Upload
ferdi151991
View
45
Download
2
Tags:
Embed Size (px)
DESCRIPTION
Medical Journal
Citation preview
Review
Scleral structure, organisation and disease. A review
Peter G. Watsona,*, Robert D. Youngb
a17 Adams Road, Cambridge CB3 9AD, UKbBiophysics Group, Department of Optometry and Vision Sciences, Cardiff University, Redwood Building, King Edward VII Avenue,
Cardiff, Wales CF10 3NB, UK
Received 25 June 2003; accepted 26 June 2003
Abstract
Although disease of the sclera is unusual, when it occurs it can rapidly destroy both the eye and vision. However, normally the sclera
provides an opaque protective coat for the intraocular tissues and a stable support during variations in internal pressure and eye movements,
which would otherwise perturb the visual process through distortion of the retina and the lens/iris diaphragm. This stability, which is vital for
clear vision is made possible by the organisation and viscoelastic properties of scleral connective tissue. Microscopically, the sclera displays
distinct concentric layers including, from outside, Tenons capsule, episclera, the scleral stroma proper and lamina fusca, melding into
underlying choroid. Two sites exhibit specialised structure and function: the perilimbal trabecular meshwork, through which aqueous filters
into Schlemms canal, and the lamina cribrosa, which permits axons of the optic nerve to exit the posterior sclera. Throughout, sclera is
densely collagenous, the stroma consisting of fibrils with various diameters combining into either interlacing fibre bundles or defined
lamellae in outer zones. Scleral fibrils are heterotypic structures made of collagen types I and III, with small amounts of types V and VI also
present. Scleral elastic fibres are especially abundant in lamina fusca and trabecular meshwork. The interfibrillar matrix is occupied by small
leucine-rich proteoglycans, decorin and biglycan, containing dermatan and dermatan/chondroitin sulphate glycosaminoglycans, together
with the large proteoglycan, aggrecan, which also carries keratan sulphate sidechains. Decorin is closely associated with the collagen fibrils at
specific binding sites situated close to the C-terminus of the collagen molecules. Proteoglycans influence hydration, solute diffusion and fluid
movement through the sclera, both from the uvea and via the trabecular meshwork. As the sclera is avascular, nutrients come from the
choroid and vascular plexi in Tenons capsule and episclera, where there is an artery to artery anastomosis in which blood oscillates, rather
than flows rapidly. This predisposes to the development of vasculitis causing a spectrum of inflammatory conditions of varying intensity
which, in the most severe form, necrotising scleritis, may destroy all of the structural and cellular components of the sclera. Scleral cells
become fibroblastic and the stroma is infiltrated with inflammatory cells dominated by macrophages and T-lymphocytes. This process
resembles, and may be concurrent with, systemic disease affecting other connective tissues, particularly the synovial joints in rheumatoid
arthritis. Current views support an autoimmune aetiology for scleritis. Whilst the role of immune complexes and the nature of initial pro-
inflammatory antigen(s) remain unknown, the latter may reside in scleral tissue components which are released or modified by viral infection,
injury or surgical trauma.
q 2003 Elsevier Ltd. All rights reserved.
Keywords: human sclera; review; structure; collagens; proteoglycans; vasculature; innervation; development; aging; inflammatory diseases
1. Introduction
The human sclera, although relatively inert metaboli-
cally, is a remarkable structure which performs several
important functions essential for the visual integrity of the
eye. Primarily, the sclera provides a firm substrate for the
delicate intraocular contents and protects them from injury.
Its opacity ensures that internal light scattering does not
affect the retinal image. In addition, it facilitates rotation of
the eyeball without significant distortion through nearly
1808 by powerful muscles. The shape of the eye is, in part,maintained by the presence of the intraocular contents and
the intraocular pressure. However, the sclera must be rigid
enough to provide relatively constant conditions so that,
when the eyeball is moved, the intraocular pressure does not
fluctuate and adversely affect vision. Scleral deformation
would impair vision not only because of wrinkling of the
retina itself, but also through irregular distortion of the lens
0014-4835/$ - see front matter q 2003 Elsevier Ltd. All rights reserved.
DOI:10.1016/S0014-4835(03)00212-4
Experimental Eye Research 78 (2004) 609623
www.elsevier.com/locate/yexer
* Corresponding author. Dr Peter G. Watson, 17 Adams Road,
Cambridge CB3 9AD, UK.
E-mail address: [email protected] (P.G. Watson).
iris diaphragm. Theoretically the functional requirements of
the sclera could be satisfied by a rigid globe, but they have
been achieved in different ways throughout the animal
kingdom. In most animals the globe is circular, the sclera
thin and of even thickness throughout its circumference, but
often supported with cartilage or even bone. It is possible
that the less rigid fibrous structure of the sclera in mammals
allows a more even distribution of the blood supply to the
choroid, and thence the retina, during the large excursions of
voluntary ocular movement. Optical stability is achieved
through the balance of intraocular pressure and the
curvatures of the sclera/corneal envelope. This relationship
is so constant that it can be relied on when the power of a
surgically implanted lens is calculated. Certainly, softening
of the eye, for example through injury or inflammation, can
lead to a disproportionately greater visual loss than might be
expected from the distortion of the intraocular contents
alone. Conversely, when patients with dysthyroid ophthal-
mopathy look upwards, their intraocular pressure rises
because of the pressure of the rigid rectus muscles on the
globe and, in some cases, this is accompanied by a dramatic
fall in vision. However, scleral folding on its own does not
usually affect vision unless the macula is involved, as can be
seen sometimes after retinal detachment surgery when the
intraocular pressure is normal.
The sclera is able to fulfill these functions owing to the
unique microscopical structure and arrangement of protein
and carbohydrate molecules, which interact to form its
connective tissue matrix. In common with other connective
tissues, the sclera may also succumb to immuno-inflamma-
tory diseases which degrade its components. In these, and
surgical procedures involving access to the intraocular
contents via incision of scleral tissue, the potential of the
sclera for regeneration and repair is crucial for the healthy
eye. It is perhaps therefore surprising that the human sclera
remains such an under-researched structure. Many of the
new discoveries relating to connective tissue composition
and organisation have come from studies on cornea, tendon
and cartilage. In this article, we review current knowledge
on the structure of the human sclera, make reference where
applicable to new evidence from studies on other tissues and
comment briefly on contemporary aspects of scleral disease
processes and repair.
2. Anatomy of human sclera
The sclera comprises five-sixths of the outer tunic of the
eye extending posteriorly from the corneal perimeter to the
optic foramen, perforated by the optic nerve. It is
approximately spherical with an average vertical diameter
of 24 mm. The thickness of the adult human sclera is not
uniform. It is thickest at the posterior pole (1135 mm),
decreasing gradually to 0406 mm at the equator and
thinnest under the recti muscles (03 mm), increasing again
to 06 mm, where the parallel shiny tendon fibres merge
with the scleral collagen. From the insertion of extraocular
muscles towards the limbus, the sclera gradually increases
in thickness up to 08 mm, where it blends with the cornea.
Women have slightly thinner sclera than men. There is also
an increase in scleral thickness, together with opacity, in
relation to age.
Opaque, yellowish-white sclera merges with transparent
cornea across an intermediate zone extending about 2 mm,
termed the limbus. Here, a sulcus is formed owing to the
higher radius of curvature of cornea than the sclera.
However, this is not readily visible as it is filled in by
overlying episclera and conjunctiva. The sclera encroaches
slightly more into the cornea in superior and inferior
quadrants than it does laterally (corneal horizontal axis:
116 mm; vertical axis: 106 mm), but the internal diameter
of the so-called scleral foramen is circular at 116 mm.
Thus, the posterior edge of the scleral sulcus is almost
parallel to the optic axis laterally, but lies obliquely
elsewhere. Two vascularised fascial layers invest the outer
surface of the sclera: Tenons capsule and the episclera.
2.1. Tenons capsule (Fascia bulbi)
Tenons capsule is identified as a distinct hypocellular
layer of radially-arranged, compact collagen bundles
running parallel to the scleral surface. At its anterior origin
in the limbus, the capsule is firmly attached to overlying
conjunctival tissue and the episclera below. About 3 mm
from the limbus, it thickens and becomes freely mobile over
the underlying episclera to which it maintains attachment
via fine interconnecting trabeculae. It extends from the
limbus backwards to ensheath the rectus muscles and
becomes continuous with their perimysium. The importance
of Tenons capsule as a muscle pulley for the extraocular
muscles, particularly in relation to strabismus, where
collagen fibrils in the capsule show increased diameter
and packing density (Shauly et al., 1992), was recently re-
emphasised (Roth et al., 2002). Continuing posteriorly as a
simple condensation of collagenous fibres, it probably
merges with the dural sheath of the optic nerve and with
fibrous bands connecting the eyeball to the orbit. Tenons
capsule lies anteriorly between two vascular layers, the
conjunctival plexus and the episcleral plexus, both of which
nourish it. Ramifications of the anterior ciliary vessels
course throughout the matrix with the veins running
superficially and the arteries coming close to the surface
only near the limbal arcade. Towards the equator poster-
iorly, a fine tenuous network of vessels runs in this tissue
from the posterior ciliary arteries.
2.2. Episclera
The episclera is a thin and dense, but well-vascularised
layer of connective tissue, with fibres blending impercept-
ibly with the underlying stroma of the sclera itself. In
contrast with Tenons capsule, the bundles of collagen are
P.G. Watson, R.D. Young / Experimental Eye Research 78 (2004) 609623610
circumferentially arranged with tight attachments to the
walls of the blood vessels, preventing its independent
movement over the sclera. The attachments to Tenons
capsule are dense near the limbus and weaken progressively
towards the equator, where the episclera is bound to the
capsule only by very thin bands of collagen. A small amount
of elastic tissue can be found in the episclera together with
melanocytes and a few macrophages. A few myelinated and
unmyelinated nerve fibres also ramify within the episclera
terminating mostly around the vessels.
2.3. Scleral stroma
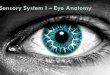
The strength and resilience of the scleral stroma is
achieved by bundles of parallel-aligned collagen fibrils, in
superficial sites grouped into dense superimposed lamellae,
which run mostly parallel to the surface of the eyeball
(Fig. 1). The majority of bundles exhibit a circular
orientation, but lie meridionally at the limbus (Hogan
et al., 1971). In contrast to cornea, scleral lamellae branch
and interlace extensively and exhibit wide-ranging dimen-
sions, up to 50 mm wide and 6 mm thick (Komai and Ushiki,1991). Increased interweaving and density of fibres replaces
the lamellar arrangement in the deep sclera, while scattered
elastic fibres are present between and within the collagen
bundles throughout the stroma. Tendon fibres of the
extraocular muscles intermingle with the scleral fibres,
extending anteriorly as far as the limbus. The innermost
layer of the sclera adjacent to the uvea is known as the
lamina fusca. In this region the collagen bundles are again
smaller and branch extensively to blend into the underlying
choroidal stroma. The sclera is traversed by blood vessels
and nerves. Anterior ciliary vessels penetrate anterior to
the rectus muscles while long and short posterior ciliary
vessels, vortex veins and nerves enter posterior to the
muscles.
This tissue organisation provides the sclera with
considerable visco-elastic properties. Indentation of the
tissue initially causes a rapid lengthening of fibres and a
rebound, followed by a slow stretching on prolonged
pressure. It also confers strong tensional properties
consistent with the requirement to resist the stresses and
strains imposed on it by the extraocular muscles. Scleral
visco-elasticity protects the eye from injury during transient
elevations of intraocular pressure. This is evident when
pressure is raised artificially by injecting fluid into the eye,
the pressure will rise rapidly and then gradually fall to its
original level without significant distortion of the eye. An
initial lengthening of the fibres is followed by slow sliding
of the fibres one upon another (Friberg and Lace, 1988); the
amount of stretch is not directly proportional to the change
in pressure, rigidity increasing as the fibres are stretched.
2.4. Scleral spur
Superficial fibres of the sclera blend with the episcleral
fibres at the limbus. The deep fibres condense in a ring to
form the scleral spur, which is an important anatomic
landmark, recognised by all ophthalmic surgeons in relation
to post cataract astigmatism. This rigid ring structure,
together with the corneal annulus, which is formed by a
circumferential swathe of limbal fibrils originating in the
cornea (Newton and Meek, 1998), probably accounts for the
stability of the corneal contour. The trabecular tissue is
inserted into the scleral spur anteriorly and it receives the
longitudinal part of the ciliary muscle posteriorly. The
collagen fibres of the scleral spur, which are continuous with
the fibres of the corneoscleral trabecular meshwork,
Fig. 1. Outer layers of normal, supero-temporal sclera from 40-year-old man showing lamellar structure. Collagen fibrils are present in longitudinal (Lc),
transverse (Tc) and oblique section (Oc) and exhibit wide variation in diameter. A fibrocyte (F) and elastin fibre (E) are also visible. Bar represents,15 mm.From Wolffs Anatomy of the Eyes and Orbit, 8th Ed., A.C. Bron, R.C. Tripathi, B.J. Tripathi, 1997. Reproduced by permission of Hodder Arnold.
P.G. Watson, R.D. Young / Experimental Eye Research 78 (2004) 609623 611
increase in size from 40 nm in the trabecular sheets to 80 nm
close to the sclera, so that the scleral spur feels firm under
surgery. The inner layers, the so-called scleral roll, surround
Schlemms canal in its whole circumference.
From the posterior end of Schlemms canal a small
circumferential band of scleral fibres projects towards the
anterior chamber. This is the part of the scleral spur to which
the meridional fibres of the ciliary muscle are attached. The
fine anterior tips of the ciliary muscle form a tendinous
structure inserting into the posterior part of the scleral spur
and hence into the trabecular meshwork. This tendon has the
same composition as the trabecular beams and consists of
collagen and elastin. It is through this connection that
contraction of the ciliary muscle can pull on the scleral spur
opening the trabecular meshwork. The rigidity of the scleral
spur may also help prevent closure of the trabecular
meshwork when the ciliary muscle relaxes (Hamanaka,
1989).
2.5. The limbus
Overlying the trabecular zone, across the limbus, a
gradation of changes in the matrix reflects the transition
from sclera to cornea in an ill-defined region, 12 mm in
width. The changes in tissue structure, composition and
biomechanical properties at this site also incur increased
susceptibility to injury and disease. Fibrils of the deep sclera
extend beyond the trabecular bands running across the
limbus to the region of Descemets membrane traversing,
and some interacting with, the circumcorneal annulus of
fibrils (Newton and Meek, 1998). The limbus is of
importance not only as the translucent surgical landmark,
but also because of the unusual cellular composition and the
presence of stem cells within the tightly adherent con-
junctival and episcleral tissues which overly it. It is from
this region that new corneal epithelium is derived and
because of the high content of antigen presenting cells in
this tissue, it is of major importance in the immunological
changes which occur in both sclera and cornea during
inflammation.
2.6. Posterior sclera
The posterior sclera is perforated 3 mm medial to the
midline and 1 mm below the horizontal by the optic nerve.
The aperture is cone-shaped, being 2 mm wide on the
internal surface and 35 mm externally. Posteriorly the outer
two thirds of the scleral fibres are continuous with the dural
sheath of the optic nerve and the rest form the lamina
cribrosa, a collagenous scaffold supporting the optic nerve.
Multiple openings, lined by bundles of scleral fibres covered
by glial tissue, form short canals that provide a passage for
the axons of the optic nerve. One of the openings in the
lamina is larger than the rest and contains the central retinal
artery and vein. The collagen fibres are vertically arranged
and condensed as septa, already present in the 160 mm
embryo, where the nerve fibre bundles pass through them
(Anderson, 1969). There is no doubt that structural
abnormalities in the lamina cribrosa contribute to the
collapse of the collagenous framework of the optic disc,
associated with the cupping which occurs in glaucoma.
However, considerable debate continues on the respective
importance of collagen remodelling, raised intraocular
pressure, ischaemia and other factors in the aetiology of
this disease.
A better understanding of matrix turnover in the posterior
sclera could also help explain the changes found in
progressive myopia and in some cases of low tension
glaucoma in which the disc head collapses. Inflammatory
oedema of the sclera in the region of the optic disc leads to
strangulation of the nerve fibres and blood vessels, as they
run in fibrous channels within the scleral tissue. These
fibrous channels penetrate the sclera at three main sites:
around the optic nerve, for the passage of the long and short
posterior ciliary vessels and nerves; 4 mm behind the
equator for the venae vorticosae; and between the limbus
and the muscle insertions, for the transmission of the
anterior ciliary vessels, nerves and perivascular lymphatics.
3. Blood supply and lymphatics of the sclera
and episclera
The sclera has a low metabolic requirement because of
the slow turnover of the collagen of which it is composed.
The scleral stroma receives no blood capillaries in the
normal healthy state, although the long posterior ciliary
arteries and nerves and the vortex veins pass through it in
fibrous canals. The stroma derives its nutrition from the
episcleral and choroidal vascular networks. Similarly,
inflammatory cells infiltrating the sclera come from both
of these sources. The reason for this total absence of direct
blood supply and the reluctance of new blood vessels to
enter the sclera even after injury is obscure and
unresearched.
The episclera and Tenons capsule derive their blood
supply from the anterior ciliary arteries and the long
posterior ciliary arteries posteriorly, with some contribution
from the conjunctival arteries at the limbus. These major
vessels contribute to the episcleral arterial circle, an often
incomplete arterial network situated about 4 mm from the
limbus (Morrison and Van Birskirk, 1983). The episcleral
arterial circle in turn contributes to the limbal arcade of
vessels. This unusual artery to artery anastomosis ensures
that the anterior segment of the eye is always supplied with
blood whatever the pressures on the globe may be. It does,
however, have the disadvantage that, in the regions between
the rectus muscles, arterial blood may not flow through the
vessel, but rather oscillate within it (Meyer, 1988). As a
consequence, extravasation of fluid or cells in the region of
these vessels stagnates and creates conditions in which
immune reactions can readily occur. In the posterior
P.G. Watson, R.D. Young / Experimental Eye Research 78 (2004) 609623612
segment, both the episcleral tissue and the overlying
Tenons capsule are thin, which results in relative
avascularity of the superficial layers of the posterior sclera.
There are well-formed lymphatic channels in conjunc-
tiva, but they are absent in the episclera and sclera, although
it has been suggested that spaces between fibre bundles
might enable the sclera itself to act as a lymphatic medium.
The conjunctival lymphatic channels are in two layers, a
well formed superficial network and a network of channels
adjacent to Tenons capsule (Bussacca, 1947). Lymph from
the superficial episcleral tissue drains into the subconjunc-
tival space and thence to the parotid node nasally and to the
submandibular nodes temporally. Lymph from elsewhere in
the sclera and episclera passes into the orbit via the
perivascular space around the veins to empty into the
jugular lymph trunks and the deep cervical nodes.
4. Nerve supply of the sclera
The nerve supply of the sclera is surprisingly rich for a
structure whose main function would appear to be
supportive. Consequently, inflammation of the sclera is
extraordinarily painful, owing both to direct stimulation of
the nerve endings by the inflammatory process and to
distension and stretching of the nerve bundles from tissue
swelling and cellular infiltration.
The primary nerve trunks divide and redivide to emerge
in the episclera as single nerve endings. The nerve supply of
the posterior sclera is derived from the short ciliary nerves,
where they enter the sclera close to the optic nerve.
Anteriorly, it is derived from branches of the long ciliary
nerves, which accompany the long posterior ciliary nerves.
At the equator the long ciliary nerves divide, some return
posteriorly in the sclera itself to re-enter the choroid in the
region of the lamina fusca. Of those which pass forward,
most enter the ciliary body, but some form the nerve loops
of Axenfeld (1907). The latter are nerves which, having
entered the ciliary body, then pass outward through the full
thickness of the sclera and back into the ciliary body
through the same canal. These nerves, which are found in
12% of eyes, can form painful tumours when they come to
lie in the episclera. The less obvious ones can often be
detected on the slit lamp by their squashed mushroom
appearance and the faint cuff of pigment which surrounds
the nerve. They are usually associated with blood vessels.
Their function is unknown, but although they have clinical
significance because they are pigmented and sometimes
painful, their removal is not advisable.
The rest of the nerves pass distally, penetrating the sclera
about 3 mm from the limbus and branching to supply the
cornea, trabecular meshwork, Schlemms canal, and
episclera. They are very prominent in the tendinous
insertion of the muscles. Numerous nerve endings staining
for nicotinamide adenine dinucleotide phosphate diaphorate
(NADPHd), and thyrotropic hormone (TH), are found on
the episcleral arteries and to a lesser extent on the veins
(Stone et al., 1987). Nerve fibres staining for neuroactive
peptide Y (NPY), vasoactive intestinal peptide (VIP),
vesicular acetyl choline transporter (VACHT), calcitonin
gene-related peptide (CGRP) and substance P (SP) are also
found largely on the arteries and at arterio-venous
anastomoses In the episclera, anterior to the vascular circle,
numerous free nerve endings staining for SP and CGRP are
also found (Selbach et al., 1998). The purpose of these
endings adjacent to the vessels and aqueous veins, is
presumably to regulate the blood supply of the anterior
segment and to influence the rate of aqueous outflow
(Selbach et al., 2000).
5. Composition of the sclera
Scleral matrix conforms to a general plan seen in other
connective tissues with a scaffold of protein fibrils, collagen
and elastin, and interfibrillar proteoglycans and glyco-
proteins, which surround a diffuse population of cells.
Although there has been a recent resurgence of interest in
the molecular components present in sclera, particularly in
relation to axial development and proper image formation at
the retina, far more is known of corneal than scleral
composition (Mayne, 2002).
5.1. Collagens
Microscopically the sclera is a dense, primarily collage-
nous tissue. Earlier estimations of human and animal scleral
collagen content by weight have varied widely from 50 to
75%, although this may be partly explained by the different
techniques employed (Polatnick et al., 1957; Keeley et al.,
1984). The collagen family of proteins contains the most
abundant proteins in the body. Classically, collagens are
defined as molecules contributing to the structure of
extracellular tissue matrices (Kielty and Grant, 2002), and
are identified as proteins consisting of three polypeptide
chains, assembled with triple-helical domains and contain-
ing Gly-X-Y amino acid repeat sequences, where X and Y
are often proline and hydroxyproline, respectively. Inter-
stitial collagens form the familiar cross-banded fibrils of
tissue matrices by assembly of molecules head to tail with a
quarter-stagger overlap of adjacent molecules. Most fibrils
are now recognised to exist as heterotypic interactions of
more than one collagen type. Twenty seven different
collagens have now been identified from protein and genetic
analysis (Pace et al., 2003; for review see Kielty and Grant,
2002), and many more are expected to be discovered from
analysis of the human genome sequence. However, many of
those found recently have no known structural function.
Types I, III, V and VI collagen are present in the sclera,
although biochemical analyses have shown that type I
predominates, with type III at less than 5% and only trace
amounts of other species present (Keeley et al., 1984;
P.G. Watson, R.D. Young / Experimental Eye Research 78 (2004) 609623 613
Heathcote, 1994). Consistent with these data, types I and III
collagen have been identified in human sclera by light
microscopy immunolocalisation (Tengroth et al., 1985;
Thale and Tillmann, 1993; Thale et al., 1996a,b; White et al.,
1997), although some studies have found type III restricted
to outermost layers, the lamina cribrosa and an interzone
between outer sclera and dura mater (Konomi et al., 1983;
Rhenberg et al., 1987). Collagen types I and III were both
synthesised by human Tenons capsule fibroblasts in vitro
(Gross, 1999). Localisation of collagens at higher resolution
by electron microscopy in macular sclera from aged human
eyes showed types I and III collagen to be present in the
major D-periodic interstitial fibrils, with type V at the fibril
perimeter and type VI in filamentous structures between
fibre bundles (Marshall et al., 1993). This suggested that co-
polymerisation of multiple collagen types into complex
heterotypic assemblies was present in human sclera, as seen
in other tissues, such as cornea and cartilage.
The banded fibrils of scleral stroma, in contrast with
those of the cornea, are coarser and exhibit a wider range of
diameters, between 25 and 300 nm (Spitznas, 1971;
Borcherding et al., 1975; Komai and Ushiki, 1991). Many
ultrastructural studies of scleral collagen fibrils have been
carried out using TEM and scanning electron microscopy
(SEM) and more recently by atomic force microscopy
(AFM, Yamamoto et al., 2000; Meek and Fullwood, 2001;
Yamamoto et al., 2002), generally with good agreement on
collagen fibril dimensions. Different periodicities of corneal
and scleral fibrils of 63 and 67 nm, respectively, have been
identified by AFM and attributed to differing inclination
angles (15 and 58, respectively), of microfibrillarcomponents.
Thinner fibrils are more common in the inner scleral
layers and also in two regions of specialised function,
namely the lamina cribrosa, where the optic nerve enters the
eye, and in the trabecular meshwork in the corneo-scleral
angle. In these regions of the sclera, significant amounts of
type III collagen accompany the main type I component,
together with types IV, V and VI collagen (Rhenberg et al.,
1987; Marshall et al., 1990, 1991; Albon et al., 1995). In the
scleral lamina, fibrils are smaller, more densely packed and
uniform in size than elsewhere in the sclera, exhibiting a
mean diameter of 47 nm, compared to 146 nm in the
equatorial sclera, according to Quigley et al. (1991). SEM
showed the circular arrangement of fibrils around the
emerging axons was lost in eyes with glaucoma (Thale
et al., 1996a,b). The presence of heterotypic, small-diameter
fibrils, rich in type III collagen, was previously considered
to be a specialised adaptation in tissues such as these in the
eye, and tendon, where resistance to deformation and
elasticity are required (Parry and Craig, 1984). However,
our current understanding is that type I:III ratios may show
wide diversity in relation to factors such as tissue, location,
age and disease, but the association of type I and type III
collagens into heterotypic fibrils is a ubiquitous occurrence
in noncartilaginous tissues (Keene et al., 1987).
Many new collagen species have come to light in the last
10 years including several with potential relevance to ocular
structure and development (Kielty and Grant, 2002),
although in many cases their specific significance, if any,
in relation to the organisation and function of the sclera has
yet to be determined. Of these, type XII collagen is thought
to be associated with type I fibrils in human sclera, as well as
cornea, but is expressed as different isoforms with only the
long form expressed in the sclera (Wessel et al., 1997;
Anderson et al., 2000). Types XII and XIV may be
important in collagen fibrillogenesis in development of
ocular connective tissues (Young et al., 2002). The type
XVIII collagen gene has been implicated in the develop-
ment of high myopia and is known to be expressed in the
human eye (Suzuki et al., 2002).
5.2. Elastin
Elastic fibres consisting of microfibrillar and amorphous
components represent an additional fibrillar system supple-
menting the collagen framework in the human sclera. At
least 19 different proteins can be identified within the elastic
fibre system (Gimeno et al., 2001). They first appear as fine
microfibrils at week 72 in human embryonic development,
forming larger composite deposits by week 18 (Sellheyer
and Spitznas, 1988). Elastin is composed of nonpolar
hydrophobic amino acids such as alanine, valine, isoleucine
and leucine and contains little hydroxyproline and no
hydroxylysine. It also contains two unique amino acids,
desmosine and isodesmosine, which serve to cross-link the
polypeptide chains (Postlethwaite and Kang, 1988). Bio-
chemical analysis showed the elastin component of adult
human sclera to be around 2%, although this increases to 5%
in the scleral spur and trabecular meshwork (Moses et al.,
1978). Fibres are most abundant in the lamina fusca and
innermost stromal layers and along the tension lines of the
extraocular muscles (Marshall, 1995), but also exhibit
localised concentrations at the equator, where the sclera is
thinnest, at the limbus and optic disc. Morphometric
analysis revealed four times as much elastin in the lamina
cribrosa as in peripapillary sclera, while in equatorial sclera
it was almost absent (Quigley et al., 1991).
5.3. Proteoglycans
The interfibrillar compartment in the scleral matrix is
occupied primarily by proteoglycans (PGs), although they
are sparsely represented compared to most other connective
tissues with, for example, a four-fold higher concentration in
cornea than sclera. Proteoglycans consist of a protein core to
which variable numbers of sulphated glycosaminoglycan
(GAG) side-chains are covalently attached (for review see
Heinegard et al., 2002). Decorin and Biglycan, members of
the small leucine-rich repeat protein (SLRP) family, are the
main PGs of human sclera, characterised by the presence of
one and two glycosaminoglycan chains, respectively, plus
P.G. Watson, R.D. Young / Experimental Eye Research 78 (2004) 609623614
oligosaccharides (Coster and Fransson, 1981). The glycan
chains in scleral PGs are mostly co-polymers of dermatan
sulphate and chondroitin sulphate, although heparan sulphate
and the unsulphated GAG hyaluronan have also been
reported in small amounts in human sclera (Trier et al.,
1990). Dermatan sulphate contains disaccharide repeats of
two types: D-glucuronic-N-acetylgalactosamine and L-idur-
onate-N-acetylgalactosamine. Unlike DSPGs from other
tissues, scleral DS is typically O-sulphated at the C-6
position on glucuronate-rich domains (Cheng et al., 1994).
Human sclera also contains smaller amounts of the large PG,
aggrecan, which is related to the large, aggregating PG of
articular cartilage and characterised by the presence of
keratan sulphate and chondroitin sulphate GAG chains (Rada
et al., 1997). Rotary shadowing electron microscopy showed
that the large PG in bovine sclera had similar domain
structure to the well-known cartilage aggrecan (Ward et al.,
1987). Decorin, biglycan and aggrecan proteoglycans are
present throughout the full thickness of the tissue, although
aggrecan is most abundant in the posterior sclera (Rada et al.,
1997, 2000). SLRP PGs have been implicated in the
regulation of collagen fibrillogenesis and thus may be
important in scleral development and repair. Decorin, in
particular, has been shown to deccelerate fibril growth and
increase fibril diameter (Neame et al., 2000; Kuc and Scott,
1997). It also binds to TGFb (Takeuchi et al., 1994) and
interacts with collagen types I, VI and XIV (Ehnis et al.,
1997). A third SLRP PG, lumican, has also been identified in
mouse sclera (Austin et al., 2002). This PG is the classical PG
of corneal stroma, but its presence in human sclera has not yet
been confirmed. Lumican is also able to influence fibril
diameter and seems to be involved in determining transpar-
ency in the cornea as well (Chakravarti et al., 2000; Quantock
et al., 2001). As with collagens, several new SLRPs have
been discovered recently, including opticin which was first
identified in the iris (Friedman et al., 2000). It is a minor
component of the trabecular meshwork (Friedman et al.,
2002), but has not so far been reported in the scleral stroma.
Asporin also is a newly discovered SLRP (Henry et al.,
2001), which seems to overlap in its expression with that of
the main scleral PGs decorin and biglycan, but which again
has not yet been confirmed in the eye.
5.4. Collagenproteoglycan interaction
The narrow interfibrillar spaces in scleral matrix would
seem highly conducive for close apposition and interactions
between fibrillar and nonfibrillar components of the matrix.
X-ray diffraction techniques applied to analyse collagen
organisation and the arrangement of fibril-associated struc-
tures in human sclera revealed axial density profiles very
similar to those recorded in rat tail tendon (Quantock and
Meek, 1988). Anionic groups on GAG sidechains of matrix
PGs have been exploited to visualise scleral PGs and their
collagen associations, using cationic dyes, such as cuprolinic
and cupromeronic blue (Young, 1985; Van Kuppevelt et al.,
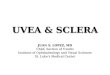
1987; Quantock and Meek, 1988). These methods reveal PGs
as electron dense filaments regularly distributed along the
fibrils and closely-associated with the collagen fibrils at the d
and e bands of the D-periodic cross banded axial pattern
(Fig. 2). Application of decorin-specific antibodies and
detection by sensitive immunogold particulate markers has
since confirmed these structures as decorin PG, periodically
associated with the collagen fibrils in human sclera (Kimura
et al., 1995). Decorin binds to a site near the C terminal end of
the type I collagen molecule (Keene et al., 2000). In addition,
decorin was found to be associated with type VI collagen in
the interfibrillar space (Kimura et al., 1995).
Accumulating evidence supports an important role for
small leucine-rich PGs, particularly decorin in regulating
Fig. 2. Normal human sclera showing proteoglycans as fine filaments (arrows) associated with collagen fibrils in longitudinal section. Bar represents 250 nm.
P.G. Watson, R.D. Young / Experimental Eye Research 78 (2004) 609623 615
the topographical organisation of the collagen fibrillar
matrix. Decorin thus appears to have a role in development
and wound healing. Significant reduction in decorin
synthesis in the posterior sclera was found to be associated
with elongation of the eye and development of myopia in
marmosets (Rada et al., 2000). Decorin-null mice exhibit
abnormal collagen fibrils in tendon and skin (Danielson
et al., 1997). Surprisingly, lumican deficiency in mice also
causes scleral anomalies with larger fibrils in anterior and
posterior scleral stroma, in spite of the small amounts of this
PG present in the tissue (Austin et al., 2002). In contrast to
studies on decorin, there is disagreement in published
reports of the binding affinity of Biglycan for collagen type I
(Schonherr et al., 1995; Heinegard et al., 2002), and no
specific studies of biglycan in sclera have been carried out.
5.5. Cellular components
All layers of the sclera exhibit low cellularity compared
to most vascularised tissues. The indigenous cell is the
scleral fibrocyte. The structural and functional integrity of
the scleral connective tissue layers is dependent upon the
biosynthetic activity of this cell population. Although few in
number, they have extended cytoplasmic extensions which
contact adjacent cells, forming a syncytium, similar to that
reported in tendon where cells associate by gap junctions
(McNeilly et al., 1996). In healthy tissue the cells appear
elongate and closely-apposed to the collagen bundles. Only
in the lamina fusca there is a noticeable increase in cell
numbers, where the sclerocyte population is supplemented
by numbers of melanocytes, the importance of which is
unclear.
Sclerocytes can undergo rapid tranformation into active
fibroblasts following any insult to the sclera. This can be
physical trauma, such as surgical incision, or chemother-
apeutic as in the topical application of cytotoxic agents to the
sclera for the treatment of neoplasia, or in the prevention of
post-operative scarring. Scleral fibroblasts appear as stellate
or spindle-shaped cells with a large nucleus and relatively
scanty cytoplasm, containing conspicuous mitochondria and
rough endoplasmic reticulum with attached ribosomes. The
cells vary in size according to function so that, during
secretory activity, the cytoplasm becomes filled with a Golgi
zone, vacuoles, vesicles and lysosomes. The fibroblast is able
to synthesise all of the component molecules of the matrix.
Scleral fibrocytes, like other connective tissue cells are
reactive to a broad range of cytokines including interferon g,growth factors (e.g. Platelet-derived growth factor (PDGF),
transforming growth factor (TGFb) and fibroblast growthfactor (FGF)), IL1 and thymocyte derived growth factors.
Histiocytes, blast cells, granulocytes, lymphocytes and
plasma cells can all occasionally be identified in small
numbers in normal scleral stroma. Mast cells and eosino-
phils, characterised by the structure of their cytoplasmic
granules, are also present. Mast cells are present in large
quantities at the limbus, around blood vessels traversing
the sclera and in choroid, but are sparse in the iris, ciliary
body and retina. Their function within the tissue matrix has
not yet been fully defined, but they are active in acute
inflammatory states, including episcleritis and scleritis and
also during the healing of scleral wounds.
In response to an inflammatory stimulus in the sclera,
cells pass rapidly from blood vessels of the choroid and
episclera, the first arriving within minutes at the site of the
insult (Watson and Hazleman, 1976). In contrast, choroidal
and intraocular tumours rarely seem to penetrate the scleral
coat. They may spread out of the globe through the emissary
foramen, but usually have to cause a secondary inflam-
mation before the cells can penetrate the scleral barrier
(Blatt et al., 1958). Inflammatory cells readily dissolve
intercellular macromolecules, but tumours rarely do so. The
tumours do not appear to be confined by an inflammatory
reaction, but the cells which are able to migrate may well be
dealt with elsewhere provided only a few manage to get
outside the globe. Intraocular abscesses are confined by the
scleral coat in the same way that any abscess will be
restricted by a fibrous envelope. Reactive inflammation of
the episclera always accompanies intraocular or intrascleral
abscesses, so that organisms which pass through the sclera
are dealt with in the episclera itself.
6. Scleral hydration and fluid transport
Hydration of scleral tissue is closely related to the
composition of the extracellular matrix. The proteoglycans
regulate diffusional transport on account of the hydrophilic
nature of their extended glycosaminoglycan side chains,
such that the water content of sclera is around 68%. The
possibility of drug delivery to the eye through a transcleral
route has recently rekindled interest in scleral hydration and
permeability (Boubriak et al., 2000). Sclera was found to
exhibit a higher permeability to globular proteins than linear
dextrans, with diffusion determined by molecular weight
and, especially, by molecular radius (Ambati et al., 2000).
Tissue hydration, together with fibrillar organisation is
believed to be crucial for corneal transparency. Sclera
contains a lower concentration of proteoglycans than
cornea, which is reflected in the three times greater swelling
of cornea over sclera under experimental conditions (Huang
and Meek, 1999). If the sclera is dehydrated, as can occur in
retinal detachment procedures when the sclera is exposed
for a prolonged period, then the sclera becomes more
transparent. David Maurice was first to suggest that this
phenomenon might be explained by the increase in
concentration of mucoprotein, through dehydration, near
to that present in cornea (Maurice, 1969).
Intraocular fluid transport is vitally important to the
health of the eye and involves the sclera via two distinct
systems: the first is represented by the scleral spur and its
ciliary muscle and tendon attachments to the trabecular
meshwork, in the conventional outflow of aqueous to
P.G. Watson, R.D. Young / Experimental Eye Research 78 (2004) 609623616
Schlemms canal. The second is uveoscleral outflow, which
accounts for 40% of aqueous outflow. This falls with age to
between 4 and 14% in those over 60, possibly as a result of
the changes which occur within the sclera with age. Uveo-
scleral outflow was demonstrated by Bill (1965) who
perfused radio-iodinated albumen into the anterior chamber
of cynomolgus monkeys and recovered the tracer from the
anterior and posterior sclera within 25 minutes. The fluid
passes through the spaces between the ciliary muscle fibres
into the suprachoroidal space and exits around the vortex
veins, other emissary channels and through the sclera itself.
The driving force for this movement is diffusion. The
gradient is jointly determined by the hydrostatic pressure of
the aqueous, the permeability of the ciliary muscle and
sclera and the osmotic pressure in the suprachoroidal space,
which is in turn determined by the concentration of plasma
protein in the surrounding vessels. The role of the sclera in
uveo-scleral outflow is indirectly of considerable import-
ance for the viability of the retinal pigment epithelium and
thus the apposition of the retina to this epithelium.
7. Scleral development
Embryologically, the sclera has dual origins arising from
both mesodermal and neural crest primordia. The mesoderm
contributes directly to only a small strip of temporal sclera,
whilst the extraocular muscles, vascular endothelium and
ocular adnexae form entirely from this source. The
remaining connective tissues of the eye and the pericytes
of the ocular vessels are all derived from the neural crest. As
with sclera, many other connective tissues are of neural
crest-mesodermal origin, including cartilage, bone, liga-
ment, tendon, dermis and perivascular smooth muscle and
their maturation follows a very similar pattern and time
scale. This may explain, at least in part, the frequent
association of sclera and joints in many systemic diseases.
A microscopical study of human embryos and foetuses
by Sellheyer and Spitznas (1988) showed that development
of the sclera begins anteriorly during the seventh gestational
week. It is probable that the differentiating uvea, and in
particular the pigment epithelium, is responsible for the
induction of the sclera (Gruenwald, 1944). Certainly if the
outer layer of the optic vesicle is destroyed, the sclera does
not develop (Giroud, 1957). Cellular changes, as indicated
by the loss of free ribosomes and polysomes and an increase
in the rough endoplasmic reticulum of the developing
scleral cells, progress from the presumptive limbus, both
posteriorly and from inside outwards. There is a marked
increase in glycogen and lipid in the outer (episcleral) sclera
from 7 to 10 weeks, but none thereafter. Elastic microfibrils
are found at week 7, but these do not develop into elastic
deposits until week 18 (Sellheyer and Spitznas, 1988),
possibly in response to intraocular pressure (Ozanics et al.,
1976). By the fourth month the scleral spur appears as
circularly oriented fibres and by the fifth month, scleral
fibres crisscross around the axons of the optic nerve to form
the lamina cribrosa. The end point of development is
determined by the rates of growth, development and
function of the adjacent structures, lens, retina and choroid
and the production of aqueous by the ciliary body. The
postnatal sclera is thin and translucent, allowing the blue
colour of the underlying uvea to show through during the
first 3 years of life.
8. Age changes in sclera
The human sclera reaches its adult size and maximum
elasticity at the age of 1213 years, after which there is a
progressive reduction in compliance and an increase in
rigidity. Increased scleral rigidity, as in other connective
tissues, is the result of a progressive cross-linking of the
lysine residues of collagen with age (Keeley et al., 1984), by
either enzyme-dependent or independent pathways. As age
increases the sclera becomes increasingly yellow as a
consequence of the deposition of fat globules between the
collagen fibres. There seems to be no age-related change in
collagen content or type, or between the anterior and
posterior segments in the sclera. However, turnover of
ocular collagens in general declines with age, although
types III and VI may show smaller changes than type I,
according to studies of collagen mRNA in ageing mice
(Ihanamaki et al., 2001). The collagen fibres become thicker
and less uniform with increased age, particularly in the
region of the muscle insertions. Here the sclera becomes
progressively thinned, increasing the colour contrasts
between one part of the sclera and the next. If the fibres
become disrupted then calcium deposition can occur,
leading to the production of hyaline plaques. PG com-
ponents of human sclera increase in concentration until the
fourth decade. Thereafter decorin and biglycan undergo a
steady decline, with aggrecan concentration maintained
until the ninth decade (Rada et al., 2000). The number of
elastic fibres also falls between the second and seventh
decade, particularly in the anterior segment. This is reflected
in the different behaviour of the surgically incised sclera in
the young and the old.
Biochemical analysis of the aging lamina cribrosa
revealed an increase in total collagen, pentosidine collagen
cross-links, and also elastin, and a decrease in type III
collagen and sulphated glycosaminoglycans (Albon et al.,
1995, 2000a). Assessment of the mechanical properties of
aging lamina demonstrated an associated increase in
rigidity and loss of compliance of the tissue (Albon
et al., 2000b).
9. Scleral disease
Frequently the more that is learnt about any condition the
more it is realised that there may be many causes leading to
P.G. Watson, R.D. Young / Experimental Eye Research 78 (2004) 609623 617
a particular clinical state. This is true in scleral disease
scleritis is not a single entity. Histologically, it is an
inflammatory response that can be simulated by a variety of
conditions consisting predominantly of lymphocytes with
few polymorphs and plasma cells. Importantly, whatever
the underlying condition, whether it be Goodpastures
syndrome, Wegeners granulomatosis or Herpes zoster, the
histological appearance is that of a rheumatoid nodule
with a central area of necrosis surrounded by a zone of
histiocytes and polymorphs and an outer zone of lympho-
cytes and plasma cells. Vasculitis is detectable in the
majority (Fong et al., 1991).
The transformation from normal tissue to necrosis was
demonstrated in studies by Young and Watson (1984a,b) in
various types of scleritis. The findings were remarkably
similar whatever the underlying disease. Correlative
fluorescein angiography and electron microscopy were
used to study the sclera, at sites from apparently normal
tissue to the centre of a necrotic area, in an eye from a 52
year-old man with severe necrotising scleritis (Watson and
Young, 1985). Changes were found in both the vasculature
and the collagen and proteoglycans. At the periphery of the
lesion there was activation of fibrocytes in the absence of
inflammatory cells. This fibroblastic transformation may be
one of the earliest events in scleral degradation in
necrotising disease. Activation of fibrocytes is associated
with breakdown of proteoglycan linkages between fibrils
and later leads inexorably to complete loss of the
proteoglycans from the scleral interfibrillar matrix (Young
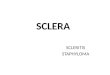
et al., 1988). Removal of proteoglycans allows collagen
fibrils to unwind (Fig. 3), to separate from their fellows, and
eventually to be digested. Whether atypical proteoglycans
are produced during this process, giving rise to the
appearance of fibrinoid is unclear. The degradation of
scleral collagen occurs by both intracellular and
extracellular mechanisms. Cells resembling active fibro-
blasts and macrophages can be seen to phagocytose collagen
fibrils into vacuoles associated with dense, intracellular
cytoplasmic granules. In the extracellular matrix, collagen
fibrils in large areas of the scleral stroma appear swollen and
unravelled or completely solubilised, without close associ-
ation with stromal cells (Fig. 4). Both activation and
degeneration of stromal fibrocytes are evident in zones of
extracellular fibril degradation.
Closer to the lesion in an area apparently unperfused on
the fluorescein angiogram, the venules showed high
endothelial changes with migration of polymorphs, lym-
phocytes, plasma cells, macrophages and a large number of
mast cells into the surrounding tissue. Adjacent to the
ulcerated lesion the vessels appeared to be completely
obstructed with the endothelium largely destroyed. These
cellular reactions and the final end point of tissue
destruction are strikingly similar to those found in the
systemic connective tissue diseases, commonly associated
with scleritis (Rao et al., 1985). Many of the aetiological
factors that lead to the systemic disorders also apply to the
eye. The disorders share common proposed immune
aetiologies although, as in the case of scleritis, neither the
initiating antigen nor the processes that result in chronicity
have been defined.
The reason why inflammation occurs in sclera is
because of its unique anatomical and vascular character-
istics, which permit transudation into tissue from which
there is sluggish clearance, allowing intense immune
reactions to occur and persist. Recent experimental data
and clinical observations (alongside comparisons with
similar disease processes elsewhere), which have enabled
a better understanding of the possible pathogenesis of
scleritis have also allowed novel and successful treatment
strategies to be formulated.
Fig. 3. Sclera adjacent to a degradative lesion in necrotising scleritis shows loss of proteoglycan filaments, separation of collagen fibrils and appearance of axial
striations along fibrils (arrows), which may be early stages of fibril breakdown. Bar represents 300 nm.
P.G. Watson, R.D. Young / Experimental Eye Research 78 (2004) 609623618
The immune system operates as an integrated system of
protection allowing the effective elimination of microbial
pathogens. The innate immune system provides a hard-
wired defence system that is activated following exposure
to characteristic microbial motifs. Cells of the innate
immune system, particularly dendritic cells, respond to
activation by migrating to local lymph nodes where they can
present peptide components from the offending pathogen on
surface MHC molecules to cells of the more flexible
adaptive immune response. The trigger for this response in
the sclera can be from without, as with infections or trauma,
or within, when it is part of the manifestations of another
systemic disease (for reviews, see Foster and Sainz de la
Maza, 1993; Watson et al., 2003).
The conjunctiva, tears and cornea are in constant contact
with bacteria, viruses and other potential antigens, but the
defence mechanisms are sophisticated and the episclera and
sclera are protected from surface antigens by the con-
junctiva. However, Herpes simplex can be cultured from the
conjunctival sac in the initial attack in some patients and
multiple systemic infections have been reported with scleral
disease (Watson and Hayreh, 1976; Sainz de la Maza et al.,
1993). Epstein-Barr virus, parvoviruses and mycobacteria
have been implicated in the production of rheumatoid
arthritis (Alspaugh et al., 1981), but although it is known
that the eye can be a portal for entry of viruses into the body,
there is no evidence to suggest this is a reason for the onset
of scleral disease in patients with rheumatoid arthritis.
Equally in Herpes zoster infection, which is frequently
associated with scleral disease, it is likely that the scleral
inflammatory response is induced by virus particles, which
have gained retrograde entry into the sclera via the nerves
and have induced a localised immune reaction as a response
to virally-induced destruction of tissue. Viruses induce a
tissue reaction by either changing the host responses once
they become intracellular, or by inducing cellular
expression of abnormal proteins, which in turn could render
that tissue antigenic (Robb, 1977). Some such mechanism is
certainly possible in scleral inflammation.
Considering the constitutional similarity between the
joint and the sclera, it is highly probable that those factors
which trigger the onset of joint problems in connective
tissue disease, such as rheumatoid arthritis, will also be
present in the sclera. Scleral involvement may arise
following local trauma, as in surgically-induced necrotising
scleritis (SINS). Here, sequestered antigen becomes
exposed in an individual already primed to induce a
response as a result of systemic disease. Alternatively, a
response may be induced because of the unique vascular
supply of the anterior segment of the eye.
9.1. Antigen and immune complexes in scleritis
No specific antigenic stimulus for the immuno-inflam-
matory cascade in patients with scleritis has yet been
detected. In contrast, in Moorens ulcer of the cornea, the
defensin protein Calgranulin C is now thought to be the
antigenic stimulus (Akpek et al., 2000). A 54 kDa epithelial
antigen has been found in association with corneal changes
in rheumatoid arthritis (John et al., 1992) and a 70 kDa
antigen in Wegeners granulomatosis (John et al., 1992).
Further research is required to identify the initial antigenic
response in necrotising scleritis. Candidate antigens may
reside in matrix proteoglycans and collagens, which as we
have shown, are modified early in the disease process
(Young et al., 1988). Disruption of proteoglycancollagen
interactions is induced by metalloproteinase enzymes
released from activated fibroblasts (Di Girolamo et al.,
1995; Riley et al., 1995; Di Girolamo et al., 1997). Once the
proteoglycan has been stripped from the fibril this collagen
Fig. 4. Advanced degradation of scleral stroma central to a lesion in necrotising scleritis illustrates swelling and unravelling of individual collagen fibrils. Bar
represents 1 mm.
P.G. Watson, R.D. Young / Experimental Eye Research 78 (2004) 609623 619
could become antigenic as it is a sequestered antigen, never
having been exposed to the immune systems tolerance
mechanisms. These antigens could be presented to the
immune system through the antigen presenting cells, such as
tissue macrophages. The subsequent T cell response
resulting in cytokine release could in turn induce collagen-
ase release from the fibrocytes. At this stage an acute pro-
inflammatory stimulus, such as a virus infection, would
perpetuate the response. Such an intense immune response
may remain localised, as in Herpes zoster infection or some
cases of SINS, or it may become generalised, spreading and
progressing to full-blown necrotising disease. The role of
immune complexes is uncertain. They were clearly demon-
strated in the sclera in an experimental model of scleritis
(Hembry et al., 1979). Fibrocytes were activated and the
immune complexes were resorbed by the local vessels,
inducing a transient but very severe necrotic vasculitic
response, which could be detected by angiography and
confirmed with histology. As the response did not occur at
the site of maximum concentration of antigen, this suggests
that the balance of antigen and/or antibody is critical for the
vasculitic response to take place.
9.2. Vasculitic response
The great majority of patients with any form of scleritis
and all those with necrotising disease have a microvascular
inflammation, the result of either local or systemic disease.
The sclera itself does not contain a capillary plexus but
derives its nutrition from the episcleral plexuses which
overly it and, in the case of the equatorial and posterior
sclera, from the choroidal vessels beneath it. The episcleral
vessels themselves lose their muscular coat at their origin
from the choroidal vessels and consist of simple, walled
tubes of endothelial cells surrounded by basement mem-
brane and a discontinuous layer of pericytes. This unusual
structure results in the arterial side of the vascular network
being thrown into tortuous folds through which the blood
flow is turbulent and, because of the artery to artery
anastomoses, the circulation is sluggish or oscillatory. As a
consequence the normal mechanisms for removing immune
complexes and other potentially noxious substances cannot
function and this, together with the poor lymphatics, means
that inflammatory reactions and micro-vascular changes can
easily occur and persist at these sites. It is a common clinical
observation that scleritis often begins and spreads from the
areas between the recti muscles, the area in which the
circulation is slowest.
Histological examination and angiography of the scleral
vessels reveal a variety of changes varying from simple
permeability, as in diffuse episcleritis, to complete endo-
thelial destruction and vascular occlusion in severe
necrotising scleritis (Nieuwenhuizen et al., 2003). Most
specimens show an inflammatory microangiopathy with
neutrophil infiltration in and around the vessel wall in which
is deposited IgG. If the inflammatory response is severe,
there is evidence of collagen destruction. In addition
the endothelial cells first swell and, in the vaso-occlusive
form of the disease, occlude the lumen. This change is
usually transient but sometimes a platelet thrombus will
form. In the most severe disease the endothelial cells
become necrotic, leading to permanent occlusion of the
vessels, which are often replaced by new ones, a common
feature in patients with a systemic vasculitis. Angiographi-
cally, these changes can be detected by the remodelling of
the vascular plexus. The swollen endothelium allows almost
any cell to move outwards from the vessel into the extra-
vascular space with the consequent release of cytokines and
the induction of an inflammatory lesion (Michel and Curry,
1999). At the same time, the vascular endothelium
upregulates HLADR Class II and thus the vessel itself
becomes a target for attack. If severe this vasculitic process
can affect even the largest vessels in the eye. Even though a
vessel may appear clinically normal it may still be inflamed
and incompetent. At present this localised inflammation can
only be detected by ICG angiography, which may also
disclose if the inflammation is fully controlled.
9.3. Cellular responses
So many reactions can occur within the span of even 1 hr
that it is extremely difficult to be certain of the sequence of
events when many cell types are present in any one
specimen, but the predominant cells found in all those with
scleritis are the macrophage and the CD4 T-lymphocyte.(Young and Watson, 1984a; Bernauer et al., 1994;
Diaz-Valle et al., 1998). There are few or no macrophages,
Langerhans cells, neutrophils or lymphocytes in normal
human sclera. After scleral inflammation, however, there is
a marked increase in T-helper lymphocytes with a high T-
helper to T-suppressor ratio (Bernauer et al., 1994).
No genetic predisposition to scleritis has been estab-
lished (Joycey et al., 1997), although there is a possibility
that possession of the HLA-DR15(2) phenotype may
predispose to corneal ulceration in response to an inflam-
matory stimulus. Immunogenetic susceptibility may how-
ever be important in the development of some of the
systemic vasculitic disorders associated with scleritis. In
rheumatoid arthritis, the connective tissue disorder most
frequently associated with scleritis, the class II major
histocompatibility complex (MHC) locus is associated with
susceptibility to rheumatoid joint disease. A majority of
patients with rheumatoid arthritis carry HLA-DR4, HLA-
DR1, or both. HLA-DR4 has five subtypes, two of which
(Dw4 and Dw14) are present in 50 and 35% of patients with
rheumatoid arthritis, respectively.
Bernauer et al. (1994) analysed the inflammatory cellular
effector mechanisms in scleritis. The inflammatory cells
infiltrating the scleral tissues were mainly T lymphocytes
and macrophages. There was a predominance of CD4
positive cells, but only few lymphocytes were activated
(expressed IL-2 receptor). Clusters of B cells were found in
P.G. Watson, R.D. Young / Experimental Eye Research 78 (2004) 609623620
perivascular areas. Signs of a granulomatous process with
activated macrophages (epithelioid and giant cells) were
present in necrotising scleritis. Expression of major
histocompatibility, class II molecules (MHC II) was found
on lymphocytes and rarely on macrophages. Sainz de la
Maza et al. (1994) found similar changes of HLA-DR
expression and increased T helper participation in 10
patients, nine of whom had an underlying autoimmune
vasculitis systemic disease. The cellular infiltrate in scleritis
thus shows, at least at certain stages, features compatible
with a T cell mediated (autoimmune) disorder.
References
Akpek, E.K., Liu, S.H., Gottsch, J.D., 2000. Induction of experimental
autoimmume keratitis by adoptive transfer of human corneal antigen
specific T cell line. Invest. Ophthalmol. Vis. Sci. 41, 41824188.
Albon, J., Karwatowski, W.J., Avery, N., Easty, D.L., Duance, V.C., 1995.
Changes in the collagenous matrix of the aging human lamina cribrosa.
Br. J. Ophthalmol. 79, 368375.
Albon, J., Karwatowski, W.J., Easty, D.L., Sims, T.J., Duance, V.C., 2000a.
Age related changes in the non-collagenous components of the
extracellular matrix of the human lamina cribrosa. Br. J. Ophthalmol.
84, 311317.
Albon, J., Puslow, P.P., Easty, D.L., Karwatowski, W.S., 2000b.
Mechanical compliance of the aging human lamina cribrosa. Br.
J. Ophthalmol. 84, 318323.
Alspaugh, M.A., Henle, G., Lennette, E.T., Henle, W., 1981. Elevated
levels of antibodies to Epstein-Barr virus antigens in sera and synovial
fluids of patients with rheumatoid arthritis. J. Clin. Invest. 67,
11341139.
Ambati, J., Canakis, C.S., Miller, J.W., Gragoudas, E.S., Edwards, A.,
Weissgold, D.J., Kim, I., Delori, F.C., Adamis, A.P., 2000. Diffusion of
high molecular weight compounds through sclera. Invest. Ophthalmol.
Vis. Sci. 41, 11811185.
Anderson, D.R., 1969. Ultrastructure of human and monkey lamina
cribrosa and optic nerve head. Arch. Ophthalmol. 82, 800804.
Anderson, S., SandarRaj, S., Fite, D., Wessel, H., SundarRaj, N., 2000.
Developmentally regulated appearance of spliced variants of type XII
collagen in the cornea. Invest. Ophthalmol. Vis. Sci. 41, 5563.
Austin, B.A., Coulon, C., Liu, C.Y., Kao, W.W., Rada, J.A., 2002. Altered
collagen fibril formation in the sclera of lumican-deficient mice. Invest.
Ophthalmol. Vis. Sci. 43, 16951701.
Axenfeld, K.T., 1907. Accessory episcleral ciliary ganglia. Von Graefe.
Arch. Ophthalmol. 34, 300.
Bernauer, W., Watson, P.G., Daiker, B., Lightman, S., 1994. Cells
perpetuating the inflammatory response in scleritis. Br. J. Ophthalmol.
78, 381385.
Bill, A., 1965. Movement of albumin and dextran through the sclera. Arch.
Ophthalmol. 74, 248252.
Blatt, N., Ursu, A., Popovici, V., 1958. Invasion potential of malignant
intraocular tumours. Klin. Monatsblat. Augenheil. 132, 808828.
Borcherding, M.S., Blacik, L.J., Sittig, R.A., Bizzel, J.W., Breen, M.,
Weinstein, H.G., 1975. Proteoglycans and collagen fibre organization in
human corneoscleral tissue. Exp. Eye Res. 21, 5970.
Boubriak, O.A., Urban, J.P., Akhtar, S., Meek, K.M., Bron, A.J., 2000. The
effect of hydration and matrix composition on solute diffusion in rabbit
sclera. Exp. Eye Res. 71, 503514.
Bussacca, A., 1947. Les vaisseaux lymphatiques de la conjonctivite
bulbaire etudies par la methode des injections vitals be Bleu Tripan.
Bull. Soc. Fr. Ophthalmol. 60, 8487.
Chakravarti, S., Petroll, W.M., Hassell, J.R., Jester, J.V., Lass, J.H., Paul, J.,
Birk, D.E., 2000. Corneal opacity in lumican-null mice: defects in
collagen fibril structure and packing in the posterior stroma. Invest.
Ophthalmol. Vis. Sci. 41, 33633373.
Cheng, F., Heinegard, D., Malmstrom, A., Schmidtchen, A., Yoshida, K.,
Fransson, L.-A., 1994. Patterns of uronosyl epimerization and 4-/6-O-
sulphation in chondroitin/dermatan sulphate from decorin and biglycan
of various bovine tissues. Glycobiology 4, 685696.
Coster, L., Fransson, L.-A., 1981. Isolation and characterization of
dermatan sulphate proteoglycans from bovine sclera. Biochem. J.
193, 143153.
Danielson, K.G., Baribault, H., Holmes, D.F., Graham, H., Kadler, K.E.,
Iozzo, R.V., 1997. Targetted disruption of decorin leads to abnormal
collagen fibril morphology and skin fragility. J. Biol. Chem. 136,
729743.
Di Girolamo, N., Lloyd, A., McCluskey, P., Filipic, M., Wakefield, D.,
1997. Increased expression of matrix metalloproteinases in vivo in
scleritis tissue and in vitro in cultured human scleral fibroblasts. Am.
J. Pathol. 150, 653658.
Di Girolamo, N., McCluskey, P.J., Lloyd, A., et al., 1995. Localisation of
stromelysin matrix metalloproteinase-3 and tissue inhibitor of metallo-
proteinase TIMP-1 mRNA in scleritis. Ocul. Immunol. Inflamm. 3,
181184.
Diaz-Valle, D., Benitez de Castillo, J.M., Castillo, A., 1998. Immunologic
and clinical evaluation of post surgical necrotic scleral ulceration.
Cornea 17, 371375.
Ehnis, T., Dieterich, W., Bauer, M., Kresse, H., Schuppan, D., 1997.
Localization of a binding site for the proteoglycan decorin on collagen
XIV (undulin). J. Biol. Chem. 272, 2041420419.
Fong, L.P., Sainz de la Maza, M., Rice, B.A., Kupferman, A.E., Foster,
C.S., 1991. Immunopathology of scleritis. Ophthalmology 98,
472476.
Foster, C.S., Sainz de la Maza, M., 1993. The Sclera. Chapters 6 and 7,
Springer, Berlin.
Friberg, T.R., Lace, J.W., 1988. A comparison of the elastic properties of
human choroid and sclera. Exp. Eye Res. 47, 429436.
Friedman, J.S., Ducharme, R., Raymond, V., Walter, M.A., 2000. Isolation
of a novel iris-specific and leucine-repeat protein (oculoglycan) using
differential selection. Invest. Opthalmol. Vis. Sci. 41, 20592066.
Friedman, J.S., Faucher, M., Hiscott, P., Biron, V.L., Malenfant, M.,
Turcotte, P., Raymond, V., Walter, M.A., 2002. Protein localization in
the human eye and genetic screen of opticin. Hum. Mol. Genet. 15,
13331342.
Gimeno, M.J., Bellon, J.M., Bujan, J., 2001. Ocular changes associated
with connective tissue disorders: role of the elastic and collagen
components. Arch. Soc. Esp. Oftalmol. 76, 459469.
Giroud, M., 1957. Phenome`nes dinduction et leurs perturbations chez
mammife`res. Acta Anat. 30, 297306.
Gross, R.L., 1999. Collagen type I and III synthesis by Tenons capsule
fibroblasts in culture: individual patient characteristics and response to
mitomycin C, 5-fluorouracil and ascorbic acid. Trans. Am. Ophthalmol.
Soc. 97, 513543.
Gruenwald, P., 1944. Studies on developmental pathology II. Sporadic
unilateral microphthalmia and associated malformations in chick
embryos. Am. J. Anat. 74, 217257.
Hamanaka, T., 1989. Scleral spur and ciliary muscle in man and monkey.
Jpn. J. Ophthalmol. 33, 221236.
Heathcote, J.G., 1994. Collagen and its disorders. In: Garner, A.,
Klintworth, G.K. (Eds.), Pathobiology of Ocular Disease. A Dynamic
Approach, 2nd Ed., Marcel Dekker, New York, pp. 10331084.
Heinegard, D., Aspberg, A., Franzen, A., Lorenzo, P., 2002. Glycosylated
matrix proteins. In: Royce, R.M., Steinmann, B. (Eds.), Connective
Tissue and its Heritable Disorders, 2nd Ed., Wiley-Liss, pp. 271291,
Chapter 4.
Hembry, R.M., Playfair, J., Watson, P.G., Dingle, J.T., 1979. Experimental
model for scleritis. Arch. Ophthalmol. 97, 13371340.
Henry, S.P., Takanosu, M., Boyd, T.C., Mayne, P.M., Eberspaecher, H.,
Zhou, W., de Crombrugghe, B., Hook, M., Mayne, R., 2001. Expression
pattern and gene characterization of asporin, a newly discovered
P.G. Watson, R.D. Young / Experimental Eye Research 78 (2004) 609623 621
member of the leucine-rich repeat protein family. J. Biol. Chem. 276,
1221212221.
Hogan, M.J., Alvarado, J.A., Weddell, J.E., 1971. Histology of the Human
Eye, The Sclera, Saunders, Philadelphia, PA, Chapter 5, p. 194.
Huang, Y., Meek, K.M., 1999. Swelling studies on the cornea and sclera:
the effects of pH and ionic strength. Biophys. J. 77, 16551665.
Ihanamaki, T., Salminen, H., Saamanen, A.M., Pelliniemi, L.J., Hartmann,
D.J., Sandberg-Lall, M., Vuorio, M.E., 2001. Age-dependent changes in
the expression of matrix components in the mouse eye. Exp. Eye Res.
72, 423431.
John, S.L., Morgan, K., Tullo, A.B., Holt, P.J., 1992. Corneal autoimmunity
in patients with peripheral ulcerative keratitis in association with
rheumatoid arthritis and Wegeners Granulomatosis. Eye 6, 630636.
Joycey, V.C., Roger, J.H., Ashwoth, F., Watson, P.G., 1997. Parrallel
studies of HLA antigens in patients with rheumatic disease and scleritis:
comparison with three control populations. J. Rheumatol. Suppl. 3,
8488.
Keeley, F.W., Morin, J.D., Vesely, S., 1984. Characterisation of collagen
from normal human sclera. Exp. Eye Res. 39, 533542.
Keene, D.R., Sakai, L.Y., Bachinger, H.P., Burgeson, R.E., 1987. Type III
collagen can be present on banded collagen fibrils regardless of fibril
diameter. J. Cell. Biol. 105, 23932402.
Keene, D.R., San Antonio, J.D., Mayne, R., McQuillan, D.J., Sarris, G.,
Santoro, S.A., Iozzo, R.V., 2000. Decorin binds near the C-terminus of
type I collagen. J. Biol. Chem. 275, 2180121804.
Kielty, C.M., Grant, M.E., 2002. The collagen family: structure, assembly
and organization in the extracellular matrix. In: Royce, R.M.,
Steinmann, B. (Eds.), Connective Tissue and its Heritable Disorders,
Wiley-Liss, pp. 159221, Chapter 2, Part 1.
Kimura, S., Kobayashi, M., Nakamura, M., Hirano, K., Awaya, S.,
Hoshino, T., 1995. Immunoelectron microscopic localization of decorin
in aged human corneal and scleral stroma. J. Electron Microsc. 44,
445449.
Komai, Y., Ushiki, T., 1991. The three-dimensional organisation of
collagen fibrils in the human cornea and sclera. Invest. Ophthalmol. Vis.
Sci. 32, 22442258.
Konomi, H., Hayashi, T., Sano, J., Terato, K., Nagai, Y., Arima, M.,
Nakayasu, K., Tanaka, M., Nakajima, A., 1983. Immunohistochemical
localization of type I, III and IV collagens in the sclera and choroids of
bovine, rat, and normal and pathological human eyes. Biomed. Res. 4,
451458.
Kuc, I.M., Scott, P.G., 1997. Increased diameters of collagen fibrils
precipitated in vitro in the presence of decorin from various connective
tissues. Connect. Tissue Res. 36, 287296.
Marshall, G.E., 1995. Human scleral elastic system: an immunoelectron
microscopic study. Br. J. Ophthalmol. 79, 5764.
Marshall, G.E., Konstas, A.G., Lee, W.R., 1990. Immunogold localisation
of type IV collagen and laminin in the aged human outflow system. Exp.
Eye Res. 51, 691699.
Marshall, G.E., Konstas, A.G., Lee, W.R., 1991. Immunogold ultrastruc-
tural localisation of collagens in the aged human outflow system.
Ophthalmology 98, 692700.
Marshall, G.E., Konstas, A.G., Lee, W.R., 1993. Collagens in the aged
human macular sclera. Br. J. Ophthalmol. 12, 143153.
Maurice, D.M., 1969. The cornea and sclera. In: Davson, H., (Ed.), 2nd Ed.,
The Eye, vol. 1. Little Brown, Boston, MA, pp. 489600.
Mayne, R., 2002. Morphological and chemical composition of connective
tissue: the eye. In: Royce, R.M., Steinmann, B. (Eds.), Connective
Tissue and its Heritable Disorders, 2nd Ed., Wiley-Liss, pp. 145157,
Chapter 1.
McNeilly, C.M., Banes, A.J., Benjamin, M., Ralphs, J.R., 1996. Tendon
cells in vivo form a three-dimensional network of cell processes linked
by gap junctions. J. Anat. 189, 593600.
Meek, K.M., Fullwood, N.J., 2001. Corneal and scleral collagensa
microscopists perspective. Micron 32, 261272.
Meyer, P.A.R., 1988. Patterns of blood flow in episcleral vessels studied by
low dose fluorescein videoangiography. Eye 2, 533536.
Michel, C.C., Curry, F.E., 1999. Microvascular permeability. Physiol. Rev.
79, 703706.
Morrison, J.C., Van Birskirk, M., 1983. Anterior collateral circulation in the
primate eye. Ophthalmology 90, 707715.
Moses, R.A., Grodzki Jr., W.J., Starcher, B.C., Galione, M.J., 1978. Elastin
content of the scleral spur, trabecular mesh, and sclera. Invest.
Ophthalmol. Vis. Sci. 17, 817818.
Neame, P.J., Kay, C.J., McQuillan, D.J., Beales, M.P., Hassell, J.R., 2000.
Independent modulation of collagen fibrillogenesis by decorin and
lumican. Cell Mol. Life Sci. 57, 859863.
Newton, R.H., Meek, K.M., 1998. Circumcorneal annulus of collagen
fibrils in the human limbus. Invest. Ophthalmol. Vis. Sci. 39,
11251134.
Nieuwenhuizen, J., Watson, P.G., Jager, M., Emmanouilidis-van der Spek,
K., Keunen, J., 2003. The value of combining anterior segment
fluorescein angiography with indocyanine green angiography in scleral
inflammation. Ophthalmology 110:16531666.
Ozanics, V., Rayborn, M., Sagun, D., 1976. Some aspects of corneal and
scleral differentiation in the primate. Exp. Eye Res. 22, 305327.
Pace, J.M., Corrado, M., Missero, C., Byers, P.H., 2003. Identification,
characterization and expression of a new fibrillar collagen gene,
COL27A1. Matrix Biol. 22, 314.
Parry, D.A.D., Craig, A.S., 1984. Growth and development of collagen
fibrils in connective tissue. In: Ruggeri, A., Motta, P. (Eds.),
Ultrastructure of the Connective Tissue Matrix, Martinus Nijhoff,
Boston, MA, pp. 3464.
Polatnick, J., Tessa, A.J., Katzin, H.M., 1957. Comparison of collagen
preparations from beef cornea and sclera. Biochim. Biophys. Acta 26,
365369.
Postlethwaite, E.A., Kang, A.H., 1988. Fibroblasts. In: Gallin, J.I.,
Goldstein, I.M., Snyderman, R. (Eds.), Inflammation: Basic Principles
and Clinical Correlates, Raven, New York, pp. 747774.
Quantock, A.J., Meek, K.M., 1988. Axial electron density of human scleral
collagen. Location of proteoglycans by X-ray diffraction. Biophys. J.
54, 159164.
Quantock, A.J., Meek, K.M., Chakravarti, S., 2001. An X-ray diffraction
investigation of corneal structure in lumican-deficient mice. Invest.
Ophthalmol. Vis. Sci. 42, 17501756.
Quigley, H.A., Dorman-Pease, M.E., Brown, A.E., 1991. Quantitative study of
collagen and elastin of the optic nerve head and sclera in human and
experimental monkey glaucoma. Curr. Eye Res. 10, 877888.
Rada, J.A., Achen, V.R., Perry, C.A., Fox, P.W., 1997. Proteoglycans in the
human sclera. Evidence for the presence of aggrecan. Invest.
Ophthalmol. Vis. Sci. 38, 17401751.
Rada, J.A., Achen, V.R., Penugonda, S., Schmidt, R.W., Mount, B.A.,
2000. Proteoglycan composition in the human sclera during growth and
aging. Invest. Ophthalmol. Vis. Sci. 41, 16391648.
Rao, N., Marak, G., Hidayat, A., 1985. Necrotising scleritis: a
clinicopathological study of 41 cases. Ophthalmoogy 92, 15421549.
Riley, G.P., Harrall, R.L., Hazleman, B.L., Watson, P.G., 1995.
Collagenase (MMP1) and (TIMP) in destructive corneal disease
associated with rheumatoid arthritis. Eye 9, 703718.
Rhenberg, M., Ammitzboll, T., Tengroth, B., 1987. Collagen distribution in
the lamina cribrosa and the trabecular meshwork of the human eye. Br.
J. Ophthalmol. 71, 886892.
Robb, J.A., 1977. Virus-cell interactions: a classification of virus causing
human disease. Prog. Med. Virol. 23, 5160.
Roth, A., Muhlendyck, H., de Gottrau, P., 2002. The function of Tenons
capsule revisited. J. Fr. Ophthalmol. 25, 968976.
Sainz de la Maza, M., Foster, C.S., Jabbur, N.S., 1994. Scleritis associated
with rheumatoid arthritis and with other systemic autoimmune diseases.
Ophthalmology 101, 12811286.
Sainz de la Maza, M., Hemady, R.K., Foster, C.S., 1993. Infectious
scleritis: report of four cases. Doc. Ophthalmol. 83, 3341.
Schonherr, E., Witsch-Prehm, P., Harrach, B., Robenek, H., Rauterberg, J.,
Kresse, H., 1995. Interaction of biglycan with type I collagen. J. Biol.
Chem. 270, 27762783.
P.G. Watson, R.D. Young / Experimental Eye Research 78 (2004) 609623622
Selbach, J.M., Gottanka, J., Wittman, M., Lutjen-Drecoll, E., 2000. Efferent
and afferent innervation of primate trabecular meshwork and scleral
spur. Invest. Ophthalmol. Vis. Sci. 41, 21842191.
Selbach, J.M., Schonfelder, U., Funk, R.H., 1998. Arteriovenous
anastomoses of the episcleral vasculature in the rabbit and rat eye.
J. Glaucoma 7, 5070.
Sellheyer, K., Spitznas, M., 1988. Development of the human sclera. A
morphological study. Graefes. Arch. Clin. Exp. Ophthalmol. 226,
89100.
Shauly, Y., Miller, B., Lichtig, C., Modan, M., Meyer, E., 1992. Tenons
capsule: ultrastructure of collagen fibrils in normals and infantile
esotropia. Invest. Ophthalmol. Vis. Sci. 33, 651656.
Spitznas, M., 1971. The fine structure of human scleral collagen. Am.
J. Ophthalmol. 71, 68.
Stone, R.A., Kuwayama, Y., Laties, A.M., 1987. Regulatory peptides in the
Eye. Experientia 43, 791800.
Suzuki, O.T., Sertie, A.L., der Kaloustian, V.M., Kok, F., Carpenter, M.,
Murray, J., Czeizel, A.E., Klieman, S.E., Rosemberg, S., Monteiro, M.,
Olsen, B.R., Passos-Bueno, M.R., 2002. Molecular analysis of collagen
XVIII reveals novel mutations, presence of a third isoform, and possible
genetic heterogeneity in Knobloch syndrome. Am. J. Hum. Genet. 71,
13201329.
Takeuchi, Y., Kodama, Y., Matsumoto, T., 1994. Bone matrix decorin
binds transforming growth factor-beta and enhances its bioactivity.
J. Biol. Chem. 269, 3263432638.
Tengroth, B., Rehnberg, M., Amitzboll, T., 1985. A comparative analysis of
the collagen type and distribution in the trabecular meshwork sclera
lamina cribrosa and the optic nerve in the human eye. Acta Ophthalmol.
Suppl. 173, 9193.
Thale, A., Tillmann, B., 1993. The collagen architecture of the sclera
SEM and immunohistochemical studies. Anat. Anz. 175, 215220.
Thale, A., Tillmann, B., Rochels, R., 1996a. Scanning electron microscopic
studies of the collagen architecture of the human scleranormal and
pathological findings. Ophthalmologica 2103, 137141.
Thale, A., Tillmann, B., Rochels, R., 1996b. SEM studies of the collagen
architecture of the human lamina cribrosa: normal and pathological
findings. Ophthalmologica 210, 142147.
Trier, K., Olsen, E.B., Ammitzboll, T., 1990. Regional glycosaminoglycan
composition of the human sclera. Acta Ophthalmol. 68, 304306.
Van Kuppevelt, T.H., Rutten, T.L., Kuyper, C.M., 1987. Ultrastructural
localization of proteoglycans in tissue using cuprolinic blue according
to the critical electrolyte concentration method: comparison with
biochemical data from the literature. Histochem. J. 19, 520526.
Ward, N.P., Scott, J.E., Coster, L., 1987. Dermatan sulphate proteoglycans
from sclera examined by rotary shadowing and electron microscopy.
Biochem. J. 242, 761766.
Watson, P.G., Hazleman, B.L., 1976. The Sclera and Systemic Disorders,
1st Ed., Saunders, London, pp. 198199.
Watson, P.G