Embed Size (px)
Citation preview

Secreting Tumors of Chromaffin Tissue *
MAJ. GILBERT D. HUEBNER, " MC, USA, COL. PAUL A. REED, * MG, USA
FUNCrIONING chromaffin tumors are arare but surgically curable cause of hyper-tension. Approximately 90 per cent de-velop within the medullary portion of theadrenal gland and are more commonlycalled pheochromocytomas. The remainderarise from the sympathetic ganglia or theirectopic remnants and are generally referredto as paragangliomas. The latter occasion-ally originate within the para-aortic bodies(organs of Zuckerkandl). These are pairedstructures located at the aortic bifurcationjust distal to the origin of the inferiormesenteric artery. Although these bodiesnormally disappear by the second year oflife, they may persist and hence predisposeto subsequent tumor formation.8 Regard-less of location, chromaffin tissue is com-prised of cells which are histologicallysimilar and stain yellow with chromic acid.The designation 10 per cent tumor has beenapplied to these neoplasms because 10 percent are malignant, 10 per cent bilateraland, as already noted, 10 per cent areextra-adrenal.
Secreting paragangliomas of the organsof Zuckerkandl are most uncommon. Only17 cases have been documented in themedical literature to date. Of these fourhave been surgically extirpated, with re-versal of hypertension.4 11, 22,25 It is thepurpose of this discussion to present whatthe authors believe is the eighteenth caseof a functioning paraganglioma, located atthe organ of Zuckerkandl. It was surgically
* Submitted for publication October 12, 1962.* * Present address: 60th Station Hospital,
APO 256, New York, N. Y.*F*o* Present address: Ireland Aryy Hospital,
Fort Knox, Kentucky.
excised by one of the authors (P. A. R.)with reversal of the patient's hypertension.This case represents many if not most ofthe difficulties encountered in the diagnosisand management of secreting chromaffintumors.
Case ReportIn February 1959, a 52-year-old Negro man
was admitted to the U. S. Army Hospital, WestPoint, N. Y., for evaluation of an abdominal massand for follow up care after the excision of asoft tissue lesion as an outpatient. The patient wasa known hypertensive of eight years' duration. In1954, while serving overseas, he suffered a cerebralhemorrhage and was left with a mild left-sidedspastic paralysis. As a result of this he was retiredfrom the active military service. Other pertinentdata revealed the patient had neurofibromatosis(confirmed by biopsy specimen) and had under-gone an uneventful hernioplasty the previous year.His medical records showed numerous and per-sistently elevated blood pressure determinations re-corded by many different physicians. He had beenevaluated in several hospitals and considered tohave essential hypertension. On this admission hisblood pressure was 180/110, and multiple de-terminations showed little variation. The abdominalmass was on the left and approximately 9.0 x 10cm. Pertinent barium x-ray studies showed themass to be retroperitoneal, but extrinsic to thegastro-intestinal or genito-urinary tract. He wasoperated upon with a tentative diagnosis of retro-peritoneal neurofibroma. Exploration was per-formed through a long left paramedian incision.A 10 X 9.0 X 8.0 cc. tumor was located in theregion of Zuckerkandl's organ. During operativemanipulation of the well-encapsulated tumor mass,there was a dramatic rise in blood pressure to 240/140, with the onset of auricular fibrillation. At thispoint the mass was recognized as a secretingparaganglioma. It was therefore gently manipu-lated in order to obtain immediate occlusion of itsvascular pedicle. The neoplasm was found to besuipplied by a large artery arising directly fromthe wall of the aorta and distal to the inferior
216

SECRETING TUMORS OF CHROMAFFIN TISSUE
mesenteric artery. Following ligation of the bloodsupply, there was an equally abrupt drop in bloodpressure to 90/50. Although blood loss had beenminimal, the administration of four units of wholeblood was effective in maintaining the systolicpressure at 100, with a normal pulse of goodquality. The following day the patient's bloodpressure had stabilized at 120/80, and his hemo-globin was 14.5 Gm. His subsequent blood pres-
sure readings have levelled at a mean of 140/90.Final pathological study showed the tumor to behistologically similar to any other pheochromo-cytoma or paraganglioma.
Historical Aspects
The earliest autopsy report of an adrenalchromaffin tumor in a patient, who hadsymptoms consistent with a pheochromo-cytoma, was recorded in 1886.10 The firstsuccessful surgical removal of a chromaf-finoma, however, was performed by Mayoin 1927. Confronted with a 30-year-oldwoman, who was experiencing attacks ofheadache, pallor, nausea, and vomiting, andimpressed by the concomitant marked in-crease in blood pressure, Mayo exploredthe patient in anticipation of finding some
abnormality of the sympathetic nervous
system. He was rewarded by finding a 6.0x 4.0 cm. tumor in the left adrenal gland.The patient was subsequently relieved ofher symptoms and remained normotensive.According to Ainley-Walker, 70 per centof recorded pheochromocytomas have beenfound at autopsy 2 as an unexpected find-ing. The true incidence of secreting chro-maffin tumors is consequently speculativebecause of failure to make the correct diag-nosis. Graham had estimated that 600 to800 new cases will arise annually in thenation.'6 One regional survey indicatedthat these neoplasms were responsible for1.3 of every 100,000 hospital admissions.2'By contrast, a physician in England re-
cently reported two cases of pheochromo-cytoma within one year from among a
practice of 2,800 patients.30 Such statisticsemphasize that these lesions are found morefrequently when the clinician is aware oftheir existence.
Clinical Picture
While paroxysmal hypertension is themost significant manifestation of a chromaf-finoma, hypertension is sustained in ap-
proximately a third of all cases. Tumor sizeand duration are obviously important to
the development of sustained hypertension.Eventual impairment of cardiac and renalfunction is similar to that seen in otherforms of hypertension and lethality derivesfrom the same effects. These neoplasmsshow little predilection for either sex, butmost frequently occur in the 20 to 50 age
group. Children are not exempt, however,as Palmieri collected 68 cases in childrenunder 14 years of age.23 A seldom em-
phasized aspect of these tumors is that theyare usually symptomatic. Blacklock foundonly 11.4 per cent of 141 cases reviewedwere asymptomatic.6 The clinical symp-
toms produced are directly attributable tooverproduction of epinephrine or norepi-nephrine, or both, by the tumor cells. Ithas now been convincingly demonstratedthat the adrenal medulla elaborates bothsubstances while the chromaffin cells else-where produce only norepinephrine.32 Thisis particularly helpful in differentiating tu-mors of adrenal or of extra-adrenal origin.The typical paroxysmal attack is related
to the sudden release of catecholamines.With a predominance of epinephrine, thecardiac output and rate increase, producingtachycardia, palpitations, and occasionallysubsternal distress. Although blood pressurerises, there will be a greater elevation ofsystolic than diastolic pressure. Other mani-festations are headache, sweating, vertigo,nausea and vomiting, and visual disturb-ances in varying degrees. Norepinephrineacts more specifically as a vasoconstrictorof the peripheral vascular bed with re-
sultant sharp rise in diastolic blood pres-sure and associated bradycardia. The fre-quency of attacks will vary from ten or
more daily to but an isolated episode everyfew months. Paroxysms may last ten to 15
Volume 158Number 2 217

HUEBNER AND REED Annals of SurgeryAugust 1963
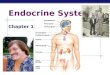
FIG. 1. Paragangliomaof the organ of Zucker-kandl. The gross speci-men reveals a 9.0 X 9.0x 8.0 cm. encapsulatedtumor mass, cut in grosssection. The cortex wasgolden yellow with a
somewhat more reddish-yellow necrotic center.
minutes or longer or occasionally may beso transient as to last but seconds. Anxiety,emotional upset, changes in posture, andother occult stimuli have been known to
precipitate an attack. In the case reportedherein, the patient volunteered, in retro-spect, that whenever he leaned forward tolace his shoes, he experienced a pounding
headache. From the location of his tumor itis logical to assume that postural changeproduced compression of the neoplasm.When the act of urinating evokes an at-tack, one should consider the possibility ofparaganglioma within the urinary bladder.Sivak recently collected 11 cases of func-tioning paragangliomas so located.29 It is
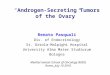
FiG. 2. Microscopic
section of the tumor re-
veals sheets and nests oflarge polygonal cells with
abundant granular cyto-
-plasm and oval vesicu-
lated nuclei. (H. & E.
stain. )
218

Volume 158 SECRETING TUMORSNumber 2
also noteworthy that a documented case ofpheochromocytoma with paroxysmal hypo-tension has occurred.26 Such a situation istheoretically explained by the fact thatsmall amounts of epinephrine may producevasodilation without significantly alteringcardiac output.
In the quiescent interval between at-tacks, there is generally increased circulat-ing epinephrine sufficient to create andmaintain a state of hypermetabolism. Ele-vated basal metabolic rate in associationwith other symptoms may lead to an er-roneous diagnosis of thyrotoxicosis. In ad-dition, the glycogenolytic effect of epineph-rine frequently causes hyperglycemia witha demonstrably abnormal glucose tolerancecurve. Elevated serum catecholamines alsoaffect lipid metabolism by mobilizing fatfrom adipose tissue and causing its deposi-tion in the myocardium,19 liver, and renaltubules. The co-existence of chromaffin tu-mor and neurofibromatosis, as seen in thiscase report, is not unusual. Schlegel col-lected 45 cases from the literature in whichboth entities were present.28 Other authorsquote an incidence of from 5.0 to 30 percent of neurofibromatosis in cases of chro-maffinoma.14' 18 The relationship betweenthe two diseases is not readily apparentalthough both represent a neoplastic aber-ration of ectodermal tissue.
Helpful Diagnostic AidsPharmacologic tests used to support the
diagnosis of chromaffinoma fall into threecategories: 1) those tests employed to stim-ulate the tumor and provoke an attack ofhypertension (provocative tests); 2) thoseintended to nullify the catecholamines andlower blood pressure by the administrationof an adrenolytic agent (blocking tests);and 3) those which directly measure cate-cholamines and their by-products withinserum or urine. Of the provocative tests,the histamine test of Roth and Kvale is themost widely used.27 The most popularblocking test depends upon the adrenolytic
of CHROMAFFIN TISSUE 219
effect of phentolamine (Regitine) to lowerblood pressure.12 It has wider applicabilityand a greater margin of safety, althoughfalse positives occur in patients who areuremic or who have been sedated withbarbiturates or tranquilizers. Prior admin-istration of antihypertensive agents maylikewise give a false negative result. Meas-urement of serum and urinary catechola-mines is more direct, more specific, andsubject to less error.15' 20 Elevated bloodand urinary levels should be present evenduring the quiescent phase in patients sub-ject to paroxysmal attacks. Armstrong3 andGitlow 13 described a simple screening test,which measures vanillylmandelic acid inurine by paper chromatography. Vanillyl-mandelic acid is a metabolic by-product ofthe degradation of catecholamines.When chromaffinoma is reasonably sus-
pected on the basis of the aforementionedclinical studies, it then becomes imperativeto attempt to localize the tumor. The epi-nephrine secreting lesion limits location toeither the right or left adrenal gland. Pre-sacral retroperitoneal pneumotography hasbeen advocated by many, while others pre-fer angiography. The combined advantagesof both procedures have been demonstratedby Flint and Bartels.9 They also reportedno untoward effects in 400 instances wherepresacral air study was employed. Anotherapproach is venous catheterization underfluoroscopic control. Blood samples takenfrom the area of the tumor have beenshown to have increased elevations ofcatecholamines.33
Surgical ConsiderationsIn general, an upper transverse abdomi-
nal incision is preferred. This permits ex-ploration of both adrenals as well as theparavertebral sympathetic ganglia and re-gion of the organs of Zuckerkandl. Theright adrenal is readily exposed by down-ward and medial retraction of the hepaticflexure of the colon while simultaneouslyretracting the liver upward. By incising the

HUEBNER AND REED Annals of Surgery220 ~~~~~~~~~~~~~~~~~~~~~~~~~~August 1963
posterior peritoneum overlying the upperpole of the right kidney, the right adrenalis readily exposed. The left adrenal is moredifficult, although it can be approachedthrough the lesser sac. When the tumor isfound, it should be gently manipulated andearly ligation of its venous drainage per-formed. On the left side there is usuallyone large vein, which empties directly intothe left renal vein. On the right side, how-ever, multiple small veins drain the adrenaland empty directly into the vena cava.
Hypertensive crises are known to occurduring tumor manipulation. Not infre-quently patients harboring unsuspectedchromaffin tumors develop acute hyperten-sion during induction of anesthesia or dur-ing operation performed for unrelated dis-ease.31 The danger of such manipulation isattested to by the fact that it is accom-panied by a 50 per cent mortality.' Admin-istration of Regitine in doses of 2.5 mg. isthe most effective means of controlling thisreaction. Bartels and Catell 5 believe thesehypertensive crises should be treated withthe same urgency as in cardiac arrest. Theyrecommend the following courses of ac-tion: 1) immediate discontinuance of theoperation and further investigation on re-covery; 2) in intra-abdominal operation, im-mediate exploration of the adrenals andthe sympathetic chain areas, with removalof the tumor if found; and 3) an adrenolyticdrug to control hypertension followed bycontinuance of the initial operation, andpostoperative investigative studies to con-firm the presence of a chromaffin tumor(the response of blood pressure to theadrenolytic drug providing additional evi-dence).Development of shock following resec-
tion of the tumor and coincident with liga-tion of its venous return is not uncommon.For many years this phenomenon was at-tributed to myocardial strain and left ven-tricular failure. It has been more recentlyshown, however, that the mechanism istrue peripheral vascular collapse or vaso-
dilatation. Peripheral arteries and arteriolesessentially become adjusted to high cir-culating levels of norepinephrine. Whenexcess production of these hormones sud-denly ceases, the vessels are unable to main-tain normal tonic contraction, and vasodila-tation follows. Administration of large vol-umes of blood frequently is insufficient torestore blood pressure. However, promptuse of norepinephrine, which can be ti-trated by intravenous drip (4.0 mg. in 1,000cc. of 5.0% glucose in water) is usuallyadequate until stability of the circulationreturns and norepinephrine therapy can bediscontinued.17 Additionally, it should bementioned that if preoperative localizationof the tumor is not possible and abdominalexploration fails to disclose it, considera-tion must be given to more remote pos-sibilities. Chromaffinomas have been re-ported as occurring both intracranially 7
and in the thoracic cavity.24
SummaryFunctioning tumors of chromaffin tissue
are more common than originally thought,as evidenced by the attention they arepresently receiving in medical literature.As a surgically curable cause of hyperten-sion, the tumors must be actively sought ifearly diagnosis and corrective operation isto be performed. An unusual case of secret-ing paraganglioma occurring at the organof Zuckerkandl is herein reported. Currenttheories and knowledge regarding clinicalsymptoms and manifestations produced byexcess production of catecholamines havebeen briefly discussed together with theinteresting background history.
Bibliography1. Agpar, V. and E. Papper: Pheochromocy-
tomata: Anesthetic Management During Sur-gical Treatment. Arch. Surg., 62:634, 1951.
2. Ainley-Walker, J. and J. Woodward: AcuteHypertension Developing under Anesthesia.Br. J. Anesthesia, 31:167, 1959.
3. Armstrong, M., K. Shaw, M. Gortatowski andH. Singer: The Indole Acids of Human

Volume 158 SECRETING TUMORS OF CHROMAFFIN TISSUE 221Number 2
Urine. Paper Chromatography of IndoleAcids. J. Biolog. Chem., 232:17, 1958.
4. Attia, A., R. L. Golden and H. Ziffer: Non-chromaffin Staining Functional Tumor of theOrgans of Zuckerkandl. New Engl. J. Med.,264:1130, 1961.
5. Bartels, E. C. and R. B. Catell: Pheochromo-cytoma: Its Diagnosis and Treatment. Ann.Surg., 131:903, 1950.
6. Blacklock, J. W., J. Ferguson, W. Mach, J.Shafar and T. Symington: Pheochromocy-toma. Br. J. Surg., 35:179, 1947.
7. Cahill, G.: Intracranial Pheochromocytoma.Surgery, 16:233, 1940.
8. Cook, J., R. Urich, H. Sample and N. Fawcett:Peculiar Familial and Malignant Pheochro-mocytomas of the Organs of Zuckerkandl.Ann. Int. Med., 52:126, 1960.
9. Flint, L. and C. Bartels: Experience with 15Operated Cases of Pheochromocytoma. Surg.Cl. N. America, 42:721, 1962.
10. Fraenkel, F.: Ein Fall von Doppelsteitigen,Voelig Latent Verlaufenen Nebenieren Tu-mor und Gleichzeitiger Nephritis mit Veraen-derungen am Circulations Apparatus undRetinitis. Virchows Arch. Path. Anat., 103:244, 1886.
11. Fullerton, C. W., J. C. Sutton and I. G. Milne:A Case of Secreting Paraganglioma of Organof Zuckerkandl. Ann. Int. Med., 40:1212,1954.
12. Gifford, R., G. Roth and W. Kvale: Evalua-tion of a New Adrenolytic Drug as a Testfor Pheochromocytoma. J.A.M.A., 149:1628,1952.
13. Gitlow, S. E., L. Ormstein, M. Mendlowitz, S.Khassis and E. Kruk: Simple ColorometricTests for Pheochromocytoma. Am. J. Med.,28:921, 1960.
14. Glenn, F.: Lesions of the Parathyroid, Ad-renal, and Thymus Glands Amenable to Sur-gery. U. S. A. F. Med. J., 11:49, 1960.
15. Goldenberg, M., I. Serlin, T. Edwards andM. Rapport: Chemical Screening Methodsfor the Diagnosis of Pheochromocytoma:Norepinephrine and Epinephrine in HumanUrine. Am. J. Med., 16:310, 1954.
16. Graham, J. B.: Pheochromocytoma and Hyper-tension: Analysis of 207 Cases. Surg., Gynec.,& Obst., 92:105, 1951.
17. Hardy, J., J. McPhail and W. B. Gallagher:Pheochromocytoma; Shock Following Re-section: Notes on Mechanism with Cate-
cholamine Measurement in a Case DuringPregnancy. J.A.M.A., 179:107, 1962.
18. Healey, F. and C. Mekalatos: Pheochromo-cytoma and Neurofibromatosis. New Engl.J. Med., 258:540, 1958.
19. Kline, I. K.: Myocardial Alterations Associatedwith Pheochromocytoma. Amer. J. Path.,38:539, 1961.
20. Lund, A.: Adrenaline and Noradrenaline inBlood and Urine in Cases of Pheochromo-cytoma. Scand. J. Clin. & Lab. Invest. 4:263, 1952.
21. Miles, R. M.: Pheochromocytoma: A Reviewof Ten Cases. Arch. Surg., 80:283, 1960.
22. Molinatti, G. M., F. Camanni and A. Pizzini:Malignant Hypertension in a Case of Non-chromaffin Paraganglioma with High Con-centration of Catecholamine. Cancer, 12:878, 1959.
23. Palmieri, A. P: Pheochromocytoma in Child-hood: Case Report. Med. Ann. D. C., 29:272, 1960.
24. Phillips, B.: Intrathoracic Pheochromocytoma.Arch. Path., 30:976, 1950.
25. Richardson, J. E., J. H. Ross and A. L. Turn-bull: Reversal of Malignant Hypertensiondue to Ectopic Pheochromocytoma. Lancet,2:275, 1955.
26. Richmond, J., S. Frazer and D. Miller: Parox-ysmal Hypotension due to an AdrenalinSecreting Pheochromocytoma. Lancet, 2:904, 1961.
27. Roth, G. and W. Kvale: A Tentative Test forPheochromocytoma. Am. J. Med. Sci., 210:653, 1945.
28. Schlegel, G.: Neurofibromatosis and Pheo-chromocytoma. Schweiz. Med. Wchnschr.,90:31, 1960.
29. Sivak, G.: Pheochromocytomas of the Bladder.J. of Urology, 86:568, 1961.
30. Stephens, A.: Two Cases of Pheochromocy-toma in One Practice in One Year. Lancet,2:901, 1961.
31. Taylor, C. and V. Stoelting: Acute Hyperten-sion During Anesthesia: The UnsuspectedPheochromocytoma. J. A. M. A., 173:753,1960.
32. Von Euler, U. S.: Adrenaline and Noradrenal-ine: Pharmacol. Review, 6:15, 1954.
33. Von Euler, U. S. and G. Strom: Present Statusof Diagnosis and Treatment of Pheochromo-cytoma. Circulation, 15:5, 1957.

![Postmenopausal Vaginal Endometriotic Cyst: A …Postmenopausal Vaginal Endometriotic Cyst 3 recurrence or occurrence of de novo lesions [2]. Ovarian estro-gen secreting tumors can](https://img.dokumen.tips/doc/110x75/5f0d71af7e708231d43a62cd/postmenopausal-vaginal-endometriotic-cyst-a-postmenopausal-vaginal-endometriotic.jpg)









![Review Article TheRolesofTumor ...Tumors secreting exo-bound OVA elicit a stronger anti-OVA responseand grow slowly in vivo [45] Human ovarian cancer ascites Exo were purified from](https://img.dokumen.tips/doc/110x75/611cc6f057c6da028d32b341/review-article-therolesoftumor-tumors-secreting-exo-bound-ova-elicit-a-stronger.jpg)