Embed Size (px)
Citation preview

SUPERVISOR dr. Sabar P. Siregar, Sp.KJ
MORNING REPORT
Sunday Morning, January 26th 2014

I. PATIENT’S IDENTITY
AutoanamnesisName : Mr. KAge : 56 years oldGender : MaleAddress : KebumenOccupation : Unemployed (ex- Labor)Marital status : MarriedLast education : Engineering schoolAlloanamnesisName : Mr. ZAge : 44 years oldRelation to patient : Younger brother

REASON PATIENT WAS BROUGHT TO HOSPITAL
Broke the household, talk to herself,
wandering around and didn’t come back

STRESSOR
Probably lost her job because of disaster
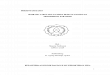
- Self grooming got worse :• Didn’t want to eat• Didn’t want to sleep• Didn’t want to take a bath- Poor utilization of leisure time- Social withdrawl
Present History 2 weeks ago
4 days ago•Patient looked sorrow, more quiet and oftenly by himself
•The patient told his wife that he heard the voice of many people want to kill him and his family and cut his body
•Patient looked confuse
- Has not worked.- Patient was wandering around, but
still able to come home. Never talk to his neighbors (social withdrawl)
- Poor utilization of leisure time- Self grooming still good
• The symptoms getting worse
• Looking more confuse• Loss of appetite and only
taking bath when he is asked
• Patient gave a knife to his wife to protect herself as he thought that someone
wanted to kill him and his family

Present History 1 day ago•Patient told his family that he wanted to go to his neighbor’s house. But the patient didn’t go home, and found naked in the field. The patient took off his clothes because he thought that he has been followed.
Has not worked., bizzare behaviourPatient was wandering around and not
coming back Poor utilization of leisure timeSelf grooming worser

Present History Day of admission
• The symptoms get worse• When his brother visits him, he threatens his brother with his carpenter tools.
• The family concerned about the patient’s condition
• Patient was accompanied by his brother
Self grooming got worsePoor utilization of leisure time
Social relationship getting worse
Psychiatric History
•Patient has psychiatric history before. 8 years ago the patient being hospitalized in RSJ Magelang for 2 weeks. The patient didn’t take the medicine afterwards and did not go to the hospital for his medical check up.

•Head injury (-)•Hypertension (?) – no valid data•Convulsion (-)•Asthma (-)•Allergy (-)•History of admission (-)
General medical history
•Drugs consumption (-) •Alcohol consumption (-)•Cigarette Smoking (-)
Drugs and alcohol abuse
history and smoking history
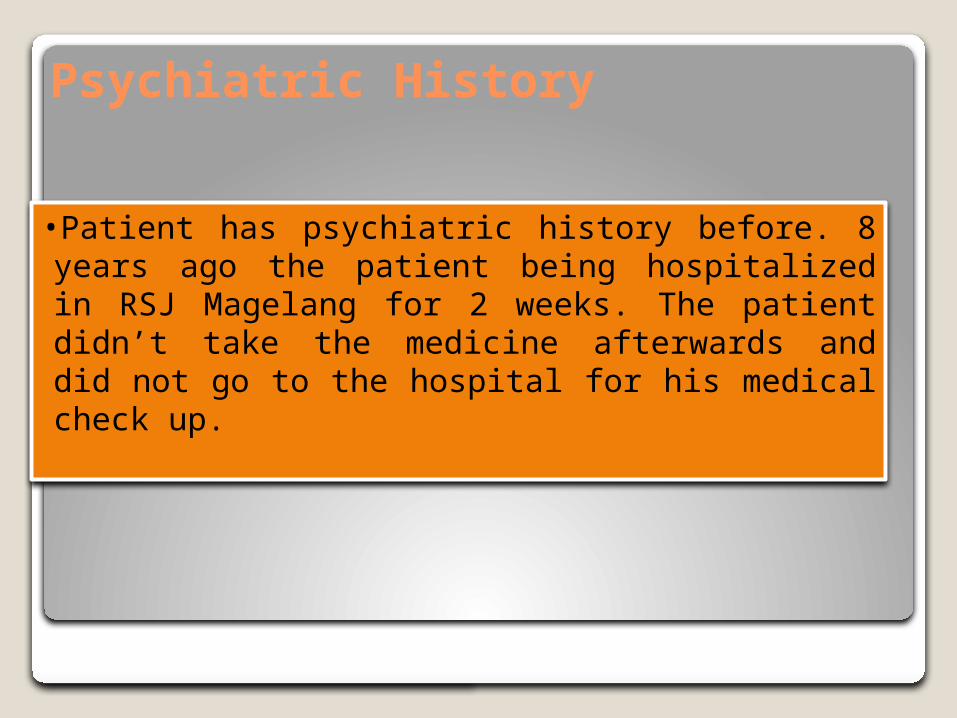
EARLY CHILDHOOD PHASE (0-3 YEARS OLD)Psychomotoric (NO VALID DATA) • There were no valid data on patients growth and development such as:
• first time lifting the head (3-6 months)• rolling over (3-6 months)• Sitting (6-9 months)• Crawling (6-9 months)• Standing (6-9 months)• walking-running (9-12 months)• holding objects in her hand(3-6 months)• putting everything in her mouth(3-6 months)
Psychosocial (NO VALID DATA) • There were no valid data on which age patient
• started smiling when seeing another face (3-6 months)• startled by noises(3-6 months)• when the patient first laugh or squirm when asked to play, nor playing claps with
others (6-9 months)
Communication (NO VALID DATA) • There were no valid data on when patient started saying words 1 year like ‘mom’ or ‘dad’.
(6-9 months)

Emotion (NO VALID DATA) There were no valid data of patient’s reaction when playing,
frightened by strangers, when starting to show jealousy or competitiveness towards other and toilet training.
Cognitive (NO VALID DATA) There were no valid data on which age the patient can follow objects,
recognizing her mother, recognize his family members. There were no valid data on when the patient first copied sounds
that were heard, or understanding simple orders.

INTERMEDIATE CHILDHOOD (3-11 YEARS OLD)
Psychomotor (NO VALID DATA) No valid data on when patient’s first time playing hide and seek or if patient
ever involved in any kind of sports.
Psychosocial (NO VALID DATA) No valid data on patient interaction with his surrounding, no valid data on
when patient first entered primary school, on how well patient handle separation from parent, how well he play with his new friend on first day school.
Communication (NO VALID DATA) No valid data regarding patient ability to make friends at school and how
many friends patient have during his school period
Emotional (NO VALID DATA)No valid data on patient’s adaptation under stress, any incidents of
bedwetting were not known.
Cognitive (NO VALID DATA)No valid data on patient’s cognitive.
LATE CHILDHOOD & TEENAGE PHASE
Sexual development signs & activity (NO VALID DATA) No data on when patient first experience wet dream, etc.
Psychomotor (NO VALID DATA) No data if patient had any favourite hobbies or games, if patient involved in
any kind of sports.Psychosocial (NO VALID DATA)
Patient had never been told the parent about patient friend.Emotional (NO VALID DATA)
No valid data on patients reaction on playing, scared, showed jealously or competitiveness
Communication (NO VALID DATA) No valid data on how well the relationship between patient with parent and
other family.

ADULTHOOD Educational History
Engineering School
Occupational history Unemployed
The patient worked as labor for 10 years, unsettled work place. 2 weeks ago patient got fired because the company was bankrupt
Marital Status Married
Criminal HistoryNo
Social Activity Restricted, only have a few
friends.
Current Situation He lives with his wife and one child
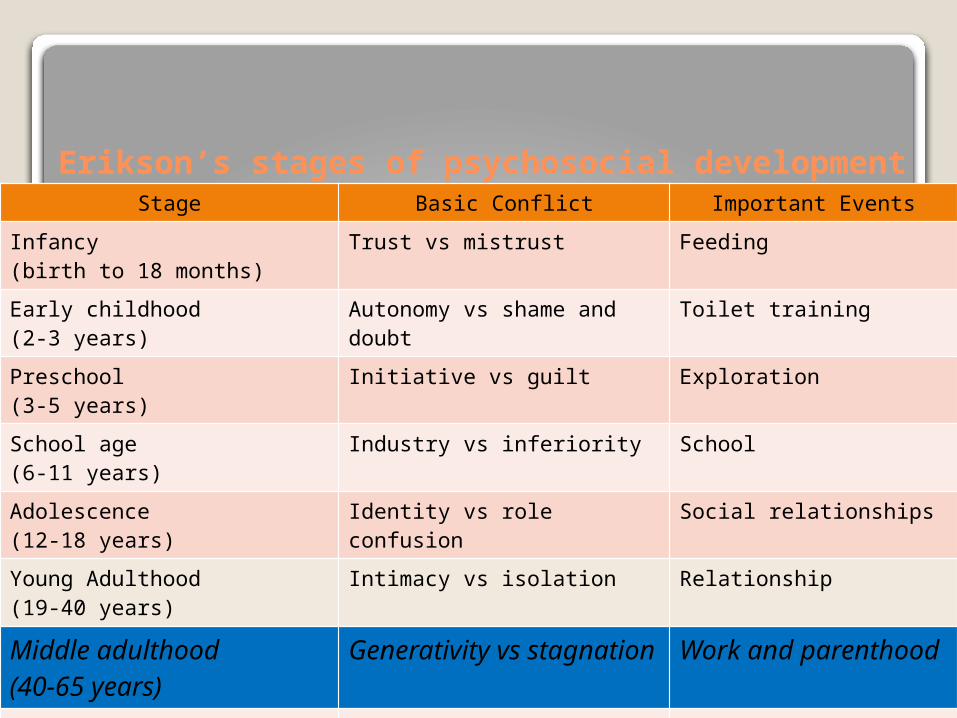
Erikson’s stages of psychosocial developmentStage Basic Conflict Important Events
Infancy(birth to 18 months)
Trust vs mistrust Feeding
Early childhood(2-3 years)
Autonomy vs shame and doubt
Toilet training
Preschool(3-5 years)
Initiative vs guilt Exploration
School age(6-11 years)
Industry vs inferiority School
Adolescence(12-18 years)
Identity vs role confusion Social relationships
Young Adulthood(19-40 years)
Intimacy vs isolation Relationship
Middle adulthood(40-65 years)
Generativity vs stagnation
Work and parenthood
Maturity(65- death)
Ego integrity vs despair Reflection on life

Family history
Patient is the 1st child out of seven siblings.
Patient has 3 children that lives and only one child living together with him and his wife
Psychiatry history in the family (-)

Patient realises that he is male, his behaviour is appropriate for male and is attracted to woman.
Psychosexual history

Genogram• Suffers from
mental illness• Female• Male

Socio-economic history• Economic scale : average
Validity
• Alloanamnesis : valid• Autoanamnesis : not valid

Progression of disorder
Symptom
Role function
2006 2014
Mental State(Sunday Morning, 26th January 2014)
Appearance • a woman, appropriate to her age, completely
clothedState of Consciousness• Clouded
Speech• Quantity : decreased• Quality : decreased
Behaviour
HypoactiveHyperactiveEchopraxiaCatatoniaActive negativismCataplexyStreotypyMannerismAutomatismBizarre
Command automatismMutismAcathysiaTicSomnabulismPsychomotor agitationCompulsiveAtaxiaMimicryAggresiveImpulsiveAbulia

ATTITUDE
• Non-cooperative
• Indiferrent• Apathy• Tension• Dependent• Passive
• Infantile• Distrust• Labile• Rigid• Passive negativism
• Stereotypy• Catalepsy• Cerea flexibility• Excitement

Emotion
Mood• Dysphoric• Euthymic• Elevated• Euphoria• Expansive• Irritable• Agitation• Can’t be assesed
Affect• Appropriate• Inappropriate• Restrictive• Blunted• Flat• Labile
Disturbance of perception
Hallucination
• Auditory (-) • Visual (+)• Olfactory (-)• Gustatory (-)• Tactile (-)• Somatic (-)
Illusion
• Auditory (-)• Visual (-)• Olfactory (-)• Gustatory (-)• Tactile (-)• Somatic (-)
Depersonalization (-) Derealization (-)
Thought progressionQuantity
• Logorrhea• Blocking• Remming• Mutism• Talk active
Quality• Irrelevant answer• Incoherence• Flight of idea• Poverty of speech• Confabulation• Loosening of association• Neologisme• Circumtansiality• Tangential • Verbigrasi • Perseverasi • Sound association• Word salad• Echolalia
Content of thought
Idea of Reference Idea of GuiltPreoccupationObsessionPhobia Delusion of PersecutionDelusion of ReferenceDelusion of JealousyDelusion of HipochondryDelusion of magic-mystic
Delusion of grandiose Delusion of Control Delusion of Influence Delusion of Passivity Delusion of Perception Delusion of Suspicious Thought of Echo Thought of
Insertion/withdrawal Thought of Broadcasting

Form of thought
RealisticNon RealisticDereisticAutistic
Sensorium and Cognition Level of education : average General knowledge : average Orientation of time/place/people/situation:
bad/good/good/bad Working/short/long memory: not cooperative Writing and reading skills : not cooperative Visuospatial : not cooperative Abstract thinking : not cooperative Ability to self care : poor

MMSE Orientation of time/place/people/situation:
bad/bad/bad/bad Registration : poor Attention : poor Memory : poor Language : not cooperative Visuospatial : not cooperative
MMSE couldn’t be asseses completedly because the patient is not cooperative
Impulse control when examined•Self control: enough•Patient response to
examiners question: poor
Insight •Impaired insight•Intellectual Insight•True Insight

Internal StatusConsciousnes : compos mentisVital sign :
◦Blood pressure : 120/90 mmHg◦Pulse rate : 100x/mnt◦Temperature : afebris◦RR : 20 x/mnt
Head : normocephali
Eyes : anemic conjungtiva -/-, icteric sclera -/-, pupil isocore
Neck : normal, no rigidity, no palpable lymph nodes
Thorax:
Cor : S 1,2 Sound and normal
Lung : vesicular sound, wheezing -/-, ronchi-/-
Abdomen : Pain (-) , normal peristaltic, tympany sound
Extremity : Warm acral, capp refill <2”,
Neurological exam : not examined
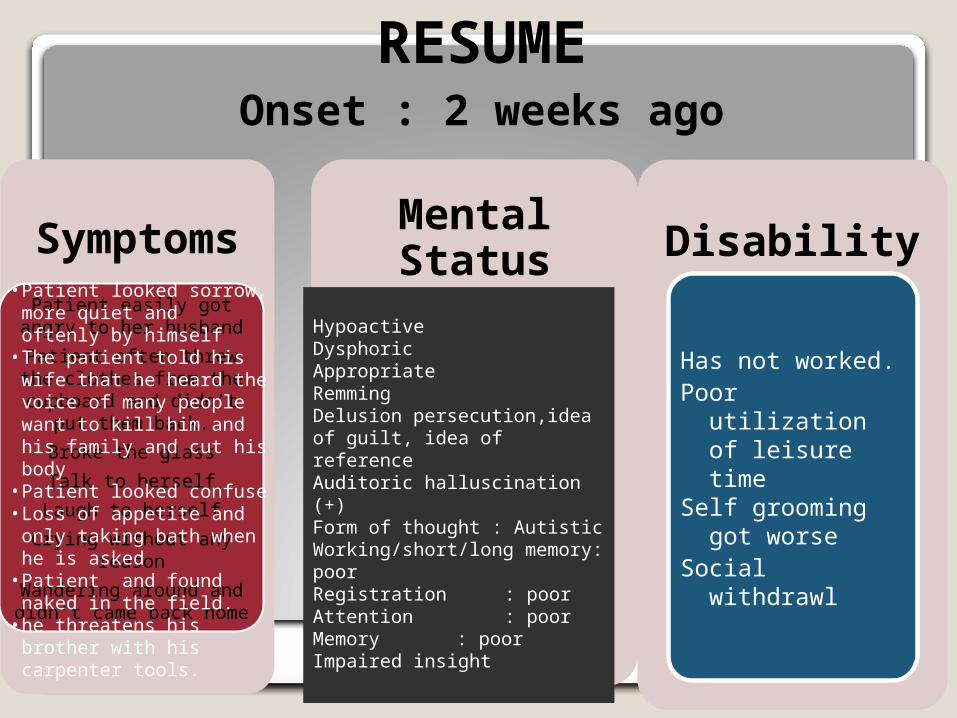
RESUMEOnset : 2 weeks ago
Symptoms
Patient easily got angry to her husband
Patient often threw the clothes from the
cupboard and didn’t put them back.
Broke the glassTalk to herself
Laugh to herselfCrying without any
reasonWandering around and didn’t came back home
Mental Status
HypoactiveDysphoricAppropriateRemmingDelusion persecution,idea of guilt, idea of reference Auditoric halluscination (+)Form of thought : AutisticWorking/short/long memory: poorRegistration : poorAttention : poorMemory : poorImpaired insight
Disability
Has not worked.Poor utilization of
leisure timeSelf grooming got
worse Social withdrawl
• Patient looked sorrow, more quiet and oftenly by himself
• The patient told his wife that he heard the voice of many people want to kill him and his family and cut his body
• Patient looked confuse• Loss of appetite and only
taking bath when he is asked• Patient and found naked in
the field.• he threatens his brother with
his carpenter tools.
Differential Diagnosis
F20.0 Schizophrenia ParanoidF23.1 Acute Polymorfic Psychotic
Disorder with Schizophrenia Symptom
F25.3 Schizoaffective Disorder Depressive type
Multiaxial DiagnosisAxis I : F 20.0 schizofrenia paranoidAxis II : R46.8 delayed diagnosis of axis IIAxis III : No diagnosisAxis IV : Problem with occupation and economic
status (patient’s got fired from his recent job)
Axis V : GAF admission 20-11
PLANNING MANAGEMENT
Inpatient (hospitalization)The patient had shown aggressive behaviour that was disrupting and endanger people around him.
Response Recovery
RESPONSE PHASE
Emergency department Inj. Haloperidol 5mg i.m. Inj. Diazepam 10 mg i.v.
Ward (routine therapy)Antipsychotics : Tab Haloperidol 5mg
s2dd1 tab
RECOVERY PHASE
Outpatient managementPharmacotherapyOccupation Therapy

Thank You…

















![[LIBRO] Schizofrenia](https://img.dokumen.tips/doc/110x75/5571f91049795991698eb5a1/libro-schizofrenia.jpg)