consent was obtained from all individualparticipants in the study.
References
Beckstead, J. W. (2012). Isolating and examining sources of suppressionand multicollinearity in multiple linear regression. MultivariateBehavioral Research, 47, 224–246. https://doi.org/10.1080/00273171.2012.658331.
Bernstein, D. P., & Fink, L. (1998). Childhood Trauma Questionnaire: aretrospective self-report (CTQ). San Antonio: NCS Pearson.
Bifulco, A., Moran, P. M., Baines, R., Bunn, A., & Stanford, K. (2002).Exploring psychological abuse in childhood: II. Association withother abuse and adult clinical depression. Bulletin of the
Mindfulness (2020) 11:1446–1459 1457
Menninger Clinic, 66, 241–258. https://doi.org/10.1521/bumc.66.3.241.23366.
Bluth, K., Campo, R. A., Futch, W. S., & Gaylord, S. A. (2017). Age andgender differences in the associations of self-compassion and emo-tional well-being in a large adolescent sample. Journal of Youth andAdolescence, 46, 840–853. https://doi.org/10.1007/s10964-016-0567-2.
Boykin, D. M., Himmerich, S. J., Pinciotti, C. M., Miller, L. M., Miron,L. R., &Orcutt, H. K. (2018). Barriers to self-compassion for femalesurvivors of childhood maltreatment: the roles of fear of self-compassion and psychological inflexibility. Child Abuse &Neglect, 76, 216–224. https://doi.org/10.1016/j.chiabu.2017.11.003.
Bravo, A. J., Villarosa-Hurlocker, M. C., Pearson, M. R., & ProtectiveStrategies Study Team. (2018). College student mental health: anevaluation of the DSM-5 self-rated level 1 cross-cutting symptommeasure. Psychological Assessment, 20, 1381–1389. https://doi.org/10.1037/pas0000628.
Bryant-Davis, T. (2019). The cultural context of trauma recovery: con-sidering the posttraumatic stress disorder practice guideline andintersectionality. Psychotherapy, 56, 400–408. https://doi.org/10.1037/pst0000241.
Cohen, J. R., McNeil, S. L., Shorey, R. C., & Temple, J. R. (2019).Maltreatment subtypes, depressed mood, and anhedonia: a longitu-dinal study with adolescents. Psychological Trauma: Theory,Research, Practice, and Policy, 11(7), 704–712. https://doi.org/10.1037/tra0000418.
DiLillo, D., Fortier, M. A., Hayes, S. A., Trask, E., Perry, A. R.,Messman-Moore, T., Fauchier, A., & Nash, C. (2010).Retrospective assessment of childhood sexual and physical abuse:a comparison of scaled and behaviorally specific approaches.Asse s smen t , 13 , 297–312 . h t t p s : / / do i . o rg /10 .1177 /1073191106288391.
Edwards, V. J., Holden, G. W., Felitti, V., & Anda, R. F. (2003).Relationship between multiple forms of childhood maltreatmentand adult mental health in community respondents: results fromthe adverse childhood experiences survey. American Journal ofPsychiatry, 160, 1453–1460. https://doi.org/10.1176/appi.ajp.160.8.1453.
Eller, L. S., Rivero-Mendez, M., Voss, J., Chen, W.-T., Chaiphibalsarisdi,P., Iipinge, S., et al. (2014). Depressive symptoms, self-esteem, HIVsymptom management self-efficacy and self-compassion in peopleliving with HIV. AIDS Care, 26, 795–803. https://doi.org/10.1080/095-40121.2013.841842.
Evans, S. E., Steel, A., & DiLillo, D. (2013). Child maltreatment severityand adult trauma symptoms: does perceived social support play abuffering role?Child Abuse & Neglect, 37, 934–943. https://doi.org/10.1016/j.chiabu.2013.03.005.
Fritz, J., de Graaff, A. M., Caisley, H., van Harmelen, A. L., &Wilkinson,P. O. (2018). A systematic review of amenable resilience factors thatmoderate and/or mediate the relationship between childhood adver-sity and mental health in young people. Frontiers in Psychiatry, 9,230. https://doi.org/10.3389/fpsyt.2018.00230.
Gilbert, P., & Procter, S. (2006). Compassionate mind training for peoplewith high shame and self-criticism: overview and pilot study.Clinical Psychology and Psychotherapy, 13, 353–379. https://doi.org/10.1002/cpp.507.
Gilbert, P., McEwan, K., Matos, M., & Rivis, A. (2011). Fears of com-passion: development of three self-report measures. Psychology andPsychotherapy: Theory, Research, and Practice, 84, 239–255.https://doi.org/10.1348/147608310X526511.
Hagborg, J. M., Tidefors, I., & Fahlke, C. (2017). Gender differences inthe association between emotional maltreatment with mental, emo-tional, and behavioral problems in Swedish adolescents. ChildAbuse & Neglect, 67, 249–259. https://doi.org/10.1016/j.chiabu.2017.02.033.
Hartford, T. C., Yi, H., & Grant, B. F. (2014). Associations betweenchildhood abuse and interpersonal aggression and suicide attemptamong U.S. adults in a national study. Child Abuse & Neglect, 38,1389–1398. https://doi.org/10.1016/j.chiabu.2014.02.011.
Hayes, A. F. (2013). Introduction to mediation, moderation, and condi-tional process analysis: a regression-based approach. New York:The Guilford Press.
Játiva, R., & Cerezo, M. A. (2014). The mediating role of self-compassion in the relationship between victimization and psycho-logical maladjustment in a sample of adolescents. Child Abuse &Neglect, 38, 1180–1190. https://doi.org/10.1016/j.chiabu.2014.04.005.
Körner, A., Coroiu, A., Copeland, L., Gomez-Garibello, C., Albani, C.,Zenger, M., & Brähler, E. (2015). The role of self-compassion inbuffering symptoms of depression in the general population. PLoSOne, 10, e0136598. https://doi.org/10.1371/journal.pone.0136598.
Krieger, T., Berger, T., & Holtforth, M. G. (2016). The relationship ofself-compassion and depression: cross-lagged panel analyses in de-pressed patients after outpatient therapy. Journal of AffectiveDisorders, 202, 39–45. https://doi.org/10.1016/j.jad.2016.05.032.
Li, M., D’Arcy, C., & Meng, X. (2016). Maltreatment in childhood sub-stantially increases the risk of adult depression and anxiety in pro-spective cohort studies: systematic review, meta-analysis, and pro-portional attributable fractions. Psychological Medicine, 46, 717–730. https://doi.org/10.1017/S0033291715002743.
Little, R. A. (1988). A test of missing completely at random for multivar-iate data with missing values. Journal of the American StatisticalAssociation, 83(404), 1198–1202. https://doi.org/10.2307/2290157.
López, A., Sanderman, R., & Schroevers, M. J. (2018). A close exami-nation of the relationship between self-compassion and depressivesymptoms. Mindfulness, 9, 1470–1478. https://doi.org/10.1007/s12671-018-0891-6.
Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negativeemotional states: comparison of the depression anxiety stress scales(DASS) with the Beck depression and anxiety inventories.Behaviour Research and Therapy, 33, 335–343. https://doi.org/10.1016/0005-7967(94)00075-U.
MacBeth, A., & Gumley, A. (2012). Exploring compassion: a meta-analysis of the association between self-compassion and psychopa-thology. Clinical Psychology Review, 32, 545–552. https://doi.org/10.1016/j.cpr.2012.06.003.
MacDonald, K., Thomas, M. L., Sciolla, A. F., Schneider, B., Pappas, K.,Bieijenberg, G., Bohus, M., Bekh, B., Carpenter, L., Carr, A.,Dannlowski, U., Dorahy, M., Fahlke, C., Finzi-Dottan, R., Karu,T., Gerdener, A., Glaesmer, H., Grabe, H. J., Heins, M., et al.(2016). Minimization of childhood maltreatment is common andconsequential: results from a large, multinational sample using theChildhood Trauma Questionnaire. PLoS One, 11(1), e0146058.https://doi.org/10.1371/journal.pone.0146058.
Maples, L. A., Park, S. S., Nolen, J. P., & Rosen, L. A. (2014). Resilienceto childhood abuse and neglect in college students. Journal ofAggression, Maltreatment & Trauma, 23, 1001–1019. https://doi.org/10.1080/10926771.2014.964435.
Merikangas, K. R., He, J. P., Burstein, M., Swanson, S. A., Avenevoli, S.,Cui, L., et al. (2010). Lifetime prevalence ofmental disorders in U.S.adolescents: results from the National Comorbidity SurveyReplication—Adolescent Supplement (NCS-A). Journal of theAmerican Academy of Child and Adolescent Psychiatry, 49, 980–989. https://doi.org/10.1016/j.jaac.2010.05.017.
Miron, L. R., Orcutt, H. K., Hannan, S. M., & Thompson, K. L. (2014).Childhood abuse and problematic alcohol use in college females: therole of self-compassion. Self and Identity, 13, 364–379. https://doi.org/10.1080/15298868.2013.836131.
Miron, L. R., Seligowski, A. V., Boykin, D. M., & Orcutt, H. K. (2016).The potential indirect effect of childhood abuse on posttrauma pa-thology through self-compassion and fear of self-compassion.
1458 Mindfulness (2020) 11:1446–1459

Mindfulness, 7, 596–604. https://doi.org/10.1007/s12671-016-0493-0.
Muris, P., & Petrocchi, N. (2017). Protection or vulnerability? A meta-analysis of the relations between positive and negative componentsof self-compassion and psychopathology. Clinical Psychology andPsychotherapy, 24, 373–383. https://doi.org/10.1002/cpp.2005.
Naismith, I., Zarate Guerrero, S., & Feigenbaum, J. (2019). Abuse, inval-idation, and lack of early warmth show distinct relationships withself-criticism, self-compassion, and fear of self-compassion in per-sonality disorder. Clinical Psychology and Psychotherapy, 26, 350–361. https://doi.org/10.1002/cpp.2357.
Nanni, V., Uher, R., & Danese, A. (2012). Childhood maltreatment pre-dicts unfavorable course of illness and treatment outcome in depres-sion: a meta-analysis. The American Journal of Psychiatry, 169,141–151. https://doi.org/10.1176/appi.ajp.2011.11020335.
Neff, K. (2003). Development and validation of a scale to measure self-compassion. Self and Identity, 2, 223–250.
Nolen-Hoeksema, S., & Aldao, A. (2011). Gender and age differences inemotion regulation strategies and their relationship to depressivesymptoms. Personality and Individual Differences, 51, 704–708.https://doi.org/10.1016/j.paid.2011.06.012.
Podsakoff, P. M., MacKenzie, S. B., Lee, J. Y., & Podsakoff, N. P. (2003).Common method biases in behavioral research: a critical review ofthe literature and recommended remedies. Journal of AppliedPsychology, 88(5), 879–903. https://doi.org/10.1037/0021-9010.88.5.879.
Preacher, K. J., & Hayes, A. F. (2004). SPSS and SAS procedures forestimating indirect effects in simple mediation models. BehaviorResearch Methods, Instruments, & Computers, 36, 717–731.
Reffi, A. N., Boykin, D.M., &Orcutt, H. K. (2019). Examining pathwaysof childhood maltreatment and emotional dysregulation using self-compassion. Journal of Aggression, Maltreatment, & Trauma, 28,1269–1285. https://doi.org/10.1080/10926771.2018.1485810.
Rehan, W., Antfolk, J., Johansson, A., Jern, P., & Santtila, P. (2017).Experiences of severe childhood maltreatment, depression, anxietyand alcohol abuse among adults in Finland. PLoS One, 12(5),e0177252. https://doi.org/10.1371/journal.pone.0177252.
Rehan, W., Antfolk, J., Johansson, A., & Santtila, P. (2019). Do singleexperiences of childhood abuse increase psychopathology symp-toms in adulthood? Journal of Interpersonal Violence, 34, 1021–1038. https://doi.org/10.1177/0886260516647004.
Ross, N. D., Kaminski, P. L., & Herrington, R. (2019). From childhoodemotional maltreatment to depressive symptoms in adulthood: theroles of self-compassion and shame.Child Abuse&Neglect, 92, 32–42. https://doi.org/10.1016/j.chidabu.2019.03.016.
Sachs-Ericsson, N., Verona, E., Joiner, T., & Preacher, J. K. (2006).Parental verbal abuse and the mediating role of self-criticism in adultinternalizing disorders. Journal of Affective Disorders, 93, 71–78.https://doi.org/10.1016/j.jad.2006.02.014.
Scher, C. D., Forde, D. R., McQuaid, J. R., & Stein, M. B. (2004).Prevalence and demographic correlates of childhood maltreatmentin an adult community sample. Child Abuse & Neglect, 28, 167–180. https://doi.org/10.1016/j.chiabu.2003.09.012.
Schmidt, M. R., Narayan, A. J., Atzl, V. M., Rivera, L. M., & Lieberman,A. F. (2018). Childhood maltreatment on the Adverse ChildhoodExperiences (ACEs) Scale versus the Childhood TraumaQuestionnaire (CTQ) in a perinatal sample. Journal of Aggression,Maltreatment & Trauma. Advance online publication. https://doi.org/10.1080/10926771.2018.1524806.
Scoglio, A. A. J., Rudat, D. A., Garvert, D., Jarmolowski, M., Jackson,C., & Herman, J. L. (2018). Self-compassion and responses to trau-ma: the role of emotion regulation. Journal of InterpersonalVio l ence , 33 , 2016–2036 . h t t p s : / / do i . o rg /10 .1177 /0886260515622296.
Taillieu, T., Brownridge, D. A., Sareen, J., & Afifi, T. O. (2016).Childhood emotional maltreatment and mental disorders: resultsfrom a nationally representative adult sample from the UnitedStates. Child Abuse & Neglect, 59, 1–12. https://doi.org/10.1016/j.chiabu.2016.07.005.
Tanaka, M., Wekerle, C., Schmuck, M. L., Paglia-Boak, A., & ResearchTeam, M. A. P. (2011). The linkages among childhood maltreat-ment, adolescent mental health, and self-compassion in child wel-fare adolescents. Child Abuse & Neglect, 35, 887–898. https://doi.org/10.1016/j.chiabu.2011.07.003.
Teicher, M. H., & Samson, J. A. (2013). Child maltreatment and psycho-pathology: a case for ecophenotypic variants as clinically andneurobiologically distinct subtypes. American Journal ofPsychiatry, 170, 1114–1133. https://doi.org/10.1176/appi.ajp.2013.12070957.
Twenge, J. M., Cooper, A. B., Joiner, T. E., Duffy, M. E., & Binau, S. G.(2019). Age, period, and cohort trends in mood disorder indicatorsand suicide-related outcomes in a nationally representative dataset,2005-2017. Journal of Abnormal Psychology. Advance online pub-lication. https://doi.org/10.1037/abn0000410.
Van Dam, N. T., Sheppard, S. C., Forsyth, J. P., & Earleywine, M. (2011).Self-compassion is a better predictor than mindfulness of symptomseverity and quality of life in mixed anxiety and depression. Journalof Anxiety Disorders, 25, 123–130. https://doi.org/10.1016/j.janxdis.2010.08.011.
Vettese, L. C., Dyer, C. E., Li, W. L., & Wekerle, C. (2011). Does self-compassion mitigate the association between childhood maltreat-ment and later emotional regulation difficulties? A preliminary in-vestigation. International Journal of Mental Health and Addiction,9, 480–491. https://doi.org/10.1007/s11469-011-9340-7.
Werner, K. H., Hooria Jazaieri, M. A., Goldin, P. R., Ziv, M., Heimberg,R. G., & Gross, J. J. (2012). Self-compassion and social anxietydisorder. Anxiety, Stress, and Coping, 25, 543–558. https://doi.org/10.1080/10615806.2011.608842.
Widaman, K. F. (2006). III. Missing data: what to do with or withoutthem. Monographs of the Society for Research in ChildDevelopment, 71(3), 42–64. https://doi.org/10.1111/j.1540-5834.2006.00404.x.
Wilson, A. C., Mackintosh, K., Power, K., & Shan, S. W. Y. (2019).Effectiveness of self-compassion related therapies: a systematic re-view and meta-analysis. Mindfulness, 10, 977–995. https://doi.org/10.1007/s12671-018-1037-6.
Wu, Q., Chi, P., Lin, X., & Du, H. (2018). Child maltreatment and adultdepressive symptoms: roles of self-compassion and gratitude. ChildAbuse & Neglect, 80, 62–69. https://doi.org/10.1016/j.chiabu.2018.03.013.
Yarnell, L. M., Stafford, R. E., Neff, K. D., Reilly, E. C., Knox, M. C., &Mullarkey, M. (2015). Meta-analysis of gender differences in self-compassion. Self and Identity, 14, 499–520. https://doi.org/10.1080/15298868.2015.1029966.
Publisher’s Note Springer Nature remains neutral with regard to jurisdic-tional claims in published maps and institutional affiliations.
Mindfulness (2020) 11:1446–1459 1459