Embed Size (px)
Citation preview

P E R S P E C T I V E S
foods, sugars, saturated fat and meats. Theseadaptations are due, in part, to the mecha-nization and modernization of processesranging from transportation to householdchores. Additionally there is increasing avail-ability and demand for cheaper food options,which tend to be high in both fat and sodiumand low in fibre. Such adaptations are oftenreferred to as ‘Westernization’ — theumbrella term that encompasses thesebehaviours, which are common in NorthAmerica and parts of Europe.
Most of the research into cancer has beendone on people living in North America andEurope, representing only a fraction of theglobal population and their dietary patternsand lifestyle factors. The wide variety of diet,lifestyle and environmental exposures, as wellas genetic variation between populations indeveloping countries, can add valuable infor-mation to our knowledge of the factors thatcontribute to the development of cancer. Theinternational portfolio of cancer studies there-fore needs to be expanded to developingcountries. These types of studies would notonly serve the needs of people in developingcountries, but also progress our overall knowl-edge of cancer aetiology. There are, however,many logistical issues that need to beaddressed when performing epidemiologicalstudies in developing nations. These includedefining research priorities by taking into con-sideration past scientific discoveries so thatefforts are not unnecessarily repeated and lim-ited resources are preserved. Furthermore, keyinfrastructure requirements need to be con-sidered, as well as strengthening the epidemio-logical research capabilities of institutions indeveloping countries.
Regional variation in cancer incidenceIncidence of cancer varies dramaticallybetween geographic regions (FIG. 2); as somecancers are more common in people in thedeveloped world (for example, breast andprostate), others occur more frequently inpeople who live in developing countries (forexample, cervical and stomach). Cancers of the lung have high incidence in bothdeveloped countries and areas undergoing economic development such as China1.Although these regional differences might beexplained by genetic differences among pop-ulations, variations in lifestyles, environmen-tal exposures and medical practices such asscreening are also likely to be importantdeterminants of cancer risk. This assumptionis reinforced by migration patterns that showthat incidence of cancer among migrantschanges to more closely reflect the rates in theadoptive country. This has been observed
125. Love, R. R. et al. Her-2/neu overexpression andresponse to oophorectomy plus tamoxifen adjuvanttherapy in estrogen receptor-positive premenopausalwomen with operable breast cancer. J. Clin. Oncol. 21,453–457 (2003).
126. Santen, R. J. et al. Estrogen production via thearomatase enzyme in breast carcinoma: which cell typeis responsible? J. Steroid Biochem. Mol. Biol. 61,267–271 (1997).
127. Smithers, D. W. An attack on cytologism. Lancet 1,493–499 (1962).
128. Watson, J. V. What does “response” in cancerchemotherapy really mean? Br. Med. J. 283, 34–37(1981).
129. Onuffer, J. J. & Horuk, R. Chemokines, chemokinereceptors and small-molecule antagonists: recentdevelopments. Trends Pharmacol. Sci. 23, 459–467(2002).
130. Hatse, S., Princen, K., Bridger, G., De Clercq, E. &Schols, D. Chemokine receptor inhibition by AMD3100is strictly confined to CXCR4. FEBS Lett. 527, 255–262(2002).
131. Zhang, L., Kharbanda, S., Hanfelt, J. & Kern, F. G. Bothautocrine and paracrine effects of transfected acidicfibroblast growth factor are involved in the estrogen-independent and antiestrogen-resistant growth of MCF-7 breast cancer cells. Cancer Res. 58, 352–361(1998).
132. Bogdanos, J. et al. Endocrine/paracrine/autocrinesurvival factor activity of bone microenvironmentparticipates in the development of androgen ablationand chemotherapy refractoriness of prostate cancermetastasis in skeleton. Endocr. Rel. Cancer 10,279–289 (2003).
133. Kouniavsky, G. et al. Stromal extracellular matrix reduceschemotherapy-induced apoptosis in colon cancer celllines. Clin. Exp. Metastasis 19, 55–60 (2002).
134. Fortney, J. E., Zhao, W., Wenger, S. L. & Gibson L. F.Bone marrow stromal cells regulate caspase 3 activity inleukemic cells during chemotherapy. Leuk. Res. 25,901–907 (2001).
135. Pietras, K. et al. Inhibition of PDGF receptor signaling intumor stroma enhances antitumor effect ofchemotherapy. Cancer Res. 62, 5476–5484 (2002).
136. Zondor, S. D. & Medina, P. J. Bevacizumab: anangiogenesis inhibitor with efficacy in colorectal and othermalignancies. Ann. Pharmacother. 38, 1258–1264 (2004).
137. Liang, Z. et al. Inhibition of breast cancer metastasis byselective synthetic peptides against CXCR4. Cancer Res.64, 4302–4308 (2004).
138. Tamamura, H. et al. T140 analogs as CXCR4 antagonistsidentified as antimetastatic agents in the treatment ofbreast cancer. FEBS Lett. 550, 79–83 (2003).
139. Mihara, M. et al. p53 has a direct apoptogenic role at themitochondria. Mol. Cell 11, 577–590 (2003).
140. Erster, S., Mihara, M., Kim, R. H., Petrenko, O. & Mol, U. M. In vivo mitochondrial p53 translocationtriggers a rapid first wave of cell death in response toDNA damage that can precede p53 target geneactivation. Mol. Cell. Biol. 24, 6728–6741 (2004).
AcknowledgementsThanks are due to B.S. Mann of the Center for Drug Evaluationand Research, FDA, Rockville, Maryland, USA, and to J.C. Chimfrom the Division of Haematology/Oncology, Queen Mary Hospital,Hong Kong, for constructive comments on the manuscript.
Competing interests statementThe author declares no competing financial interests.
Online links
DATABASESThe following terms in this article are linked online to:Entrez Gene:http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=geneAKT | β-catenin | cathepsin G | CXCL12 | CXCR4 | DPPIV | E-cadherin | ERBB2 | FAK | G-CSF | p53 | VCAM1 | VHLNational Cancer Institute: http://cancer.gov/breast cancerAccess to this interactive links box is free online.
NATURE REVIEWS | CANCER VOLUME 4 | NOVEMBER 2004 | 909
Opportunities for cancerepidemiology in developing countries
Tanuja Rastogi, Allan Hildesheim and Rashmi Sinha
S C I E N C E A N D S O C I E T Y
Abstract | Most cancer epidemiologystudies involve people living in NorthAmerica and Europe, which represent onlya fraction of the global population. Thewide variety of dietary, lifestyle andenvironmental exposures, as well as thegenetic variation among people indeveloping countries can provide valuablenew information on factors that contributeto cancer or that protect against it. Whatare the challenges and advantages toperforming large epidemiological studies indeveloping nations?
The incidence of cancer and other chronicdiseases is increasing in developing countriesowing to increased life expectancy andchanges in risk factors that are concomitantwith economic development. The dramaticimprovements in life expectancy that are
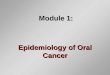
observed in middle-income countries can beattributed to better public health practicessuch as immunization and improved nutrition. This has reduced infant and child mortalities from infectious diseases and malnutrition. By contrast, according to theWorld Health Organization, mortality fromcancer is expected to increase considerably indeveloping countries including Asia, Africaand Latin America (FIG. 1). Although cancerincidence rates are still substantially lower indeveloping countries than in developed coun-tries, the burden of cancer and other chronicdiseases pose an important threat to alreadyoverwhelmed health-care systems.
Changes in lifestyle and diet that occurwith economic development typicallyinclude unhealthy practices such as sedentarybehaviour, smoking, increased total energyintake and consumption of highly refined

910 | NOVEMBER 2004 | VOLUME 4 www.nature.com/reviews/cancer
P E R S P E C T I V E S
and other region-specific exposures canexpand our understanding of cancer epi-demiology beyond what has been gainedfrom developed countries.
Exposure to a wider range of factors. Thehomogeneity (narrow range) of lifestylesand environmental exposures among peopleliving in developed nations has resulted inan incomplete understanding of the rela-tionship between many factors and cancerrisk. People living in developing countriescan be exposed to a wider range of environ-mental factors. The developing world con-sists of many countries with populationsthat are ethnically, culturally and sociallydifferent from each other. Ranges in lifestyleand exposures are further widened by dra-matic socioeconomic differences of popula-tions in countries where both ‘rich andpoor’ subgroups coexist together. Factorsthat might make only a small contributionto cancer risk, such as fat or fibre intake, areeasier to detect over this greater range, assometimes their contribution to cancer riskcan only be detected at very high or lowexposure levels.
Changing patterns. Changes in lifestylesand environmental exposures can be associ-ated with an increase or decrease in diseaserisk, providing useful clues for aetiologicalstudies. Epidemiological studies that corre-late increased or decreased exposure to cer-tain environmental factors with cancer riskneed to be carried out quickly, as manypeople worldwide are rapidly adopting‘Western’ lifestyles. Although not all seg-ments of populations in developing coun-tries are undergoing such changes, it isplainly visible that others, particularlyurban populations, are increasing theirconsumption of fast, energy-dense butnutrient-poor foods, and sedentarylifestyles are becoming the norm. Studies ofthese populations can be used to determinewhich of these factors might contribute tocertain types of cancer.
Patterns of confounding factors. ‘Confounding’is a major challenge to studies examining theassociation between multiple exposures andrisk of disease. When two variables are highlycorrelated and are both associated with diseaserisk, it is difficult to separate them and deter-mine which variable is involved in diseasepathogenesis. If an association between a spe-cific factor and disease can be reproduced in populations with different confounder andcorrelation structures, it is more likely be considered ‘significant’. For example, studies
complex diseases. One approach is to studythe risks of cancer in different populations indifferent environments. Population studiesthat collect data from different races incorpo-rate global variability in both genes and envi-ronmental factors such as different diets,tobacco or pesticide exposures, and theytherefore have enormous potential in expand-ing our understanding of mechanismsinvolved in carcinogenesis.
Research potentialDeveloping countries have unique featuresthat make them important to include in stud-ies of the environmental and genetic factorsthat contribute to cancer risk.
Specific exposures. People living in develop-ing countries or geographic regions outsideof North America or Europe are exposed todifferent environmental factors than peoplein the Western world. Some examplesinclude arsenic in tube-well water of theIndo-Gangatic plains, or exposure to radon,which is produced naturally from the earth,in specific regions of China. There are alsomany dietary variations, especially amongpopulations in Asia, Africa or LatinAmerica, that might be associated with dis-ease risk. Turmeric, a yellow-colour spiceand flavour commonly consumed by mil-lions of people, particularly in South Asia,has traditionally been used as a remedy forliver ailments. Curcumin, a constituent ofturmeric, is a phytochemical that is cur-rently being researched for its anti-tumourproperties, such as inducing cell-growthinhibition and apoptosis. Research on these
with the incidence of colon cancer in Japanesepeople emigrating to Hawaii and SanFrancisco2. Additionally, the incidence ofprostate and breast cancers are low amongChinese people in Asia, but increases havebeen observed when these people move to theUnited States of America3. Dramatic increasesin cancer incidence have also occurred withincountries that experienced massive economicdevelopment in the past 50 years1. Forinstance, younger generations of Japanese(born after 1930) now have a similar if notgreater incidence of colorectal cancers thantheir US Caucasian counterparts4. So aslifestyles also change in developing countries,we are likely to see a significant rise in the inci-dence of cancers that have previously beenassociated with developed countries, such asbreast, colon, prostate and lung cancers.
Both environment and genetic variationare important factors in the aetiology of manychronic diseases. Genetic variation causesmany metabolic differences between individ-uals, and there is much interest in under-standing the potential impact of this variationon susceptibility to cancer and cancer patho-genesis. Specific mutations in single geneshave been reported to greatly increase the riskof some types of cancer, although the preva-lence of these mutations is rare at a popula-tion level. By contrast, common genetic poly-morphisms that contribute only a modestvariation in risk can have a greater impact onpublic health, especially in conjunction withenvironmental exposures.
Understanding these gene–environmentinteractions is one of the main challenges inunravelling the aetiology of cancer and other
World
Established market economy
Former socialist economy
Latin American and Caribbean
China
Sub-Saharan Africa
Other parts of Asia and islands
India
Middle Eastern crescent
0 50 100 150 200
Increase in deaths from cancer (%)
104%
26%
53%
144%
145%
149%
154%
158%
181%
Figure 1 | Changes in cancer mortality by region. According to the World Health Organization, deathfrom cancer is expected to increase 104% worldwide by the year 2020. The largest increases arepredicted to occur among people living in developing countries (Latin America, the Caribbean, Asia, theMiddle East and Africa) in comparison with those in developed countries (established market economiesand the former Soviet economy). Although actual cancer incidence rates are still lower in developingcountries than in North America and Europe, the rise in cancer-related deaths will represent a significantburden to the already overwhelmed health systems in developing countries. Data taken from REF. 53.

P E R S P E C T I V E S
Accuracy in assessment. Another challenge toepidemiological studies of environmental fac-tors and disease risk is measuring levels ofexposure to a given agent. Error in diet assess-ment, for instance, has long been recognizedas a potentially serious problem in nutritionalepidemiological research that can substan-tially attenuate risk estimates. Problems inaccurately determining food intake might
into the effects of vegetarianism are gener-ally confounded by other aspects of an over-all healthy lifestyle among Western popula-tions, such as higher amounts of exerciseand lower alcohol and tobacco use. In India,however, people are vegetarians for religiousreasons and are otherwise likely to have sim-ilar lifestyles to the rest of the population.Also, in developed countries, factors such as
increased physical activity are confoundedby factors such as higher socio-economicstatus, which is also related to better health.However, poorer groups tend to be moreactive in developing countries. The effectsof physical activity on cancer risk can there-fore be more clearly evaluated by assessingdata from both developed and developingcountries.
NATURE REVIEWS | CANCER VOLUME 4 | NOVEMBER 2004 | 911
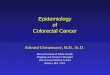
c Incidence of lung cancer
<5.7<16.7<27.8<48.4<95.5
a Incidence of stomach cancer
<5.9<9.6<14.6<22.0<70.0
b Incidence of cervical cancer
<9.3<16.1<23.8<35.8<93.9
d Incidence of breast cancer
<19.3<26.1<36.0<54.2<91.6
e Incidence of prostate cancer
<7.6<14.5<23.7<34.7<104.3
Figure 2 | Global variations in cancer incidence for specific cancers. There is substantial global variability in cancer incidence (measured as age-standardized rates) occurring in people living in developing countries (a–c) and those in developed nations (d,e). a | The incidence of stomach cancer for men of allages is highest (orange and red) in developing countries such as Asia and South America, and lowest (light and dark green) in North America, parts of Africa, Indiaand Australia. b | The incidence of cervical cancer is also high in developing regions of the world including Latin America, Africa and India, and is low (green) inNorth America, Europe and Australia. c | Lung cancer incidence is currently high in developed countries as well as those countries undergoing economictransition, such as China. d,e | Cancers with the highest incidence in developed countries include breast and prostate cancer, which occur most commonly inNorth America, Europe and Australia, and with much lower incidence in Asia and Africa. These differences highlight the role that environmental and lifestyle factorssuch as diet have in cancer development. Data from REF. 54.

912 | NOVEMBER 2004 | VOLUME 4 www.nature.com/reviews/cancer
P E R S P E C T I V E S
investigations in developing countries suchas Asia, Africa and Latin America17–19. Also,helicobacter pylori infection has been associ-ated with a two- to three-fold elevation inrisk for stomach cancer in epidemiologicalinvestigations20. Studies on hepatocellularcarcinoma from Asia and Africa indicatethat persistent hepatitis B infection and afla-toxin exposure can act synergistically toincrease cancer risk21–25. So for infectiousdisease-related cancers, we are now at thenext stage of research where attention isfocused on how to prevent cancer-causinginfections. Novel screening strategies andvaccines are already being developed for cervical cancer prevention that is caused by HPV26. Also, studies in Taiwan havereported reduced rates of hepatocellularcarcinoma after widespread vaccination ofchildren against hepatitis B27. Other keyareas of infectious disease research that needto be expanded include surveillance for bothinfection with a particular agent and forcancer, as well as the effects of promotingcancer prevention programmes. For a list ofother agents that contribute to cancerpathogenesis, see TABLE 2.
Environmental and occupational exposures.People in developing countries are exposed tobroader ranges of occupational and environ-mental hazards, as more people are involved inmanufacturing, farming, mining or otherindustrial occupations than developednations. Research in China, for instance, hasshown a positive association between lungcancer and radon gas exposure28, which is highin some homes and among undergroundminers. In both China and India, indoor airpollution due to burning of coal and biomassfor cooking and heating in homes has alsobeen associated with lung cancer29–34. Studiesare also underway to analyse levels of arsenic,which has been associated with bladder andlung cancers, in the drinking water inBangladesh, India, Chile, Taiwan andChina35–41. Further research in these areasmight provide important and unique infor-mation that cannot be gained from studies inthe developed world and ultimately used incancer-prevention efforts.
The prevalence of tobacco smoking, clearlyan important risk factor for cancer, is high indeveloping countries, with over 80% of theworld’s smokers living in low- or middle-income countries, and a disproportionatelyhigh number of these people being in EastAsia42. Moreover, the forms of tobacco that areused vary in developing countries. Smoking ofbidis — small unfiltered cigarettes that arehand-rolled in a temburni leaf — and chewing
of foods with high salt contents such as saltyfish, which is consumed in high levels in sev-eral East Asian countries, has been associatedwith gastric cancer incidence in China, Japanand Korea9–14.
In their report, Food, Nutrition and thePrevention of Cancer: A Global Perspective, aninternational panel of experts recommendedthat comprehensive dietary studies should beconducted in diverse populations, includingthose that consume low and high levels ofplant proteins, cereal intake, starchy roots andtubers, and bioactive components of vegetar-ian diets and spices15. In TABLE 1 we list certaindietary components that are associated withspecific populations and that have not beenpreviously studied extensively. Little is knownabout how many of these dietary componentsinfluence cancer risk. It is therefore importantto study a range of diets consumed by theworld’s population to gain a broader under-standing of its relation with the diseaseprocess — only analyzing diets of NorthAmericans and Europeans provides a limitedview of how diet can increase or decrease risk.
Infectious agents. Approximately 20% ofcancers among men and women in develop-ing countries are attributable to infectiousagents, compared with 9% in developedcountries16. Advances in our understandingof cancer mechanisms have therefore beenmade by studying infectious disease-relatedcancers in developing countries. The role ofHPV (human papilloma virus) infection incervical cancer aetiology has been clearlydemonstrated through epidemiological
account for some of the inconsistency in thenutrition and cancer research from NorthAmerica and Europe. Estimating food con-sumption in developing countries might beeasier, as food represents a larger percent oftotal expenses and is usually prepared athome. Preliminary evidence indicates thatdietary assessment error might be lower inIndia5. Other researchers have speculatedthat recall of physical activity amongChinese is more likely to be accuratelyreported, as major forms of energy expendi-ture are not leisure-time but transportationor occupation-related activities, such asbicycling to work. Such essential activitiesare done on a daily basis and can be moreaccurately recalled, thereby reducing measurement error.
Cancer-related factors to be studiedThere are so many advantages to performingepidemiological studies in the developingworld, but which environmental factors aremost important to evaluate immediately forassociation with cancer risk?
Diet. So far, much of the diet and cancerresearch conducted in developing nations hasfocused on specific diet components. Forexample, studies in South and Southeast Asiahave elucidated the association between oralcancer and intake of areca nut — the seed of the betel palm that is chewed with leaves ofthe betel pepper and lime as a digestive stimu-lant and narcotic in southeastern Asia6–8. Thisnut has been found to be carcinogenic evenwhen consumed without tobacco. Also, intake
Table 1 | Dietary factors to examine in developing countries*
Dietary factor Region Cancer risk
Meat — overall intake, specific South and Central Colorectal cancer (potential)specific types of meat, cooking America, Chinamethods, fat content, intake of processed meats
Soy Southeast Asia Breast cancer (potential)
Pulses, lentils and beans Central and South NSAmerica, South Asia, Africa
Vegetarian diets South Asia Colorectal and othercancers (potential)
Micronutrient deficient — Rural Asia and Africa NScarbohydrate-dense diets
Allium vegetables East Asia Colorectal and prostatecancers (potential)
Spices (for example, curcumin South and Southeast Colorectal cancer (potential)in turmeric) Asia, Caribbean
Vegetable oils: palm oil, coconut oil, Eastern Europe, South NSrapeseed/flaxseed oils, and trans and Southeast Asiafatty acids in hydrogenated oils
*See ref. 15. NS, not studied; there is currently no information available on how these diet componentsinfluence risk.

P E R S P E C T I V E S
oestrogen levels51. Reproductive factors alsomodulate oestrogen levels and can influencecancer risk. These factors include total life-time oestrogen exposure, the time span frommenarche to menopause, parity, lactation andage at first birth.
Studies in countries such as Brazil andIndia provide opportunities to better under-stand these mechanisms, as the prevalence ofoverweight and obesity is rising, if not highalready, among certain segments of the popu-lation. Different populations often have varying body shapes — for example, theprevalence of central obesity is particularlyhigh among South Asians. Compared withWestern nations, there are also significant dif-ferences in reproductive patterns among peo-ple in developing nations, where traditionalsegments of the population tend to have morechildren at younger ages. This is in juxtaposi-tion with women in major urban regions whoare employed and have fewer children at laterages, which is more typical of the Westernworld. These variations provide a potentiallyrich opportunity to compare how differencesin parity contribute to hormone-relatedbreast and endometrial cancers.
ChallengesFor cancer epidemiology research to be sup-ported and sustained in developing countries,specific issues such as the development ofinfrastructure, strengthening of the epidemi-ological research capabilities, and the foster-ing of fair and effective collaborations mustbe addressed. Establishing all or even some ofthese factors can be major undertakings inregions where the capacity for cancer researchis in a formative stage.
Infrastructure. The challenges that are facedin physical infrastructure involve improvingthe quality of epidemiological data that iscollected, as well as improving systems forbiological specimen collection, processingand storage. The existence of many basic ele-ments, such as registries to determine diseaseincidence or mortality data, or surveys ofenvironmental exposures, might requireimplementation. Population studies of can-cer incidence will become logistically easier asimprovements are made in access to medicalcare, diagnostics, laboratories and record/reg-istry systems. There are some health-care sys-tems already in place in developing countriesthat can be used as models, such as vaccina-tion programs or national nutrition surveys.The information gained from these estab-lished infrastructures can be used in settingup epidemiological population-based studiesand cancer screening programs.
tobacco are particularly common amonglower-income groups of Asia. It will also beimportant to study the interaction betweentobacco use and other features of developingcountries, such as the high incidence of tuber-culosis, indoor air pollution and radon expo-sure. Furthermore, in developing countriesthere is much need for public health educationon the risks of tobacco use, so this data can beused to support government policies designedto reduce tobacco use.
Another major environmental and occupa-tional factor that contributes to lung cancerrisk is fuel exhaust, which contains diesel parti-cles and polycyclic aromatic hydrocarbons43.This association is not well-studied in develop-ing countries, where exhaust levels are high.The interactions between exhaust and otherlung carcinogens, such as tobacco use, radon or silica, can also be examined. The use of pes-ticides has also increased drastically in develop-ing countries over the last three decades, owingto increased crop production44. These chemi-cals have been associated with leukaemia,lymphoma and prostate cancer risk45, and rep-resent important areas for further research.Studies investigating benzene exposure ofworkers in the shoe and paint industries, whichare common in developing countries46, canprovide information about the dose-responserelationship between benzene and cancerssuch as lymphoma, leukaemia and even lungcancer. Moreover, aromatic amines are stillextensively used in various industries for textiledye and rubber making in India, China andSoutheast Asia. Research into the associationbetween these compounds and cancer mightexpand our understanding of its potential rolein bladder cancer.
Physical activity. Research in developing coun-tries on the association between physical activity and cancer can provide valuable infor-mation on the magnitudes and types of activi-ties that can protect people from cancer.Although there have been many studies into
the affects of physical activity, energy balanceand obesity on disease incidence in NorthAmerica and Europe, these types of studiesshould be expanded to developing coun-tries. Both the level and type of physicalactivity vary dramatically between devel-oped and developing countries. Mainsources of energy expenditure in economi-cally developed countries are derived fromleisure-time exercise, which is a focus ofboth research and health promotion.Studies in China, India and Brazil indicatethat the main forms of energy expenditurearise from occupation and transportation-related activities, as well as chores and othertypes of non-leisure-related exercise47–49.Additionally, levels of physical activitymight have wider ranges in developingnations, owing to the diversity of activitiesundertaken and because of the dramaticdifferences of ‘rich and poor’ subgroupswithin the same population
Hormones. Developing countries providemany opportunities to examine a number ofunique hormonally-related variables. Forexample, they can address the effects of widerranges in body sizes — from underweight toobese — which in addition to physical activ-ity are believed to affect cancer risk by modu-lating hormone levels. Excess body weight orincreases in abdominal fat have been reportedto alter serum levels of insulin and insulin-like growth factor-1 (IGF1), which functionto stimulate cell proliferation, inhibit apopto-sis and promote angiogenesis50,51. Moreover,weight gain often results in insulin resistance,leading to further production of insulin bythe pancreas. Cancer researchers are currentlyexamining the association between obesity-related increased insulin levels and insulinresistance with risk of colon, prostate, breastand pancreatic cancer50. Adiposity is alsothought to influence risk of breast canceramong post-menopausal women andendometrial cancer by increasing circulating
NATURE REVIEWS | CANCER VOLUME 4 | NOVEMBER 2004 | 913
Table 2 | Environmental factors and cancer risk in developing countries
Cancer Regions Environmental factors Referencestype that increase risk
Cervical Asia, Africa, Human papilloma virus 17–19 Latin America
Liver Egypt, East Asia, Africa Hepatitis B and C virus, aflatoxin 21–25
Oral India, Southeast Asia Areca nut, tobacco chewing 6–8,55,56
Stomach China, Japan, Korea, Salt, high intake of salty foods, salty 9–14,20,57 Chile fish, Helicobacter pylori infection
Lung China, India, Radon exposure, indoor air pollution, 28–34,58,59tobacco smoking
Thyroid India Radiation exposure 60

914 | NOVEMBER 2004 | VOLUME 4 www.nature.com/reviews/cancer
P E R S P E C T I V E S
participants, the loss to follow-up can biasany observed association between particulardietary factors and cancer incidence.
Another obstacle that is faced by epidemio-logical studies in developing countries is that,owing to high illiteracy levels and lack of offi-cial addresses among certain segments of thepopulation, follow-up might be difficult —particularly when mailed questionnaires areinvolved. This can be addressed, in part, byhaving researchers visit households to collectboth exposure and outcome data. Whereastrained, non-medical research assistants can beappropriate in some locations, research nursesor paramedical technicians might be requiredin others. One advantage to studies carried outin developing nations is that in-person homeinterviews can cost substantially less than theywould in developed nations, where thisresearch approach is prohibitively expensiveowing to higher labour costs. Informationobtained through household visits can also besupplemented with medical records, doctor’sreports and laboratory test results, if available.
Follow-up is difficult in populations that aretransient, such as migrant groups or labour-ers who shift from one geographic region tothe next in search of employment. Failure tofollow participants carefully can bias thestudy results if the loss primarily occurs inone particular population that has differentexposures or disease incidence than the oth-ers. For example, the likelihood of follow-upof individuals in slums or shanty towns indeveloping countries is low, as these areas areoften unplanned and lack official addresses.As individuals living in slums also have lessaccess to health care, cancer cases wouldmore often go undiagnosed and would neverbe recorded in a cancer registry in compari-son with middle-income participants. In astudy that obtains cancer outcome data solelyfrom cancer registries, data would incorrectlyshow that participants living in slums havelower incidence of cancer than the middle-income subjects. As the diets and lifestyles ofpeople living in these deprived areas differsignificantly from those of middle-class
Important factors for conducting prospec-tive cohort studies include being able to linkcancer registry data with study subjects andthe ability to follow up subjects to obtainadditional information on exposure and pos-sibly outcome that is not usually availablethrough registries. For a list of the various fea-tures of different study designs, see TABLE 3.Developed countries generally have high-quality national registries that record cancerincidence and mortality data, such as the USNational Cancer Institute’s Surveillance, Epi-demiology and End Results (SEER) database.The situation varies among developing coun-tries — some areas such as Shanghai, China,already have well-linked population-basedcancer registries, whereas other countrieshave few or no records of cancer incidence.
Patient follow-up is also difficult in somepopulations. It is important that individualsthat participate in a prospective cohort study (TABLE 3) are not ‘lost’ over the course ofthe study (loss to follow-up), as no disease information would be available.
Table 3 | Epidemiological study designs
Study type Time Basic design Sample Data and samples Knowledge gained frame size collected
Cross-sectional Short term One-time data Tens to Questionnaire, biological Population distribution of exposures (for survey collection thousands samples* example, intake of vegetables, serum
cholesterol levels, prevalence of geneticpolymorphisms)
Case-control Several Retrospective design. Hundreds Questionnaire, biological Questionnaire data and biological measuresstudy years Compare risk factors to possibly samples*‡ compared between diseased and non-
of cases with disease thousands diseased people. Case-control bias, whereand controls without it is possible that disease status affectsdisease questionnaire responses or biomarker levels
is a concern. Biomarkers with a long half-life (for example, adipose fatty-acid levels) and genetic polymorphisms might not be influenced by this bias
Cohort study Decades Prospective design. Thousands Questionnaire, biological Questionnaire data and biomarker levels Cause-effect examined to tens of samples* are useful (without biases inherent in case-with a temporal thousands control studies) and compared betweensequence of events. people who develop disease and thoseHealthy subjects who remain disease-freeprovide information (for example, diet, occupation, medical history, and so on) and are then followed for health-related events (for example, cancer, heart disease, diabetes) for a given period of time
Clinical trials Variable Prospective evaluation Tens to Exposure is determined Efficacy of intervention evaluated based onof specific intervention thousands by the investigator and biomarker levels and/or disease oroptimally randomized is controlled (for example, intermediate status of disease (for example, where subjects and vitamin E supplementation, effect of dietary fat and fibre intake on investigators are vaccine trial). Repeated colorectal cancer or polyp occurrence).blinded to the biological sampletreatment status collection to assess
effect of intervention
*An array of biological samples are used in epidemiological studies and include the following examples: blood components, saliva/buccal cells from mouthwash, urine,faeces, nails, hair, and more invasive samples include biopsies of adipose tissue, rectal biopsies or tumour blocks. DNA for use in genetic analyses can be extracted fromblood and buccal cells as well as from tumour blocks. ‡Use of biological samples in case-control studies need to be carefully evaluated as disease status mightsubstantially effect biological measures.

P E R S P E C T I V E S
goals of the study and to explain how find-ings might improve the well-being of bothlocal and global populations. It is impor-tant for investigators to transfer knowledgeand scientific skills to scientists of collabo-rating developing countries whenever pos-sible. Equitable credit should also be nego-tiated and given to both sets of researchersin the form of shared authorships and pre-sentations at international scientific confer-ences. The promotion of technologieswithin developing countries by local scien-tists should also be encouraged throughtechnology transfer programmes supportedby both private and public governmentalagencies.
Obtaining accurate cause-specific mortalityinformation from death registries is often diffi-cult in some developing countries owing toincomplete death reports, and is especiallyimportant for prospective cohort studies, inwhich both cancer incidence and mortality areassessed. Death registry data can often be sup-plemented with questionnaires that are givento the next-of-kin of deceased study partici-pants. Providing family members with ques-tionnaires about the deceased individual’ssymptoms and signs of illness can be an alter-nate method for tracking causes of death indeveloping countries52. However, the accuracyand validity of these questionnaires should beevaluated in known study populations beforeimplementation. Retrieving medical records ofdeceased study participants is important, par-ticularly for determining the type of cancerthat the deceased individual had.
Biological sample collection is anotherintegral part of any epidemiological study, butis also a challenge in developing nations.Specimen collection in hospital-based case-control studies can be easily managed, whereaspopulation-based samples are much more dif-ficult to collect. Compliance can be low whensubjects are recruited from the general popu-lation, especially for blood collection. Even ifsubjects agree to give blood, the amountmight be minute, so more sensitive laboratorymethodologies or other types of biologicalspecimen collection (blood spots, DNA frommouthwash) need to be developed. Educationor appropriate incentives can increase partici-pation. Other challenges involve the storage ofsamples at the appropriate temperature, trans-port to the processing centre, correct process-ing and long-term storage, which can beexpensive. So without a functional infrastruc-ture, it is not always possible to carry out certain types of epidemiological studies indeveloping nations.
Training. Epidemiology research capabili-ties must be strengthened in non-Westernregions of the world in order for globalstudies of cancer incidence and preventionto be sustained. Scientists in developingcountries must be properly trained to allowcancer research programs to develop. Thiscan be achieved, in part, through collabora-tive research, which not only allows scien-tists in developing countries to learn newresearch skills, but also allows scientistsfrom developed nations to better under-stand local scientific capabilities and customs. This is important, as patient participation often depends on people’strust of local institutes and investigators. Itis also important to develop programs to
train new epidemiologists of developingregions, improve the interactions between sci-entists from developed and developing coun-tries, and support education programs formid-career scientists of developing nations.Ultimately, the creation of accredited gradu-ate schools of public health and epidemiologyin these countries will improve the level ofresearch in these regions of the world.
Fair and effective collaborations. The successof research in developing countries alsodepends on fostering fair collaborationsbetween investigators from developed anddeveloping countries. One role of investigatorsin developed countries is to clearly define the
NATURE REVIEWS | CANCER VOLUME 4 | NOVEMBER 2004 | 915
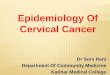
Box 1 | Continuum of research
Research into risk factors associated with cancer develops along a continuum that spans frombasic laboratory to epidemiological and, ultimately, prevention/policy research. The stages ofresearch development generally include basic laboratory research, early epidemiology anddiscovery-stage studies, aetiological studies in humans, prevention studies, late-stage preventionstudies and, ultimately, policy and implementation research. Whereas prevention studiesaddress whether the preventive measure works (proof of concept and efficacy), late-stageprevention studies aim to prove effectiveness in different settings (for example, testing whetherPap smear screening for cervical cancer works in developing countries even though it has beenproven be effective in the USA).
Whereas some research topics, such as genetic markers of cancer, are on the left side of thecontinuum (stages 1–2, red boxes), others — including tobacco and cancer research — oftenbelong in the realm of prevention and policy research (stages 5–6, yellow boxes) as a largenumber of epidemiological studies have implicated its role in carcinogenesis. Findings derivedfrom studies conducted in stages 1–2 are universally applicable regardless of the geographiclocation of the laboratory (provided that laboratory conditions are standard). However, studiesbecome more population-specific as one moves right across the spectrum, with preventionstudies being conducted in settings where the prevention strategy will be applied. Some areas ofresearch have subtopics that span the spectrum. Studies of HPV and cervical cancer now focuson prevention and policy research (stages 5–6), however the role of nutritional status in HPVinfection is a subtopic that requires basic epidemiological research (stages 1–3). As biologicalmechanisms of exposures that are examined in early and in aetiological epidemiological studiescan be further understood with more detailed basic research, the initial stages are reversible(stages 1–3). This overall construct displays stages in chronological order and not necessarily thedepth and diversity of studies required within each stage.
Basic research Prevention and policy research
Basic laboratory research stage
Early epidemiological and discovery stage
Confirmatory/aetiological
Policy andimplementationresearch
Early prevention research
Late prevention research stage
Research is universally applicableResearch is universally applicable or region specificResearch is region specific
1
2
3
6
5
4

916 | NOVEMBER 2004 | VOLUME 4 www.nature.com/reviews/cancer
P E R S P E C T I V E S
reasons that the incidence of these cancers islow in developing regions include the lowerprevalence of risk factors such as obesity.Alternatively, there could be a high preva-lence of preventive factors such as increasedintake of chemopreventive agents (phytoe-strogens found in soy products or curcuminin spices), or higher levels of physical activ-ity. Studying cancer in these populations istherefore an important approach to identi-fying possible factors that could be appliedto cancer prevention worldwide.
Tanuja Rastogi, Allan Hildesheim and Rashmi Sinha are at the Division of Cancer
Epidemiology & Genetics,National Cancer Institute,
NIH, DHHS, 6120 Executive Boulevard,Rockville, Maryland 20852, USA.
Correspondence to R.S.e-mail: [email protected]
doi:10.1038/nrc1475
1. Parkin, D. M., Whelan, S. L., Ferlay, J., Teppo, L. &Thomas, B. D. Cancer Incidence in the Five ContinentsVIII. IARC Scientific Publication No. 155 (InternationalAgency for Research on Cancer (IARC) Press, Lyon,France, 2002).
2. Dunn, J. E. Cancer epidemiology in populations of theUnited States — with emphasis on Hawaii andCalifornia — and Japan. Cancer Res. 35, 3240–3245(1975).
3. Yu, H., Harris, R. E., Gao, Y. T., Gao, R. & Wynder, E. L.Comparative epidemiology of cancers of the colon,rectum, prostate and breast in Shanghai, China versusthe United States. Int. J. Epidemiol. 20, 76–81 (1991).
4. Yiu, H. Y., Whittemore, A. S. & Shibata, A. Increasingcolorectal cancer incidence rates in Japan. Int. J. Cancer109, 777–781 (2004).
5. Hebert, J. R. et al. Sources of variability in dietary intake intwo distinct regions of rural India: implications for nutritionstudy design and interpretation. Eur. J. Clin. Nutr. 54,479–486 (2000).
6. Zain, R. B. Cultural and dietary risk factors of oral cancerand precancer — a brief overview. Oral Oncol. 37,205–210 (2001).
7. Gupta, P. C., Sinor, P. N., Bhonsle, R. B., Pawar, V. S. &Mehta, H. C. Oral submucous fibrosis in India: a newepidemic? Natl Med. J. India 11, 113–116 (1998).
8. Sharma, D. C. Betel quid and areca nut are carcinogenicwithout tobacco. Lancet Oncol. 4, 587 (2003).
9. Lee, J. K., Park, B. J., Yoo, K. Y. & Ahn, Y. O. Dietaryfactors and stomach cancer: a case-control study inKorea. Int. J. Epidemiol. 24, 33–41 (1995).
10. Lopez-Carrillo, L., Hernandez Avila, M. & Dubrow, R. Chilipepper consumption and gastric cancer in Mexico: acase-control study. Am. J. Epidemiol. 139, 263–271(1994).
11. Ji, B. T. et al. Dietary habits and stomach cancer inShanghai, China. Int. J. Cancer 76, 659–664 (1998).
12. Ye, W. M. et al. Diet and gastric cancer: a casecontrolstudy in Fujian Province, China. World J. Gastroenterol.4, 516–518 (1998).
13. Ngoan, L. T., Mizoue, T., Fujino, Y., Tokui, N. &Yoshimura, T. Dietary factors and stomach cancermortality. Br. J. Cancer 87, 37–42 (2002).
14. Tsugane, S., Sasazuki, S., Kobayashi, M. & Sasaki, S.Salt and salted food intake and subsequent risk of gastriccancer among middle-aged Japanese men and women.Br. J. Cancer 90, 128–134 (2004).
15. World Cancer Research Fund. Food, Nutrition and thePrevention of Cancer: A Global Perspective (WorldCancer Research Fund, American Institute for CancerResearch, Washington DC, 1997).
16. Pisani, P., Parkin, D. M., Munoz, N. & Ferlay, J. Cancer andinfection: estimates of the attributable fraction in 1990.Cancer Epidemiol. Biomarkers Prev. 6, 387–400 (1997).
17. Franco, E. L., Schlecht, N. F. & Saslow, D. Theepidemiology of cervical cancer. Cancer J. 9, 348–359(2003).
18. Munoz, N. Human papillomavirus and cancer: theepidemiological evidence. J. Clin. Virol. 19, 1–5 (2000).
also hinders future endeavours and fostersmistrust. Some governments have banned theexport of biological samples from their coun-tries. In forming research collaborations withdeveloping countries, scientists should notonly outline the potential for technologytransfer, but can also make provisions forsome sample export permissable. As geneticanalysis can be a controversial topic regardlessof where it takes place, complete transparency,involving explanations of research protocolsand objectives, can help address this issue.
Social issues. Investigators in developingcountries are faced with unique social issuesthat range from cultural and gender to super-stitions or concerns about being taken advan-tage of. Guidance from local scientists, whoare most familiar with the beliefs of the popu-lation, is the best way to address most of theseissues. Outreach and education programmesthat familiarize communities with researchcan also be undertaken to improve participa-tion, often involving local community or religious leaders.
Future directionsDeveloping countries have already made sig-nificant contributions to our understandingof cancer aetiology (TABLE 2). Examinationsinto hot-spots or exposure–disease relation-ships unique to specific geographic regionshave advanced our knowledge of the factorsthat contribute to cancer risk. Developingcountries often have vastly different sub-groups coexisting together. Whereas somegroups lead traditional lifestyles that havenot changed for generations, such as in ruralvillages of Asia, others in urban areas ofLatin America and Asia have undergonerapid changes owing to economic develop-ment. For instance, gains in women’s educa-tion and improvements in nutritional statusalso lead to earlier menarche and latermenopause in women, extending the periodof hormone exposure, particularly oestro-gen, which is associated with breast cancerrisk. Modernization and mechanization ofprocesses such as transportation and house-hold chores are also resulting in reduced lev-els of physical activity in urban areas aroundthe world. These forces of globalization arehomogenizing lifestyles worldwide, increas-ing the urgency of performing epidemiologi-cal studies in developing regions.
In addition to studies of cancers typicallyassociated with developing countries,research should expand to include othercancers, particularly those that have lowerincidence rates in these areas such as lung,prostate, breast and colon cancers. Some
Bureaucracy. The large amount of bureau-cracy that is often required to initiate and tocarry out epidemiological studies in somecountries is another impediment to research.Bureaucratic obstacles can arise from govern-mental regulatory agencies in both developedand developing nations. Although it is neces-sary to have rules to guide research practicesin other countries, manoeuvring throughcomplicated and often dated regulations canbe daunting. One serious long-term conse-quence of overwhelming amounts of bureau-cracy is that collaborative research plans areoften substantially delayed or cancelled.
Issues surrounding internal study bureau-cracy is another concern that can beaddressed by establishing clear agreementsand guidelines during the planning stagesand ‘oversight’ or ‘steering’ committees.These usually consist of a group of knowl-edgeable researchers that are not the mainstudy investigators, but are tangentiallyinvolved. It is important to outline whichoversight or steering committees will moni-tor progress, and which will provide scientificand management guidance.
Ethical issues. Some studies in developingcountries have been conducted without theinformed consent and overview of ethicalcommittees — either these committeeswere never fully established, or the subjectswere uninformed of their rights and there-fore were coerced into study participation.Other examples of ethical lapses in researchconducted in developing countries includeimplementing potentially harmful inter-ventions when subjects were not fully pro-tected from side effects, or using coercionto improve participation. Data and sampleshave also been collected from people indeveloping counties without consent of thegovernment or local scientists.
It is important that scientists from devel-oping countries and their collaborators fromdeveloped countries follow international ethi-cal regulations when conducting population-based studies (see Further information forwebsites for international standards for con-duct of ethical research). This is not only nec-essary to allow researchers from developingcountries to obtain recognition for contribu-tions, but also because failure to follow theseregulations can prevent subjects from partici-pating in future studies. An important con-cern in the last few years has involved theunauthorized collection, export and analysesof biological samples, and the lack of benefitto local scientists and especially to local popu-lations. Unapproved collection and shipmentof biological samples is not only wrong but

P E R S P E C T I V E S
projected to 2020 (Harvard University Press, Cambridge,Massachusetts, 1996).
54. Ferlay, J., Bray, F., Pisani, P. & Parkin, D. M. CancerIncidence, Mortality and Prevalence Worldwide,Globocan, 2000 (International Agency for Research onCancer (IARC) Press, World Health Organization, Lyon,France, 2001).
55. Sham, A. S., Cheung, L. K., Jin, L. J. & Corbet, E. F. Theeffects of tobacco use on oral health. Hong Kong Med. J.9, 271–277 (2003).
56. Zain, R. B. et al. Oral mucosal lesions associated withbetel quid, areca nut and tobacco chewing habits:consensus from a workshop held in Kuala Lumpur,Malaysia, November 25-27, 1996. J. Oral Pathol. Med.28, 1–4 (1999).
57. Lee, S. A. et al. Effect of diet and Helicobacter pyloriinfection to the risk of early gastric cancer. J. Epidemiol.13, 162–168 (2003).
58. Pandey, M., Mathew, A. & Nair, M. K. Globalperspective of tobacco habits and lung cancer: a lessonfor third world countries. Eur. J. Cancer Prev. 8,271–279 (1999).
59. Zhong, L., Goldberg, M. S., Gao, Y. T. & Jin, F. A case-control study of lung cancer and environmental tobaccosmoke among nonsmoking women living in Shanghai,China. Cancer Causes Control 10, 607–616 (1999).
60. Nagataki, S. & Nystrom, E. Epidemiology and primaryprevention of thyroid cancer. Thyroid 12, 889–896 (2002).
AcknowledgementsWe thank Mustafa Dosemeci for his input on the role of environ-mental risk factors in cancer aetiology.
Competing interests statementThe authors declare no competing financial interests.
Online links
DATABASESThe following terms in this article are linked online to:National Cancer Institute: http://www.cancer.gov/breast cancer | cervical cancer | colon cancer | lung cancer |prostate cancer | stomach cancer
FURTHER INFORMATIONBelmont Report:http://www.nihtraining.com/ohsrsite/guidelines/belmont.htmlDeclaration of Helsinki:http://www.nihtraining.com/ohsrsite/guidelines/helsinki.htmlGLOBOCAN 2000 — Cancer Incidence, Mortality andPrevalence Worldwide:http://www-dep.iarc.fr/globocan/globocan.htmlNuremberg Code:http://ohsr.od.nih.gov/guidelines/nuremberg.htmlProtection of Human Subjects:http://www.nihtraining.com/ohsrsite/guidelines/45cfr46.htmlSEER: http://seer.cancer.gov/Access to this interactive links box is free online.
19. Clifford, G. M., Smith, J. S., Aguado, T. & Franceschi, S.Comparison of HPV type distribution in high-gradecervical lesions and cervical cancer: a meta-analysis. Br.J. Cancer 89, 101–105 (2003).
20. Huang, J. Q., Zheng, G. F., Sumanac, K., Irvine, E. J. &Hunt, R. H. Meta-analysis of the relationship betweencagA seropositivity and gastric cancer. Gastroenterology125, 1636–1644 (2003).
21. Montalto, G. et al. Epidemiology, risk factors, and naturalhistory of hepatocellular carcinoma. Ann. NY Acad. Sci.963, 13–20 (2002).
22. Yu, M. C., Yuan, J. M., Govindarajan, S. & Ross, R. K.Epidemiology of hepatocellular carcinoma. Can. J.Gastroenterol. 14, 703–709 (2000).
23. Ming, L. et al. Dominant role of hepatitis B virus andcofactor role of aflatoxin in hepatocarcinogenesis inQidong, China. Hepatology 36, 1214–1220 (2002).
24. Turner, P. C. et al. The role of aflatoxins and hepatitisviruses in the etiopathogenesis of hepatocellularcarcinoma: a basis for primary prevention in Guinea-Conakry, West Africa. J. Gastroenterol. Hepatol. 17,S441–S448 (2002).
25. Hall, A. J. & Wild, C. P. Liver cancer in low and middleincome countries. BMJ 326, 994–995 (2003).
26. Koutsky, L. A. et al. A controlled trial of a humanpapillomavirus type 16 vaccine. N. Engl. J. Med. 347,1645–1651 (2002).
27. Chang, M. H. et al. Hepatitis B vaccination andhepatocellular carcinoma rates in boys and girls. JAMA284, 3040–3042 (2000).
28. Lubin, J. H. et al. Risk of lung cancer and residentialradon in China: pooled results of two studies. Int. J.Cancer 109, 132–137 (2004).
29. Kleinerman, R. et al. Lung cancer and indoor air pollutionin rural china. Ann. Epidemiol. 10, 469 (2000).
30. Bruce, N., Perez-Padilla, R. & Albalak, R. Indoor airpollution in developing countries: a major environmentaland public health challenge. Bull. World Health Organ.78, 1078–1092 (2000).
31. Zhou, B. S., Wang, T. J., Guan, P. & Wu, J. M. Indoor airpollution and pulmonary adenocarcinoma amongfemales: a case-control study in Shenyang, China. Oncol.Rep. 7, 1253–1259 (2000).
32. Smith, K. R. Inaugural article: national burden of diseasein India from indoor air pollution. Proc. Natl Acad. Sci.USA 97, 13286–13293 (2000).
33. Kleinerman, R. A. et al. Lung cancer and indoor exposureto coal and biomass in rural China. J. Occup. Environ.Med. 44, 338–344 (2002).
34. Lan, Q., Chapman, R. S., Schreinemachers, D. M., Tian,L. & He, X. Household stove improvement and risk oflung cancer in Xuanwei, China. J. Natl Cancer. Inst .94,826–835 (2002).
35. Chen, Y. & Ahsan, H. Cancer burden from arsenic indrinking water in Bangladesh. Am. J. Public Health 94,741–744 (2004).
36. Khan, M. M., Sakauchi, F., Sonoda, T., Washio, M. &Mori, M. Magnitude of arsenic toxicity in tube-welldrinking water in Bangladesh and its adverse effects on
human health including cancer: evidence from a review ofthe literature. Asian Pac. J. Cancer Prev. 4, 7–14 (2003).
37. Lamm, S. H., Byrd, D. M., Kruse, M. B., Feinleib, M. &Lai, S. H. Bladder cancer and arsenic exposure:differences in the two populations enrolled in a study insouthwest Taiwan. Biomed. Environ. Sci. 16, 355–368(2003).
38. Guo, H. R. Arsenic level in drinking water and mortality oflung cancer (Taiwan). Cancer Causes Control 15,171–177 (2004).
39. Xia, Y. & Liu, J. An overview on chronic arsenism viadrinking water in PR China. Toxicology 198, 25–29(2004).
40. Ferreccio, C. et al. Lung cancer and arsenicconcentrations in drinking water in Chile. Epidemiology11, 673–679 (2000).
41. Weinberg, C. Arsenic and drinking water. Epidemiology15, 255–256 (2004).
42. Jha, P., Ranson, M. K., Nguyen, S. N. & Yach, D.Estimates of global and regional smoking prevalence in1995, by age and sex. Am. J. Public Health 92,1002–1006 (2002).
43. Chattopadhyay, B. P., Alam, J. & Roychowdhury, A.Pulmonary function abnormalities associated withexposure to automobile exhaust in a diesel bus garageand roads. Lung 181, 291–302 (2003).
44. Ueno, D. et al. Global pollution monitoring of PCBs andorganochlorine pesticides using skipjack tuna as abioindicator. Arch. Environ. Contam. Toxicol. 45,378–389 (2003).
45. Zahm, S. H., Ward, M. H. & Blair, A. Pesticides andcancer. Occup. Med. 12, 269–289 (1997).
46. Dosemeci, M. et al. Cohort study among workersexposed to benzene in China: II. Exposure assessment.Am. J. Ind. Med. 26, 401–411 (1994).
47. Hallal, P. C., Victora, C. G., Wells, J. C. & Lima, R. C.Physical inactivity: prevalence and associated variables inBrazilian adults. Med. Sci. Sports Exerc. 35, 1894–1900(2003).
48. Rastogi, T. et al. Physical activity and risk of coronaryheart disease in India. Int. J. Epidemiol. (2004).
49. Tudor-Locke, C., Ainsworth, B. E., Adair, L. S., Du, S. &Popkin, B. M. Physical activity and inactivity in Chineseschool-aged youth: the China Health and NutritionSurvey. Int. J. Obes. Relat. Metab. Disord. 27,1093–1099 (2003).
50. Boyd, D. B. Insulin and cancer. Integr. Cancer Ther. 2,315–329 (2003).
51. Calle, E. E. & Kaaks, R. Overweight, obesity and cancer:epidemiological evidence and proposed mechanisms.Nature Rev. Cancer 4, 579–591 (2004).
52. Gajalakshmi, V., Peto, R., Kanaka, S. &Balasubramanian, S. Verbal autopsy of 48 000 adultdeaths attributable to medical causes in Chennai(formerly Madras), India. BMC Public Health 2, 7 (2002).
53. Murray, C. J. L., Lopez, A. D. & World HealthOrganization. The Global Burden of Disease, Volume 1. Acomprehensive assessment of mortality and disabilityfrom diseases, injuries, and risk factors in 1990 and
NATURE REVIEWS | CANCER VOLUME 4 | NOVEMBER 2004 | 917