Embed Size (px)
Citation preview

ARTICLE IN PRESS
Current Anaesthesia & Critical Care (2007) 18, 303–310
0953-7112/$ - sdoi:10.1016/j.c
�CorrespondiFulham Road, L
E-mail addr
www.elsevier.com/locate/cacc
FOCUS ON: INTENSIVE CARE
Secondary transfer of the critically ill patient
J.M. Handyc,�, G. Van Zwanenberga,b
aChelsea & Westminster Hospital, 369 Fulham Road, London SW10 9NH, UKbImperial College London, South Kensington Campus, London SW7 2AZ, UKcMinistry of Defence Hospital Unit Peterborough, Peterborough District Hospital, Thorpe Road,Peterborough PE36DA, UK
KEYWORDSTransfer;Transport;Physiology;Legal;Hazards;Problems
ee front matter & 2006acc.2006.11.003
ng author. Chelsea & Wondon SW10 9NH, UK.ess: j.m.handy@imperi
Summary There exist a variety of indications for transferring critically ill patientsand consequently this process is common. However despite well-documentedguidelines on appropriate conduct in such situations, critical incidents are stillcommon and the escorting personnel often lack an appreciation and understandingof the important aspects of performing safe transfers. The aim of this article is to tryand emphasize these areas and provide a basic introduction to their substance.& 2006 Published by Elsevier Ltd.
Introduction
The process of transferring critically ill patientswithin and between hospitals is increasingly com-mon. Intra-hospital transfers are most commonlyperformed to facilitate diagnostic or therapeuticinvestigations and interventions, while inter-hospi-tal (secondary) transfers may be performed for anumber of clinical or non-clinical (bed capacity)reasons. The last published national data1 esti-mated that in excess of 11,000 patients weretransferred between intensive care units (ICUs) inGreat Britain. This figure had increased by about10% on the previously published data from 8 yearsearlier.2 It is likely that this national figure hasincreased significantly since this data were pub-lished. At a regional level, the data from Northwest
Published by Elsevier Ltd.
estminster Hospital, 369
al.ac.uk (J.M. Handy).
London Critical Care Network show that during theperiod 2004–2005, 314 level-3 patients underwentsecondary transfer. This latter data were compiledfrom transfer documentation with cross-referenceto Emergency Bed Bureau (EBS) data but is stilllikely to be an under-estimate of the true numberand does not represent transfers of level-2patients.
The significance of these figures lies in the highnumber of critical incidents that have beenreported during such transfers3 and the frequencywith which transfers are undertaken for non-clinical reasons (between 50% and 66% of alltransfers). The aim of this article is not to reiteratecurrent published guidelines regarding the transferof critically ill patients,4 but to highlight thephysiological, logistical and legal problems thatcan occur when undertaking various modes oftransfer. Such aspects are seldom covered in thesmall number of publications pertinent to thistopic, and yet a basic knowledge of these facts

ARTICLE IN PRESS
J.M. Handy, G. Van Zwanenberg304
together with meticulous attention to patientpreparation prior to transfer can significantly reducethe risks to patients from such an intervention.
Transport medicine—a Cinderellasub-specialty?
There is a paucity of specific training in transferringcritically ill patients despite this being a commonoccurrence in both the National Health Service(NHS) and Private Healthcare of the United Kingdom.Knowledge and skills are taken for granted on theassumption that these must be present for theclinician to perform their day-to-day duties. Thereare increasing data, however, to show that thisassumption is incorrect. While many cliniciansperforming transfers will possess the necessaryskills that are required, they may never have beenrequired to apply these skills outside of theirfamiliar and controlled work environment and theirknowledge of the physiological, equipment andlogistical aspects of the transfer is frequentlyinadequate.
It is significant that when the transfer is theclinical focus (as with aeromedical, military anddedicated retrieval teams) ‘transport medicine’ isconsidered a sub-specialty in which clinicians mustbe educated. Such education includes a numberof areas often neglected during non-specialisttransfers:
�
Understanding the physiological effects of trans-portation. � Familiarity with equipment and environment(including the ambulance or aircraft).
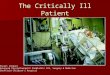
� Timing—adequate stabilization and preparation.X-axis
� Anticipation of common problems and theirsolutions—particularly communication failure. � Available modes of transport and their uniqueproblems.
Y-axis
� Legal aspects of transfer.The aim of this article is to cover the funda-mentals of some of these topics; however, it isimpossible to include the ‘hands-on’ aspects suchas equipment and ambulance familiarization whichare best achieved in the workplace or throughattending a dedicated transfer training course.
Z-axis
Figure 1 Illustration of the axes through which accel-eratory forces act relative to the human body.
Physiological effects of transfer
The process of moving patients exposes them tocertain physical forces. If these forces are mild andunder conditions of normal health, they will usually
result in minimal physiological sequelae. However,if the forces are of high magnitude and if thepatient’s ability to compensate is attenuated bycritical illness then significant physiological altera-tions can occur. These have been discussed in detailelsewhere5 but are summarized below.
The hazards to which we are exposed duringtransportation can be considered dynamic or static.
Dynamic hazards
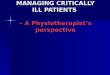
The main dynamic hazard is that of accelerationwhich may be positive or negative, linear orangular. Newton’s third law states that ‘for everyaction there is an equal and opposite reaction’.Thus when a body is accelerated due to the actionof an external force, it will experience an equaland opposite force termed ‘inertia’. This inertialforce may be experienced in the x-axis (antero-posterior), y-axis (lateral), z-axis (cephalo-caudal)or in any combination of the above (Figs. 1 and 2).The physiological effects of this inertia result fromthe displacement of solid organs and (moreimportantly) the blood, and depend upon the rate,magnitude (measured in numbers of gravities orG’s) and direction of acceleration (axis). The mostsignificant effects are seen during acceleration inthe z-axis, during which forces acting towards thefeet (resulting from accelerating the body in thefoot-to-head direction) are designated positive andthose acting towards the head, negative. Thus a+Gz force is experienced when an inertial force of

ARTICLE IN PRESS
+ Gz Inertia Force
Direction of acceleration
Figure 2 Diagram illustrating linear acceleration (solid arrows) of patient with inertial force acting in the oppositedirection (white arrow).
Secondary transfer of the critically ill patient 305
one gravity acts in the z-axis towards the patient’sfeet (Fig. 2).
When the body is exposed to +Gz forces, anymovable organ will be accelerated in the directionof that inertial force. The most important of theseis the blood. During exposure to such forces, bloodwill ‘pool’ in the feet resulting in decreased cardiacpreload, decreased cardiac output and bloodpressure. In health, the baroreceptor and vasocon-strictor reflexes will limit these effects, but suchreflexes are often obtunded or absent in thecritically ill due to illness or drug therapy. Conse-quently, hypotension may be profound, particularlyif preload is already reduced due to hypovolaemiaor positive pressure ventilation. This can beprevented by optimizing preload prior to transfer,the use of pneumatic anti-shock suits or by raisingthe patient’s legs during the acceleration (thuslimiting the vector acting in the z-axis). Generallyspeaking, ‘well-filled’ patients tolerate transferbetter than those who are hypovolaemic.
The cardiovascular consequences of exposure to�Gz forces can be predicted in the same way asabove. The most profound influencing factor duringsuch forces is the movement of blood from thelower body towards the thorax and head. Thisresults in increase in right heart pre-load with rightatrial distension. Normal compensatory mechan-isms would counter this by increasing cardiaccontractility and heart rate; however in patientswho have cardiac dysfunction or in whom compen-satory mechanisms are absent, this process mayresult in cardiac dysrhythmias, pulmonary oedemaand even cardiac arrest. Such forces are mostcommonly experienced during negative accelera-tion (deceleration), which can be of far greatermagnitude than those experienced during accel-eration. This is due to most vehicles having fargreater braking than accelerating power. Preven-tion is best achieved by limiting hard braking andhaving head-up tilt during transfer. On the whole,the potential physiological derangements fromdeceleration are greater than those from accelera-tion due to the greater forces experienced and sohead-up positioning is optimum. This has the effect
of limiting the Gz forces exerted on the thorax andhead during linear acceleration and deceleration.
The neurological effects of +Gz exposure havebeen well documented through military aviationstudies,6,7 and although these effects are unlikelyduring patient transfers it may be impossible toassess their effects accurately in an unconsciouspatient. The pooling of blood in the lower body andfeet results in reduced blood supply to the brain. Inhealth, progressive +Gz exposure will lead to loss ofperipheral vision (grey-out), loss of vision withconsciousness maintained (black-out) and completeloss of consciousness (G-LOC). Significantly, sei-zures have been reported on return of blood supplyto the brain after cessation of these forces.Although the symptoms of reduced supply maynot be recognized in an unconscious patient, it isimportant to have an appreciation of the risks thismay pose and also of the possibility of convulsionsonce this situation reverses. These effects can beprevented through the same actions used toprevent the cardiovascular effects of +Gz forces.The exception to this is the use of a Valsalvamanoevre (taught to military pilots to counteractgrey-out, black-out or G-LOC), which reduces theloss of blood volume from the brain due to theincrease in intra-thoracic pressure. This does,however, exacerbate the subsequent cardiovascu-lar effects.
Contrary to the above situation, the neurologicaleffects of �Gz forces have been less well studieddue to the extreme discomfort experienced whenhealthy individuals are exposed to forces greaterthan �1Gz for any prolonged period of time. Theeffects of �1Gz are those experienced whenhanging upside-down. Prolonged exposure to thisor higher forces has resulted in a condition of ‘red-out’ whereby vision becomes red due to bloodengorgement or the lower eyelid being forced overthe pupil. Haemorrhages have been reported inboth retina and brain following such forces, but themost important effect is to increase intra-cranialpressure (ICP). This can have potentially devastat-ing effects in patients with critical brain injury andexisting compromised cerebral blood flow. In such

ARTICLE IN PRESS
J.M. Handy, G. Van Zwanenberg306
situations, an increase in ICP can result in criticalreduction in blood flow resulting in cerebralischaemia. The main mode of prevention in thissituation is again to keep the patient in the head-upposition and to limit positive and negative accel-eratory forces as much as possible.
The most significant effect of acceleration on thegastrointestinal system is that of gastro-oesopha-geal reflux during exposure to �Gz forces. This isbest prevented by intubating the stomach andaspirating the contents at appropriate moments,or simply maintaining free drainage into a collec-tion bag.
In addition to the effects described above,consideration must be given to the potential axialloading effect that Gz forces have on the verteb-rae. This can be significant when transferringpatients with unstable vertebral fractures andagain emphasizes the point that, where possible,a smooth transfer is the safest transfer.
Finally, it is important to emphasize that theforces described above will act on any equipmentor objects that are inadequately immobilized,turning them into ballistics. An extreme exampleof this was seen by the London Ambulance Service(personal communication) when a 90 kg incubatorbecame mobile while the ambulance carrying itwas travelling at high speed. Such occurrencescan prove extremely dangerous to patient andescorts alike.
Static hazards
The main static hazards to which we are exposedduring transportation are:
�
noise, � vibration, � temperature, � atmospheric pressure.While noise can cause significant difficulties withcommunication during transfers, and vibration andtemperature alterations can be significant andpotentially damaging, it is the latter of these thatwill be considered in most detail here. Thedamaging effects of vibration can be reduced bypaying meticulous attention to padding and pro-tecting any areas of the patient in contact withhard objects. The most common temperatureconsideration is that of hypothermia, particularlywhen travelling in vehicles or aircraft that are opento the environment or lack heating facilities. Insuch situations, arrangements must be made to
provide adequate warming for the patient and toprevent heat loss.
Atmospheric considerations are only really ofrelevance during air transfers, where the reductionin ambient pressure (even in pressurized aircraft)results in relative hypoxia and expansion of gas-filled cavities. The hypoxia at altitude needs to beaccounted for in calculating oxygen requirementsfor the transfer: higher inspired oxygen fractionmay be required than that used on the ground andthus oxygen consumption during the flight may begreater than would otherwise be predicted.
The important gas-filled cavities to consider arelisted below:
�
ears, � sinuses, � teeth, � bowels, � pleura, � blood, � equipment.In any of the above cavities, loss of communica-tion with the environment results in inability toequalize with the ambient pressure thus creating apressure gradient. This can result in problemsranging from discomfort (ears, sinuses, teeth) tolife-threatening (perforated bowel, pneumothorax,gas embolism). The effect on the cavity will dependon its rigidity, contents and whether the pressuregradient develops at altitude or at ground level.For example the Eustachian tube connecting themiddle ear to the pharynx is a non-rigid structure,which is expanded during aircraft ascent due to thegas in the middle ear expanding. Thus communica-tion is maintained with the external environmentand gas equilibration occurs. However on descent,the pressure gradient reverses and the tube cancollapse preventing communication. This causesthe gas within the middle ear to contract and thetympanic membrane to be pulled inwards. It is forthis reason that tympanic membrane rupturesoccur most frequently during descent rather thanascent.
Any gas containing equipment or drugs willexhibit the same phenomena described above,with gas expansion during ascent and contractionduring descent. This is most frequently seen withpressure bags used to assist infusion of intravenousfluids or flush lines. During ascent, care should begiven to prevent rupture by reducing the pressureappropriately. Conversely during descent, the bagmay require re-inflation.
Less obvious than the above, but more importantis to remember that the cuff on the tracheal tube

ARTICLE IN PRESS
Secondary transfer of the critically ill patient 307
will expand during ascent and this may result intracheal mucosal damage, or cuff rupture. The bestway to prevent this is to fill the cuff with sterilewater or saline. This prevents the need to decreasethe cuff volume during take-off and re-inflateduring landing.
Figure 3 An example of a dedicated transfer trolley.
Common problems during transfer—‘‘If itcan go wrong it will go wrong’’
There are several phases of the transfer which canbe examined. Appendix 4 of the ICS guidelines4
suggests breaking your preparation into patient,staff, equipment, organization and departure. As apre-departure check-list, this is a useful toolutilized in many regional transfer forms in theUnited Kingdom. Sadly these are often poorlycompleted and unfamiliar to the transferring team.The transfer check-list and preparation requires ateam approach in advance of the transfer takingplace. Poor haemodynamic preparation for pre-dictable physiological changes will result in thedeterioration of the patient in transit. Withoutrobust equipment servicing schedules and equip-ment maintenance, discovery that an infusiondevice, running on battery, is not at optimalcapability occurs when it is disconnected from themains supply. Prevention of anticipated problems isoptimized if preparation for transfers takes placeevery day. Emphasis must be placed on theimportance and rationale for equipment checksespecially on items usually in storage. Transfer bagsneed to be checked and signed for daily, userchecks must be carried out on all equipment dailyand battery charge status and that of spares needsto be recorded.
Intra-hospital transfer needs to be given thesame importance as that of inter-hospital transfer.Therefore whether going to CT scan or to anotherhospital, the preparation and equipment should bethe same. This provides the cultural and organiza-tional change to ensure that it becomes routine.Few secondary transfers require urgent departureand the transfer itself should only require a fewobservations, vigilance and monitoring of thepatient. This is usually the sign of a well-preparedtransfer. The following provides additional informa-tion and preparation that may prevent problems.
Patient
It is common to wait for the transportation vehicleto arrive before connecting the patient to thetransfer equipment. However this often delays both
departure and identification of any problems withthe equipment. It is useful to monitor and ventilatepatients on the appropriate transfer equipment(using piped oxygen and mains-electricity) for aprolonged period of time so that when thetransportation crew arrives time is saved andproblems have been rectified. The ‘packaging’ ofthe patient can also be done prior to the crewarriving. Attention should be paid to which direc-tion to slide the patient and which side the lines areorientated; the patient will be head first with theirleft side up against the side of the ambulance.Critical care trolleys with space for equipment willspeed up the total time of a transfer (Fig. 3).Temperature loss can be reduced by insulating thepatient’s head and torso with gamgee or blankets.Eye protection should be considered if the lids donot close completely and ear defenders should beused for rotary air transfer. Analgesia should beconsidered as ambulance trolleys have no suspen-sion and the journey may cause significant dis-comfort to the patient.
Staff
Transfer training and experience is desirable.Handover should be done at the earliest opportu-nity and, most importantly, preparation for thetransfer should be done well in advance of thetransfer occurring. The individual performingthe transfer is responsible for appropriate prepara-tions and failure to perform relevant checks willrender them liable. An appropriate transfer mottois ‘assume nothing and trust no-one’!
Equipment
Drugs: The duration of the transfer should beestimated and used to calculate drug, oxygen and

ARTICLE IN PRESS
J.M. Handy, G. Van Zwanenberg308
battery requirements. Where possible, the chan-ging of infusions mid-journey should be avoided. Itis worth establishing a plan for all eventualities. Forexample, what should be done if the inotropeinfusion pump becomes faulty? In all circum-stances, drug infusions should be rationalized. Ifan infusion is continued, such as insulin, it shouldbe considered essential and monitored during thetransfer. In the event of infusion pump failure,sedative and neuromuscular blocking drugs canoften be given as boluses thus freeing a pump forother infusions requiring accurate administration.
Ambulance equipment: Oxygen and defibrillatorsare carried on the ambulance and the ambulancecrew should be contacted if these are desired forthe transfer to and from the vehicle. Knowledge ofthe ambulance equipment is essential but in realitythe clinicians performing the transfer should beself-sufficient.
Transfer bag: Appendix 1 of the ICS guidelineslists recommended items for the kit bag includingHeimlich valves for chest drains. In general,contents should be kept to the minimum required.Individuals should be familiar with these contentsand remember to take emergency items such asmoney, a mobile phone (with appropriate numbers)and something to eat and drink in the event of along transfer or delay.
Airway bag: In the event of an airway emergency,there is no substitute for having an ‘ambu-bag’ withsimple airway adjuncts, a laryngoscope and spareendotracheal tube contained in a transparent bagand secured to the head-end of the patient’strolley. Most disposable ‘ambu-bags’ are suppliedin a transparent bag with draw-string, which caneasily be used for the above. In the event oftracheostomy decannulation, rapid insertion ofan endotracheal tube through the stoma can belife-saving and avoids the need for hasty attemptsto access an appropriate replacement tracheo-stomy tube.
Oxygen: This is the most important drug that wecarry during transfers. To run out is always a littleembarrassing; especially when travelling long-haulat 35,000 feet! Modern transfer ventilators willindicate oxygen consumption allowing ‘worse case’calculation of necessary oxygen requirements. It isprudent to carry 150% of this requirement to allowfor unforeseen situations and delays.
Organization
Communication failure is often the root cause ofmishaps. Organizational issues rely upon soundwritten and verbal communications and one in-
dividual should be responsible for coordinating thetransfer. The nurse is often the most appropriateteam leader, as equipment competencies andknowledge of the unit transfer procedures will bepart of their ongoing professional education. Thisallows the other escort to concentrate on note-making, referral letters, discussion with relativesand liaising with other clinicians at receivinghospitals. It is always important to identify theteam leader and keep them appropriately in-formed.
Finally, a plan for the return journey shouldalways be made from the outset in the event of thetransferring ambulance crew being diverted else-where.
Departure
At the time of departure all check-lists should becomplete. One of the most frequent communica-tion errors is failure to inform the receiving teamthat the referring team is about to leave. Whilemaking this call it is worth checking the exactdestination and how the ward is accessed via thehospital (e.g., via the Emergency department ormain entrance). The transfer form and check-listprovide documentation of adequate preparation,and their completion after handover to the receiv-ing hospital team completes the legal record of thetransfer.
Modes of transfer
There are several factors to consider when select-ing a mode of transport:
�
speed, � distance, � availability, � clinical condition, � training, � cost.Road ambulance
The ideal road transfer should be slow and steady.It is exceptionally rare for secondary transfers torequire anything other than steady driving withminimal braking and accelerating; if necessary, thisshould be facilitated by the use of blue lights andsiren to clear obstructing traffic. It is rare torequire a police escort, and such situations providedifficult and demanding circumstances for theambulance driver: in the event of an accident,

ARTICLE IN PRESS
Secondary transfer of the critically ill patient 309
the lead clinician needs to be able to justify suchactions.
Advantages of road ambulance:
�
low cost, � rapid mobilization, � purpose built, � familiarity, � door to door, � few weather restrictions.Disadvantages:
�
long journey time, � acceleration, � deceleration, � travel sickness often for staff.Helicopter and fixed-wing transfer
Advantages:
�
speed, � reach.Disadvantages:
�
Cramped environment. Access to patients can belimited. � Noisy. � Vibration. � Altitude. � Number of transfers: as with fixed wing trans-fers, rotary transfers usually come with a ‘3 forthe price of 1’ offer. Both fixed-wing and rotarytransfers often require the use of local air-strips(unless helipads are available) and a roadambulance transfer will thus be required at eachend of the air transfer. This requires consider-able coordination and presents many possibili-ties for communication error.
� Training: this is expensive. � Poor-preparation: there is no leeway for this.Forgotten or faulty equipment is not readilyreplaced.
Top tips
�
A transfer wallet that will accommodate scansand radiographs is extremely useful. On the frontof the wallet should be a laminated check-list ofwhat needs to be inside, handover notes, scans,patient valuables, etc., which can be reused forsubsequent transfers.�
Loss of PEEP while transferring ventilation fromone machine to another can be avoided byclamping the endotracheal tube with a softclamp prior to disconnection and unclampingonce reconnection and commencement of gasflow occurs. � If the transfer team has to return by taxi, it isimportant to note that only vehicles displaying agreen compressed gas sticker and license cancarry compressed gas cylinders. Thus it is best toleave any cylinders at the receiving hospital,remembering to disconnect the regulator andthe ventilator adaptor. If the regulator andadaptor are left behind, they will not beavailable for subsequent patient transfers.
� If the transfer monitor records observations,these can be printed in order to avoid writing inthe back of an ambulance.
� The use of helicopters for secondary transfershould be minimized.
� Training and familiarity are the most significantissues. An increasing number of regional trainingcourses are being developed.
� Many of the problems would be solved if transferforms were available and utilized.
� Network solutions can make the process oftransfer much smoother (e.g., standardizedtransfer trolleys (Fig. 3)).
Legal, insurance and safetyconsiderations
There are numerous legal conundrums when trans-ferring and retrieving patients and yet there is alack of case-law to provide appropriate solutions.Generally speaking the most important aspect ofthe transfer process is to maintain the sameprofessional and personal conduct that would beconsidered ‘good clinical practice’ in the normalworking environment. The Consultant in charge ofthe ICU transfer must take ultimate responsibilityfor the appropriateness of the transfer, withadequately trained and experienced staff. Thepatient remains the responsibility of these staffuntil formal handover has been completed at thereceiving hospital, with the legal record of thetransfer process being an essential piece ofdocumentation. In the event of advice beingoffered by telephone, little legal guidance isavailable. Certainly the individual administeringdrugs and providing the bedside care has anobligation to question and defer advice if they feelthat to act on it would be of detriment to thepatient. Telephone advice is simply guidance and is

ARTICLE IN PRESS
J.M. Handy, G. Van Zwanenberg310
only as valid as the information that was receivedand utilized in formulating that advice; thus, thereis inevitable potential for communication errorsand subsequent ‘finger-pointing’, should harmcome to the patient. This stresses the importanceof stating and ensuring clear and precise instruc-tions when giving and receiving telephone advice,with appropriate documentation and records.Several retrieval centres in the United Kingdomutilize hard-drive recordings of all telephoneconversations where medical information is ex-changed in order to keep adequate legal records. Inthe event of an individual being required to escorta patient outside of their place of employment,personal and professional indemnity will be pro-vided by the employing Trust provided the indivi-dual is a member of the Trust’s ‘Liabilities to ThirdParties Scheme’ (LTPS). In essence, the transfervehicle and route becomes an extension of thatindividuals work environment for the duration ofthe transfer and return, provided this is spentperforming Trust duties. Individuals performinghigh volume retrievals and transfers may feelbetter ‘protected’ through the insurance providedto members of institutions such as the Intensive CareSociety of the United Kingdom and the Associationof Anaesthetists of Great Britain and Ireland.
The safety of performing transfers has beenbrought into question. Accidents have occurredduring the transfer process itself and during allmodes of transfer. One report from the UnitedStates highlighted the deaths of sixty air ambulanceteammembers as a result of 84 crashes over a 5-yearperiod.8 Such data emphasize the importance ofjustifying such transfers; if transfers are deemedessential, they should be performed in a sedate andcareful manner in order to avoid risks to thoseinvolved. High-speed transfers should be the excep-tion, not the norm. The few minutes gained rarelybenefit the patient but expose the transferring teamto significant potential risks; individuals requestingsuch transfers must be able to justify these risks.
Summary
Adequate preparation, communication and antici-pation of potential problems are the key to
performing safe transfers for critically ill patients.Despite these measures, the nature of the patientgroup dictates that incidents will happen; the dutyof the transfer team is to ensure that such incidentsare not directly attributable to the transferprocess. After equipment problems, communica-tion errors are the most common incidents empha-sizing the need to standardize the process andutilize transfer documentation as an aide-memoir.In short: If it can go wrong, it will go wrong. Assumenothing and trust no-one!
Acknowledgements
We would like to thank Ms. Angela Walsh (NetworkDirector) and Mrs. Ann Ashworth (Service Improve-ment Lead) of Northwest London Critical CareNetwork for the use (with permission) of theirtransfer data in this article.
References
1. Mackenzie PA, Smith EA, Wallace PG. Transfer of adultsbetween intensive care units in the United Kingdom: postalsurvey. Br Med J 1997;314(7092):1455–6.
2. Wright IH, McDonald JC, Rogers PN, Ledingham IM. Provisionof facilities for secondary transport of seriously ill patients inthe United Kingdom. Br Med J (Clin Res Ed) 1988;296(6621):543–5.
3. Lovell MA, Mudaliar MY, Klineberg PL. Intrahospital transportof critically ill patients: complications and difficulties.Anaesth Intens Care 2001;29(4):400–5.
4. Whiteley S, Gray A, McHugh P, O’Riordan B. Guidelines for thetransport of the critically ill adult. Standards and guidelines.Intensive Care Society, 2002.
5. Handy J. The physiological effects of transferring critically illpatients. Clin Intens Care 2005;16(2):65–9.
6. A hazard in aerobatics: effects of G-forces on pilots. Advisorycircular 1984: retrieved 18.04.2005; Available at /www.faa.gov/avr/afs/ac91-61.txtS.
7. Houghton JO, McBride DK, Hannah K. Performance andphysiological effects of acceleration-induced (+Gz) loss ofconsciousness. Aviat Space Environ Med 1985;56(10):956–65.
8. Levin A, Davis, R. US report: air ambulance crashes hitrecord. Paramedic UK July 2005: retrieved 24.02.2006;Available at /http://www.usatoday.com/news/nation/2005-07-17-air-ambulance-crashes_x.htmS.